GT/BME/UNIT-I/1 Bio-Medical Engineering (UNIT-I) Introduction: Biomedical Engineering: It is the application of Engineering principles (electronics, electrical, computer, mechanical and others) to medicine and biology for the health care complications (Diagnostic, monitoring, supporting and therapeutic). It is multidisplinary branch of Engineering, which contains many areas as follows 1. Medical Instrumentation 2. Signal and Image processing 3. Biomaterials 4. Biotelemetry 5. Medical Informatics Age of biomedical Engineering: Age refers to long and distinct period of history (era) of biomedical engineering, similarly age of automobile and radio communication. After the World War II (1939-45) nuclear, aerospace engineering reached its peak activity and settled down but at this era computer science has been rapidly growing and biomedical engineering started its origin or significance. In 1970 will be well known decade in which most of the rapid progress was made in this highly important filed. There is one vital advantage that biomedical engineering has over many of other fields that preceded it. Bioengineering subdivides into different areas for example, bioelectronics and mechanics. These are categories usually indicate the use of that area of engineering applied to living committees have been formed to define these terms , IEEE engineering in medicine and biology group, the ASME biomechanical and human factor division and the instrument society of America. One of the societies that emerged in the interface area is the association for advancement of medical instrumentation (AAMI). It consists of both engineers and physicians. Engineers are divided into clinical engineers and medical engineers. Clinical engineer who brings to health care facilities a level of education, experience and effectively and safely manage the medical