78
1 Good mornin g
| Date post: | 22-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | npdch-visnagar |
| View: | 36 times |
| Download: | 2 times |

1
Good morning

INFLAMMATION
&
CHEMICALMEDIATIORS
2
Dr. Sharanprakash R S1st year MDS NPDCH, Visnagar.

INTRODUCTION - History
General features of inflammation
3
CLASSIFICATION OF INFLAMMATION
ACUTE INFLAMMATION – Stimuli
Vascular Events & Cellular Events
Morphology of acute inflammation
CHEMICAL MEDIATORS OF INFLAMMATION
CHRONIC INFLAMMATION – causes
features
DENTAL ASPECTS OF INFLAMMATION
DENTAL ABSCESS
4
CONCLUSION
REFERENCE
INTRODUCTION
,, and. Hence in the importance of inflammation is that it can
sometimes be, and is thus the cause of tissue injury in many
disorders.
According to ROBINSINFLAMMATION is a complex reaction to injurious agent such as microbes and damaged , necrotic cells that consist of vascular responses , migration , and activation of leukocytes and systemic reaction
5
Without inflammation
, infections would go
unchecked
Wounds would
never heal
Injured tissues might
remain permanent
decaying lesions
In practice of medicine
inappropriately triggered
or poorly controlled
Imagine suppose
inflammation is not present
HISTORICAL HIGHLIGHTS
Egyptian Papyrus , 3000 BC CELSUS , Roman Writer
- 1 AD - CARDINAL SIGNS
JOHN HUNTER , 1793 –
“ Inflammation is not a disease
but a constructive effect on host”
JULIUS CONHEIM-1st used
microscope to observe inflamed
blood vessels & cells 6
7
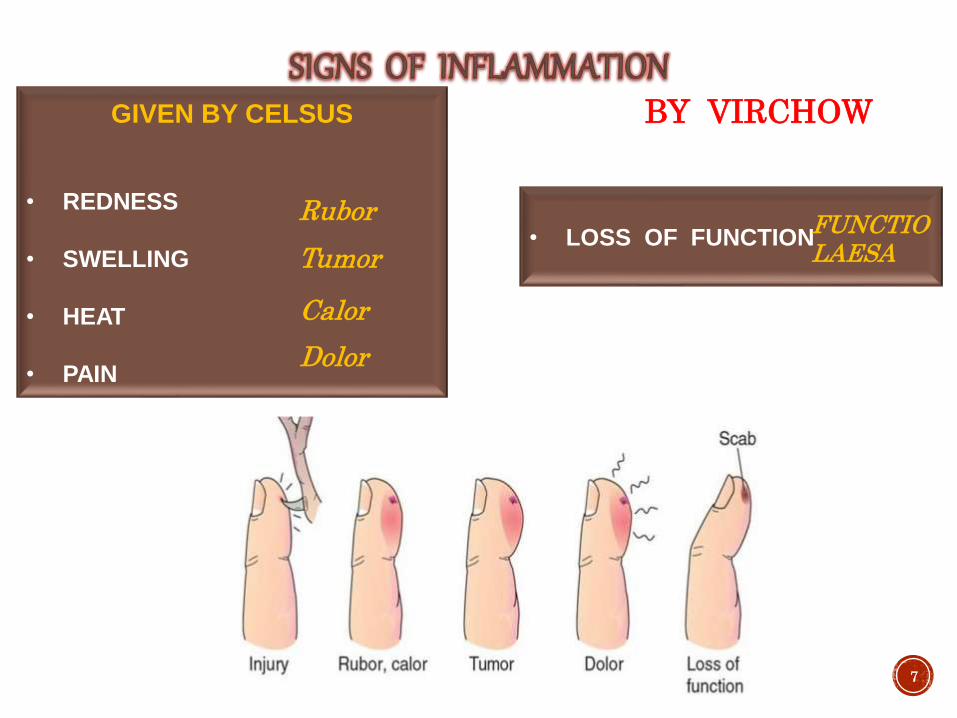
GIVEN BY CELSUS
• REDNESS
• SWELLING
• HEAT
• PAIN
Rubor
Tumor
Dolor
Calor
• LOSS OF FUNCTION FUNCTIO LAESA
BY VIRCHOW
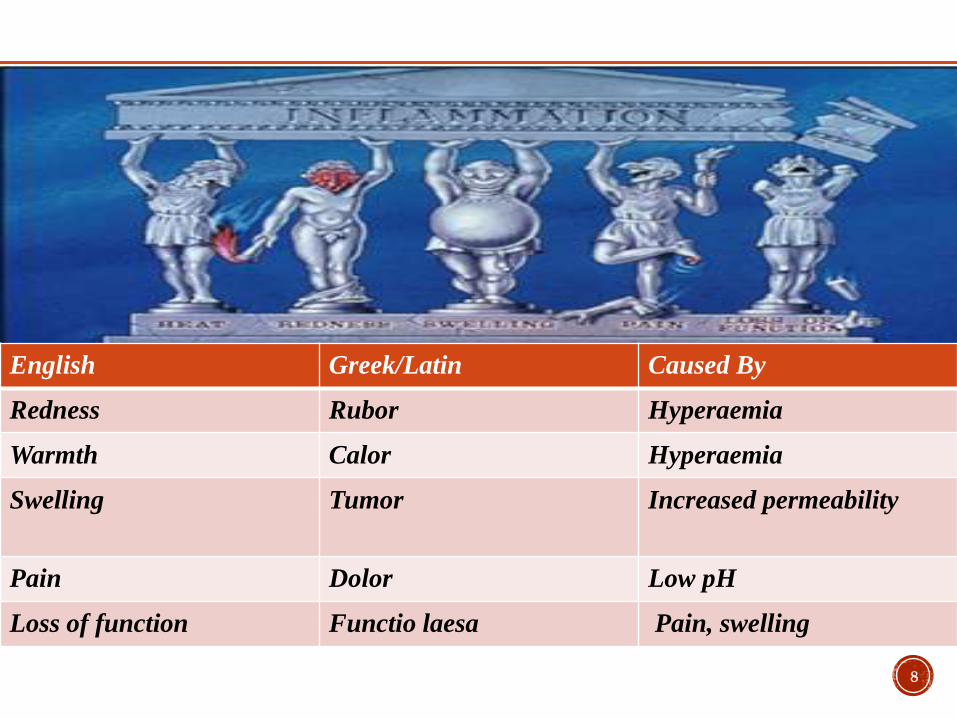
8
English Greek/Latin Caused By
Redness Rubor Hyperaemia
Warmth Calor Hyperaemia
Swelling Tumor Increased permeability
Pain Dolor Low pH
Loss of function Functio laesa Pain, swelling
CLASSIFICATION
9
ACUTE INFLAMMATION
CHRONIC INFLAMMATION
ACUTE INFLAMMATION
An acute condition is one with a rapid onset and/or a short course
INFECTIONS :
Bacterial / viral /
parasitic &
microbial toxins
Trauma :
Blunt /
penetrating
Physical /
chemical
agents eg
thermal injury
Foreign body eg
sutures / splinters
Immune reactions /
hypersensitivity
reactions
10
ACUTE INFLAMMATION
11
CHANGES
CELLULAR EVENTS
ACUTE INFLAMMATION
HEMODYNAMIC
CHANGES / Change in
vascular flow & calibre
CHANGE IN VASCULAR
PERMEABILITY
12

Transient vasoconstriction
Vasodilation
Increased permeability of microvasculature
Stasis
Emigration of leukocytes13
HEMODYNAMIC CHANGES / Change in vascular flow
& caliber
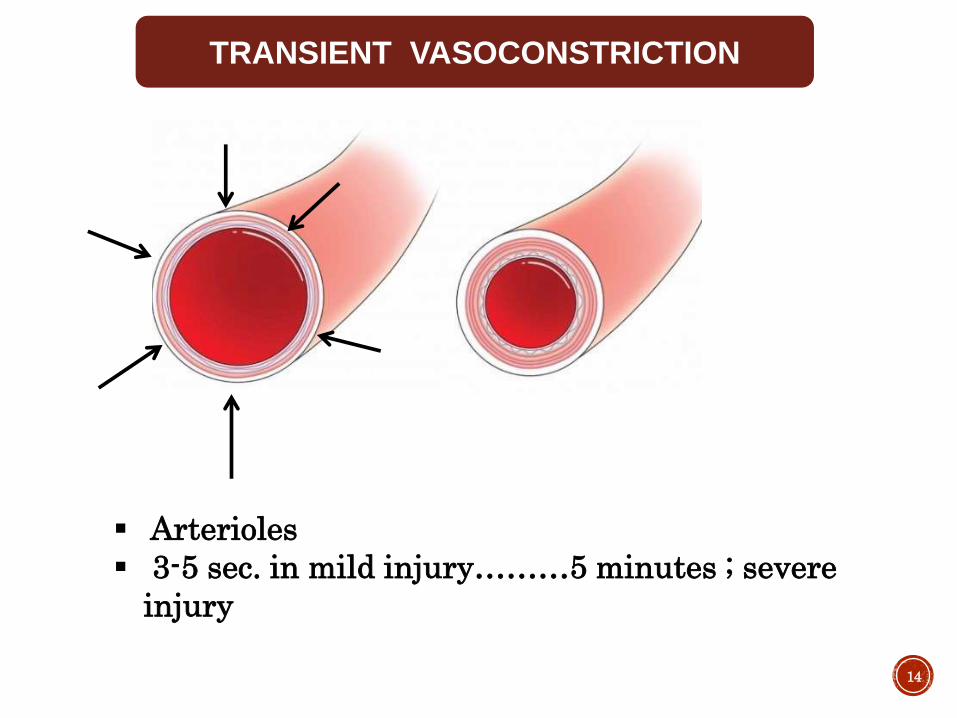
TRANSIENT VASOCONSTRICTION
Arterioles
3-5 sec. in mild injury………5 minutes ; severe
injury
14

