25
Induction Therapy in Transplant Eligible MM 2 December 2017 Tontanai Numbenjapon, M.D.

Induction Therapy in Transplant Eligible MM
2 December 2017
Tontanai Numbenjapon, M.D.

What we need from induction therapy in NDMM
• Depth of response: MRD-negative, sCR, CR
• Longest response
• Acceptable toxicity
• Good quality of life

• Maximize the depth of response• Minimize the burden of the residual cells
New treatment paradigm for transplant candidate MM
NDMM-transplant candidate
Induction regimen
High dose melphalan and
ASCT
Post ASCT consolidation
Post ASCT maintenance

Agents to make induction combination regimen for NDMM-transplant eligible
• 6 different classes of agents
– Sterioids
– Alkylators
– PIs: 2nd generation-carfilzomib and ixazomib
– IMiDs: 3rd generation-pomalidomide
– DACIs: panobinostat
– mAbs: elotuzumab and daratumumab

Novel agent-based induction therapies for transplant eligible MM
Combination Thalidomide-based
Bortezomib-based
Lenalidomide-based
PI + IMiD-based
2-drug TD VD RdRD
3-drug TADCTD
PADVCD
RADCRD
VTDVRD
KRd/KTDIxa-RD
4-drug - - - VTDCRVCD
VTD-DaraVRD-Elo
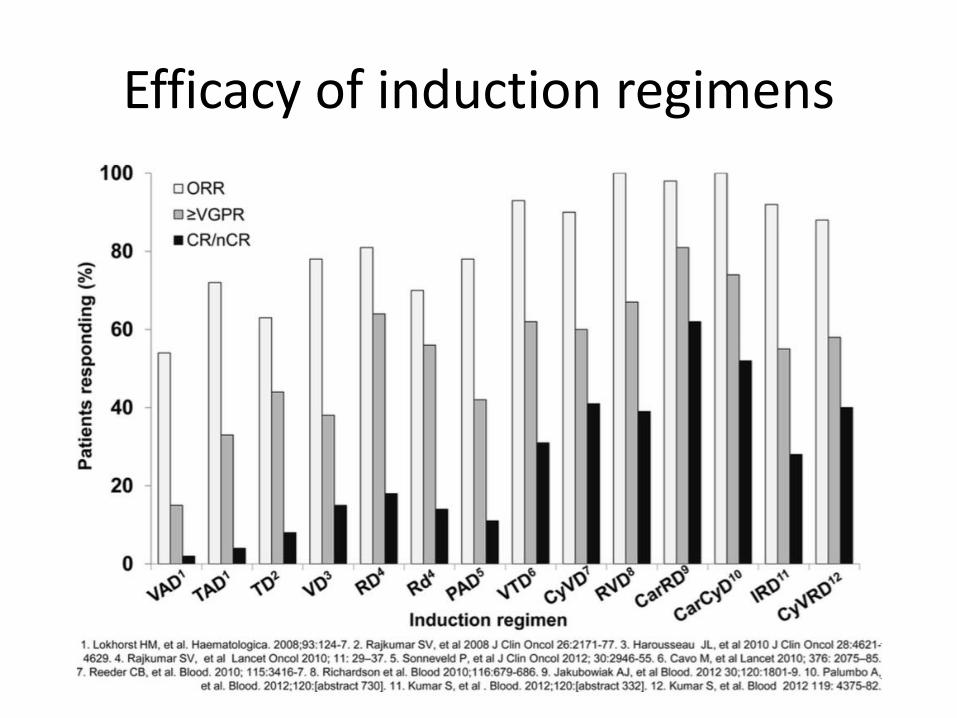
Efficacy of induction regimens

Role of ASCT in MM (non-novel agent era)
Group/trial NAge
(years)Median F/U
CR rate (%)
Median EFS (months)
Median OS (months)
CCT HDT CCT HDT CCT HDT
IFM-90 200 <65 7 years 5 22 18 28 44 57
MAG91 190 55-65 56 months 5 19 19 24 50 55
PATHEMA 164 <65 44 months 11 30 33 42 66 61
Italian MMSG 195 <70 39 months 6 25 15.6 28 42 58+
MRC7 407 <65 42 months 8 44 19 31 42 54
MAG95 190 55-65 10 years 20 48 19 25 48 48
US S9321 516 ≤70 76 months 15 17 14 17 38 38
J Clin Oncol 2011;29:1898-906.

