T he management of conditionsassociated with an intense in-flammatory response such assevere trauma and sepsis rep-
resents a major challenge in the care ofthe critically ill. There is an emergingconsensus that the acute inflammatoryresponse to major stress might be inap-propriate or lead to undesirable outcomesin patients initially resuscitated success-fully. In the last two decades, much hasbeen learned regarding cellular and mo-lecular mechanisms of the acute inflam-
matory response. This progress has led toconsiderable efforts and resources to de-velop interventions that modulate theacute inflammatory response and posi-tively affect outcome in these patients.Except for recombinant human activatedprotein C (drotrecogin alfa [activated])(1) and low-dose steroids (2), this knowl-edge has not led to effective immuno-modulatory therapies; consequently, asignificant effort to address the issue oftarget confirmation and trial design hasensued (3–9). This situation is especially
vexing considering that a reasonabletherapeutic rationale was supported byanimal and early phase human studies fordozens of interventions that failed whenevaluated in phase III (10–12).
Several researchers have proposed avariety of reasons to explain the incon-gruence between results and expecta-tions. We propose that a key reason forthis conundrum is the difficulty of pre-dicting the impact of modifying singlecomponents of the highly complex, non-linear, and redundant inflammatory re-sponse (13–18). The consequences of fail-ing to take a systems-oriented approachto understanding and predicting thetime-course of complex diseases are var-ious and significant. Indeed, prediction ofthe behavior of such systems derivedfrom localized insights gathered fromlimited experiments or observations per-taining to individual components on suchsystems may be impossible, however ac-curate these isolated observations maybe. Meteorologists, engineers, physicists,and other scientists examining complex
Objective: To determine the feasibility and potential usefulnessof mathematical models in evaluating immunomodulatory strate-gies in clinical trials of severe sepsis.
Design: Mathematical modeling of immunomodulation in sim-ulated patients.
Setting: Computer laboratory.Measurements and Main Results: We introduce and evaluate
the concept of conducting a randomized clinical trial in silicobased on simulated patients generated from a mechanistic math-ematical model of bacterial infection, the acute inflammatoryresponse, global tissue dysfunction, and a therapeutic interven-tion. Trial populations are constructed to reflect heterogeneity inbacterial load and virulence as well as propensity to mount andmodulate an inflammatory response. We constructed a cohort of1,000 trial patients submitted to therapy with one of three differ-ent doses of a neutralizing antibody directed against tumor ne-crosis factor (anti-TNF) for 6, 24, or 48 hrs. We present cytokineprofiles over time and expected outcome for each cohort. Weidentify subgroups with high propensity for being helped orharmed by the proposed intervention and identify early serummarkers for each of those subgroups.
The mathematical simulation confirms the inability of simplemarkers to predict outcome of sepsis. The simulation clearlyseparates cases with favorable and unfavorable outcome on thebasis of global tissue dysfunction. Control survival was 62.9% at1 wk. Depending on dose and duration of treatment, survivalranged from 57.1% to 80.8%. Higher doses of anti-TNF, althougheffective, also result in considerable harm to patients. A statisticalanalysis based on a simulated cohort identified markers of favor-able or adverse response to anti-TNF treatment.
Conclusions: A mathematical simulation of anti-TNF therapyidentified clear windows of opportunity for this intervention aswell as populations that can be harmed by anti-TNF therapy. Theconstruction of an in silico clinical trial could provide profoundinsight into the design of clinical trials of immunomodulatorytherapies, ranging from optimal patient selection to individualizeddosage and duration of proposed therapeutic interventions. (CritCare Med 2004; 32:2061–2070)
From the Department of Critical Care Medicine andClinical Research (G Clermont), Investigation and Sys-tems Modeling in Acute Illness (CRISMA) laboratory,University of Pittsburgh School of Medicine, Pittsburgh,PA; Immunetrics, Inc. (JB)Pittsburgh, PA; Departmentof Physics and Astronomy (RK), Department of Math-ematics and Statistics (G Constantine, CC), and De-partment of Surgery (VV), University of PittsburghSchool of Medicine, PA
Supported, in part, by grant R01-GM62740 fromthe National Institutes of Health, Bethesda, MD.
Drs. Clermont, Vodovotz, and Chow are minorityshare holders in Immunetrics, Inc (all �5%). They also
offer consultancy services to Immunetrics, Inc. Thishas been determined to be a Significant FinancialInterest by Public Health Service criteria. Their activitywith this company has been and remains monitored bythe Entrepreneurial Oversight Committee at the Uni-versity of Pittsburgh. The software used to run thesimulation is not licensed by Immunetrics and was theproduct of the combined efforts of Mr. Bartels, Ms.Kumar, and Dr. Clermont.
systems make extensive use of models,simplified representations of those com-plex systems, to shed useful insight onthe behavior of such systems.
We sought to adopt a similar approachand conduct a practical demonstration ofmodeling a clinical trial in silico, by exam-ining a therapy that had initial great prom-ise in the setting of animal models of sepsisbut failed in large, randomized clinical tri-als to meet generally accepted criteria forefficacy. Accordingly, we focused on theconsequences of the administration to sep-sis patients of a neutralizing antibody di-rected against the proinflammatory cyto-kine tumor necrosis factor (anti-TNF) (19).After promising nonhuman primate re-sults, pooled outcome of no fewer than 11clinical trials in 7,265 patients showed aconsistent absolute reduction in mortalityof approximately 3.2% (p � .006) favoringtreatment with anti-TNF antibodies, a dis-appointing result in light of the effect ex-pected from preclinical studies (20, 21). Ef-forts to select populations that woulddemonstrate a convincing benefit from an-ti-TNF have not met expectations either(20, 21).
We wish to illustrate insights thatmathematical models could provide inelucidating the reasons for the disap-pointing results of this particular agentand, more generally, in the design of fu-ture trials, especially regarding drug dos-ing, duration of therapy, and interactionamong cointerventions.
METHODS
Overview. We initially designed a mecha-nistic model of the acute inflammatory re-sponse based on information available fromthe existing literature on the roles of key cel-lular and molecular effectors in response to abacterial pathogen (22, 23). We constructed apopulation of virtual patients differing in theirinitial bacterial load, bacterial virulence, timeof initiation of intervention, and genetic abil-ity to generate effectors in response to stress.We compared outcomes across several treat-ment arms and identified determinants of fa-vorable and unfavorable outcomes.
Modeling the Human Inflammatory Re-sponse. Because the acute inflammatory re-sponse is comprised of a large number of com-ponents that each have specific roles yet arehighly interactive, we chose to model this dy-namical system with a system of differentialequations, one for each component that wechose to simulate (Appendix). Each equation de-scribes the level or concentration of componentsover time resulting from their interaction withother components following the principle ofmass-action. We chose to represent the system
at this level because serum levels of cytokines,for example, are well known to correlate withoutcome in septic patients (24–28), clinicalmeasurements are usually obtained from blood,and chemotherapeutic interventions are typi-cally administered intravenously. Limitations re-sulting from this choice are discussed subse-quently. The strengths of such an approach areseveral, in that it a) provides an intuitive meansto translate mechanistic concepts into a mathe-matical framework; b) can be analyzed using alarge body of existing techniques; c) can be nu-merically simulated easily and inexpensively ona desktop computer; d) provides both qualitativeand quantitative predictions; and e) allows ex-pansion to higher levels of complexity.
Initial values for rate constants were deter-mined empirically so that the model wouldqualitatively reproduce observed literaturedata in mice administered endotoxin or sub-jected to cecal ligation and puncture (23, 29).Some rate constants, such as cytokine half-lives, were directly extracted from the litera-ture (30–32).