PERSISTENT PROGRESSIVE
VASODILATION
• 1st involves arteriole ………then other capillary
bed
• seen in 1st 30 min.
• Results in, increase blood vol. in microvascular
bed, which is responsible for redness and warmth
at site
15
16
INCREASED PERMEABILITY OF
MICROVASULATURE
• Contraction of endothelial cells -
Histamine
• Retraction of endothelial cells -
- cytokine IL – 1 , TNF
• Direct injury to endothelial cells
• Endothelial injury mediated by
leukocytes

STASIS
Increased vascular permeability
leads to loss of fluid from
microvasculature
Concentration of red cells in
small vessels
Slower blood flow
S
T
A
S
I
S17
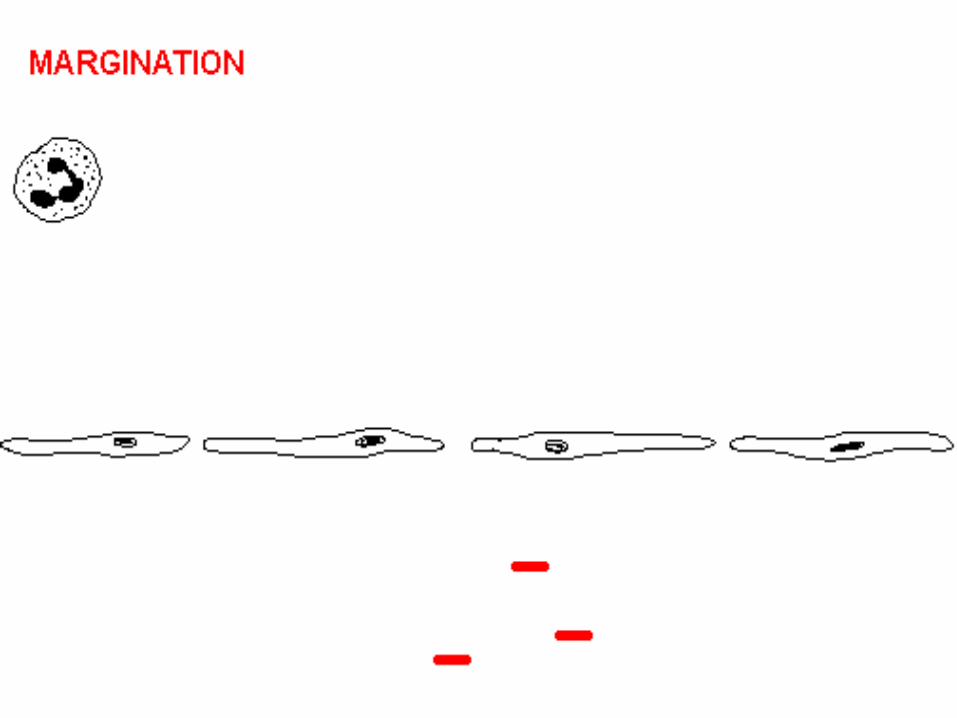
LEUCOCYTIC MIGRATION &
EMIGRATION
Stasis is followed by peripheral
orientation of leucocytes along vascular
endothelium
Movement of leucocytes in
extracellular space through gaps b/w
endothelium.
18

19
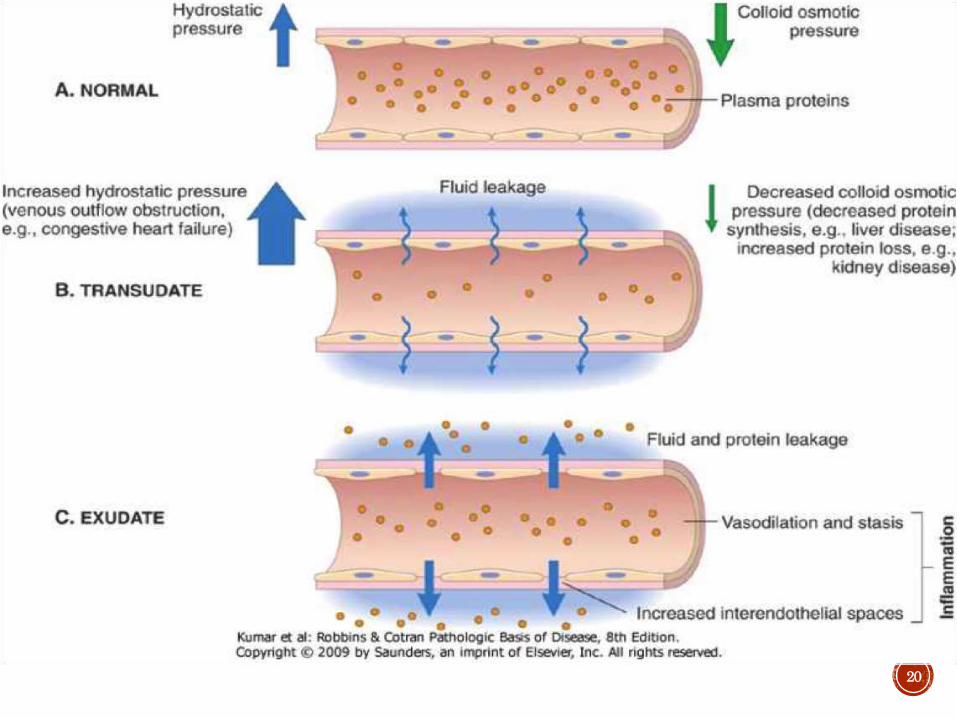
CHANGE IN VASCULAR PERMEABILITY
In initial due to vasodilation and hydrostatic pressure the fluid is seen its called transudate
Transudate is a
fluid with low
protein content
(most of which is
albumin), little or
no cellular
material, and low
specific gravity
Exudate The
escape of fluid,
proteins, and blood
cells from the
vascular system
into the interstitial
tissue or body
cavities is known
as exudation
Edema denotes an excess of fluid in the interstitial tissue or serous cavities; it can be either an exudate or a transudate
20
21
CELLULAR EVENTSDeliver leukocytes to site of
injury
To perform their
‘FUNCTION’
Ingest offending bacteria
Kill bacteria & other microbes
Get rid of necrotic tissue & foreign
substance
22
23
CELLULAR EVENTS
1) DELIVERY OF LEUKOCYTES TO SITE OF
INJURY
2) PHAGOCYTOSIS

