IN THE NAME OF GOD EVALUATION AND TREATMENT OF FECAL INCOTINENCY IN CHIDREN Ahmad Khaleghnejad Tabari MD Pediatric Surgery Research Center, Mofid Chidren’s Hospital Shaheed Beheshti University of Medeical Sciences Tehran, Iran Second annual meeting of Iranian Continence Society, June 2011
Transcript
IN THE NAME OF GOD
EVALUATION AND TREATMENT OF FECAL INCOTINENCY IN CHIDREN
Ahmad Khaleghnejad Tabari MDPediatric Surgery Research Center, Mofid Chidren’s Hospital
Shaheed Beheshti University of Medeical Sciences Tehran, Iran
Second annual meeting of Iranian Continence Society, June 2011
Etiology
Three major cause:1-Congenital Anomalies2-Mental Retardation3-Childhood Encopresis
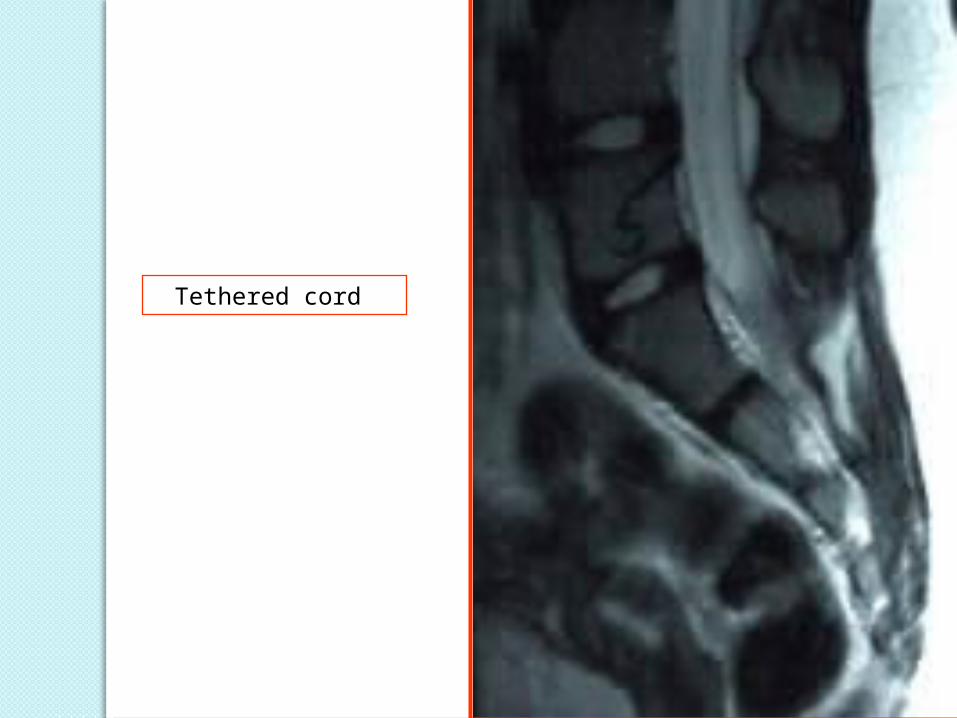
Congenital Anomalies1- Myelomeningocele2- Tethered cord3- Lipomeningocele4- High anorectal atresia
(deficiencies of pelvic musculature and innervation )
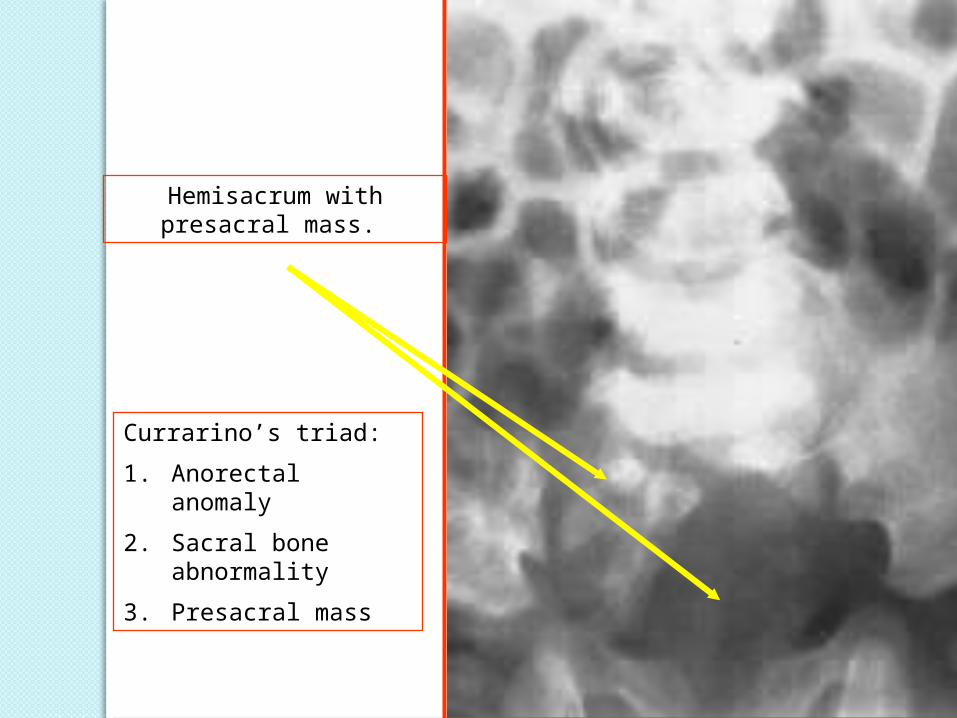
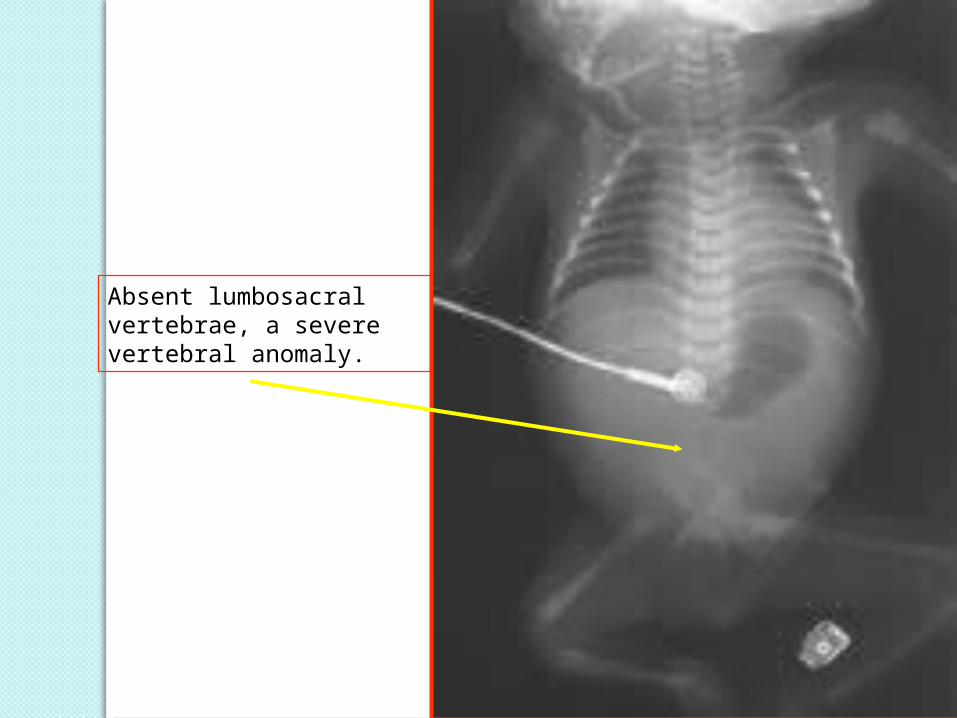
5- Three to five sacral missing
Acquired causes1- Encopresis ( chronic
constipation )2- Trauma to the sacrum and
spinal cord3- Anal sphincter destruction by
systemic disease (Crohn’s disease, severe proctitis, extensive anorectal infection)