Constructing a Clinical Trial of Anti-TNF.We generated a study population of 1,000 virtualpatients. Pathogen characteristics (growth rate
and initial load) were chosen to result in a sur-vival of approximately 60%. We varied the delaybefore medical consultation, and thus eligibilityfor treatment, reasoning that the distribution ofthe delays to medical consultation after onset ofinfection was related to initial pathogen load andvirulence (i.e., sicker patients would generallyconsult earlier). To simulate genetic diversity ofthe study population, we randomly varied indi-vidual propensity of immune cells to generateeffector molecules (proinflammatory such asTNF and interleukin [IL]-6), anti-inflammatory,and nitric oxide synthase activity) from �25% ofbaseline as dictated by literature data (33). Thosevariations were sufficient to explain wide swingsin individual serum levels of effectors.
Optimizing Trial Design. We wished to il-lustrate the application of mathematical model-ing to optimizing the design of a clinical trial.We achieved this demonstration in two steps.First, we identify administration strategies thatwould result in the best outcomes for the entirecohort. Second, we illustrate how the simulationcan help with patient selection, given a treat-ment administration regimen. Importantly, ourgoal was specifically not the optimization oftreatment regimen to individuals, although this
Table 1. Time to detection of disease and 7-day survival by quartilea of the population
Baseline Characteristics 7-Day Survival, % Mean Detection Time, Hrs
TNF, tumor necrosis factor; iNOS, inducible nitric oxide synthase.aQuartiles are from lowest values (Q1) to highest (Q4) for effector cell propensity to elaborate
products for a given stimulus, for pathogen initial inoculum, for pathogen virulence, and for time todetection of disease; bp � .01 between quartiles for mortality; cp � .01 between quartiles for differencein earliest detection time.
2062 Crit Care Med 2004 Vol. 32, No. 10
constitutes another potential application of oursimulation.
To identify optimal dosing and duration ofadministration strategies, we submitted thevirtual cohort of 1,000 patients to nine inter-ventions with anti-TNF. We varied the dura-tion of administration of anti-TNF (6, 24, or 48hrs). Comparatively, the half-life of anti-TNFantibodies in naïve patients is 40–50 hrs (34,35) We simulated the binding of serum TNFwith three different “doses” of anti-TNF (2, 10,and 20 arbitrary units). Depending on dose,TNF neutralization varied from 18.6% to55.5% of total TNF produced in controls. Aclear correlation with published reports is dif-ficult as these do not typically report areasunder the curve and do not always distinguishbetween biologically active TNF, TNF boundby antibody, and TNF bound by specific solu-ble receptors (35). Death was determined bythe inability of the individuals to clear morethan 50% of maximal sustained tissue dys-function at one week. Such a definition seg-regated the population into two outcomegroups (see the Results).
Trial optimization involves selecting a dosingstrategy that optimizes outcome in a cohort ofpatients and then selecting patients who wouldbenefit from treatment while avoiding treatingpatients for which treatment would either haveno effect or cause harm. The optimal treatmentadministration scheme has already been deter-mined as part of prior results (see precedingsection). To select patients who would most ben-efit from this treatment, we constructed a multi-nomial logistic model with a four-valued out-
come variable: a) is helped by treatment(survives but would have died without treat-ment); b) survives irrespective of treatment; c)dies irrespective of treatment; and d) is harmed(dies because of treatment). Independent vari-ables were chosen at the time of disease detec-tion (the earliest possible treatment opportu-nity) and 60 mins later, reflecting the possibilityof using short-term trends in analytes and as-suming rapid diagnostic capabilities. Variablesincluded serum TNF, anti-inflammatory activity,long-acting proinflammatory cytokine (IL-6),their ratios and products, activated protein C,thrombin, as well as blood pressure and cellcounts of activated neutrophils. The statisticalmodel was validated in a different population of1,000 simulated cases. All predictions from thestatistical model relate to the validation popula-tion.
We wrote our own software for the simu-lations and analyses (JB, RK, GC). Statisticalanalyses and multivariate statistical modelswere conducted in SPSS (Chicago, IL).
RESULTS
Baseline Population
Characteristics of the baseline popula-tion and outcome are detailed in Table 1.Mean time to medical consultation was20.1 hr from the onset of infection and wasshorter in patients with high pathogen loadand high virulence. Survivors had lower
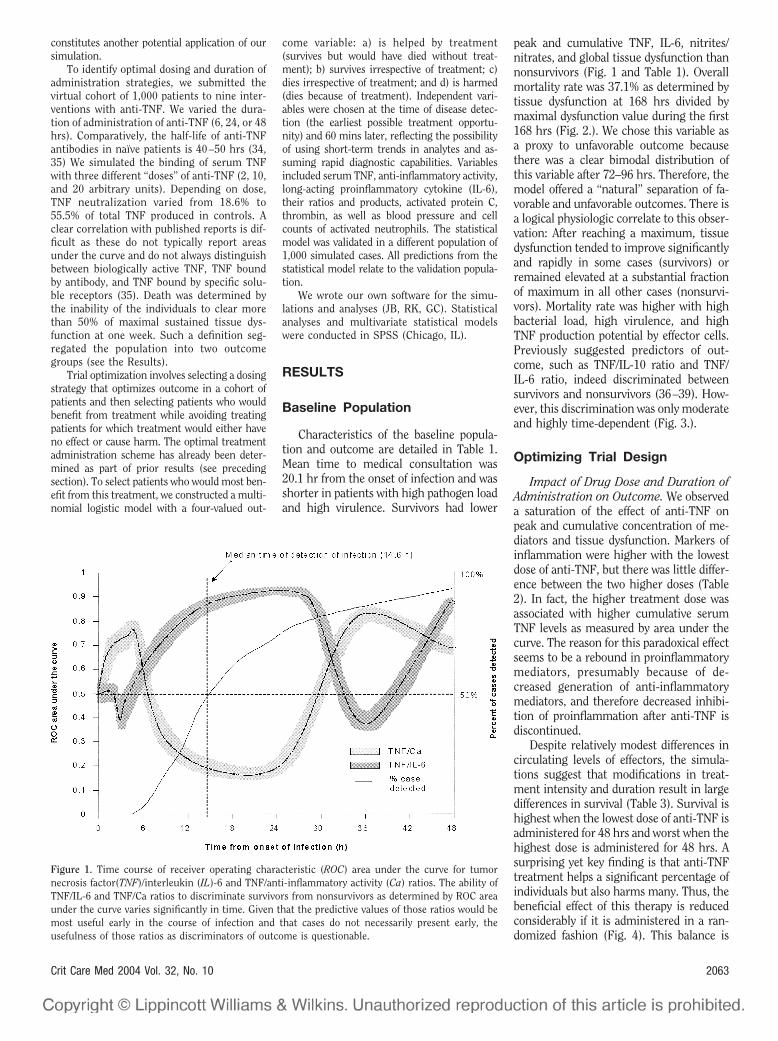
peak and cumulative TNF, IL-6, nitrites/nitrates, and global tissue dysfunction thannonsurvivors (Fig. 1 and Table 1). Overallmortality rate was 37.1% as determined bytissue dysfunction at 168 hrs divided bymaximal dysfunction value during the first168 hrs (Fig. 2.). We chose this variable asa proxy to unfavorable outcome becausethere was a clear bimodal distribution ofthis variable after 72–96 hrs. Therefore, themodel offered a “natural” separation of fa-vorable and unfavorable outcomes. There isa logical physiologic correlate to this obser-vation: After reaching a maximum, tissuedysfunction tended to improve significantlyand rapidly in some cases (survivors) orremained elevated at a substantial fractionof maximum in all other cases (nonsurvi-vors). Mortality rate was higher with highbacterial load, high virulence, and highTNF production potential by effector cells.Previously suggested predictors of out-come, such as TNF/IL-10 ratio and TNF/IL-6 ratio, indeed discriminated betweensurvivors and nonsurvivors (36–39). How-ever, this discrimination was only moderateand highly time-dependent (Fig. 3.).