devices. Medical engineer, who theory of operation, underlying physiological principles and practical, safe clinical application of biomedical equipment. His capabilities include installation, calibration, inspection, preventive maintenance and repair of general biomedical devices.
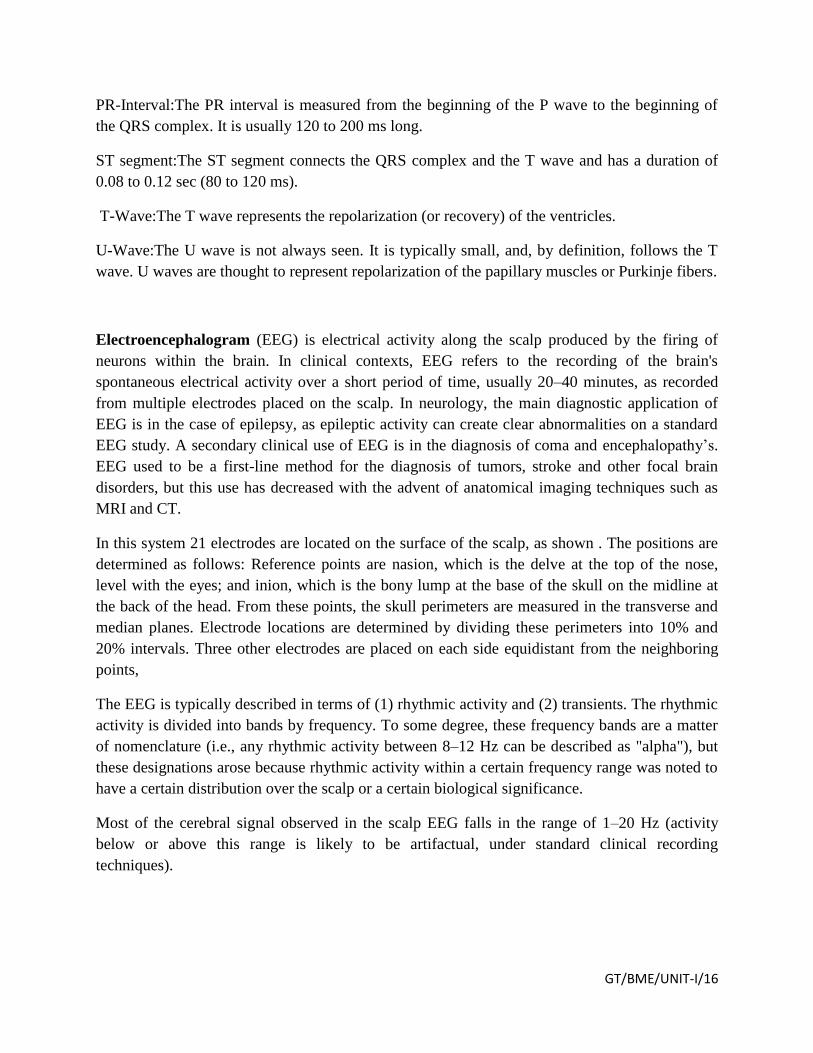
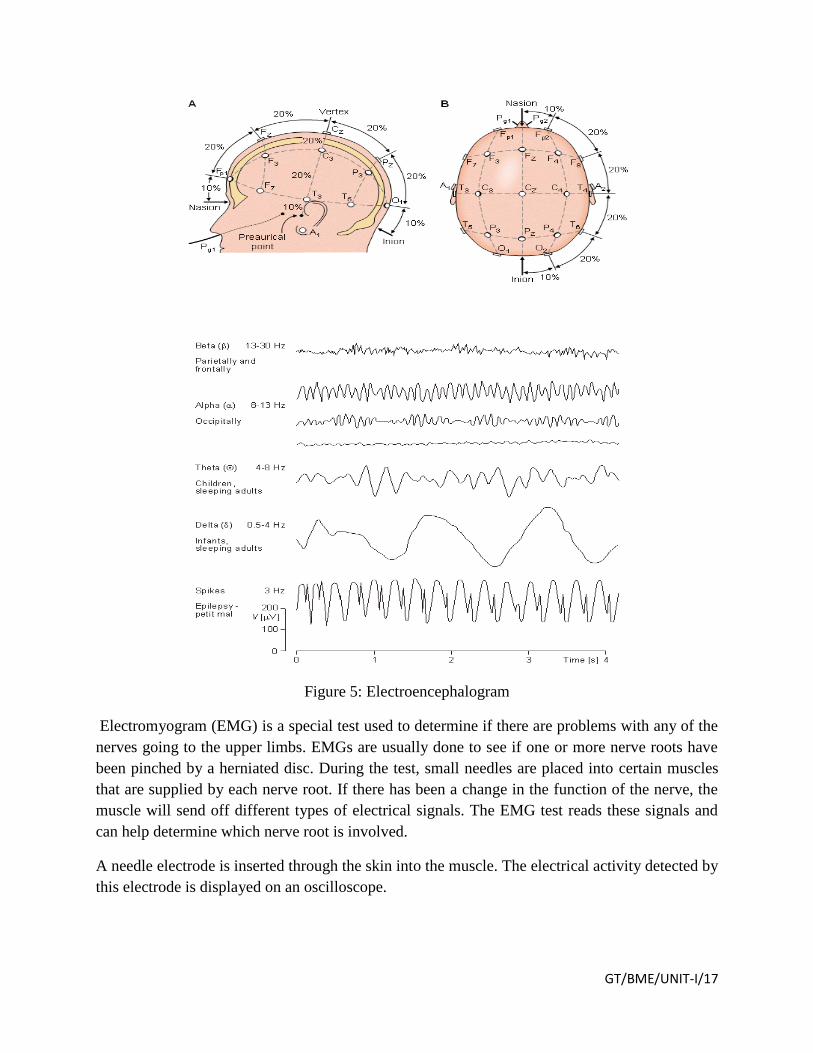
Transcript
GT/BME/UNIT-I/1
Bio-Medical Engineering (UNIT-I)
Introduction:
Biomedical Engineering: It is the application of Engineering principles (electronics, electrical,
computer, mechanical and others) to medicine and biology for the health care complications
(Diagnostic, monitoring, supporting and therapeutic).
It is multidisplinary branch of Engineering, which contains many areas as follows
1. Medical Instrumentation
2. Signal and Image processing
3. Biomaterials
4. Biotelemetry
5. Medical Informatics
Age of biomedical Engineering:
Age refers to long and distinct period of history (era) of biomedical engineering, similarly age
of automobile and radio communication. After the World War II (1939-45) nuclear, aerospace
engineering reached its peak activity and settled down but at this era computer science has been
rapidly growing and biomedical engineering started its origin or significance.
In 1970 will be well known decade in which most of the rapid progress was made in this highly
important filed. There is one vital advantage that biomedical engineering has over many of
other fields that preceded it. Bioengineering subdivides into different areas for example,
bioelectronics and mechanics. These are categories usually indicate the use of that area of
engineering applied to living committees have been formed to define these terms , IEEE
engineering in medicine and biology group, the ASME biomechanical and human factor division
and the instrument society of America.