Meta-analysis: Bortezomib-based vs. non-bortezomib-based induction prior to ASCT
Response rate Bortezomib-based
induction(n = 775)
Non-bortezomibbased induction
(n = 772)
OR 95%CI p
Post-transplant (%)
CR+nCR 38 24 2.05 1.64-2.56 <0.001
Response rate
Bortezomib-based
induction(n = 775)
Non-bortezomib
based induction
(772)
HR 95%CI p
PFS, mos 35.9 28.6 0.75
CR+nCR 50 41.1 0.75 0.65-0.85 <0.001
Sonneveid et al. J Clin Oncol 2013;31:3279-87.
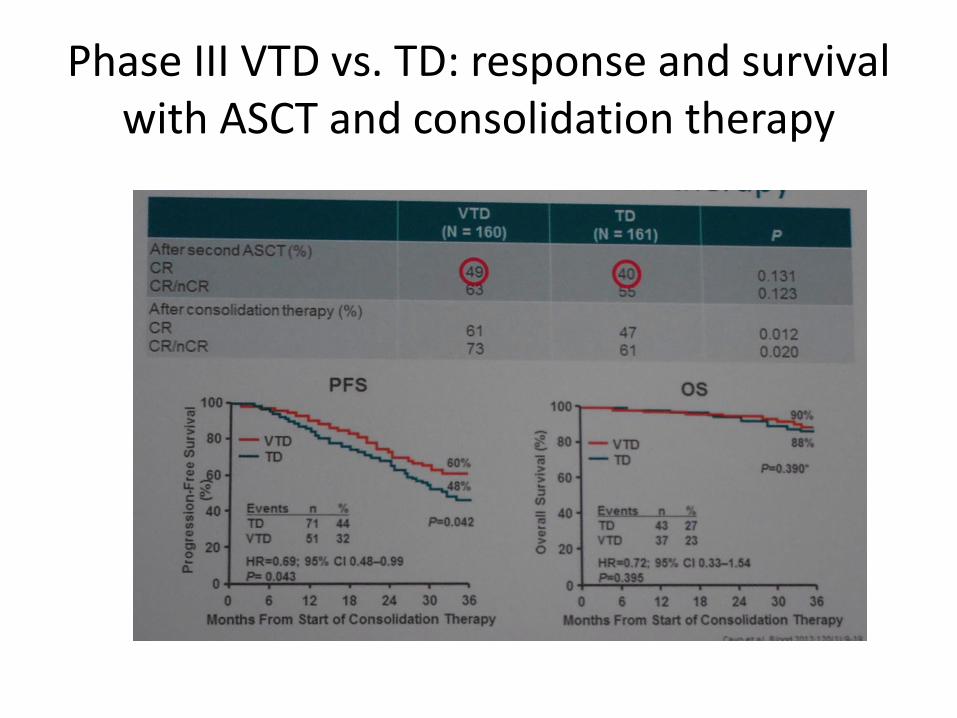
Phase III VTD vs. TD: response and survival with ASCT and consolidation therapy

VCD vs. VTD induction: response
VTD (4-cycles) VCD (4 cycles) P-value
≥CR 13.0% 8.9% 0.22
≥VGPR 66.3% 56.2% 0.05
IFM 2013-04 trial (prospective, intention-to-treat analysis)1
VTD (4-cycles) VCD (4 cycles) P-value
≥CR 13.0% 8.9% 0.22
≥VGPR 66.3% 56.2% 0.05
GIMEMA MMY-3006 and EMN-02 studies (retrospective, case-matched analysis)2
Moreau P, et al. Blood 2016;127:2569-74.Cavo , et al. Leukemia 2015;29:2429-31.

Evolving role of high-dose melphalanand ASCT in the era of novel agents
and antibodies• Novel agents
– Improved induction
– Improved consolidation
– Improved maintenance
• Early vs. late transplant
• Single vs. Tandem transplant
• Role of transplants in high-risk disease

Upfront ASCT vs. late ASCT
Palumbo A, et al. N Engl J Med 2014;371:895.

Attal M, et al. N Engl J Med 2017;376:1311-20.
NDMMAge ≤ 65 years
(n=700)R
Vd
x 3
cyc
les
R1:1
Cyc
lop
ho
sph
amid
e m
ob
iliza
tio
nP
BSC
co
llect
ion
RVd (n=350)Five 21-day cyclesV 1.3 mg/m2 D1,4,8,11R 25 mg D1-14d 10 mg daily
HDT-ASCT +
RVd x 2 cycles
(n=350)Melphalan 200 mg/m2
ASCT
R m
ain
ten
ance
R 1
0 m
g/d
x 3
mo
nth
s th
en
titr
ate
to 1
5 m
g/d
if t
ole
rate
dco
nt.
up
to
1 y
ear
or
un
til
dis
ease
pro
gres
sio
n
3 weeks
3 weeks
Primary endpoint: Progression free survival
Secondary endpoint: Response rate, time to disease
progression, overall survival, adverse events
IFM 2009: Role of ASCT in novel agent era

