Increasing Old Fashioned Caring from the Nurse: Perioperative Services and Perinatal Bereavement Anita Catlin, DNSc, FNP, CNL, FAAN Kaiser Santa Rosa ELNEC Certified Resolve Through Sharing Certified 1
Transcript
Increasing Old Fashioned Caring
from the Nurse: Perioperative Services and
Perinatal Bereavement
Anita Catlin, DNSc, FNP, CNL, FAAN Kaiser Santa Rosa ELNEC Certified
Resolve Through Sharing Certified
1
CLINICAL CARITAS –
Watson Caring Theory Be authentically present
Cultivate one's own transpersonal self
Center Oneself
Respect Human Dignity
Develop and sustain a helping, trusting, authentic caring relationship
“Be With”
Presence
2
EVIDENCE BASED PRACTICE GOAL: Use evidence to solve problem in practice PROBLEM: 1. Nurses conscientiously objecting to caring for pregnancy loss in
secular hospital perioperative services- OR, PACU; including fetal demise, miscarriage, and pregnancy terminations
2. Patients unable to be cared for in own system, being outsourced and wait listed
3. No bereavement support being offered in perioperative services METHOD: Review of evidence from national and state governing documents for nursing practice SOLUTION: Educational sessions throughout Perioperative Services RESULTS: Nurses able to make more thoughtful, evidence based decisions, resulting in improved care delivery to patients
3
EVIDENCE NEEDED
• Assist nurses in framing what duties are owed to patients using the ANA Social Contract and the ANA Code of Ethics,
• Apply definitions of duty from the professional organizations for operating room and perianesthesia organizations, AORN and ASPAN
• Define conscientious objection in nursing and outline policy to use it
• Apply BRN definition of Patient Abandonment
4
END GOAL
• Provide bereavement support to those patients whose desired pregnancy is ended due to genetic anomaly or life limiting illness of fetus
• Provide bereavement support to those patients whose desired pregnancy is ended due to maternal illness not compatible with pregnancy
• Provide bereavement support to women experiencing a fetal demise whose deceased products of conception need to be removed surgically.
• Allow conscientious objection to be used properly • Increase number of nurses willing to give pre and post
operative care to women in surgery to remove products of conception
5
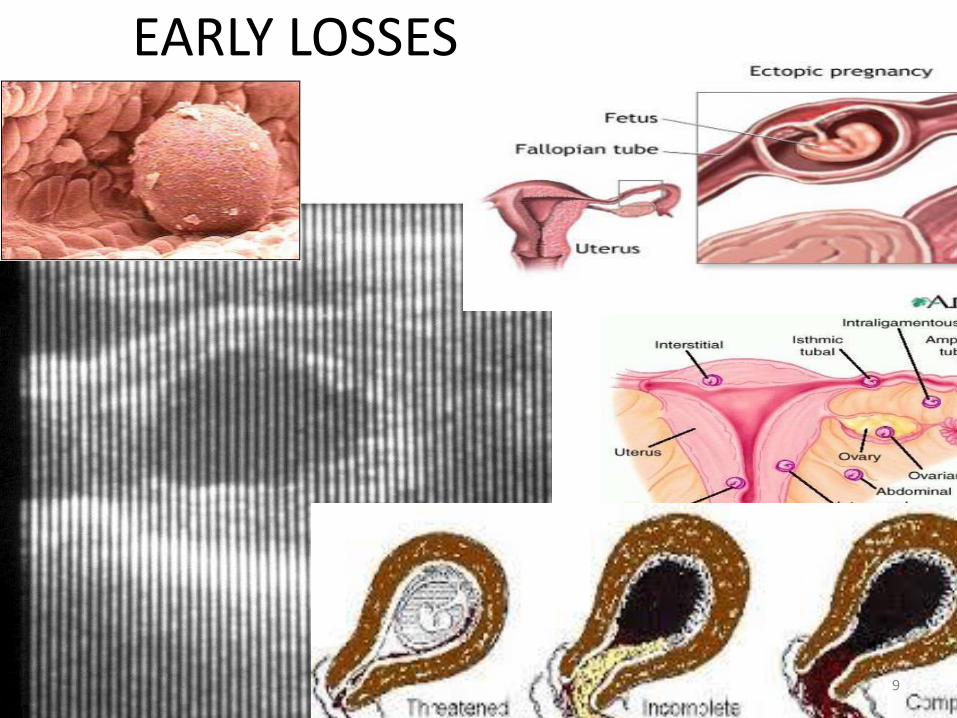
MANY TYPES OF PERINATAL LOSS • Blighted Ovum
• Miscarriage (Complete, Incomplete)
• Ectopic
• In Utero Demise (Under & over 20 weeks)
• Assisted Reproduction and Multiples
• Stillbirth
• NICU or Home with Hospice
• Pregnancy Interruption (Medical/Social)
• Giving baby up for adoption
• Safe Haven
• SIDS
• Infertility
LOSS of DREAM
6
MANY PEOPLE AFFECTED • Married Couple
• Single Woman/Baby Daddy
• Single Woman with Assisted Reproduction
• Same Sex Couple
• Surrogate Adopters
• Teen Pregnancy
WHOMEVER IS AFFECTED, THIS MAY ALSO INCLUDE
• Extended Family
• Other Children
• Staff
7
LOSSES
8
When I’m a mother, a father, a parent…….
EARLY LOSSES
EARLY LOSSES 9
USE OF TERMS MOTHER AND BABY
75% of families losing an early pregnancy referred to the woman as the ‘mother’ and the products of conception as a ‘baby’ Limbo & Wheeler, 1986, Limbo & Kobler, 2010,
Linda Layne “Motherhood Lost” 2003 He was a Real Baby; He is Worthy of Memory; He had Things
10
ATTACHMENT
(Cole, 2010) Artwork and book by Stephanie Cole
