n beginning practice in 1981 the tech-nique used by the author involved placing
he brackets on working models with toffee. Theransfer trays were then made from siliconeutty, and the adhesive was a two-paste compos-
te resin. A problem with this technique involvedhe possibility of adhesive flash remaininground the base of the brackets, which requiredemoval with a round bur and a hand piece.nother problem involved the requirement ofaiting long enough for the adhesive to gainnough bond strength to allow tray removal.
With the advent of lingual orthodontics camehe custom base indirect bonding technique.he brackets were placed on the model with aeat-cured composite resin and the flash re-oved. After the bracket position was adjusted,
he model was placed in an oven to cure theesin.
After the tray was made and the model waslaced in warm water to dissolve the separatingedium and release the brackets from theodel, the cured composite resin had formed a
From the private practice of Dr. Duncan W. Higgins, Deltarthodontic Group, British Columbia, Canada.
Address correspondence to Duncan W. Higgins, DDS, MSD,RCD(C), #203, 7313 120 Street, Delta, BC, Canada V4C 6P5.hone: 604-590-1172.
ustom base on the brackets. This custom baseould adapt so closely to the tooth that it wasnly necessary to use a thin film of self-curedomposite resin to act as the adhesive betweenhe custom base resin and the etched enamel.nitially, Concise (3M Unitek, Monrovia, CA)estorative unfilled enamel sealant was used ashe adhesive. Some clinicians preferred to sim-ly place part A of the sealant on the customase and part B on the enamel. When the trayas placed on the prepared teeth, the two partsould meet and cure. This became known as theA-B custom base” technique.
Specific indirect bonding adhesives were de-eloped for the A-B technique. Improvementsncluded adding fillers for increased viscositynd bond strength, as well as adding acceler-tors to decrease the setting time and to de-rease the time the trays had to be held inlace before they could be removed from theonded brackets.
At approximately the same time that light-ured restorative composite resins were intro-uced, orthodontists began experimentingith clear transfer trays. These trays are made
n the same manner that mouth guards areade on the Biostar® (Great Lakes Orthodon-
ics, Tonawanda, NY). The clear trays allowedhe use of light-cured, nonfilled resins to besed as an adhesive. The main advantage of these of light-cured adhesives versus chemicallyured adhesives was the relatively high initial
ond strength present at the critical time of tray
o 1 (March), 2007: pp 64-68
rwwtht
cob
DfitTSaHtiv
w
Fv
F
65Mouth Guard Transfer Tray
emoval. Another advantage was the increasedorking time available to ensure that the trayas fully seated. Subsequently, the “double tray
echnique” was introduced, which used an outerard acrylic tray in addition to the soft inner
ray. This increased stability in the tray system.The next step in the evolution of this pro-
ess involved adding a filler to the resin inrder to increase the viscosity, as well as theond strength. Fluorobond™ (Ormco, Sybron
igure 2. Micro-etching of the custom bases. (Color
ersion of figure is available online.) a
ental Specialties, Orange, CA) was a lightlylled, light-cured orthodontic sealant used by
he author as an indirect bonding adhesive.his was replaced by Ortho Solo™ (Ormco,ybron Dental Specialties, Orange, CA) whichdded some moisture tolerance to the system.alogen lights became stronger, and curing
imes decreased. When the argon laser wasntroduced, it decreased curing time and pro-ided a smaller and lighter wand. The use of
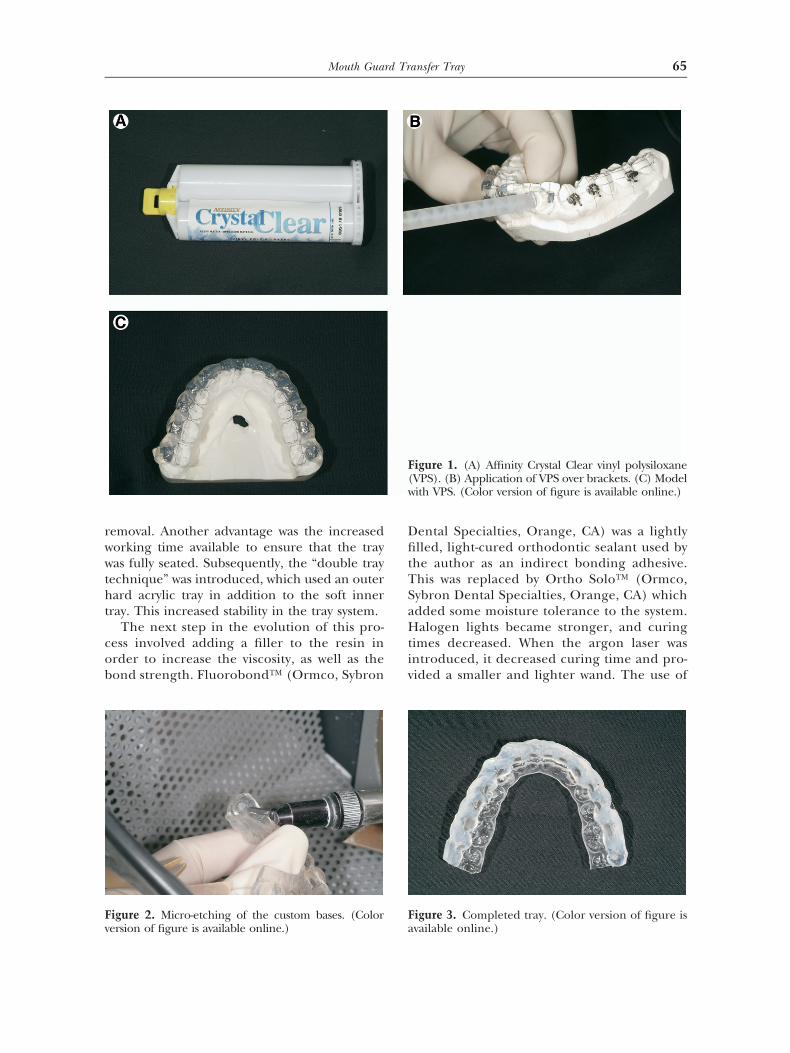
igure 1. (A) Affinity Crystal Clear vinyl polysiloxaneVPS). (B) Application of VPS over brackets. (C) Modelith VPS. (Color version of figure is available online.)
