24
In-Situ Simulation: Weaving Safety Culture into Interprofessional Education Sandeep Gangadharan, M.D. Kathleen Schmidt, RN, PNP Andrew Rotjan, ENP, FNP-BC, CHSE
In-Situ Simulation: Weaving Safety Culture into Interprofessional Education
Sandeep Gangadharan, M.D.Kathleen Schmidt, RN, PNPAndrew Rotjan, ENP, FNP-BC, CHSE
OBJECTIVES
1.Provide an overview of interprofessional clinical simulation
2.Highlight evidence base that supports simulation3.Discuss evidence based guidelines necessary for
simulation4.Review various methods of simulation5.Describe simulation modalities utilized by the
NorthShore-Long Island Jewish Health System6.Share lessons learned to promote successful
interprofessional simulation7. Implications of interprofessional simulation on patient
safety
Overview of Simulation
Simulation should: 1.“…aim to imitate real patient’s anatomic regions, or clinical tasks, or to mirror the real-life situations in which medical services are rendered1”
2.“…mimic the reality of a clinical environment and are designed to demonstrate procedures, decision-making, and critical thinking through techniques such as role playing and the use of devises such as videos or mannequins2”
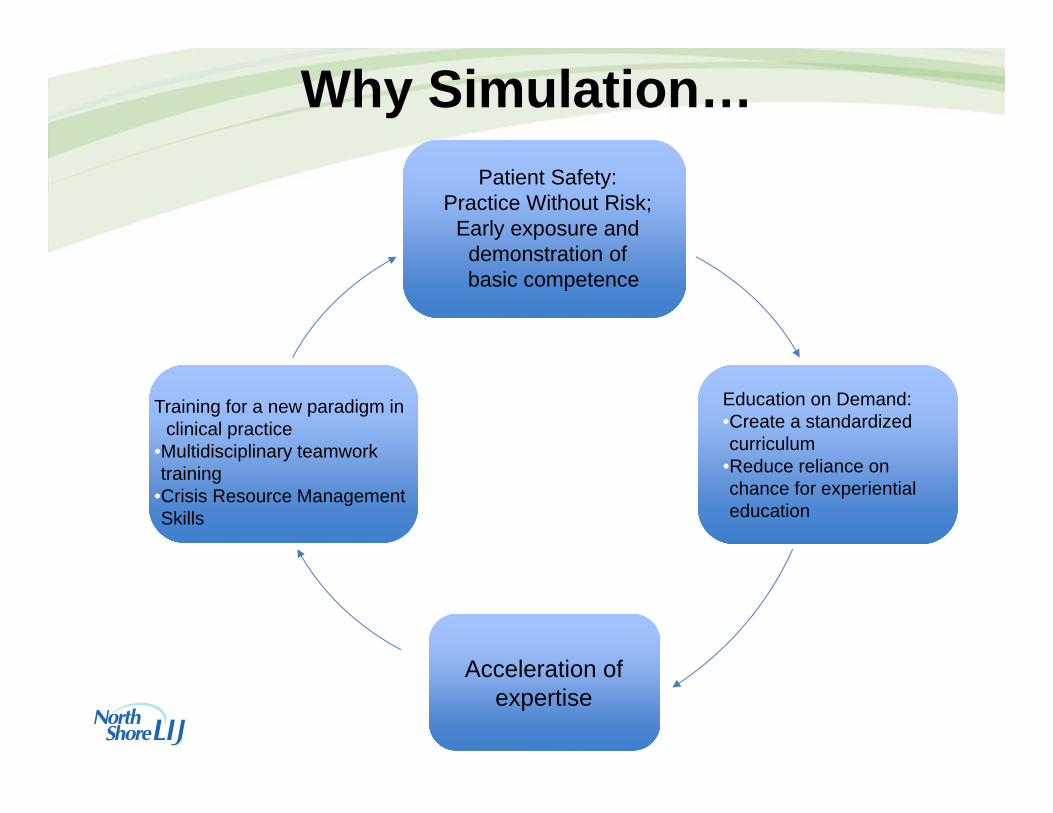
Why Simulation…Patient Safety:
Practice Without Risk;Early exposure and
demonstration ofbasic competence
Education on Demand:•Create a standardized curriculum
•Reduce reliance on chance for experiential education
Acceleration of expertise
Training for a new paradigm in clinical practice
•Multidisciplinary teamwork training
•Crisis Resource Management Skills

Why Simulation…
7. Barrett and Russell
The Circumplex Model of Affect
Childs, J. C. (2006). Clinical teaching by simulation lessons learned from a complex patient care scenario. Nurs Educ Perspect, 27(3), 154. Couto, Thomaz Bittencourt, Kerrey, Benjamin T., Taylor, Regina G., FitzGerald, Michael, & Geis, Gary L. (2015). Teamwork Skills in Actual, In Situ, and In-Center Pediatric Emergencies: Performance Levels Across Settings and Perceptions of Comparative Educational Impact. Simulation in Healthcare, 10(2), 76-84. doi: 10.1097/sih.0000000000000081Everett-Thomas, R., Valdes, B., Valdes, G. R., Shekhter, I., Fitzpatrick, M., Rosen, L. F., . . . Birnbach, D. J. (2014). Using Simulation Technology to Identify Gaps Between Education and Practice Among New Graduate Nurses. J Contin