11
TASKS OF PARENTING
Live Child
• Protecting
• Attaching
• Introducing
• Sharing Culture
• Sharing Family History
When a (Desired) Pregnancy is Lost or there is an Upcoming Loss
• Validation • See Sonogram Pictures • View, Honor, Hold Products of
Conception • Have Him as Long as Possible • Name Baby • Legitimize His Life • Create Time Together • Introducing • Create Memories • Respond within Culture
12
LOOKING AT THE MEDICAL RECORD • G6, P1, A5
• G4, P2, A2
• People are very sensitive to the word abortion, specially when they have had a miscarriage and it is referred to as a spontaneous abortion in front of them
• How they were treated (by nurses, the ED, the clinics, the hospital) with loss will impact all future pregnancies immensely (D. Cote-Arsenaut)
13
PRIOR TO 20 WEEKS
• Seen in Emergency Department • Seen in Clinics • Seen in OR • Still need Memory Making • Still need Support • Still May Need Aftercare and Counseling
AFTER 20 WEEKS • In Maternal Child Department
14
THE FETUS • When we are aware that a pregnancy/fetus is in danger
– Options are offered – Now many are offering delivery and palliative care as option
• Go to medical center that believes in fixing/repairing/replacing
• Decide to interrupt pregnancy • Have early induction to allow for short period of
bonding after birth • Continue pregnancy with special birth plan and
provision of palliative care at birth • Deliver and go home with hospice or George Mark
Children’s House https://www.youtube.com/watch?v=50NEmnEUtY0
EARLY INDUCTION • Not considered pregnancy termination by the
church
• With this decision, no monitoring or resuscitating
• Baby may take some breaths, can be baptized and blessed
• Culturally very important
– Example: Muslim infant must take a breathe to be buried in cemetery
• Mother can hold a dressed and swaddled baby
16
17
PREGNANCY INTERRUPTION • May be indicated to save mother’s life
– Lupus
– Sickle Cell
– Hypertension
– Fast growing malignancy
– High order multiples (Selective Reduction)
– Fetus has died in utero
– These women and families may have desperately wanted that dreamed for child and deserve respectful bereavement care
18
PREGNANCY INTERRUPTION
May be after a very difficult decision not to parent this particular pregnancy • Rape or Incest • Trisomies • Anencephalies • Absent kidneys • (May most be objected to) A social, cultural or
developmental decision
• These women and families, too, may have desperately wanted that dreamed for child and deserve respectful bereavement care
19
BALANCE BETWEEN NURSE’S OWN NEEDS AND BELIEFS
AND PATIENT’S NEEDS
• There are times nurse may desire not to participate
• Sources of Information:
– ANA Code of Ethics
– AORN Code of Ethics
– Perianesthesia Standards 2015-2017
– CNA Contract
20
Nurse may object
• Nurse does not have to scrub or circulate during a pregnancy termination if finds this morally unacceptable
• Important to notify supervisor in writing
• If there is a medical emergency, nurse may have to step in to save a life until relief can be found
21
IMPORTANT TO DIFFERENTIATE • In a pregnancy termination, the fetus comes to the operating
room with a heartbeat. This is a procedure you can object to. In ectopic there may be a heartbeat but not a viable fetus.