One of the societies that emerged in the interface area is the association for advancement of
medical instrumentation (AAMI). It consists of both engineers and physicians. Engineers are
divided into clinical engineers and medical engineers. Clinical engineer who brings to health care
facilities a level of education, experience and effectively and safely manage the medical devices.
Medical engineer, who theory of operation, underlying physiological principles and practical,
safe clinical application of biomedical equipment. His capabilities include installation,
calibration, inspection, preventive maintenance and repair of general biomedical devices.
GT/BME/UNIT-I/2
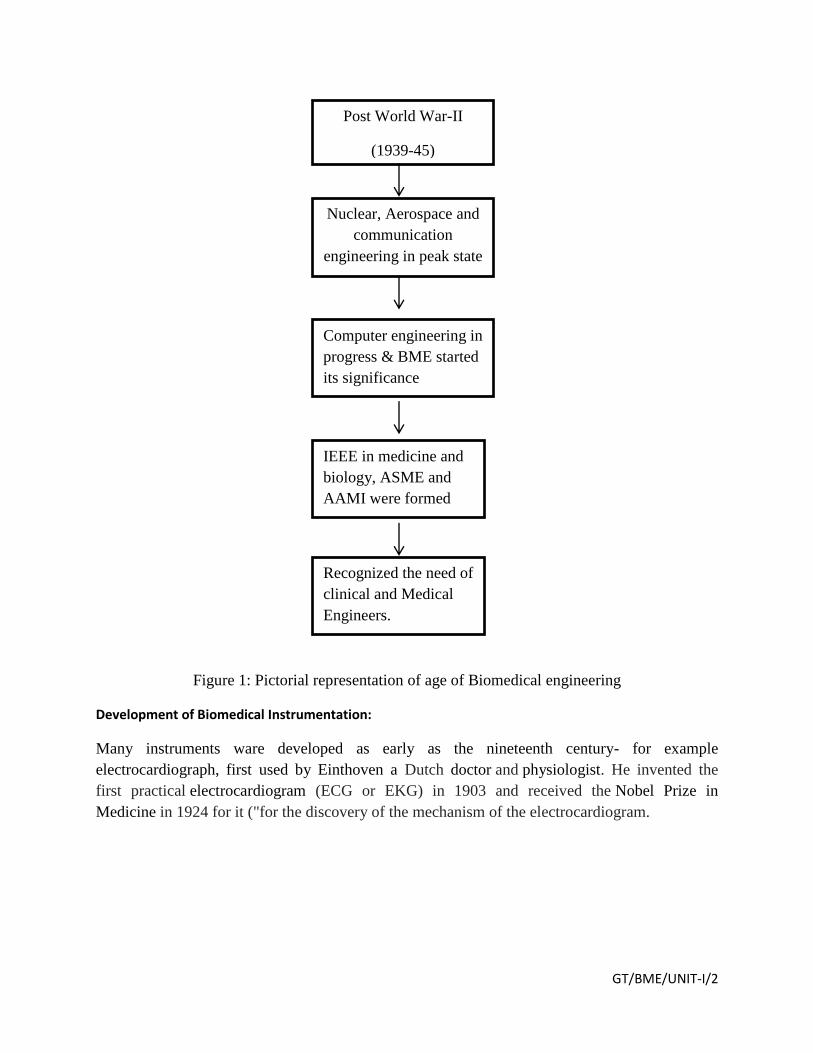
Figure 1: Pictorial representation of age of Biomedical engineering
Development of Biomedical Instrumentation:
Many instruments ware developed as early as the nineteenth century- for example
electrocardiograph, first used by Einthoven a Dutch doctor and physiologist. He invented the
first practical electrocardiogram (ECG or EKG) in 1903 and received the Nobel Prize in
Medicine in 1924 for it ("for the discovery of the mechanism of the electrocardiogram.
Post World War-II
(1939-45)
Nuclear, Aerospace and
communication
engineering in peak state
Computer engineering in
progress & BME started
its significance
IEEE in medicine and
biology, ASME and
AAMI were formed
Recognized the need of
clinical and Medical
Engineers.
GT/BME/UNIT-I/3
Progress was rather slow until after World War II, when a surplus of electronic equipment, such
as amplifiers and recorders, became available. At that time they started to experiment for medical
use, but the results were disappointing.