CELLULAR EVENTS
• Margination
• Rolling
• Adhesion
IN THE LUMENEMIGRATION
•Eigration into interstitial tissue
CHEMOTAXIS
24
1 )
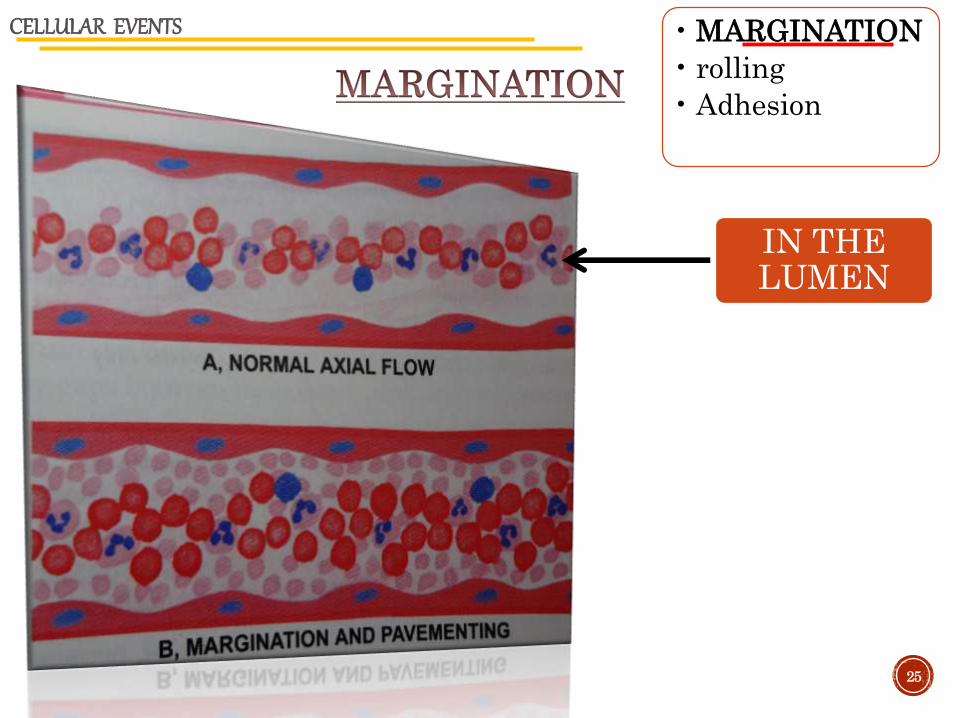
CELLULAR EVENTS • MARGINATION
• rolling
• Adhesion
IN THE LUMEN
25
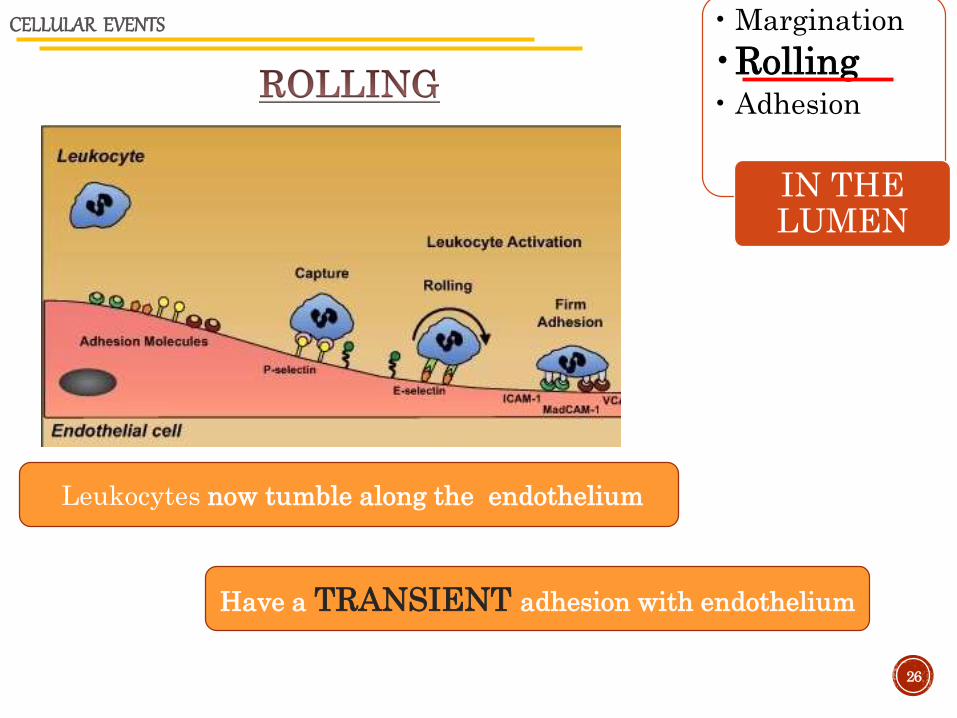
• Margination
•Rolling• Adhesion
IN THE LUMEN
CELLULAR EVENTS
Leukocytes now tumble along the endothelium
Have a TRANSIENT adhesion with endothelium
26
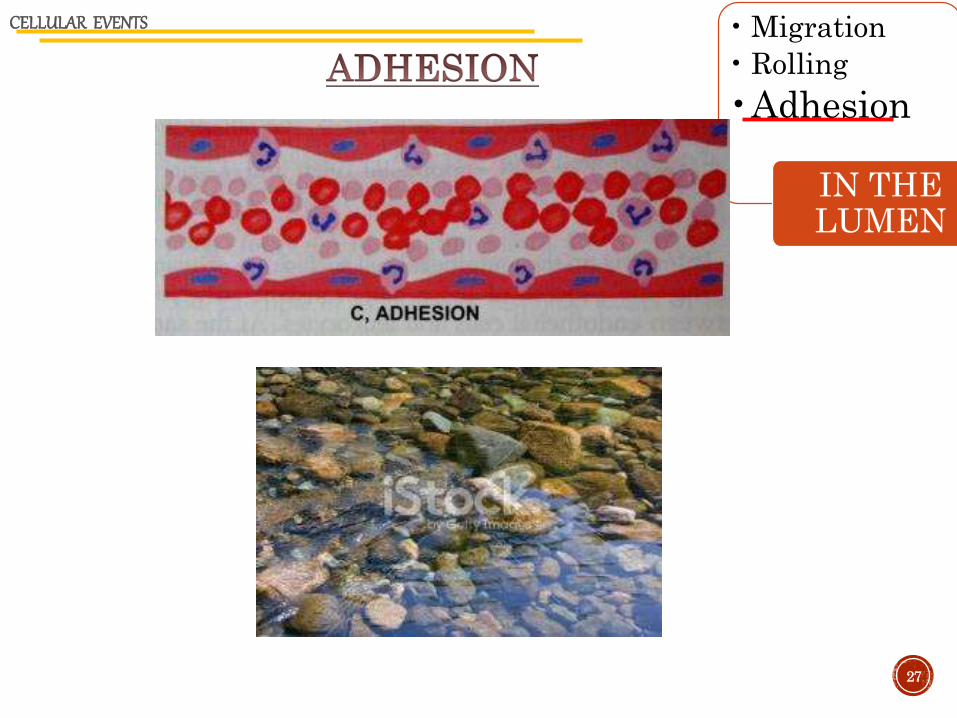
• Migration
• Rolling
•Adhesion
IN THE LUMEN
CELLULAR EVENTS
27
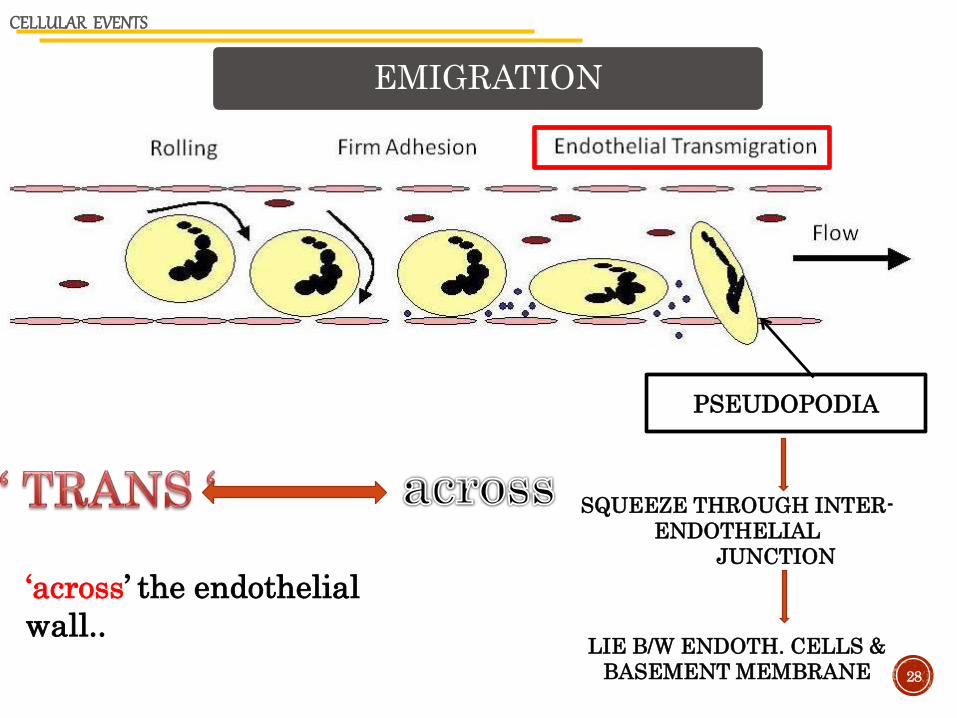
CELLULAR EVENTS
PSEUDOPODIA
SQUEEZE THROUGH INTER-
ENDOTHELIAL
JUNCTION
LIE B/W ENDOTH. CELLS &
BASEMENT MEMBRANE 28
‘across’ the endothelial
wall..
EMIGRATION
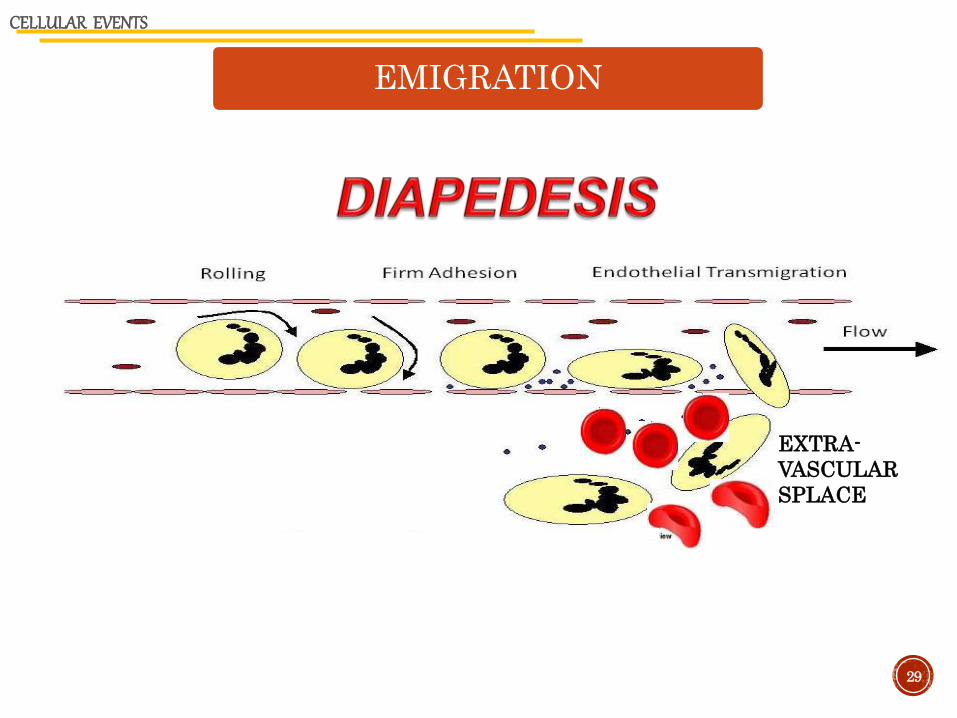
EMIGRATION
CELLULAR EVENTS
EXTRA-
VASCULAR
SPLACE
29
CHEMOTAXIS
CELLULAR EVENTS
Along chemical gradient
30
After exiting the circulation,
leukocytes emigrate in
tissues toward the site of
injury by a process called
chemotaxis
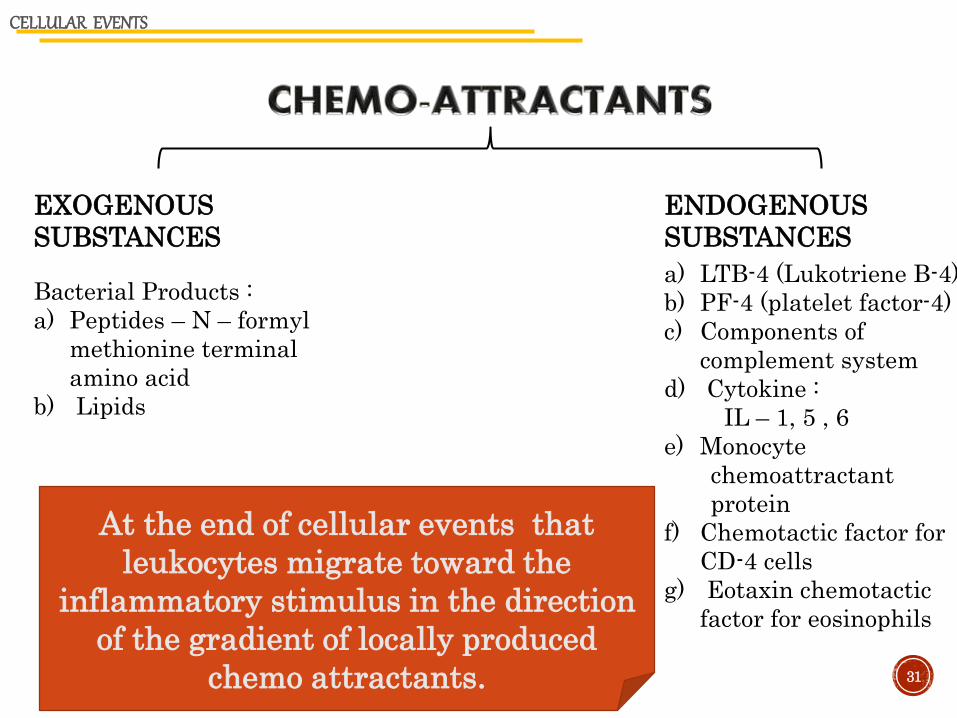
EXOGENOUS
SUBSTANCES
ENDOGENOUS
SUBSTANCES
Bacterial Products :
a) Peptides – N – formyl
methionine terminal
amino acid
b) Lipids
a) LTB-4 (Lukotriene B-4)
b) PF-4 (platelet factor-4)
c) Components of
complement system
d) Cytokine :
IL – 1, 5 , 6
e) Monocyte
chemoattractant
protein
f) Chemotactic factor for
CD-4 cells
g) Eotaxin chemotactic
factor for eosinophils
CELLULAR EVENTS
31
At the end of cellular events that
leukocytes migrate toward the
inflammatory stimulus in the direction
of the gradient of locally produced
chemo attractants.
32