Optimizing Trial Design
Impact of Drug Dose and Duration ofAdministration on Outcome. We observeda saturation of the effect of anti-TNF onpeak and cumulative concentration of me-diators and tissue dysfunction. Markers ofinflammation were higher with the lowestdose of anti-TNF, but there was little differ-ence between the two higher doses (Table2). In fact, the higher treatment dose wasassociated with higher cumulative serumTNF levels as measured by area under thecurve. The reason for this paradoxical effectseems to be a rebound in proinflammatorymediators, presumably because of de-creased generation of anti-inflammatorymediators, and therefore decreased inhibi-tion of proinflammation after anti-TNF isdiscontinued.
Despite relatively modest differences incirculating levels of effectors, the simula-tions suggest that modifications in treat-ment intensity and duration result in largedifferences in survival (Table 3). Survival ishighest when the lowest dose of anti-TNF isadministered for 48 hrs and worst when thehighest dose is administered for 48 hrs. Asurprising yet key finding is that anti-TNFtreatment helps a significant percentage ofindividuals but also harms many. Thus, thebeneficial effect of this therapy is reducedconsiderably if it is administered in a ran-domized fashion (Fig. 4). This balance is
Figure 1. Time course of receiver operating characteristic (ROC) area under the curve for tumornecrosis factor(TNF)/interleukin (IL)-6 and TNF/anti-inflammatory activity (Ca) ratios. The ability ofTNF/IL-6 and TNF/Ca ratios to discriminate survivors from nonsurvivors as determined by ROC areaunder the curve varies significantly in time. Given that the predictive values of those ratios would bemost useful early in the course of infection and that cases do not necessarily present early, theusefulness of those ratios as discriminators of outcome is questionable.
2063Crit Care Med 2004 Vol. 32, No. 10
also very dependent on drug dose and du-ration. The proportion of patients helped byanti-TNF increases with dosage, but so doesthe proportion of patients harmed. Dura-tion also had a significant impact on sur-vival, but less so than dose. There wastherefore a clear, but nonintuitive, interac-tion between dose and duration to affectoverall survival.
Improving Case Selection in aClinical Trial
To illustrate the implications of usingmodeling to improve case selection in clin-ical trials, we selected as an interventionthe administration of anti-TNF at an inter-mediate dose for 24 hrs. We chose thisintervention as opposed to the optimal one(low-dose anti-TNF administered for 48hrs) because we wished to illustrate thepotential of modeling to identify patientsharmed by an intervention. Under this in-tervention, 242 cases were helped by treat-ment, whereas 181 were harmed, for aglobal survival advantage of 6.1% in theanti-TNF arm. Cases helped by anti-TNFtreatment had higher peak TNF, IL-6, andanti-inflammatory levels. They also tendedto have higher initial pathogen load andhigher pathogen virulence. Nonsurvivorswho were not helped by treatment hadoverwhelming infection and were treatedlate, and TNF levels tended to be low atonset of treatment. Patients harmed bytherapy tended to have infections of mod-erate severity but were low TNF respondersand high anti-inflammatory responders(Fig. 5). Interestingly, low production ofTNF and high production of IL-10, deter-mined by specific genetic polymorphisms,have been shown to be beneficial in trans-plant patients (40). However, potentially in-dependent determinants of outcome suchas pathogen load, virulence, and vigor ofeffector cells to produce TNF are not acces-sible to clinicians having to decide whetherto administer treatment.
We therefore constructed a statisticalmodel in which the independent variableswere based on levels of effectors and cellcounts measured at the beginning and 60mins into the earliest treatment window,and we assessed the ability of this statisticalmodel to identify patients potentiallyhelped or harmed by the intervention. Ac-tual and predicted outcomes from this sta-tistical model are presented in Table 4. Thismodel also demonstrated that several vari-ables other than mediators were predictiveof response to therapy. Specifically, base-
line circulating TNF, IL-6, TNF to anti-inflammatory activity ratio, neutrophilscirculating thrombin, and activated proteinC were predictive of treatment efficacy (p �
.01). Sixty-minute trends in TNF, IL-6, TNFto IL-6 ratio, TNF to IL-6 product, and TNFto anti-inflammatory activity ratio werealso predictive.
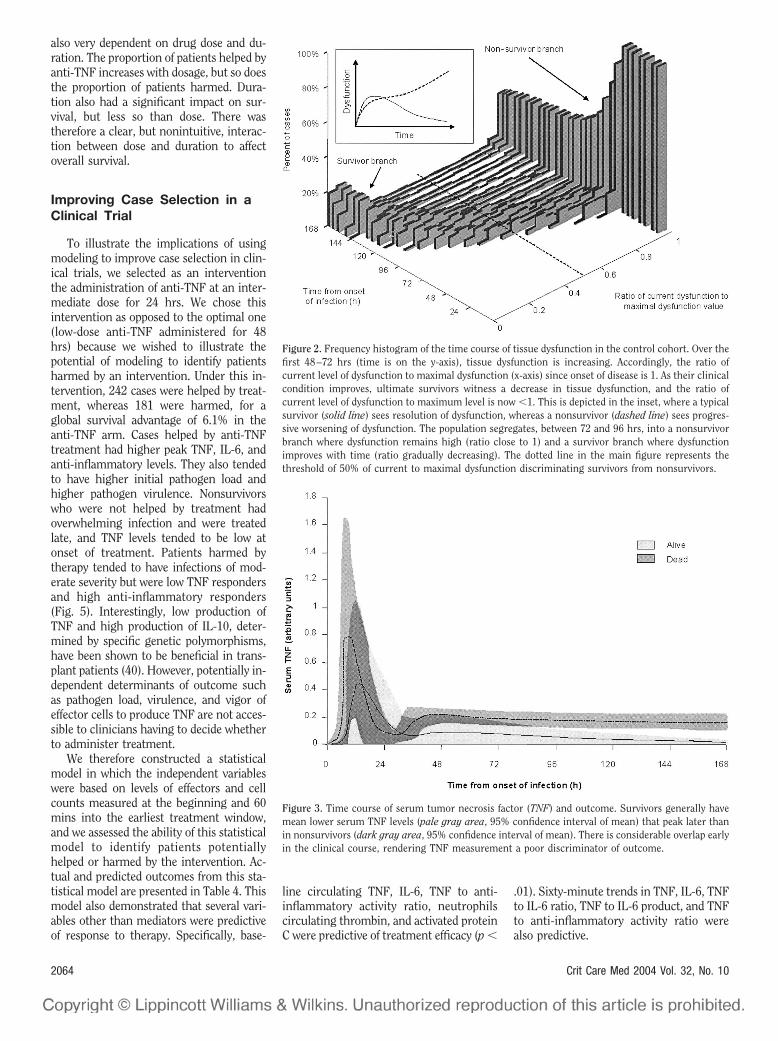
Figure 2. Frequency histogram of the time course of tissue dysfunction in the control cohort. Over thefirst 48–72 hrs (time is on the y-axis), tissue dysfunction is increasing. Accordingly, the ratio ofcurrent level of dysfunction to maximal dysfunction (x-axis) since onset of disease is 1. As their clinicalcondition improves, ultimate survivors witness a decrease in tissue dysfunction, and the ratio ofcurrent level of dysfunction to maximum level is now �1. This is depicted in the inset, where a typicalsurvivor (solid line) sees resolution of dysfunction, whereas a nonsurvivor (dashed line) sees progres-sive worsening of dysfunction. The population segregates, between 72 and 96 hrs, into a nonsurvivorbranch where dysfunction remains high (ratio close to 1) and a survivor branch where dysfunctionimproves with time (ratio gradually decreasing). The dotted line in the main figure represents thethreshold of 50% of current to maximal dysfunction discriminating survivors from nonsurvivors.