In 1960 many instrument manufactures entered the field of medical instrumentation, they
designed instrumentation for medical use. A large measure help was provided by the US
government, in particular By NASA.The mercury, Gemini and Apollo programs need accurate
physiological parameters for astronauts. Consequently, much research and development money
went to this area.
Both US government and other organization spent money through grants to universities and
hospitals research units.Awarness of need for engineers and technicians work with medical
profession developed.
GT/BME/UNIT-I/4
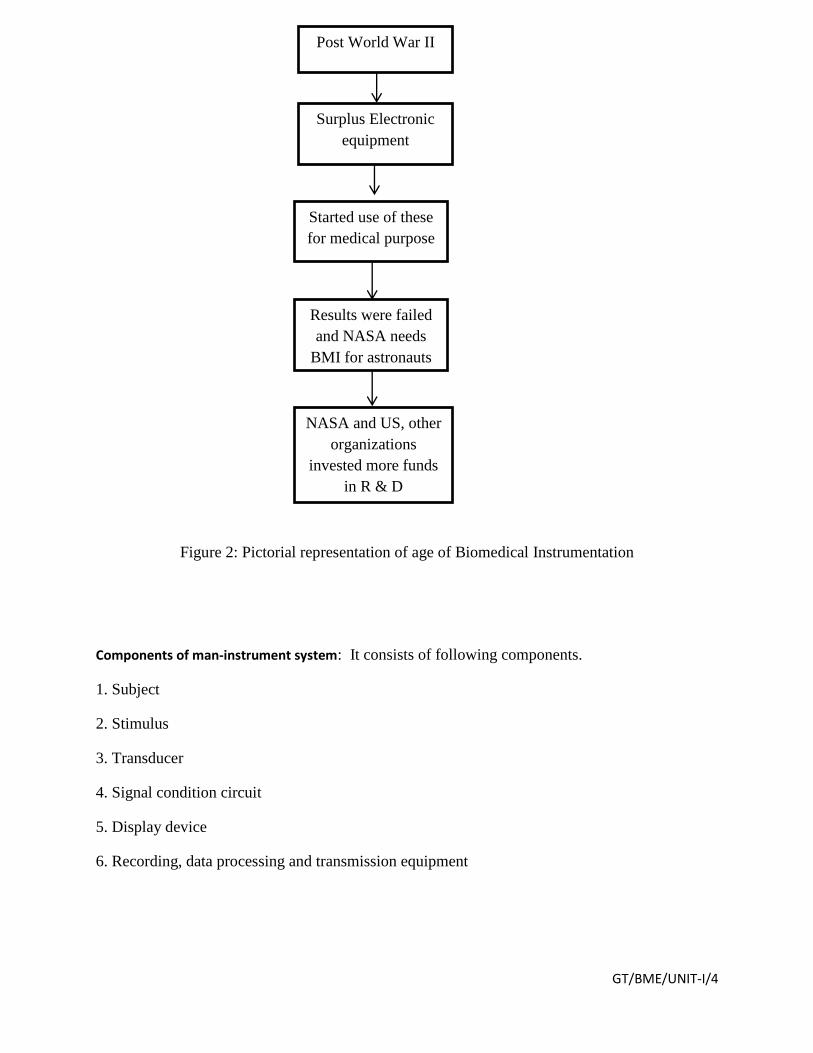
Figure 2: Pictorial representation of age of Biomedical Instrumentation
Components of man-instrument system: It consists of following components.