• In fetal demise, miscarriage, or molar pregnancy, there is no live fetus. The uterus is evacuated to safeguard the woman’s life from excessive hemorrhage or disseminated intravascular coagulation (DIC) which can occur—At times this may be emergent. This is not a condition to conscientiously object to as it is only the mother’s life which is involved.
22
A AMERICAN NURSES ASSOCIATION
• ANA Code of Ethics: “The nurse, in all professional relationships, practices with compassion and respect for the inherent dignity, worth, and uniqueness of every individual, unrestricted by considerations of social or economic status, personal attributes, or the nature of health problems. “
• ANA: Supports right to all forms of women’s health care delivery and contraception care
23
ANA CODE OF ETHICS • The nurse safeguards patient autonomy
• The nurse cares for all patients in his or her care, regardless of gender, age, ethnicity, condition, decisions……..
• The nurse may object, and this objection is to be respected, to participation in certain procedures or forms of therapy, but never to a specific patient under care
• Conscientious objection is allowable when the procedure is one that causes the nurse moral distress
• A common example is when the nurse in the maternal child unit says “I will provide care and comfort for this baby, and all ordered therapies, but I will not participate in the one therapeutic order to assist in a circumcision. I can give Tylenol before and provide sugar pacifier after.”
24
SPE CODE OF ETHICS, SECTION 5.4
• “Moral objections cannot be based on personal preference, prejudice, bias, convenience, or arbitrariness”
• Must be a sincere and longstanding moral objection to a specific nursing action
• Example: May choose not to participate in actual circumcision if another nurse is available and willing; however, still care for infant prior to and after procedure as would care for any other patient
25
AORN
• “In order to provide care that is culturally relevant to a diverse patient population, it is vital that nurses recognize the importance of each patient’s values, beliefs, and health practices… It is an ethical imperative for the nurse to provide nursing care respecting the patient’s worth and dignity regardless of diagnosis, disease process, procedure, or projected outcome.” p. 713-714.
26
ASPAN
• “The perianesthesia nurse provides care to each patient while preserving human dignity, autonomy, confidentiality, protecting patient rights, and ..provides quality care to all patients regardless of race, religion, gender, age, disability, socioeconomic status, sexual orientation, gender identification and care decisions.” p.11
27
ASPAN
• Personal convictions allow the nurse to remove her/himself from a patient care situation, as long as:
• Such removal does not harm the patient
• Does not constitute a breach of duty
• The manager knows in advance and can plan
However, if no other registered nurse is available, the objecting nurse must ensure care needs are met p.11
28
SAMPLE CONTRACT
• “The rights of the patient to receive necessary nursing care …must be recognized and respected. In the case of therapeutic abortions, the nursing profession accepts the obligation of providing competent nursing care as a major responsibility;
• The facility agrees that a nurse may, except in an emergency situation where the patient’s needs will not allow for a personnel substitution, refuse to participate in therapeutic abortion procedures.