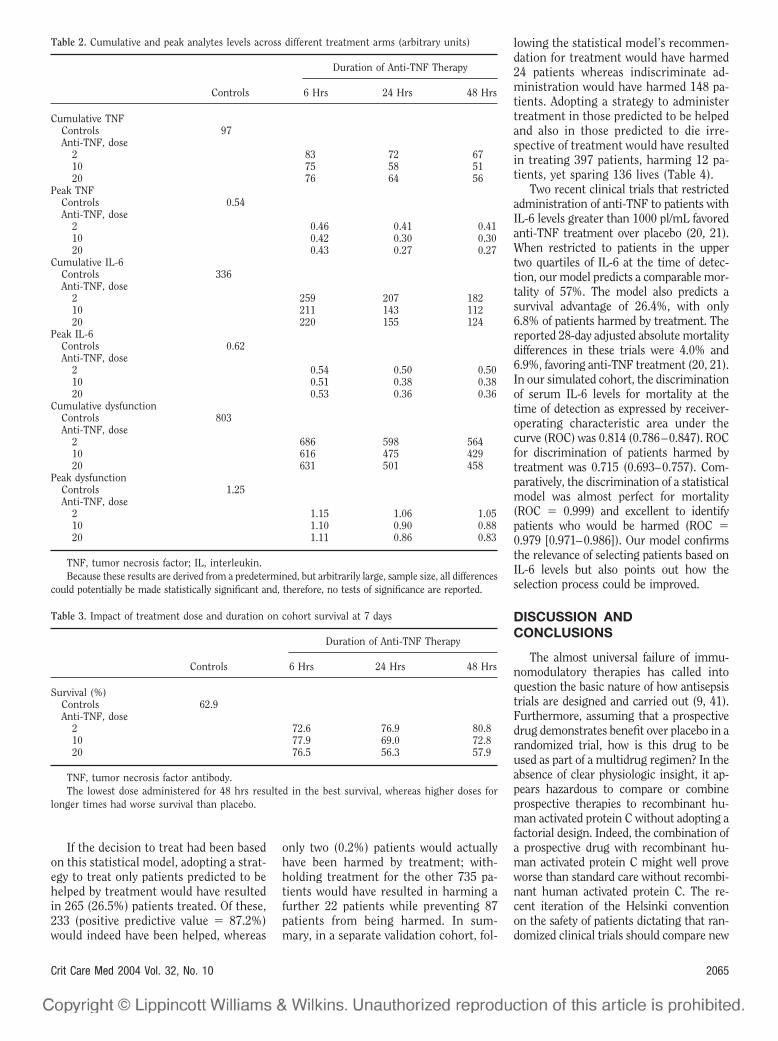
Figure 3. Time course of serum tumor necrosis factor (TNF) and outcome. Survivors generally havemean lower serum TNF levels (pale gray area, 95% confidence interval of mean) that peak later thanin nonsurvivors (dark gray area, 95% confidence interval of mean). There is considerable overlap earlyin the clinical course, rendering TNF measurement a poor discriminator of outcome.
2064 Crit Care Med 2004 Vol. 32, No. 10
If the decision to treat had been basedon this statistical model, adopting a strat-egy to treat only patients predicted to behelped by treatment would have resultedin 265 (26.5%) patients treated. Of these,233 (positive predictive value � 87.2%)would indeed have been helped, whereas
only two (0.2%) patients would actuallyhave been harmed by treatment; with-holding treatment for the other 735 pa-tients would have resulted in harming afurther 22 patients while preventing 87patients from being harmed. In sum-mary, in a separate validation cohort, fol-
lowing the statistical model’s recommen-dation for treatment would have harmed24 patients whereas indiscriminate ad-ministration would have harmed 148 pa-tients. Adopting a strategy to administertreatment in those predicted to be helpedand also in those predicted to die irre-spective of treatment would have resultedin treating 397 patients, harming 12 pa-tients, yet sparing 136 lives (Table 4).
Two recent clinical trials that restrictedadministration of anti-TNF to patients withIL-6 levels greater than 1000 pl/mL favoredanti-TNF treatment over placebo (20, 21).When restricted to patients in the uppertwo quartiles of IL-6 at the time of detec-tion, our model predicts a comparable mor-tality of 57%. The model also predicts asurvival advantage of 26.4%, with only6.8% of patients harmed by treatment. Thereported 28-day adjusted absolute mortalitydifferences in these trials were 4.0% and6.9%, favoring anti-TNF treatment (20, 21).In our simulated cohort, the discriminationof serum IL-6 levels for mortality at thetime of detection as expressed by receiver-operating characteristic area under thecurve (ROC) was 0.814 (0.786–0.847). ROCfor discrimination of patients harmed bytreatment was 0.715 (0.693–0.757). Com-paratively, the discrimination of a statisticalmodel was almost perfect for mortality(ROC � 0.999) and excellent to identifypatients who would be harmed (ROC �0.979 [0.971–0.986]). Our model confirmsthe relevance of selecting patients based onIL-6 levels but also points out how theselection process could be improved.
DISCUSSION ANDCONCLUSIONS
The almost universal failure of immu-nomodulatory therapies has called intoquestion the basic nature of how antisepsistrials are designed and carried out (9, 41).Furthermore, assuming that a prospectivedrug demonstrates benefit over placebo in arandomized trial, how is this drug to beused as part of a multidrug regimen? In theabsence of clear physiologic insight, it ap-pears hazardous to compare or combineprospective therapies to recombinant hu-man activated protein C without adopting afactorial design. Indeed, the combination ofa prospective drug with recombinant hu-man activated protein C might well proveworse than standard care without recombi-nant human activated protein C. The re-cent iteration of the Helsinki conventionon the safety of patients dictating that ran-domized clinical trials should compare new
Table 2. Cumulative and peak analytes levels across different treatment arms (arbitrary units)
TNF, tumor necrosis factor; IL, interleukin.Because these results are derived from a predetermined, but arbitrarily large, sample size, all differences
could potentially be made statistically significant and, therefore, no tests of significance are reported.
Table 3. Impact of treatment dose and duration on cohort survival at 7 days
TNF, tumor necrosis factor antibody.The lowest dose administered for 48 hrs resulted in the best survival, whereas higher doses for
longer times had worse survival than placebo.
2065Crit Care Med 2004 Vol. 32, No. 10
compounds to the current “best” does nottrivially apply to the problem of sepsis (6).Insights as to how to improve the design ofsuch trials, including reducing the need foran unrealistically large number of patientsyet preserving enough sensitivity to detectclinical benefit, are yet to emerge. There isgrowing sense of the need for a paradigmshift in this regard and that the concept ofthe randomized controlled trial, as weknow it, might face insurmountable chal-lenges in the context of multimodal thera-pies of complex disease. We propose that anintense effort at modeling of complex phys-iologic processes and their modulationmight become an essential tool in the de-sign of clinical trials of emerging therapiesin this context. Although basic scientistsand clinicians perceive the need for a morecomprehensive approach to understandingphysiologic dynamics and their modula-tion, significant advances in the implemen-tation of practical tools derived from this“complex systems” approach have not beenforthcoming. Reasons for this include theunfamiliarity of medical scientists with thenecessary analytical tools involved, the per-ceived complexity of the processes to bemodeled, the incomplete knowledge of themechanisms involved, the difficulty in gen-erating results that are perceived useful byinterested parties, and lack of insight as tothe limits and biases of conventional statis-tical approaches and reductionism-drivenhypothesis testing (13, 14, 17).