Educ Nurs, 1-7. doi: 10.3928/00220124-20141122-01Gaba, D. M. (2007). The future vision of simulation in healthcare. Simul Healthc, 2(2), 126-135. doi: 10.1097/01.SIH.0000258411.38212.32Hallenbeck, V. J. (2012). Use of high-fidelity simulation for staff education/development: a systematic review of the literature. J Nurses Staff Dev, 28(6), 260-269; quiz E269-210. doi: 10.1097/NND.0b013e31827259c7Hunt, E. A., Duval-Arnould, J. M., Nelson-McMillan, K. L., Bradshaw, J. H., Diener-West, M., Perretta, J. S., & Shilkofski, N. A. (2014). Pediatric resident resuscitation skills improve after "rapid cycle deliberate practice" training. Resuscitation, 85(7), 945-951. doi: 10.1016/j.resuscitation.2014.02.025Issenberg, S. B., McGaghie, W. C., Petrusa, E. R., Lee Gordon, D., & Scalese, R. J. (2005). Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach, 27(1), 10-28. doi: 10.1080/01421590500046924Issenberg, S. B., & Scalese, R. J. (2008). Simulation in health care education. Perspect Biol Med, 51(1), 31-46. doi: 10.1353/pbm.2008.0004Kolb, David A. (1984). Experiential learning : experience as the source of learning and development. Englewood Cliffs, N.J.: Prentice-Hall.Motola, I., Devine, L. A., Chung, H. S., Sullivan, J. E., & Issenberg, S. B. (2013). Simulation in healthcare education: a best evidence practical guide. AMEE Guide No. 82. Med Teach, 35(10), e1511-1530. doi: 10.3109/0142159X.2013.818632Norman, Jamil. (2012). Systematic Review of the Literature on Simulation in Nursing Education. ABNF Journal, 23(2), 24-28. Okuda, Y., Bryson, E. O., DeMaria, S., Jr., Jacobson, L., Quinones, J., Shen, B., & Levine, A. I. (2009). The utility of simulation in medical education: what is the evidence? Mt Sinai J Med, 76(4), 330-343. doi: 10.1002/msj.20127Pittman, Oralea A. (2012). The use of simulation with advanced practice nursing students. Journal of the American Academy of Nurse Practitioners, 24(9), 516-520. doi: 10.1111/j.1745-7599.2012.00760.xSalas, Eduardo, Wilson, Katherine A., Burke, C. Shawn, & Priest, Heather A. (2005). Using Simulation-Based Training to Improve Patient Safety: What Does It Take? Joint Commission Journal on Quality and Patient Safety, 31(7), 363-371. Tsai, T. C., Harasym, P. H., Nijssen-Jordan, C., & Jennett, P. (2006). Learning gains derived from a high-fidelity mannequin-based simulation in the pediatric emergency department. J Formos