CELLULAR EVENTS
33
PHAGOCYTOSIS
CELLULAR EVENTS
PHAGOCYTOSIS
RECOGNITION AND ATTACHMENT OF PARTICLE
ENGULFMENT WITH FORMATION OF PHAGOCYTIC VESICLE
DEGRANULATION STAGE
KILLING & DEGRADATION STAGE
34
1
2
3
4
CELLULAR EVENTS
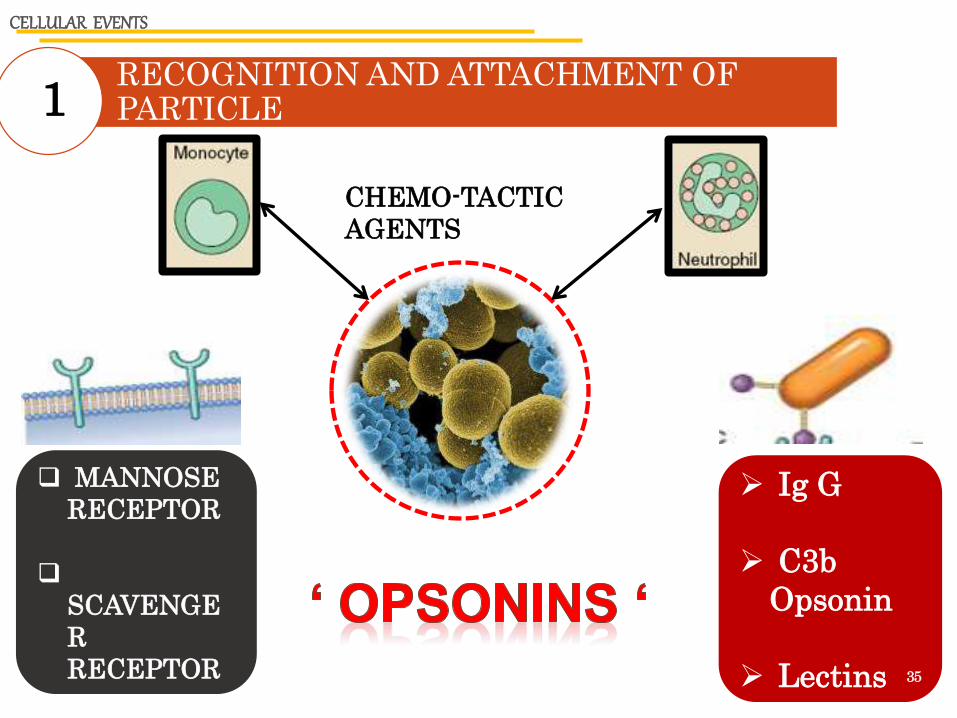
RECOGNITION AND ATTACHMENT OF PARTICLE1
CHEMO-TACTIC
AGENTS
Ig G
C3b
Opsonin
Lectins
MANNOSE
RECEPTOR
SCAVENGE
R
RECEPTOR 35

ENGULFMENT WITH FORMATION OF PHAGOCYTIC VESICLE2
CELLULAR EVENTS
Fig 10.6 harsh mohan pg 10136
PHAGO-
LYSO-SOME

DEGRANULATION STAGE3
CELLULAR EVENTS
During this stage the
PMNs (ploymorphonuclear neutrophils)
&
Mononuclear phagocyte secrete enzymes eg
IL-2 , 6-TNF
Arachidonic acid metabolites (Prostaglandin , leukotriene ,
platelet activating factor
Oxygen metabolites
• are released into phagolysosome37
KILLING & DEGRADATION STAGE4
CELLULAR EVENTS
OXYGEN – DEPENDENT BACTERICIDAL
MECHANISM
OXYGEN–INDEPENDENT
MECHANISM
38
Phagocytes as scavenger cells
killing and digest's the micro-organism
If this mechanism fails to kill and degrade some bacteria like
TUBERCLE BACILLI
THEN

KILLING & DEGRADATION STAGE
39
Production of reactive oxygen metabolites is necessary to kill the micro
organism & Increased oxygen consumption by the phagocytic leucocytes
(respiratory brust )
2o2
NADPH
oxidase
(superoxid
e anion )
NADPH NADP + H(PLUS
ION )
2H(plus ion)
H2O2
Hydrogen peroxide
CELLULAR EVENTS
Followed by :
Lysosomal hydrolases
Permeability increasing factors
Defensing
Cationic proteins
40