1. Subject
2. Stimulus
3. Transducer
4. Signal condition circuit
5. Display device
6. Recording, data processing and transmission equipment
Post World War II
Results were failed
and NASA needs
BMI for astronauts
Started use of these
for medical purpose
Surplus Electronic
equipment
NASA and US, other
organizations
invested more funds
in R & D
GT/BME/UNIT-I/5
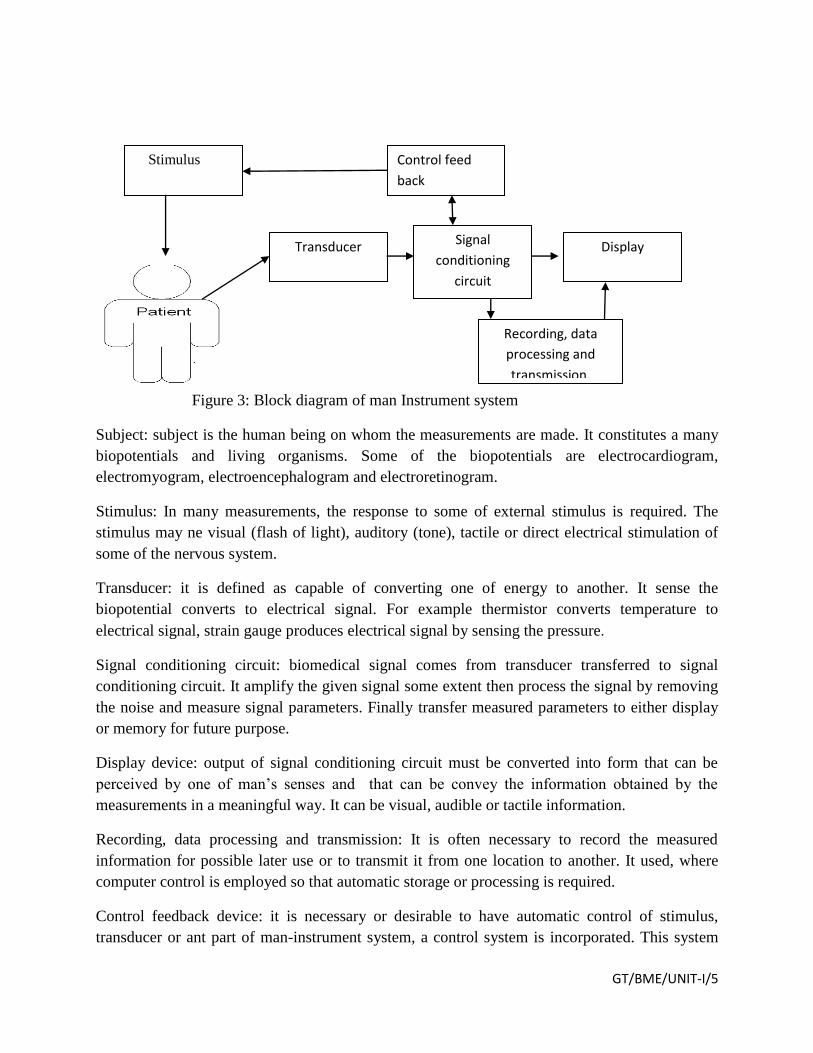
Figure 3: Block diagram of man Instrument system
Subject: subject is the human being on whom the measurements are made. It constitutes a many
biopotentials and living organisms. Some of the biopotentials are electrocardiogram,
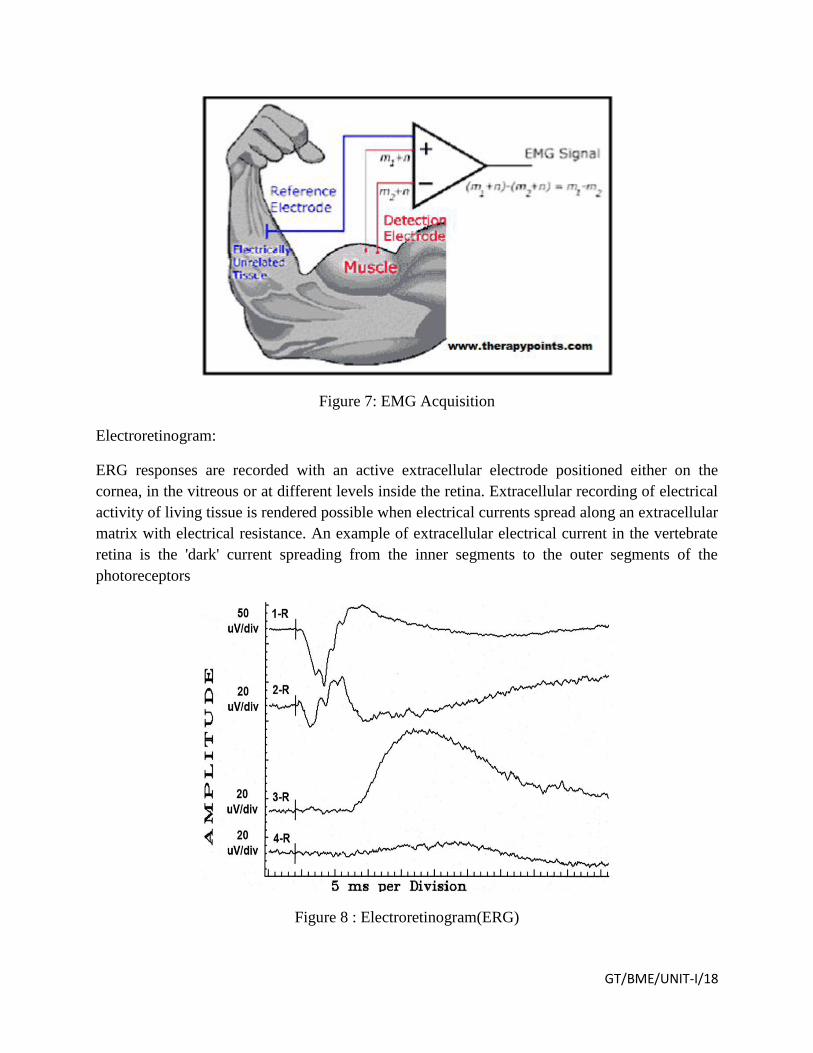
electromyogram, electroencephalogram and electroretinogram.