Med Assoc, 105(1), 94-98. doi: 10.1016/S0929-6646(09)60116-9Yang, Chih-Wei, Yen, Zui-Shen, McGowan, Jane E., Chen, Huiju Carrie, Chiang, Wen-Chu, Mancini, Mary E., . . . Ma, Matthew Huei-Ming. (2012). A systematic review of retention of adult advanced life support knowledge and skills in healthcare providers. Resuscitation, 83(9), 1055-1060. doi: http://dx.doi.org/10.1016/j.resuscitation.2012.02.027
Evidence for Simulation
Contribution to the Evidence
•International Network for Simulation‐Based Pediatric Innovation, Research and Education (INSPIRE) Network
ImPACTSSimulation Research Group
Fundamentals of Simulation Based Education
Setting the Foundation:• Fundamental Belief/Basic Assumption• Safety Contract
• We’re in Vegas!• Participant orientation and buy-in
• Formative assessment approachPeople who choose to participate in simulation based
training exercises are mature, intelligent, well-trained adults who want to improve and grow
Fundamentals of Simulation Based Education
Setting the Foundation:• Preparing for Simulation Based Education (SBE)
• Curriculum/Learning Objectives• Match objectives with learning outcomes3
• 1-4 key objectives that should be specific, relevant, and appropriate to the learner4
• Simulation scenario design1-4
• Always keep the objectives in mind• Relevant9• Realism vs theater• Map scenario pathways• Use a template


Fundamentals of Simulation Based Education
Setting the Foundation:• Simulation
• The Team• Who they are• Where are they• What is there mission
• Patient Care• History• Physical• Procedures
• Team Work• Communication
Remember the
Learning Objectives
Fundamentals of Simulation Based Education
Setting the Foundation:• Debrief
• Participant learning• Organization learning/latent safety errors• Models
• Plus/Delta model• What went well/What would you change3
• Advocacy/Inquiry (Debriefing with good judgement)• Advocate for objective data, follow with inquiry5
• Rapid Cycle Deliberate Practice6
• Correct behaviors as they occur• Review Objectives and Take-Aways
• Evaluations
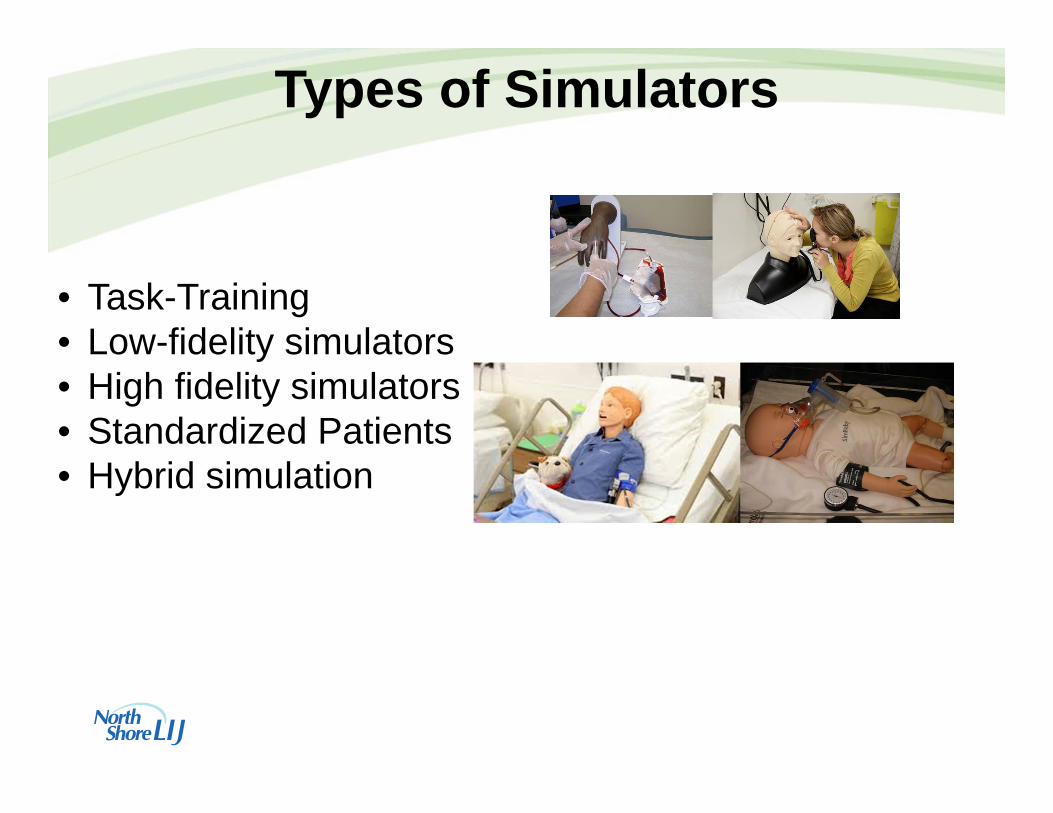
Types of Simulators
• Task-Training• Low-fidelity simulators• High fidelity simulators• Standardized Patients• Hybrid simulation

Types of Simulation
• Simulation Center (Corporate University)• In-Situ Simulation• Profession specific• Interprofessional

Types of Simulation Based Education