41
‘ MEDIATOR ‘ : one that reunites differences b/w disputants
CHEMICAL MEDIATORS : chemical substances that mediate the process of inflammation………..
42
CHEMICAL MEDIATORS OF INFLAMMATION
Present in plasma in
precursor form
Must be activated to
acquire biologic
properties
Pr. In intracellular granules
Major cellular sources
Platelets
Neutrophil
Monocyte / macrophage
43
CHEMICAL MEDIATORS OF INFLAMMATION
VASO – ACTIVE AMINES
44
HISTAMINE
SOURCE : 1) Mast cells in C.T
adjacent to blood vessels
2) Blood basophils
3) Platelets
STIMULI : Injury
Immune reactions
SEROTONIN
SOURCE : 1) Platelets
2) Enterochromaffin cells
STIMULI : Platelet aggregation after
contact with collagen ,
thrombin
45
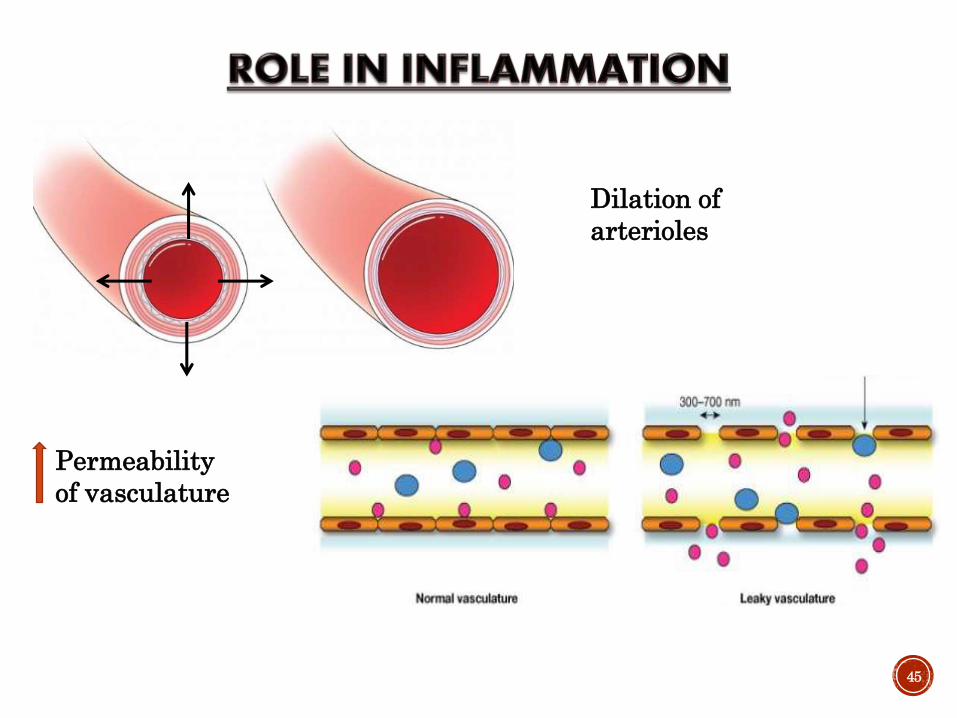
Dilation of
arterioles
Permeability
of vasculature
CHEMICAL MEDIATORS OF INFLAMMATION
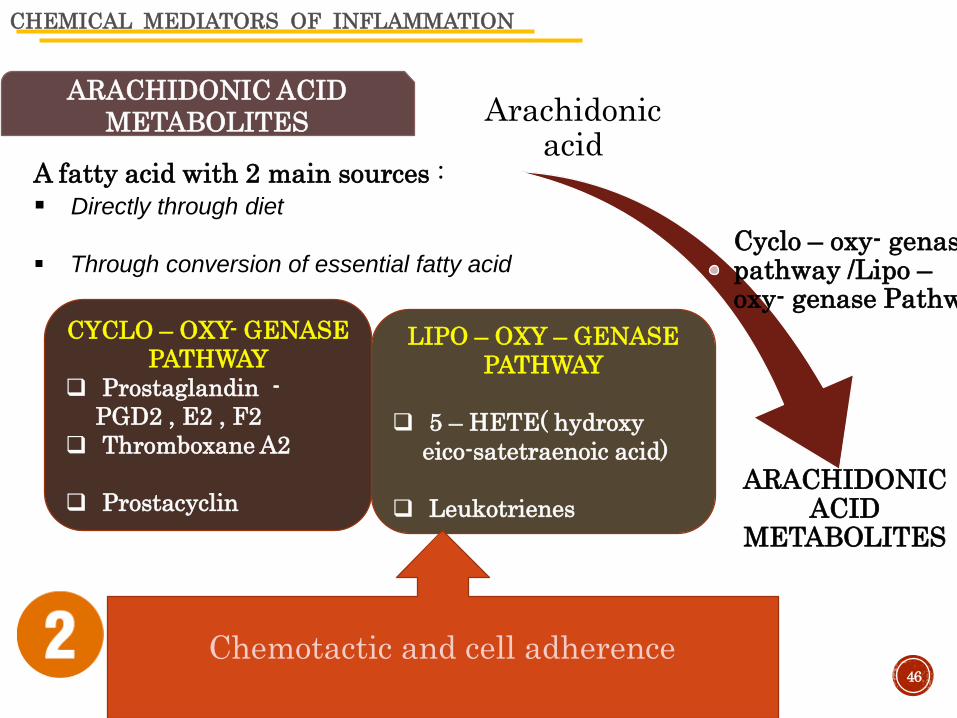
ARACHIDONIC ACID
METABOLITES
A fatty acid with 2 main sources :
Directly through diet
Through conversion of essential fatty acid
CYCLO – OXY- GENASE
PATHWAY
Prostaglandin -
PGD2 , E2 , F2
Thromboxane A2
Prostacyclin
LIPO – OXY – GENASE
PATHWAY
5 – HETE( hydroxy
eico-satetraenoic acid)
Leukotrienes
46
Arachidonic acid
Cyclo – oxy- genasepathway /Lipo –oxy- genase Pathwa
ARACHIDONIC ACID
METABOLITES
Chemotactic and cell adherence
CHEMICAL MEDIATORS OF INFLAMMATION
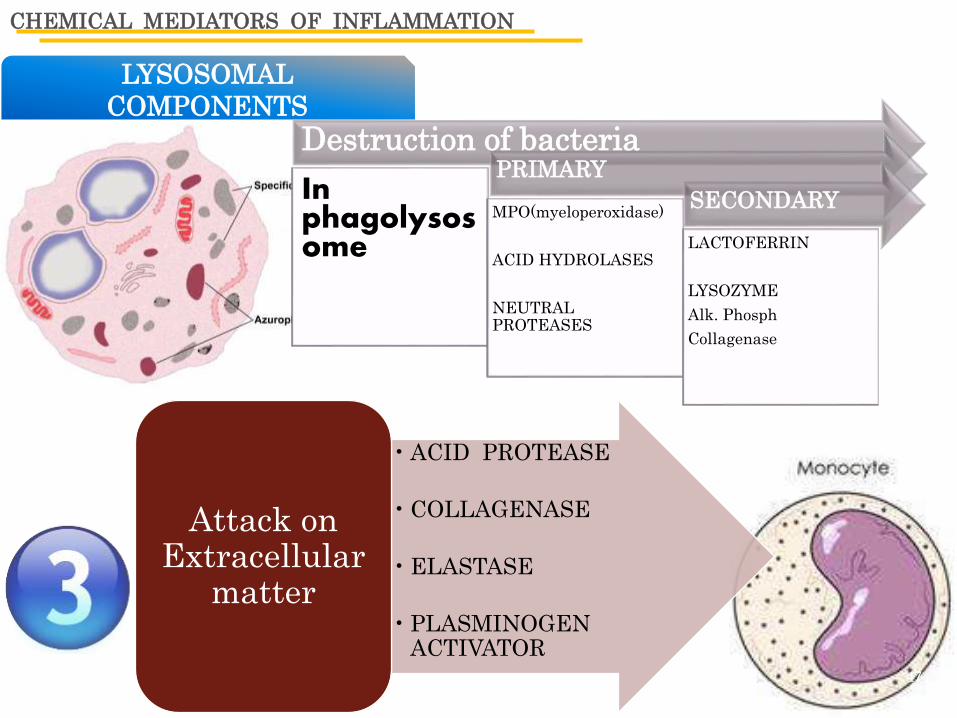
LYSOSOMAL
COMPONENTS
47
Destruction of bacteria
In phagolysosome
PRIMARY
MPO(myeloperoxidase)
ACID HYDROLASES
NEUTRAL PROTEASES
SECONDARY
LACTOFERRIN
LYSOZYME
Alk. Phosph
Collagenase
• ACID PROTEASE
• COLLAGENASE
• ELASTASE
• PLASMINOGEN ACTIVATOR
Attack on Extracellular
matter
CHEMICAL MEDIATORS OF INFLAMMATION
CYTOKINES
• proteins produced mainly by- activated lymphocytes &
macrophages , also from endothelium, epithelium & connective
tissue cells.
TNF and IL - 1
• major cytokines that mediate inflammation.
• Produced mainly by activated macrophages
STIMULI :
• Immune reactions,
• physical injury & variety of inflammatory stimuli.
• endotoxins & other microbial products
48
NITROUS OXIDE
CHEMICAL MEDIATORS OF INFLAMMATION
Released by activated neutrophils and macrophages,such as
Superoxide , hydrogen peroxide , hydroxyl ion
ACTION : Endothelial cell damage- inc. vascular permeability
49
6 OXYGEN METABOLITES
mediates in vascular dilation
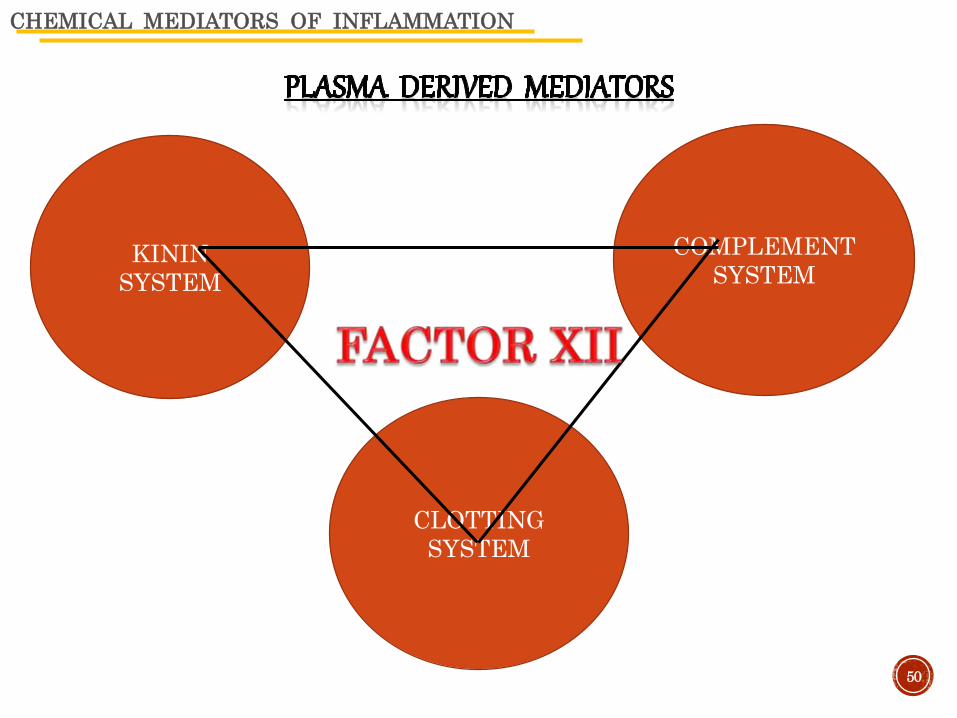
CHEMICAL MEDIATORS OF INFLAMMATION
KININ
SYSTEM
CLOTTING
SYSTEM
COMPLEMENT
SYSTEM
50
51
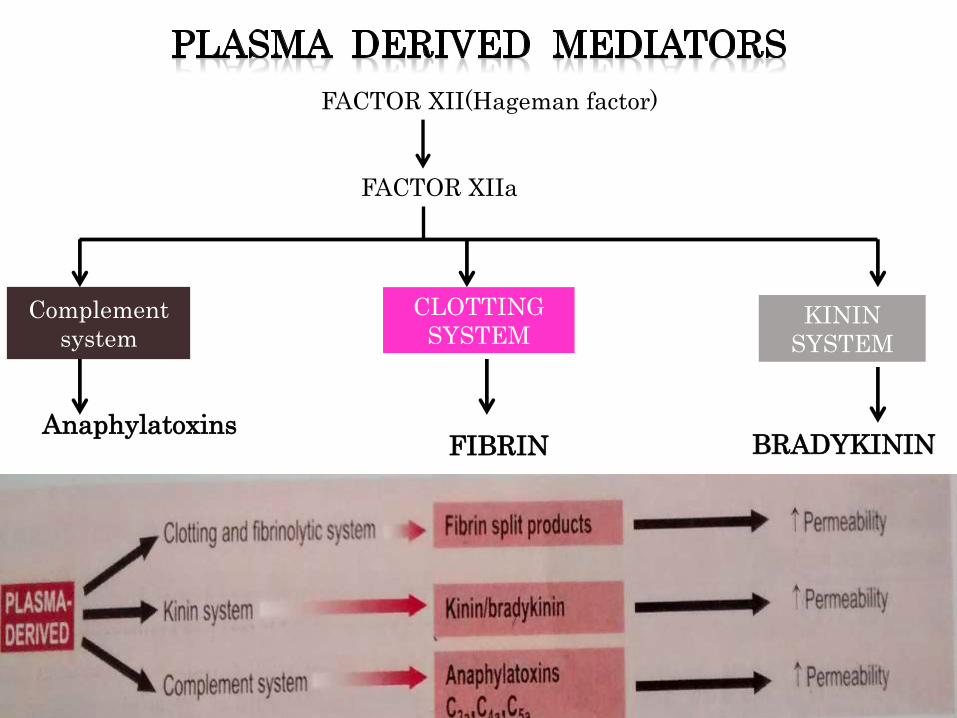
FACTOR XII(Hageman factor)
FACTOR XIIa
Complement
system
CLOTTING
SYSTEMKININ
SYSTEM
AnaphylatoxinsFIBRIN BRADYKININ