We present such an implementation as apractical approach to the vexing problem ofimmunomodulation in patients with severesepsis. The results of the simulation pre-sented herein reproduce many observa-tions characteristic of this disease process.
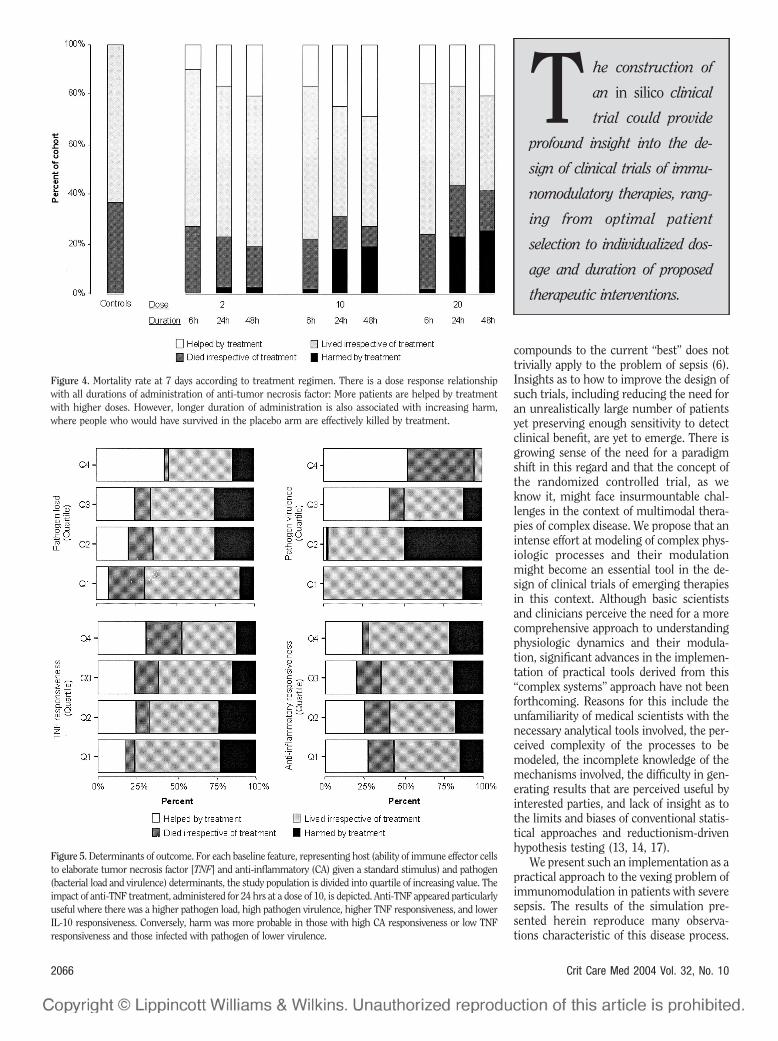
Figure 4. Mortality rate at 7 days according to treatment regimen. There is a dose response relationshipwith all durations of administration of anti-tumor necrosis factor: More patients are helped by treatmentwith higher doses. However, longer duration of administration is also associated with increasing harm,where people who would have survived in the placebo arm are effectively killed by treatment.
Figure 5. Determinants of outcome. For each baseline feature, representing host (ability of immune effector cellsto elaborate tumor necrosis factor [TNF] and anti-inflammatory (CA) given a standard stimulus) and pathogen(bacterial load and virulence) determinants, the study population is divided into quartile of increasing value. Theimpact of anti-TNF treatment, administered for 24 hrs at a dose of 10, is depicted. Anti-TNF appeared particularlyuseful where there was a higher pathogen load, high pathogen virulence, higher TNF responsiveness, and lowerIL-10 responsiveness. Conversely, harm was more probable in those with high CA responsiveness or low TNFresponsiveness and those infected with pathogen of lower virulence.
T he construction of
an in silico clinical
trial could provide
profound insight into the de-
sign of clinical trials of immu-
nomodulatory therapies, rang-
ing from optimal patient
selection to individualized dos-
age and duration of proposed
therapeutic interventions.
2066 Crit Care Med 2004 Vol. 32, No. 10
For example, in a disease where tissue dys-function results from excessive immunestimulation, it is reasonable to find thatthere is dose-response behavior to inter-vention in patients who are helped. It isalso reasonable that excessive suppressionof appropriate inflammation, especially ifan individual has a limited capacity to gen-erate inflammation, results in harm. Yet,the simulation furnishes nonintuitive pre-dictions as to how an intervention wouldhave to be designed to optimize clinicalresponse. Our results are humbling in thatthere clearly appear to be opposing effectsof immunomodulation in severe sepsis,where patients are both saved and killed,that are not apparent in the outcome ofclinical trials as currently measured. How-ever, our simulation also suggests thatmodeling could assist in further refiningenrollment criteria for trials or treatmentcriteria for approved interventions. Asshown, an intervention targeted to all thoseindividuals predicted to be helped, based onmeasured circulating analytes, physiologicparameters, and possibly genetic polymor-phisms, could be successful.
Further methodological developmentmight improve on the ability to predictlikely response to treatment. We presentherein a statistical model to achieve thisgoal. The intuition, however, is that thesame mathematical model that describesthe likely course of illness in individualpatients could be used to obtain improvedpredictions in individual patients based onsequential measurements of several ana-
lytes. How to accomplish this goal is ananalytical problem yet to be explored. Wesuggest that a diagnostic device that wouldmeasure relevant analytes repeatedly and innear-real time, coupled to a mathematicalmodel such as the one presented herein,could help predict the dynamics of inflam-mation of a particular patient and therebyguide intervention. An immediate exten-sion of such a development could be real-time monitoring of response to interven-tion, resulting in modification of theintervention before harm occurs or be-comes irreversible.
There are several limitations to our ap-proach. Our model remain essentially qual-itative, although we are currently conduct-ing efforts to calibrate the simulation usinganimal data (42, 43). A more quantitativecomparison to data from existing trialswould certainly be possible and would pro-vide further validation of the predictiveability of the model, assuming that longi-tudinal measurements of analytes were ob-tained. Although our simulations repro-duce several observations from clinicaltrials of anti-TNF treatment, we cannot atthis stage address nonattributable mortalityor attributable mortality beyond a limitedtime horizon. It is likely that the success oftreatments for severe sepsis is limited byfactors, such as burden of chronic diseaseand parameter organ physiologic reserve,which are not easily modeled. Our ap-proach does not take such factors into con-sideration. Equation-based models includea large number of parameters that express
the relative importance and time-scale ofinteraction and processes involved. The val-ues of these parameters are typically diffi-cult to extract from existing literature andtherefore attributed in such as way that themodel reproduces known kinetics of asmany variables as possible under a varietyof experimental conditions. This qualitativefitting exercise is time-consuming and doesnot guarantee that the resulting set of pa-rameters is either unique or optimal. Therelationship between gene polymorphismand outcome of patients with sepsis hasbeen difficult to document (33, 44–50). Al-though models such as the one presentedherein provide clear predictions, these aredifficult to confirm in the absence of con-sistent clinical and epidemiologic studies.One expects systematic advances in thenext few years as substantial efforts are un-derway to elucidate the relationship be-tween sepsis outcome and polymorphismsof effectors of the acute inflammatory re-sponse.