• Simulation Center (Corporate University)• PASS11
• PEDS Communication12
• PEDS Clinical Scenarios12
• Pediatric Critical Interventions11
• Southside Family Medicine• Recognition of Contrast Media Reactions• Responding to Sedation Emergencies for OMFS Residents• Crisis Resource Management• Orientation to Clinical Responsibility
Types of Simulation Based Education
• In-Situ Simulation• Pediatric Trauma In-situ Program• Hospital Based In-situ programs11
• Unannounced simulations in different care areas in the hospital during day and night hours every other week
• Data collection of consistent systems and equipment issues common to all resuscitation scenarios
• Assess specific systems issues that impact delivery in different clinical areas of the hospital

Simulation Approached
Positives•Captive attention of participants•Resources for planning and debriefing- Rooms, large monitors
Drawbacks•Participants who attend self-select•Teams do not assemble or function as in the clinical setting•Equipment, setting can add to the artificiality of the scenario•Reduce participant buy-in•Expensive– Dedicated non-clinical time
Simulation CenterPositives
•Capture practitioners in their normal work environment and with their usual clinical colleagues•Capture the important dynamic between care delivery systems and equipment and practitioners
Drawbacks• Potential resources pulled from
patient care• Potential for large audience• Limited time for multiple
scenarios
In-Situ Simulation
Interprofessional Simulation
‘‘occasions when two or more professions learnfrom and about each other to improve collaboration and
the quality of care9’’
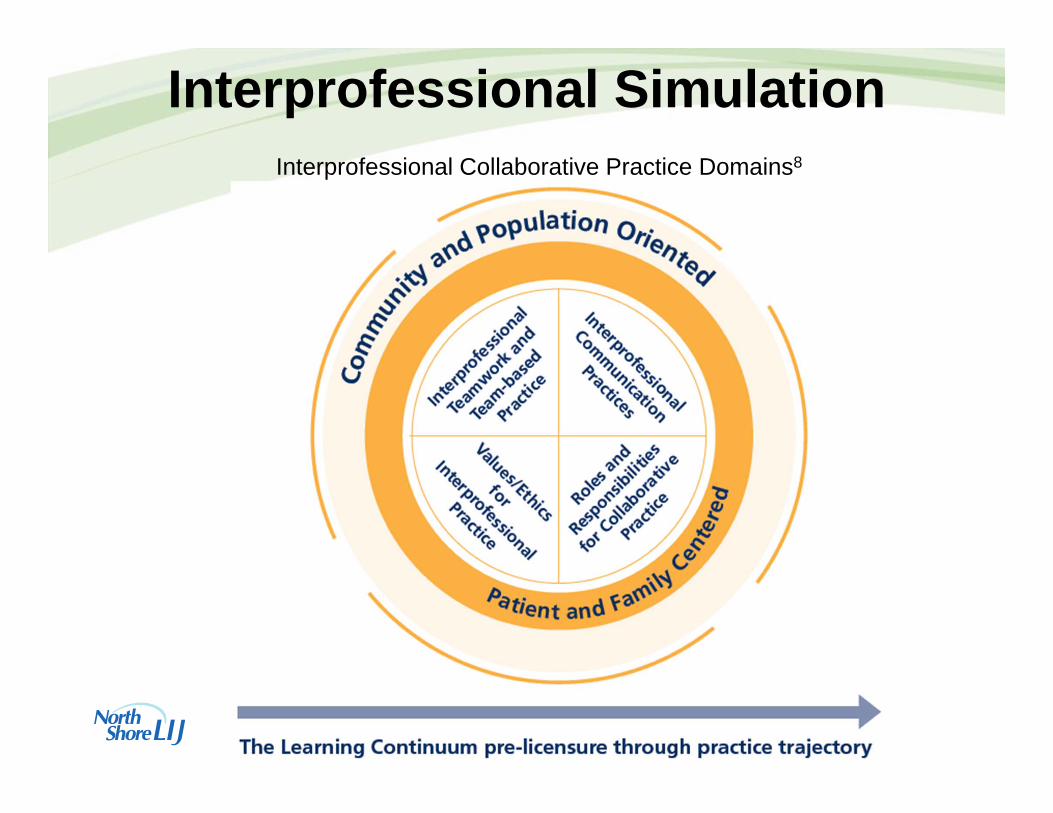
Interprofessional SimulationInterprofessional Collaborative Practice Domains8

Implications for Patient Safety
• TeamSTEPPS™• Escalation strategies
• Crisis Resource Management10
1 Know The Environment
2 Anticipate and Plan
3 Call for help early
4 Exercise leadership and followership
5 Distribute the workload
6 Mobilize all available resources
7 Communicate effectively
8 Use all available information
9 Prevent and manage fixation errors
10 Cross (double) check
11 Use cognitive aids
12 Re‐evaluate repeatedly
13 Use good teamwork
14 Allocate attention wisely
15 Set priorities dynamically
Implications for Patient Safety1. The difficulty of the simulation scenario was a good match for my level of experience.