FATE OF ACUTE INFLAMMATION
ACUTE
INFLAMMATIO
N
RESOLUTION
HEALING BY
SCARRING
PROGRESSION
TO
SUPPURATION
PROGRESSION
TO CHRONIC
INFLAMMATION
52
CHRONIC INFLAMMATION
Inflammation of prolonged duration (weeks to
months) in which inflammation , tissue
destruction and attempts at repair are
proceeding simultaneously.CAUSES
Following acute inflammation
Begin insidiously as a low – grade
inflammation
Persistent inf. By micro-organisms : Eg-
tubercle bacilli
Prolonged exposure to toxic agents
Auto - immunity 53
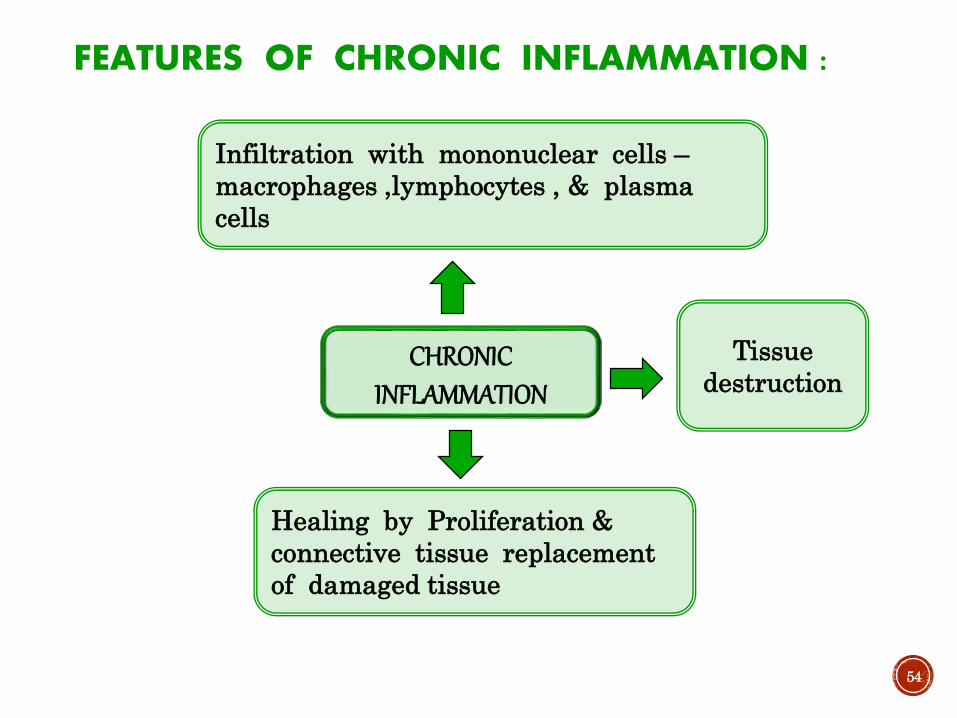
FEATURES OF CHRONIC INFLAMMATION :
54
CHRONIC INFLAMMATION
Infiltration with mononuclear cells –
macrophages ,lymphocytes , & plasma
cells
Tissue
destruction
Healing by Proliferation &
connective tissue replacement
of damaged tissue

INFILTRATION WITH MONO-NUCLEAR CELLS
55

• Incr. lysosomal enzymes
• Greater ability to
phagocytose 56
ACTIVATION OF
MACROPHAGE
Cytokine
IFN - ɤ
Endotoxin ,
fibronectin
chemical
mediators
MACROPHAGE
IN ACUTE
INFLAMMATION
IN CHRONIC
INFLAMMATION
* Irritant
eliminated –
macrophage
disappears
Persistent macrophage accumulation by
following mechanisms :
1)Recruitment from circulation –
Chemotactic stimuli include :
a) Platelet derived growth factor
b) Transforming growth factor
2.) Local proliferation of macrophages
3.) Immobilization of macrophages57
58
TISSUE DESTRUCTION OR NECROSIS
• ACTIVATED
MACROPHAGES Elastase
Protease
Collagenase
Reactive oxygen
radical
Cytokine IL-1,8
59
Part 2
Dental aspect
Cont……