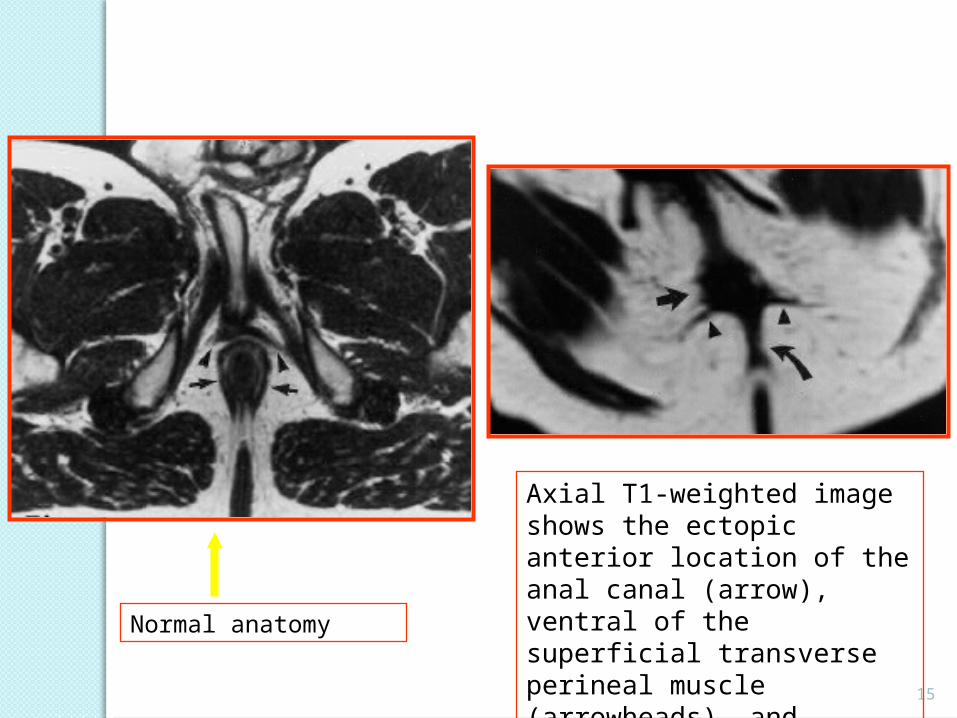
Axial T1-weighted image shows the ectopic anterior location of the anal canal (arrow), ventral of the superficial transverse perineal muscle (arrowheads), and outside the normally developed external anal sphincter (curved arrow)
Normal anatomy
16
Unsuccessful repair
PR-sling incomplete
17
Axial SE T1-weighted image in a boy, afterreconstructive surgery for a high anorectal malformation. Theneorectum (black arrow) is positioned outside and to the right ofa normally developed external anal sphincter (white arrow)
2- Defecography ( rectoanal angle, completeness of emptying and descent of the pelvic floor one cm below the pubococcygeal line)
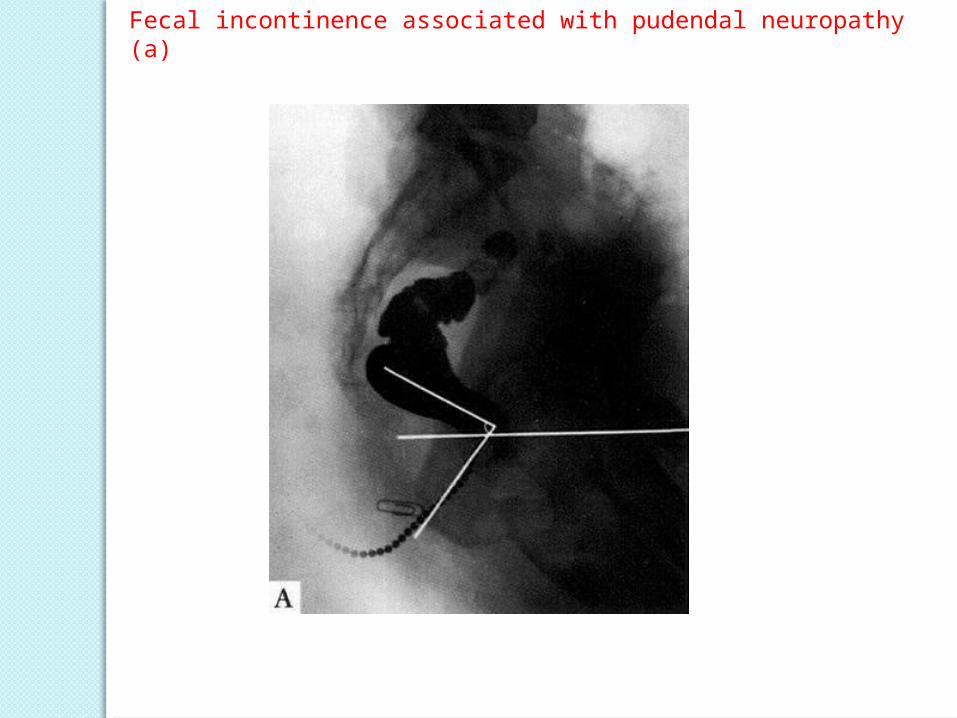
Fecal incontinence associated with pudendal neuropathy (a)
Fecal incontinence associated with pudendal neuropathy (b)
Fecal incontinence associated with pudendal neuropathy (c)
Fecal incontinence associated with pudendal neuropathy (d)
TREATMENT
Three approaches to treatment of incontinence :
1- Control of stool consistency
2- Conditioning or Biofeedback therapy
3- Operation to strengthen the sphincter muscles
TREATMENTBOWEL MANAGEMENT PROGRAMM