In recent years, modeling complex bio-logical systems has become increasinglyuseful and is moving toward practical ap-plications (18, 51, 52). Companies have of-fered similar approaches to simulate clini-cal trials (www.entelos.com) pertaining toasthma and diabetes but not to critical ill-ness. It appears essential to continuedprogress that complex biological problemssuch as sepsis be approached through col-laborative efforts to enhance the face valid-ity and acceptance of the process for allthose involved. It is therefore necessary tocall on the resources and insights of clini-cians, bench scientists, and mathemati-cians to address this problem. Importantly,efforts to construct models applicable tohumans would greatly benefit from unpub-lished data collected in phase I and II trials.This is a nontrivial endeavor that requiresclose collaboration between academiciansof disparate backgrounds and industry (13–15). It is our hope that given such an effort,we will see a new generation of therapeu-tics to successfully address the seeminglyintractable problem of sepsis and organdysfunction.
REFERENCES
1. Bernard GR, Vincent JL, Laterre PF, et al:Efficacy and safety of recombinant humanactivated protein C for severe sepsis. N EngJ Med 2001; 344:699–709
2. Annane D, Sebille V, Charpentier C, et al: Effectof treatment with low doses of hydrocortisoneand fludrocortisone on mortality in patientswith septic shock. JAMA 2002; 288:862–871
3. Levi M, van der Poll T, ten Cate H, et al: The
Table 4. Comparison of simulated outcome and prediction of a statistical model regarding the benefitof anti-tumor necrosis factor (TNF) before treatment administration
Observed Outcome
Predicted Outcome
TotalPercentage
Helped byTreatment
AliveIrrespective of
Treatment
DeadIrrespective of
TreatmentHarmed byTreatment
Helped by treatment 231 6 12 4 25.3Alive irrespective of treatment 17 409 3 38 46.7Dead irrespective of treatment 15 0 117 0 13.2Harmed by treatment 2 59 0 87 14.8
Total percentage 26.5 47.4 13.2 12.9 100
The sum of the rows corresponds to observed simulated outcome for anti-TNF administered at a doseof 10 units for 24 hrs, whereas the sum of the columns corresponds to predicted outcome from a logisticmultinomial model. Adopting a strategy to treat patients predicted to be either helped by anti-TNF orpatients predicted to die irrespective of treatment would result in 397 patients treated (sum of the first andthird column). In ten patients, the model recommended withholding treatment while it would bebeneficial, thus resulting in an error of omission (italicized numbers). Of those in whom treatment isrecommended by the statistical model, two of 265 would actually be harmed (boldface number), thusresulting in an error of commission. With indiscriminate administration, 148 patients would, in fact, havebeen harmed by treatment. Following the recommendation of a statistical model would, therefore, save 136lives (148–2–10) and avert the administration of drug in 603 patients.
2067Crit Care Med 2004 Vol. 32, No. 10
cytokine-mediated imbalance between coagulantand anticoagulant mechanisms in sepsis and en-dotoxaemia. Eur J Clin Invest 1997; 27:3–9
4. Warren BLE: High-dose antithrombin III insevere sepsis: a randomized controlled trial.JAMA 2001; 286:1869–1878
5. Cohen J, Guyatt G, Bernard GR, et al: New strat-egies for clinical trials in patients with sepsis andseptic shock. Crit Care Med 2001; 29:880–886
6. Cross AS, Opal SM: A new paradigm for the treat-ment of sepsis: Is it time to consider combinationtherapy? Ann Intern Med 2003; 138:502–505
7. Cross AS, Opal SM, Bhattacharjee K, et al:Immunotherapy of sepsis: Flawed concept orfaulty implementation? Vaccine 1999;17(Suppl 2):S13–S21
8. Levy MM, Fink MP, Marshall JC, et al: 2001SCCM/ESICM/ACCP/ATS/SIS InternationalSepsis Definitions Conference. Crit Care Med2003; 31:1250–1256
9. Opal SM: Clinical trial design and outcomesin patients with severe sepsis. Shock 2003;20:295–302
10. Bone RC: Immunologic dissonance: A con-tinuing evolution in our understanding ofthe systemic inflammatory response syn-drome (SIRS) and the multiple organ dys-function syndrome (MODS). Ann Intern Med1996; 125:680–687
11. Freeman BD, Quezado Z, Zeni F, et al: rG-CSF reduces endotoxemia and improves sur-vival during E. coli pneumonia. J ApplPhysiol 1997; 83:1467–1475
12. Zeni F, Freeman B, Natanson C: Anti-inflammatory therapies to treat sepsis andseptic shock: A reassessment. Crit Care Med1997; 25:1095–1100
13. Buchman TG, Cobb JP, Lapedes AS, et al:Complex systems analysis: A tool for shockresearch. Shock 2001; 16:248–251
14. Neugebauer EA, Willy C, Sauerland S: Complex-ity and non-linearity in shock research: Reduc-tionism or synthesis? Shock 2001; 16:252–258
15. Tjardes T, Neugebauer E: Sepsis research in thenext millennium: concentrate on the softwarerather than the hardware. Shock 2002; 17:1–8
16. Godin PJ, Buchman TG: Uncoupling of bio-logical oscillators: A complementary hypoth-esis concerning the pathogenesis of multipleorgan dysfunction syndrome. Crit Care Med1996; 24:1107–1116
17. Seely AJE, Christou NV: Multiple organ dys-function syndrome: Exploring the paradigmof complex nonlinear systems. Crit Care Med2000; 28:2193–2200
18. An G: Agent-based computer simulation andSIRS: Building a bridge between basic scienceand clinical trials. Shock 2001; 16:266–273
19. Reinhart K, Karzai W: Anti-tumor necrosisfactor therapy in sepsis: Update on clinicaltrials and lessons learned. Crit Care Med2001; 29:S121–S125
20. Reinhart K, Menges T, Gardlund B, et al:Randomized, placebo-controlled trial of theanti-tumor necrosis factor antibody frag-ment afelimomab in hyperinflammatory re-sponse during severe sepsis: The RAMSESStudy. Crit Care Med 2001; 29:765–769
21. Panacek EA, Marshall J, Fischkoff S, et al:Neutralization of TNF by a monoclonal anti-body improves survival and reduces organdysfunction in human sepsis: Results of theMONARCS trial. Chest 2000; 118:88S