igure 3. Completed tray. (Color version of figure is
F(
vailable online.)
aa
(rabvopwnco
L
TcUpa
1
2
3
4
FFl
F
66 D.W. Higgins
n argon laser also decreases enamel deminer-lization.1
Filtek™ Supreme Plus Flowable Restorative3M ESPE, St. Paul, MN) acts as an intermediaryesin in our indirect bonding process. The use of
flowable light-cured adhesive with indirectonding was first described by Miles.2 Filtek isiscous enough so that it stays where it is placedn the custom base; however, it flows under theressure of seating the tray down to 10 microns,hich is considered an ideal cement line thick-ess. Very little flash is present after bonding, ifare is taken to place a minimal amount of Filtekn the custom base.
aboratory Technique
he indirect bonding technique combining alear double transfer tray with an APC™ II (3Mnitek, Monrovia, CA) custom base has beenreviously described by Sondhi.3 The followingre the modifications that the author has made:
. Use a resin-reinforced model stone such asGC Fujirock® EP (GC America Inc., Alsip,IL).
. Use a separating medium and place thebrackets on the models. A technique for pre-cision bracket placement using marginalridges, and functional and esthetic surfaces asa reference point, has been previously de-scribed by Kalange.4
. Cure the custom base resin in a Triad 2000™
Visible Light Curing Unit (Dentsply Interna-tional, York, PA) for 10 minutes from the
igure 4. Isolation and etching using the Nola Dryield System. (Color version of figure is available on-
ine.)
occlusal and 10 minutes from the gingival. o
. Lay down a bead of Affinity™ Crystal Cleartransparent vinyl polysiloxane or VPS (Clini-cians Choice, Inc., New Milford, CT) to capturethe brackets (Fig 1A-C). Use a small, yellow (4.2mm) mixing tip. The bead should be approxi-mately the diameter of a pencil so that it can beremoved in one piece in the mouth. Hold themixing tip at a 45 degree angle to the bracket
igure 5. (A) Dry Tips. (B) Dri-Angle. (Color version
f figure is available online.)
5
6
7
89
1
C
1
2
3
4
5
6789
Fu
Fl
Ffi
67Mouth Guard Transfer Tray
face. Keep the VPS flowing ahead of the tip tosurround the brackets.
. Using a Biostar® machine (Great Lakes Orth-odontics, Tonawanda, NY) and 0.5 mm clearSplint Biocryl (Great Lakes Orthodontics,Tonawanda, NY; item #021-023) make anouter tray over the VPS using the lead pellettechnique.
. Soak the working model with the customtransfer tray in warm water for a minimum ofone hour to dissolve the separating medium,and release the custom bases from the model.Remove the tray from the model in onepiece. Do not separate the VPS from theouter tray.
. Return the tray to the curing unit for oneminute to cure any “soft spots”.
. Trim the tray with scissors or a scalpel.
. Micro-etch the custom bases with Ortho Pro-phyTM SA-85 abrasive (Danville Engineering,San Ramon, CA). This will clean the custom
igure 6. Application of Filtek. (Color version of fig-re is available online.)
igure 7. Curing of the composite with an argon
aser. (Color version of figure is available online.)
bases without removing a significant amountof the resin (Fig 2).
0. Rinse the tray well to remove all abrasive.Shake off the excess water and allow to airdry (Fig 3).
linical Procedure
. Apply the smallest amount of Filtek that willcover the custom base of each bracket, andspread the adhesive with the end of the sy-ringe (Fig 6). Place the trays in the dark.