Upfront ASCT is important in novel agent era
RVD arm Transplant arm P value
CR 49% 59%
VGPR 29% 29% 0.02
PR 20% 11%
At least VGPR 78% 88% 0.001
Neg MRD by FCM 65% 80% 0.001
4-y PFS 35% 47% HR: 0.69 (0.56-0.84; P<0.001)
4-y OS 83% 86% HR: 1.2(0.7-1.8; P = NS)
Attal M, et al. Blood 2015;126:391a
Attal M, et al. N Eng J Med 2017;376:1311-20.ç

PFS OS
Upfront ASCT is important in novel agent era
Attal M, et al. Blood 2015;126:391a
Attal M, et al. N Eng J Med 2017;376:1311-20.ç

Blood 2016;128:LBA-1
NDMM symptomatic
Age ≤ 70 years,
(n=758)
R1:1:1
Second ASCTMel 200 mg/m2
Consolidation
VRd x 4 cycles
BMT CTN0702 StaMINA trial
Firs
t A
SCT
Mel
20
0 m
g/m
2
R m
ain
ten
ance
R 1
0 m
g/d
fo
r 3
yea
rs o
r u
nti
l d
isea
se p
rogr
essi
on
• Median follow up from randomization: 38 months• 38-month PFS: ACM 57% vs. TAM 56% vs. AM 52% • Median OS not been reached; 38-month ACM 86% vs. TAM 82% vs. AM 83%• Cumulative incidence of disease progression is not different**Addition of second ASCT or RVd consolidation was NOT superior to single ASCT followed by Lenalidomide maintenance**
ACM
TAM
AM
No improvement of PFS and OS using tandem ASCT or post ASCT consolidation over single ASCT

With more effective induction, consolidation and maintenance, ASCT is still required
Zimmerman T, et al. ASH 2016. abstract 675
Treatment arm Induction ASCT Consolidation Post maintenance
≥VGPR ≥CR ≥CR ≥VGPR ≥CR ≥VGPR ≥CR
ASCT 73% 16% 27% 91% 67% 94% 86%
No ASCT 69% 18% 89% 34% 90% 59%

Transplant increases MRD-neg CR

Autograft 1 vs. 2
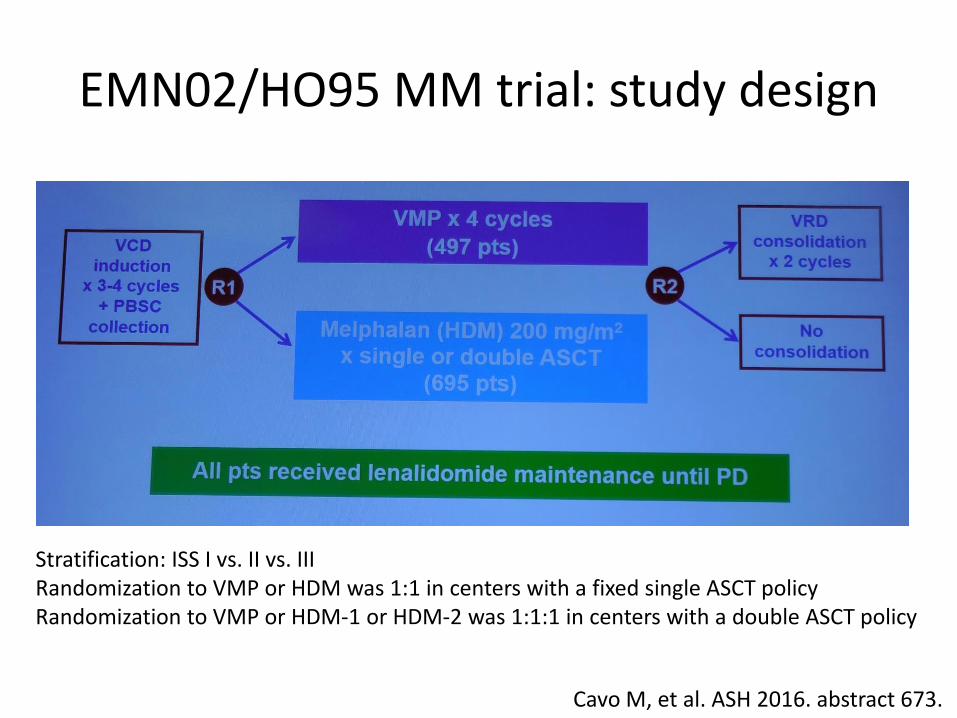
EMN02/HO95 MM trial: study design
Cavo M, et al. ASH 2016. abstract 673.
Stratification: ISS I vs. II vs. IIIRandomization to VMP or HDM was 1:1 in centers with a fixed single ASCT policyRandomization to VMP or HDM-1 or HDM-2 was 1:1:1 in centers with a double ASCT policy