22. Clermont G, Chow CC, Kumar R, et al: Math-ematical simulation of the innate immuneresponse. Crit Care Med 2001; 29:A111
23. Lagoa CE, Clermont G, Kumar R, et al: Predic-tion of the acute inflammatory response from amathematical model. Chest 2003; 124:121S
24. Waage A, Brandtzaeg P, Halstensen A, et al:The complex pattern of cytokines in serumfrom patients with meningococcal septicshock. Association between interleukin 6, in-terleukin 1, and fatal outcome. J Exp Med1989; 169:333–338
25. Marks JD, Marks CB, Luce JM, et al: Plasmatumor necrosis factor in patients with septicshock. Mortality rate, incidence of adult re-spiratory distress syndrome, and effects ofmethylprednisolone administration. Am RevRespir Dis 1990; 141:94–97
26. Calandra T, Gerain J, Heumann D, et al: Highcirculating levels of interleukin-6 in patientswith septic shock: Evolution during sepsis,prognostic value, and interplay with othercytokines. The Swiss-Dutch J5 Immunoglob-ulin Study Group. Am J Med 1991; 91:23–29
27. Thijs LG, Hack CE: Time course of cytokinelevels in sepsis. Intensive Care Med 1995;21(Suppl 2):S258–S263
28. van Dissel JT, van Langevelde P, WestendorpRG, et al: Anti-inflammatory cytokine profileand mortality in febrile patients. Lancet1998; 351:950–953
29. Kumar R, Chow CC, Clermont G, et al: Atheoretical model for the simulation of sep-sis. J Leukoc Biol 2001; (Suppl):90
31. Ferraiolo BL, Moore JA, Crase D, et al: Phar-macokinetics and tissue distribution of recom-binant human tumor necrosis factor-alpha inmice. Drug Metab Dispos 1988; 16:270–275
32. Oliver JC, Bland LA, Oettinger CW, et al:Cytokine kinetics in an in vitro whole bloodmodel following an endotoxin challenge.Lymphokine Cytokine Res 1993; 12:115–120
33. Louis E, Franchimont D, Piron A, et al: Tu-mour necrosis factor (TNF) gene polymor-phism influences TNF-alpha production inlipopolysaccharide (LPS)-stimulated wholeblood cell culture in healthy humans. ClinExp Immunol 1998; 113:401–406
34. Moller A, Emling F, Blohm D, et al: Mono-clonal antibodies to human tumor necrosisfactor alpha: in vitro and in vivo application.Cytokine 1990; 2:162–169
35. Fisher CJ Jr, Opal SM, Dhainaut JF, et al: Influ-ence of an anti-tumor necrosis factor monoclonalantibody on cytokine levels in patients with sep-sis. The CB0006 Sepsis Syndrome Study Group.Crit Care Med 1993; 21:318–327
36. Taniguchi T, Koido Y, Aiboshi J, et al: Changein the ratio of interleukin-6 to interleukin-10predicts a poor outcome in patients with sys-
temic inflammatory response syndrome. CritCare Med 1999; 27:1262–1264
37. Brivet FG, Emilie D, Galanaud P: Pro- andanti-inflammatory cytokines during acute se-vere pancreatitis: An early and sustained re-sponse, although unpredictable of death. Pa-risian Study Group on Acute Pancreatitis.Crit Care Med 1999; 27:749–755
38. Dodoo D, Omer FM, Todd J, et al: Absolutelevels and ratios of proinflammatory and anti-inflammatory cytokine production in vitro pre-dict clinical immunity to Plasmodium falcipa-rum malaria. J Infect Dis 2002; 185:971–979
39. Payen D, Faivre V, Lukaszewicz AC, et al: As-sessment of immunological status in the criti-cally ill. Minerva Anestesiol 2000; 66:757–763
40. Bathgate AJ, Pravica V, Perrey C, et al: Theeffect of polymorphisms in tumor necrosisfactor-alpha, interleukin-10, and transform-ing growth factor-beta1 genes in acute he-patic allograft rejection. Transplantation2000; 69:1514–1517
41. Remick DG: Cytokine therapeutics for thetreatment of sepsis: Why has nothingworked? Curr Pharm Des 2003; 9:75–82
42. Lagoa C, Clermont G, Kumar R, et al: Pre-diction of the acute inflammatory responsefrom a mathematical model. Chest 2003;124:121S
43. Vodovotz Y, Chow C, Kumar R, et al: Simu-lating the roles of NO in septic shock. NitricOxide 2002; 6:484–484
44. Freeman BD, Buchman TG: Gene in a hay-stack: Tumor necrosis factor polymorphismsand outcome in sepsis. Crit Care Med 2000;28:3090–3091
45. Gallagher PM, Lowe G, Fitzgerald T, et al:Association of IL-10 polymorphism with se-verity of illness in community acquiredpneumonia. Thorax 2003; 58:154–156
46. Holmes CL, Russell JA, Walley KR: Geneticpolymorphisms in sepsis and septic shock:Role in prognosis and potential for therapy.Chest 2003; 124:1103–1115
47. Majetschak M, Flohe S, Obertacke U, et al:Relation of a TNF gene polymorphism tosevere sepsis in trauma patients. Ann Surg1999; 230:207–214
48. Mira JP, Cariou A, Grall F, et al: Associationof TNF2, a TNF-alpha promoter polymor-phism, with septic shock susceptibility andmortality: A multicenter study. JAMA 1999;282:561–568
49. Reid CL, Perrey C, Pravica V, et al: Geneticvariation in proinflammatory and anti-inflammatory cytokine production in multi-ple organ dysfunction syndrome. Crit CareMed 2002; 30:2216–2221
50. Stuber F: Effects of genomic polymorphismson the course of sepsis: Is there a concept forgene therapy? J Am Soc Nephrol 2001;12(Suppl 17):S60–S64
52. Bonabeau E: Agent-based modeling: methodsand techniques for simulating human sys-tems. Proc Natl Acad Sci USA 2002; 99(Suppl3):7280–7287
2068 Crit Care Med 2004 Vol. 32, No. 10
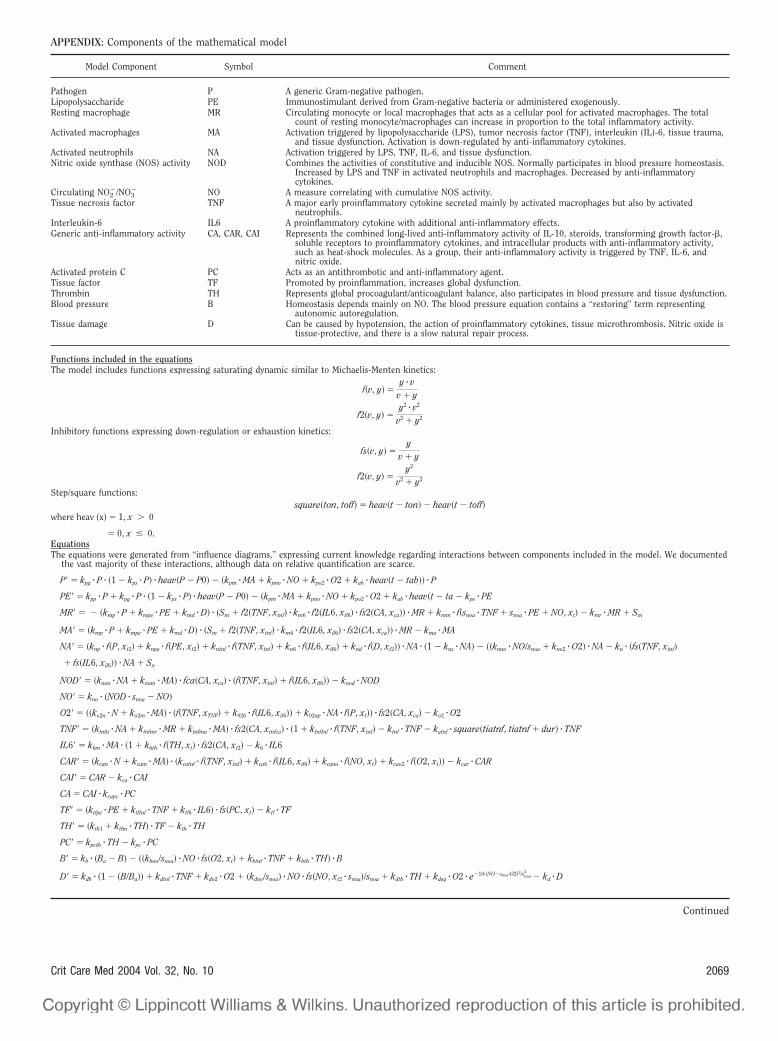
APPENDIX: Components of the mathematical model
Model Component Symbol Comment
Pathogen P A generic Gram-negative pathogen.Lipopolysaccharide PE Immunostimulant derived from Gram-negative bacteria or administered exogenously.Resting macrophage MR Circulating monocyte or local macrophages that acts as a cellular pool for activated macrophages. The total
count of resting monocyte/macrophages can increase in proportion to the total inflammatory activity.Activated macrophages MA Activation triggered by lipopolysaccharide (LPS), tumor necrosis factor (TNF), interleukin (IL)-6, tissue trauma,
and tissue dysfunction. Activation is down-regulated by anti-inflammatory cytokines.Activated neutrophils NA Activation triggered by LPS, TNF, IL-6, and tissue dysfunction.Nitric oxide synthase (NOS) activity NOD Combines the activities of constitutive and inducible NOS. Normally participates in blood pressure homeostasis.