. Isolate the oral cavity using a Nola Dry FieldSystem (Great Lakes Orthodontics,Tonawanda, NY) (Fig 4). Use Dry Tips®
(Molnlyke Health Care, Goteborg, Sweden)for maximum moisture control or the morerigid Dry Angles (Dental Health Products,Inc., Youngstown, NY) to hold the cheek awayfrom the second molars (Fig 5A and B).
. Etch the facial surface of all teeth to bebonded on one arch, rinse well, and dry witha tooth dryer.
. Apply a thin layer of Ortho Solo to the etchedenamel.
. Seat the tray and cure each tooth for 10 sec-onds with either a high intensity halogen orLED curing light or 5 to 10 seconds with anargon laser (Fig 7).
. Repeat the procedure for the opposite arch.
. Remove the outer trays.
. Remove the VPS.
. Remove any interproximal adhesive flash. The
igure 8. Removal of the outer tray. (Color version ofgure is available online.)
patient is now ready for archwire placement.
S
Imiedttspc
ol
R1
2
3
4Fu
Ffi
68 D.W. Higgins
ummary
ndirect bonding has undergone many improve-ents since its introduction in the 1970s and the
nterest in this technique has increased; how-ver, it does not enjoy the popularity that iteserves. Opponents of the technique equate
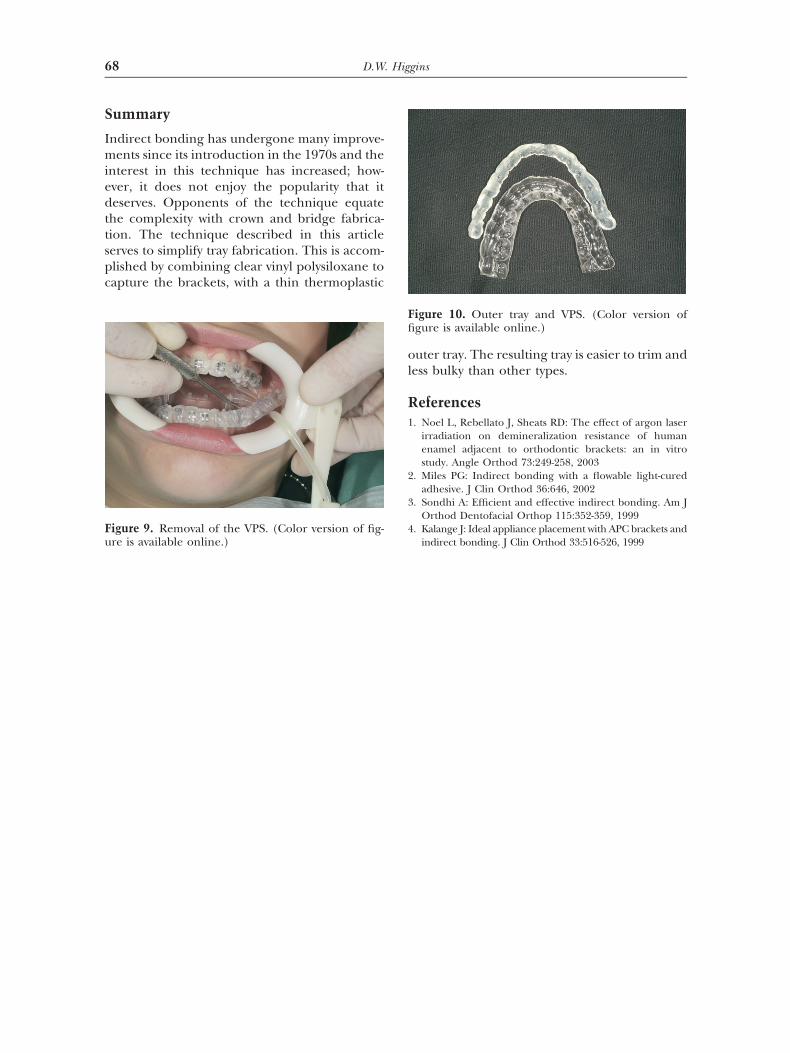
he complexity with crown and bridge fabrica-ion. The technique described in this articleerves to simplify tray fabrication. This is accom-lished by combining clear vinyl polysiloxane toapture the brackets, with a thin thermoplastic
igure 9. Removal of the VPS. (Color version of fig-
re is available online.)
uter tray. The resulting tray is easier to trim andess bulky than other types.
eferences. Noel L, Rebellato J, Sheats RD: The effect of argon laser
irradiation on demineralization resistance of humanenamel adjacent to orthodontic brackets: an in vitrostudy. Angle Orthod 73:249-258, 2003
. Miles PG: Indirect bonding with a flowable light-curedadhesive. J Clin Orthod 36:646, 2002
. Sondhi A: Efficient and effective indirect bonding. Am JOrthod Dentofacial Orthop 115:352-359, 1999
. Kalange J: Ideal appliance placement with APC brackets and
igure 10. Outer tray and VPS. (Color version ofgure is available online.)