‐”The scenarios were very familiar to my clinical setting.”
2.The debriefing session provided adequate time for discussion of key issues.‐”In‐depth, productive discussion occurred with each scenario “
3.When you reflect back on the simulation‐based program, what were the 3 most important things you learned?
‐”call for help sooner, introduce and answer parent questions, timely management ofsymptoms”
‐”Importance and effectiveness of closed‐loop communication, strategies to deal withfamily members, improving leadership skills.”
‐”The tendency for people to fixate on the easiest or most comfortable problem to solve. How important recapping and knowing the algorithms are.”
Implications for Patient Safety4. What did you learn about how you work with others in a team?
‐”reinforced communication between RNs and MDs and between RNs”
‐”I tend to let the physician take the lead, offer suggestions in a polite and calm toneand try to keep the group focused.”
‐”It is important to actively seek team member's input when there are team members whoare newer in their training/careers because they may not feelempowered to make suggestions.”

Challenges in Simulation Based Education
1. Issenberg, S. B., & Scalese, R. J. (2008). Simulation in health care education. Perspect Biol Med, 51(1), 31-46. doi: 10.1353/pbm.2008.00042. Jeffries, P. R. (2005). A framework for designing, implementing, and evaluating simulations used as teaching strategies in nursing. Nurs
Educ Perspect, 26(2), 96. 3. Motola, I., Devine, L. A., Chung, H. S., Sullivan, J. E., & Issenberg, S. B. (2013). Simulation in healthcare education: a best
evidence practical guide. AMEE Guide No. 82. Med Teach, 35(10), e1511-1530. doi: 10.3109/0142159X.2013.8186324. Alinier, Guillaume. (2011). Developing High-Fidelity Health Care Simulation Scenarios: A Guide for Educators and Professionals.
Simulation & Gaming, 42(1), 9-26. doi: 10.1177/10468781093556835. Rudolph, Jenny W, Simon, Robert, Dufresne, Ronald L, & Raemer, Daniel B. (2006). There's no such thing as “nonjudgmental”
debriefing: a theory and method for debriefing with good judgment. Simulation in Healthcare, 1(1), 49-55. 6. Hunt, E. A., Duval-Arnould, J. M., Nelson-McMillan, K. L., Bradshaw, J. H., Diener-West, M., Perretta, J. S., & Shilkofski, N. A.
(2014). Pediatric resident resuscitation skills improve after "rapid cycle deliberate practice" training. Resuscitation, 85(7), 945-951. doi: 10.1016/j.resuscitation.2014.02.025
7. Barrett, Lisa Feldman, & Russell, James A. (1999). The Structure of Current Affect: Controversies and Emerging Consensus. CURRENT DIRECTIONS IN PSYCHOLOGICAL SCIENCE 8(1), 4.
8. IPEC. (2011). Core competencies for interprofessional collaborative practice: Report of an expert panel. Washington, D.C: Interprofessional Education Collaborative.
9. Oandasan, I., & Reeves, S. (2005). Key elements for interprofessional education. Part 1: the learner, the educator and the learning context. J Interprof Care, 19 Suppl 1, 21-38. doi: 10.1080/13561820500083550
10. Howard, S. K., Gaba, D. M., Fish, K. J., Yang, G., & Sarnquist, F. H. (1992). Anesthesia crisis resource management training:teaching anesthesiologists to handle critical incidents. Aviat Space Environ Med, 63(9), 763-770.
11. Gangadharan, Sandeep, & Rotjan, Andrew. (2014). Pediatric Emergencies: Targeted Programs and Crafted Scenarios. In K. Gallo & L. G. Smith (Eds.), Building a Culture of Patient Safety through Simulation: An Interprofessional Learning Model (1 ed.). Springer Publishing Co., Inc.
12. Scott, Helen Maliagros, Perrone, John, & Drozd, Andrew. (2014). Dimensions in Pediatrics Simulation: Teamwork and Communication. In K. Gallo & L. G. Smith (Eds.), Building a Culture of Patient Safety through Simulation: An Interprofessional Learning Model (1 ed.): Springer Publishing Co., Inc.
References






![ASCR WORKSHOP Priority Research Directions …tpeterka/talks/2019/peterka-works19-talk.pdfStacks. In Situ Yesterday 8 [Zajac, 1964] Simulation Visualization Simulation Visualization.](https://static.documents.pub/doc/80x56/5ed0f2ee2a742537f26e9f82/ascr-workshop-priority-research-directions-tpeterkatalks2019peterka-works19-talkpdf.jpg)