• In writing to Director…consider whether or not to transfer to another area
• In emergency, patient’s needs that precedence over nurse’s rights, but attempt at substitution should be at earliest possible opportunity.
Article XXI-P73 2101-2103 29
OTHER GROUPS • American Medical Association Code of Ethics • 1887-2005
– “Physicians may choose their patients and to whom they provide care,”
• 2005-2016 – After Katrina added “Unless in the case of epidemic or national
emergency.”
• July 2016-Draft Care for patients, unless – No resources – Against conscious – Invalid, non beneficial care – Can’t care for others – Abusive
• CRNA May choose whom to administer anesthesia to 30
CONSCIENTIOUS OBJECTION
• Came from soldiers objecting
to particular activities of war
• Often religion based
• Pattern of principles
• Catlin and colleagues studied
conscientious objection in
nurses in PICUs and NICUs
• Reviewed literature
• Antecedents, Consequences,
Cases
CONSCIENTIOUS OBJECTION
• “For the nurse, conscientious objection may occur when the nurse interprets that the specific treatment that has been ordered for a patient is harmful or causing suffering. The nurse does not wish to provide this form of therapy and feels sincerely and has felt for some time that this situation warrants a conscientious objection.
• The nurse objects to the nature of the orders for treatment, willing to assist in other forms of treatment and not wishing to abandon the patient.”
• Catlin, 2007
32
RELIGIOUS versus SECULAR HOSPITAL • Religious hospital guided by tenets of faith, such as
Orders of Bishops for Catholic Health Care
– Faith determines whether birth control, sterilizations, or terminations are offered
• Secular- Best health care to community at low cost
– All reproductive services provided
• Respect for Mission and Vision
– Best to match one’s own goals with hospital goals
33
RECENT SUGGESTIONS DURING and AFTER PROCEDURE
• Ask what event means to the woman • Allow mother to visualize products of conception • Dispose of remains as medical waste only with parents
permission • Call OB to obtain memory box , memento making • Over 20 weeks, NOW I LAY ME DOWN TO SLEEP;
photography • Offer chaplain’s blessing • If desired pregnancy, say: “I understand you were
pregnant. I am sorry for your loss.” • Regardless of situation, may have been a really horrible
experience; They will remember your care all of their lives 34
YOUR PEERS
• Supporting one another regardless of beliefs is essential
• Not judging one another’s decisions
• Bravery either way
35
PATIENT ABANDONMENT per CA BRN
• For patient abandonment to occur, the nurse must: – a) Accept the patient assignment, thus establishing a
nurse-patient relationship, and then
– b) Sever that nurse-patient relationship without giving reasonable notice to the appropriate person (e.g., supervisor, patient) so that arrangements can be made for continuation of nursing care by others.
• Not abandonment: – Failure to notify the employing agency
that the nurse will not appear to work an assigned shift
– Refusal to accept an assignment
– Refusal to work additional hours or shifts would not be considered patient abandonment by the BRN.
36
MATERNAL NEEDS • Normal post partum needs
• May ask if she wishes to donate milk to Mother’s Milk Bank 408-998-4550 Milk can be shipped from her home
• Medications, peripads
• Follow up Appointment
• Phone number to call if overwhelmed
• Does patient need help with telling longer others she is no longer pregnant; how will she do this?
37
FOR NURSES: QUESTIONS TO ASK YOURSELF • Is this an instance in which saving the mother’s life
is at stake?
• Is the fetus already dead or incapable of life outside of the uterus?
• Can I reframe this to supporting a dignified end of a very wanted child for the family?
• Can I provide supportive bereavement care before and after, without participation in the procedure?
• Can I realize that the only kindness the patient may receive may be from me?