Treatment in neurologic deficiency:( myelominingocele, spinal malformations
and variant of high imperforate anus )1- Dietary and pharmacologic manipulation
to thicken the stool2- Regular emptying of the rectum each
morning with glycerin suppositories, saline enema or Bisacodyl suppositories within 30 minutes of a meal
3- Malone appendicocecostomy or sigmoidostomy tube for antegrade enema
TREATMENTBiofeedback
Biofeedback therapy play a role in patients with decreased sphincter function
1- A rectal balloon manometry device is placed into the rectum
2- The rectal and sphincter pressures are shown to the patient
3- The rectal balloon is inflated and the patient is encouraged to contract the external sphincter in response
4- The sensation of rectal distention and external sphincter contraction is learned which may enhance continence
TREATMENTEncopresisIn patients with encopresis associated with chronic
constipation, incontinence is relieved when constipation is alleviated
1- Initial evacuation of stool by aggressive enema program, disimpaction in operating room, rectal water soluble contrast administration under fluoroscopy guidance
2- Administration of stool softeners, mineral oil, polyethylene glycol
3- Biofeedback therapy in pshycogenic incontinence4- Malone appendicocecostomy or sigmoidostomy
tube for antegrade enema5- Resection of megasigmoid
Malone Appendicostomy
Megarectosigmoid in contrast enema
Resection of megarectosigmoid
TREATMENT OF INCONTINENCE AFTER ANORECTAL MAIFORMATION OPERATIONS
Incontinence after repair with normal sacrum and appropriately positioned and functioning sphincter muscle, dietary manipulation and regular evacuation of rectum ( saline enema , Malone )
The rectum positioned inappropiately outside the levator of external sphincter muscles on PE, MRI, endosono and electromyographic localization, remedial operative correction via PSA is indicated
34
Axial SE T1-weighted image in a boy, afterreconstructive surgery for a high anorectal malformation. Theneorectum (black arrow) is positioned outside and to the right ofa normally developed external anal sphincter (white arrow)
TREATMENT OF INCONTINENCE AFTER ANORECTAL MAIFORMATION OPERATIONS
Surgical transplantation of one or two gracilis muscles arround the external sphincter, stimulation with special devices
prianal autologous fat injection may enhance continence
Artificial anal sphincter devices Stem cell implantation for muscle