60
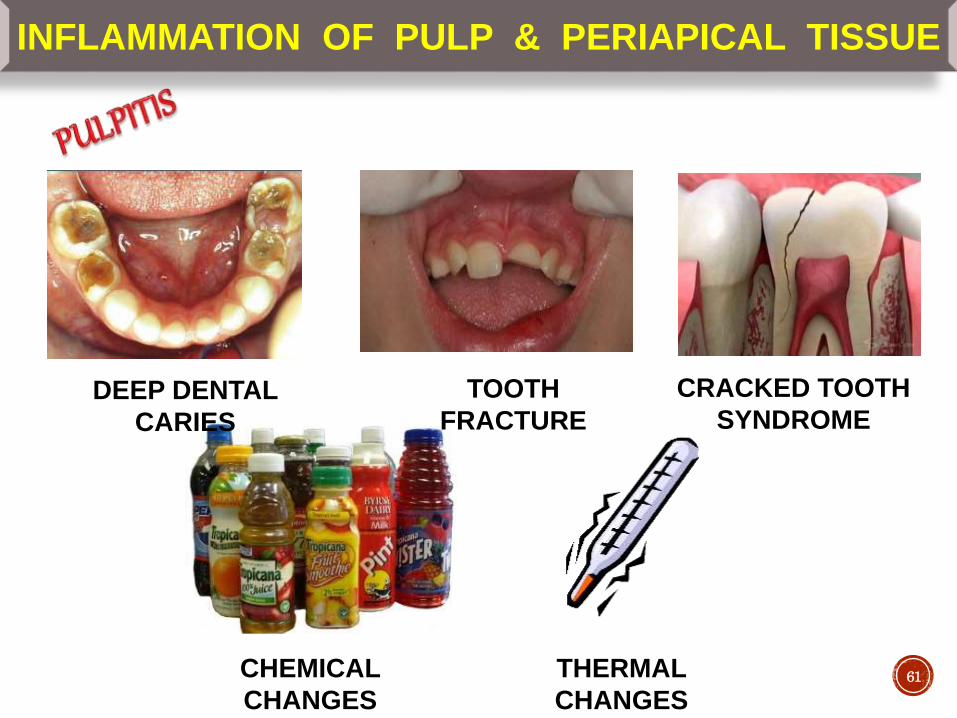
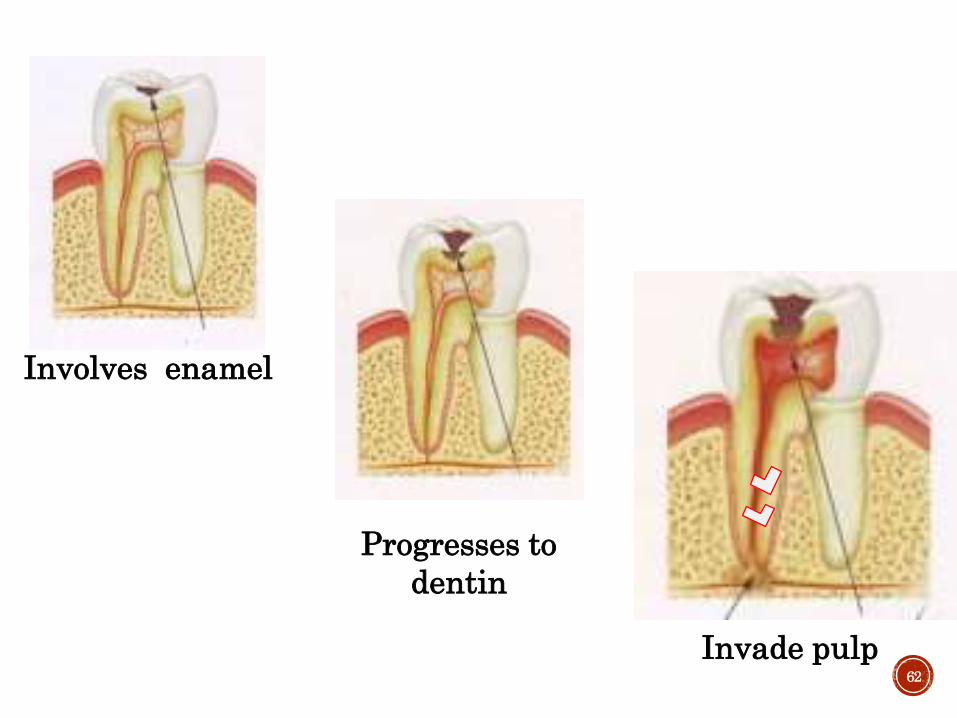
INFLAMMATION OF PULP & PERIAPICAL TISSUE
DEEP DENTAL
CARIES
TOOTH
FRACTURE
CRACKED TOOTH
SYNDROME
CHEMICAL
CHANGES
THERMAL
CHANGES61
62
Involves enamel
Progresses to
dentin
Invade pulp
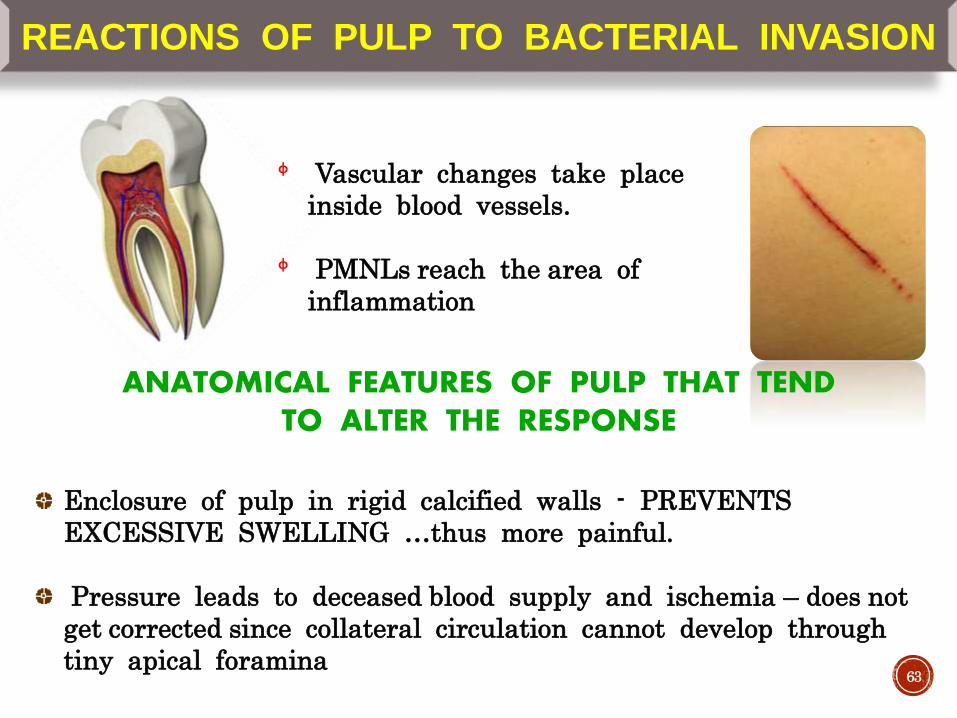
REACTIONS OF PULP TO BACTERIAL INVASION
ᶲ Vascular changes take place
inside blood vessels.
ᶲ PMNLs reach the area of
inflammation
ANATOMICAL FEATURES OF PULP THAT TEND TO ALTER THE RESPONSE
Enclosure of pulp in rigid calcified walls - PREVENTS
EXCESSIVE SWELLING …thus more painful.
Pressure leads to deceased blood supply and ischemia – does not
get corrected since collateral circulation cannot develop through
tiny apical foramina 63
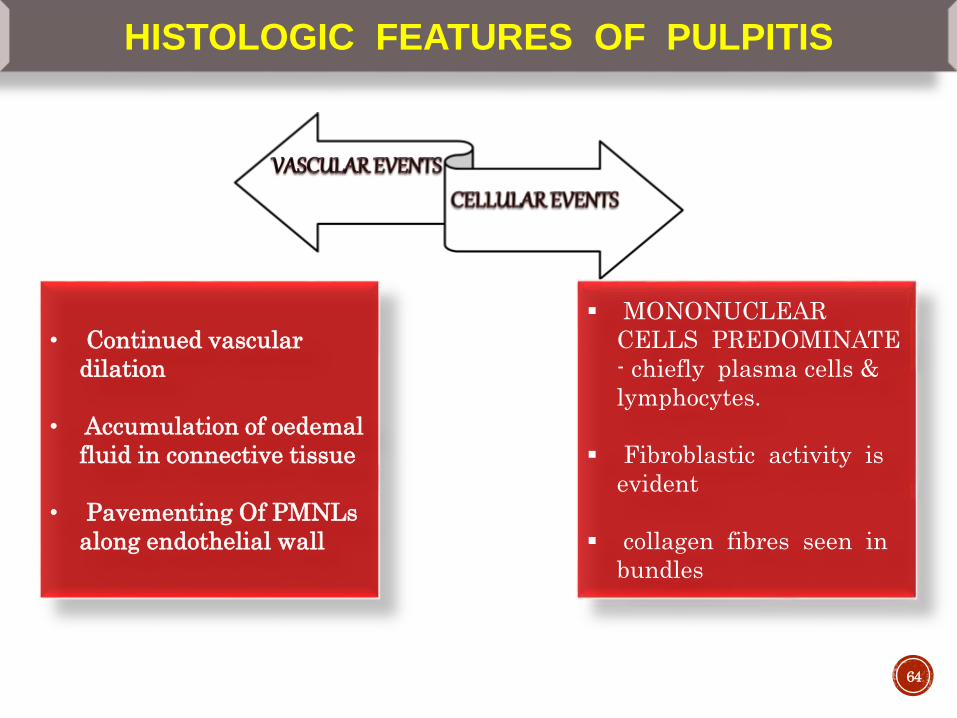
HISTOLOGIC FEATURES OF PULPITIS
64
MONONUCLEAR
CELLS PREDOMINATE
- chiefly plasma cells &
lymphocytes.
Fibroblastic activity is
evident
collagen fibres seen in
bundles
• Continued vascular
dilation
• Accumulation of oedemal
fluid in connective tissue
• Pavementing Of PMNLs
along endothelial wall
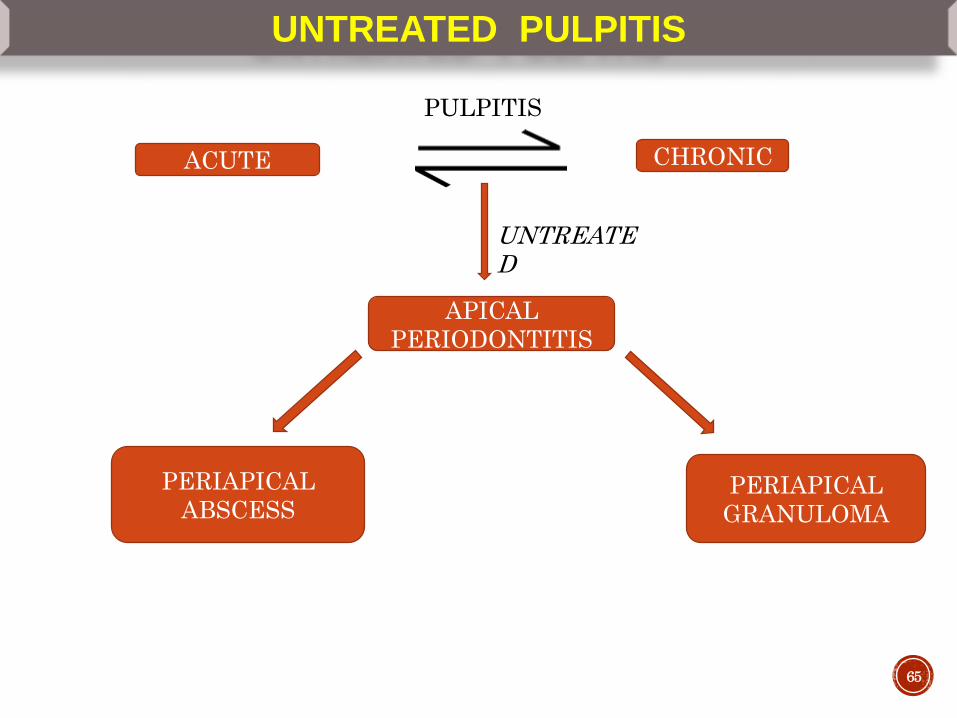
UNTREATED PULPITIS
ACUTE CHRONIC
PULPITIS
UNTREATED
APICAL
PERIODONTITIS
PERIAPICAL
ABSCESSPERIAPICAL
GRANULOMA
65
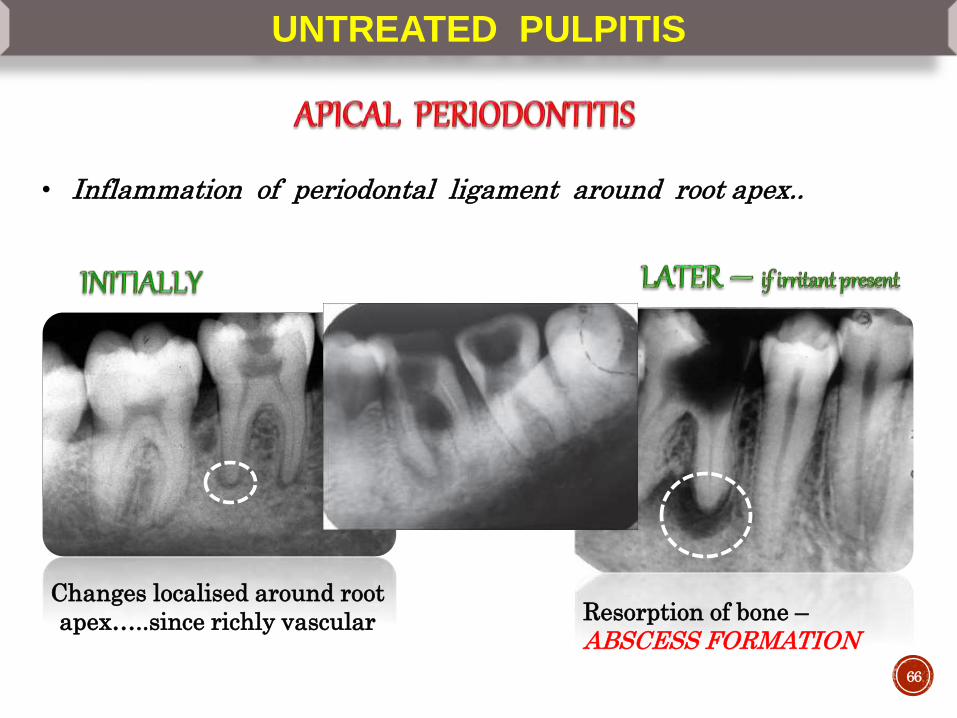
UNTREATED PULPITIS
• Inflammation of periodontal ligament around root apex..
Changes localised around root
apex…..since richly vascular Resorption of bone –
ABSCESS FORMATION
66
67
PYOGENIC
ABSCESS
PYAEMIC
ABSCESSCOLD ABSCESS
• Commonest type
• mostly found in soft
tissues
• eg periapical abscess
• occurs due to
circulating
bacterial emboli in
blood
Abscess without
signs of inflammation
Eg Tubercular
abscess
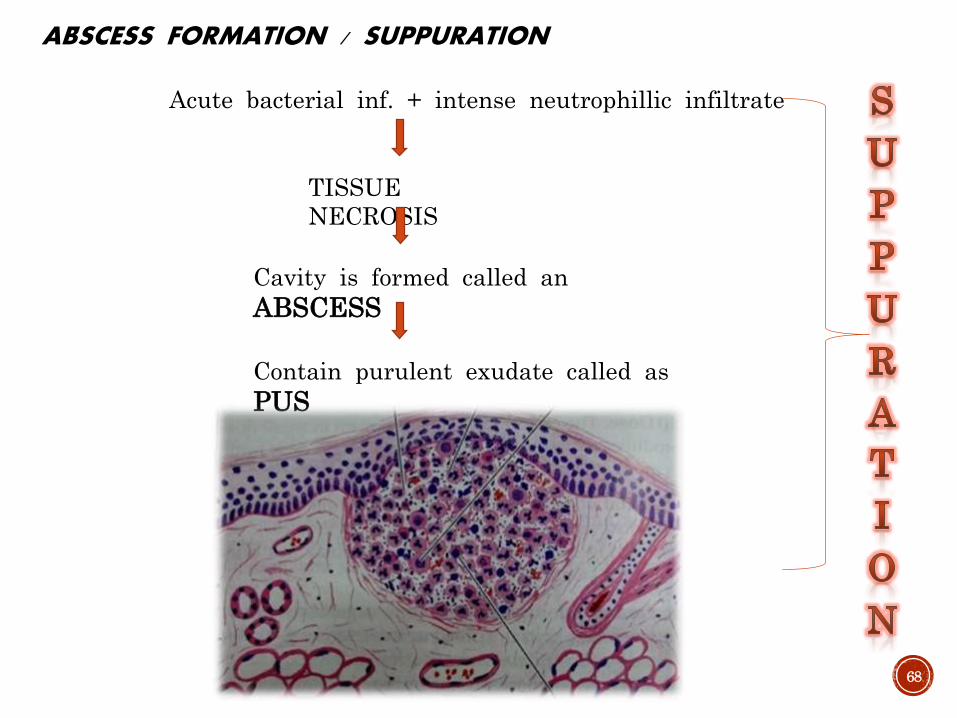
ABSCESS FORMATION / SUPPURATION
Acute bacterial inf. + intense neutrophillic infiltrate
TISSUE
NECROSIS
Cavity is formed called an
ABSCESS
Contain purulent exudate called as
PUS
68
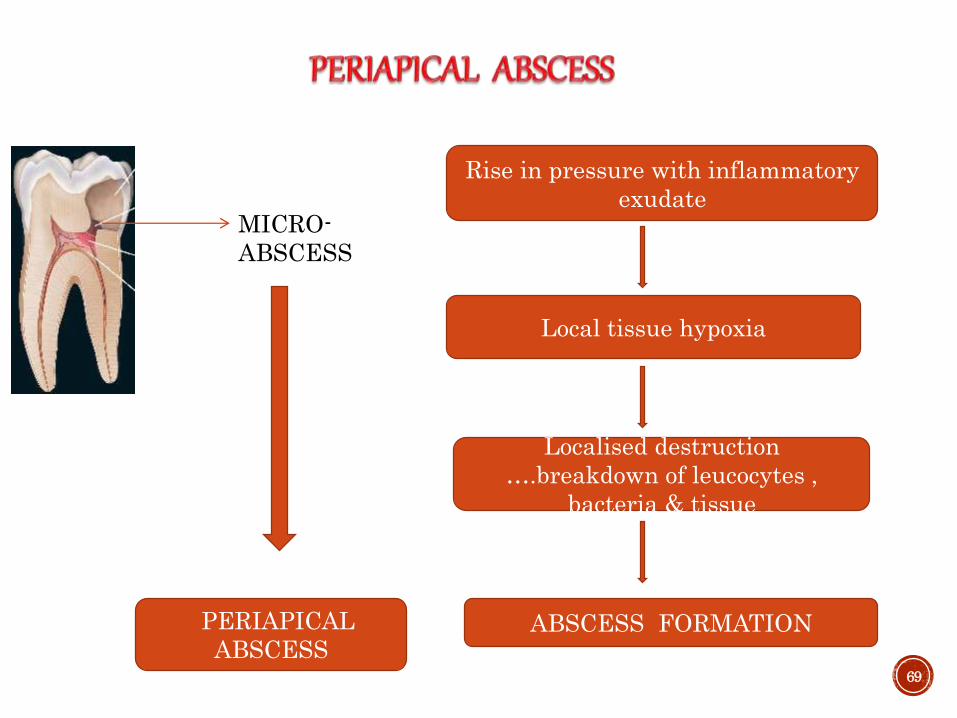
MICRO-
ABSCESS
Rise in pressure with inflammatory
exudate
Local tissue hypoxia
Localised destruction
….breakdown of leucocytes ,
bacteria & tissue
ABSCESS FORMATIONPERIAPICAL
ABSCESS69