Stimulus: In many measurements, the response to some of external stimulus is required. The
stimulus may ne visual (flash of light), auditory (tone), tactile or direct electrical stimulation of
some of the nervous system.
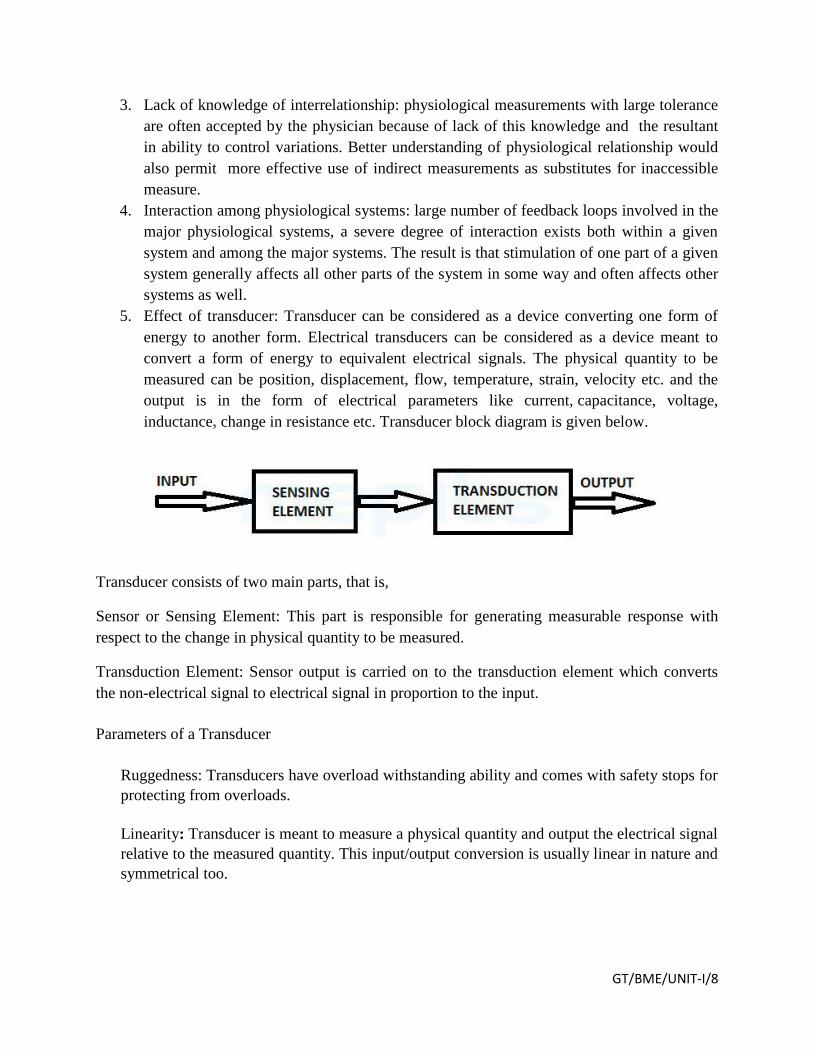
Transducer: it is defined as capable of converting one of energy to another. It sense the
biopotential converts to electrical signal. For example thermistor converts temperature to
electrical signal, strain gauge produces electrical signal by sensing the pressure.