Increased by LPS and TNF in activated neutrophils and macrophages. Decreased by anti-inflammatorycytokines.
Circulating NO2�/NO3
� NO A measure correlating with cumulative NOS activity.Tissue necrosis factor TNF A major early proinflammatory cytokine secreted mainly by activated macrophages but also by activated
neutrophils.Interleukin-6 IL6 A proinflammatory cytokine with additional anti-inflammatory effects.Generic anti-inflammatory activity CA, CAR, CAI Represents the combined long-lived anti-inflammatory activity of IL-10, steroids, transforming growth factor-�,
soluble receptors to proinflammatory cytokines, and intracellular products with anti-inflammatory activity,such as heat-shock molecules. As a group, their anti-inflammatory activity is triggered by TNF, IL-6, andnitric oxide.
Activated protein C PC Acts as an antithrombotic and anti-inflammatory agent.Tissue factor TF Promoted by proinflammation, increases global dysfunction.Thrombin TH Represents global procoagulant/anticoagulant balance, also participates in blood pressure and tissue dysfunction.Blood pressure B Homeostasis depends mainly on NO. The blood pressure equation contains a “restoring” term representing
autonomic autoregulation.Tissue damage D Can be caused by hypotension, the action of proinflammatory cytokines, tissue microthrombosis. Nitric oxide is
tissue-protective, and there is a slow natural repair process.
Functions included in the equationsThe model includes functions expressing saturating dynamic similar to Michaelis-Menten kinetics:
f�v, y� �y � v
v � y
f2�v, y� �y2 � v2
v2 � y2
Inhibitory functions expressing down-regulation or exhaustion kinetics:
� 0, x � 0.EquationsThe equations were generated from “influence diagrams,” expressing current knowledge regarding interactions between components included in the model. We documented
the vast majority of these interactions, although data on relative quantification are scarce.
P� � kpg � P � �1 � kps � P� � heav�P � P0� � �kpm � MA � kpno � NO � kpo2 � O2 � kab � heav�t � tab�� � P
PE� � kpp � P � kpg � P � �1 � kps � P� � heav�P � P0� � �kpm � MA � kpno � NO � kpo2 � O2 � kab � heav�t � ta � kpe � PE
MR� � � �kmp � P � kmpe � PE � kmd � D� � �Sm � f2�TNF, xtnf� � km6 � f2�IL6, xil6� � fs2�CA, xca�� � MR � kmm � f�snoa � TNF � snoa � PE � NO, xt� � kmr � MR � Sm
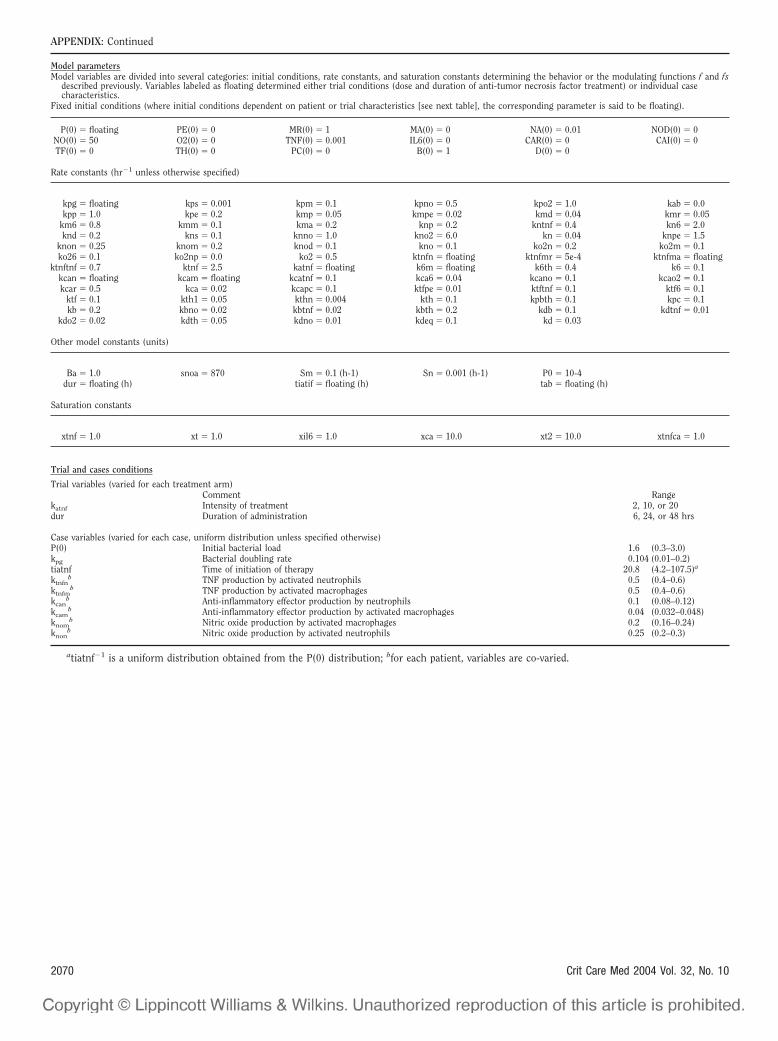
Trial variables (varied for each treatment arm)Comment Range
katnf Intensity of treatment 2, 10, or 20dur Duration of administration 6, 24, or 48 hrs
Case variables (varied for each case, uniform distribution unless specified otherwise)P(0) Initial bacterial load 1.6 (0.3–3.0)kpg Bacterial doubling rate 0.104 (0.01–0.2)tiatnf Time of initiation of therapy 20.8 (4.2–107.5)a
ktnfnb TNF production by activated neutrophils 0.5 (0.4–0.6)
ktnfmb TNF production by activated macrophages 0.5 (0.4–0.6)
kcanb Anti-inflammatory effector production by neutrophils 0.1 (0.08–0.12)
kcamb Anti-inflammatory effector production by activated macrophages 0.04 (0.032–0.048)
knomb Nitric oxide production by activated macrophages 0.2 (0.16–0.24)
knonb Nitric oxide production by activated neutrophils 0.25 (0.2–0.3)
atiatnf�1 is a uniform distribution obtained from the P(0) distribution; bfor each patient, variables are co-varied.
APPENDIX: Continued
Model parametersModel variables are divided into several categories: initial conditions, rate constants, and saturation constants determining the behavior or the modulating functions f and fs
described previously. Variables labeled as floating determined either trial conditions (dose and duration of anti-tumor necrosis factor treatment) or individual casecharacteristics.
Fixed initial conditions (where initial conditions dependent on patient or trial characteristics [see next table], the corresponding parameter is said to be floating).