1192 pts eligible for randomization 1
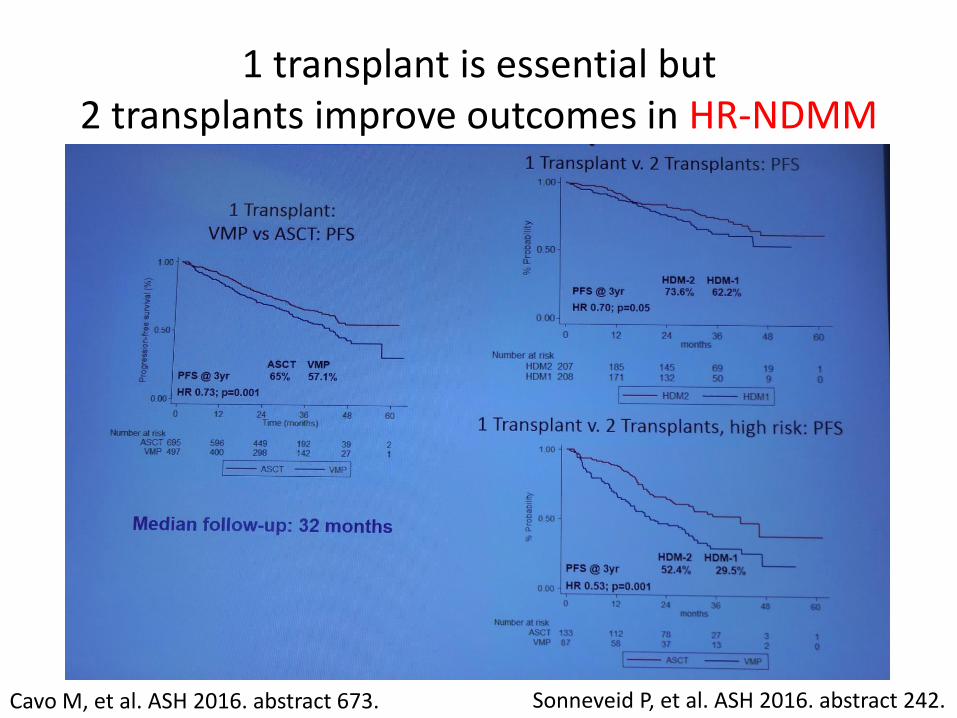
1 transplant is essential but 2 transplants improve outcomes in HR-NDMM
Cavo M, et al. ASH 2016. abstract 673. Sonneveid P, et al. ASH 2016. abstract 242.

Single vs. double ASCT for patients who failed CR after bortezomib-based induction regimens and had del(17p) and or t(4;14)
Harousseau et al. JCO 2010;28:4621-9.Cavo M, et al. Lancet 2010;376:2075-85.Rosinof L, et al. Blood 2012;120:1589-96.
Cavo M, et al. ASH 2013 abstract 768

OS by study group and by treatment arm (single vs. double HDM/ASCT)
• HOVON PAD and VAD arms:
single ASCT
• GMMG PAD and VAD arms:
double ASCT
• PAD: single vs. double HDM/ASCT
at 96 moths: 42% vs. 55%
• Cox all arms:
HR: 0.71, 95% CI = 0.54-0.94;
P = 0.018
Double ASCT subanalysis
PFS at 5 years, % OS at 5 years, %
FISH n Bor p standard Bor p Standard
Del(17p) y/n
39/312 22% vs. 27%
0.47 5% vs. 24%
65% vs. 72%
0.48 18% vs. 66%
Sonneveid P, et al. ASH 2015 abstract 27

Conclusions: Management of transplant candidate in the era of new drugs
• 3-drug combinations are recommended induction regimens, with the recent EMA-approval of VTD in this setting
• ASCT should remain as standard of care in 2017 in the frontline treatment of patients eligible for high-dose therapy– Double tandem transplant is of use, particularly in high-risk patients?
• Conventional CR is inadequate to predict outcomes since in most of the cases may logs of residual tumor cells still persist
• MRD negativity should be the current treatment endpoint, but not in Thailand now
• Consideration of the whole treatment sequence, including induction regimen and post-ASCT therapy, will maximize the depth of response.
• 4-drug regimens may possibly be the next standard of care.

