Signal conditioning circuit: biomedical signal comes from transducer transferred to signal
conditioning circuit. It amplify the given signal some extent then process the signal by removing
the noise and measure signal parameters. Finally transfer measured parameters to either display
or memory for future purpose.
Display device: output of signal conditioning circuit must be converted into form that can be
perceived by one of man’s senses and that can be convey the information obtained by the
measurements in a meaningful way. It can be visual, audible or tactile information.
Recording, data processing and transmission: It is often necessary to record the measured
information for possible later use or to transmit it from one location to another. It used, where
computer control is employed so that automatic storage or processing is required.
Control feedback device: it is necessary or desirable to have automatic control of stimulus,
transducer or ant part of man-instrument system, a control system is incorporated. This system
Transducer
Stimulus
Signal
conditioning
circuit
Display
Control feed
back
Recording, data
processing and
transmission.
GT/BME/UNIT-I/6
usually consists of a feedback loop in which part of the output from the signal conditioning or
display equipment is used to control the operation of the system in some way.
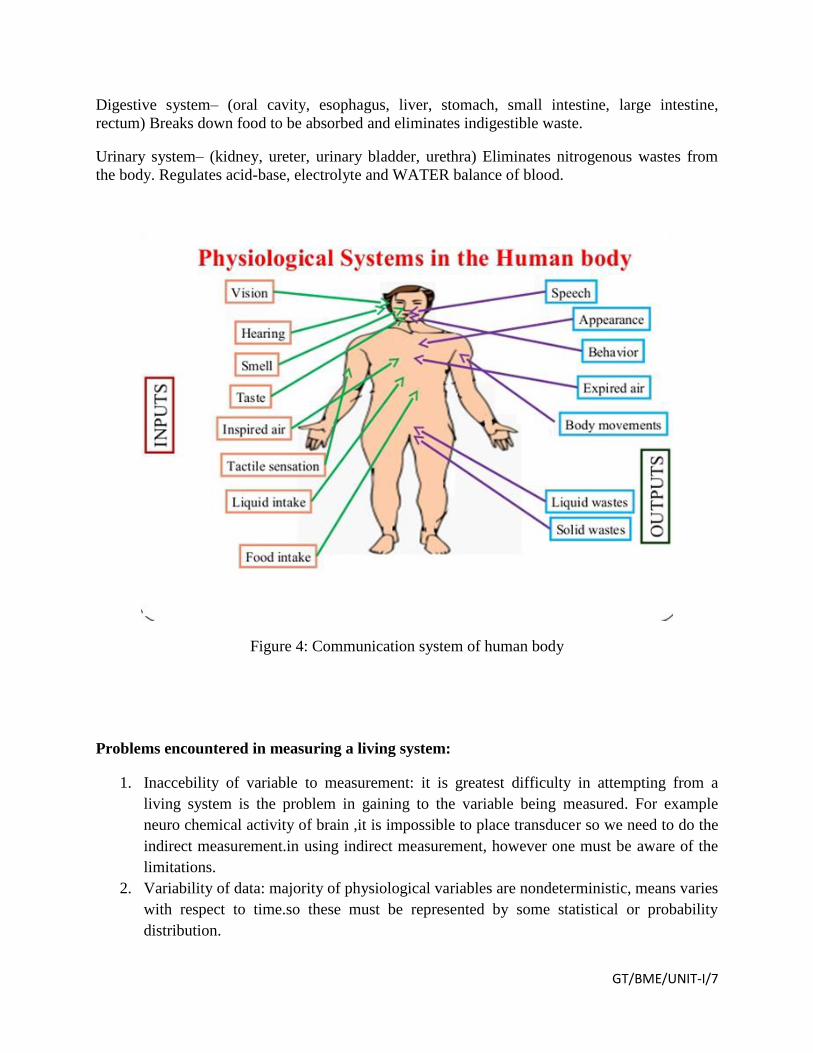
Physiological Systems of Human Body:
Physiology means functional activities of living organs and every organ responsible for one
activity in turn these are work together to achieve systematic activity of human body.
Human Body Organ Systems:
These systems include the Biochemical system, skeletal system, muscular system, lymphatic