Disintegrating PMNLs
Viable leukocytes , lymphocytes , bacterial colonies
Dil. Blood vessels in adj. PDL and marrow spaces + serous exudate
70

( DENTO-ALVEOLAR ABSCESS / ALVEOLAR ABSCESS )
Tender on
percussion
Will feel slightly
extruded from socket
Fever & regional
lymphadenitis71
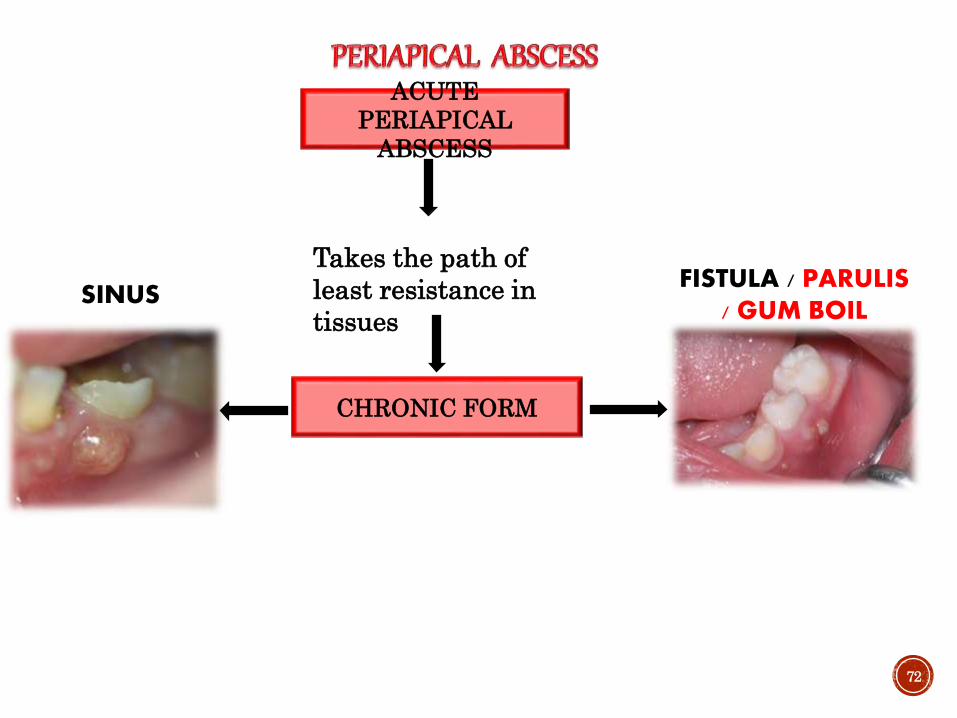
72
ACUTE
PERIAPICAL
ABSCESS
CHRONIC FORM
Takes the path of
least resistance in
tissuesSINUS
FISTULA / PARULIS / GUM BOIL
73
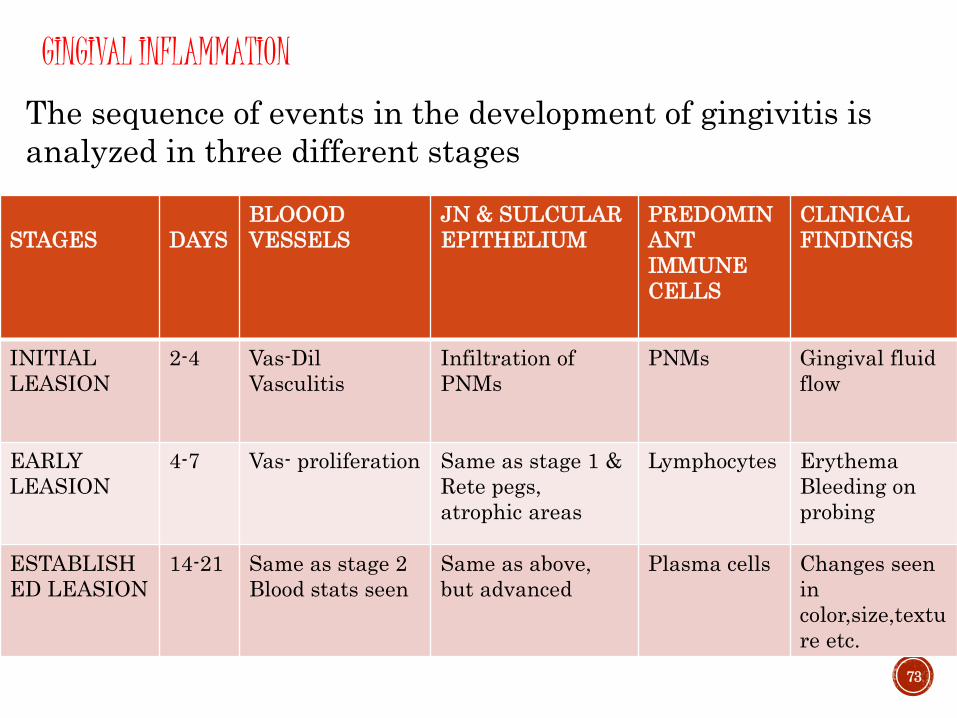
STAGES DAYS
BLOOOD
VESSELS
JN & SULCULAR
EPITHELIUM
PREDOMIN
ANT
IMMUNE
CELLS
CLINICAL
FINDINGS
INITIAL
LEASION
2-4 Vas-Dil
Vasculitis
Infiltration of
PNMs
PNMs Gingival fluid
flow
EARLY
LEASION
4-7 Vas- proliferation Same as stage 1 &
Rete pegs,
atrophic areas
Lymphocytes Erythema
Bleeding on
probing
ESTABLISH
ED LEASION
14-21 Same as stage 2
Blood stats seen
Same as above,
but advanced
Plasma cells Changes seen
in
color,size,textu
re etc.
The sequence of events in the development of gingivitis is
analyzed in three different stages
GINGIVAL INFLAMMATION
74
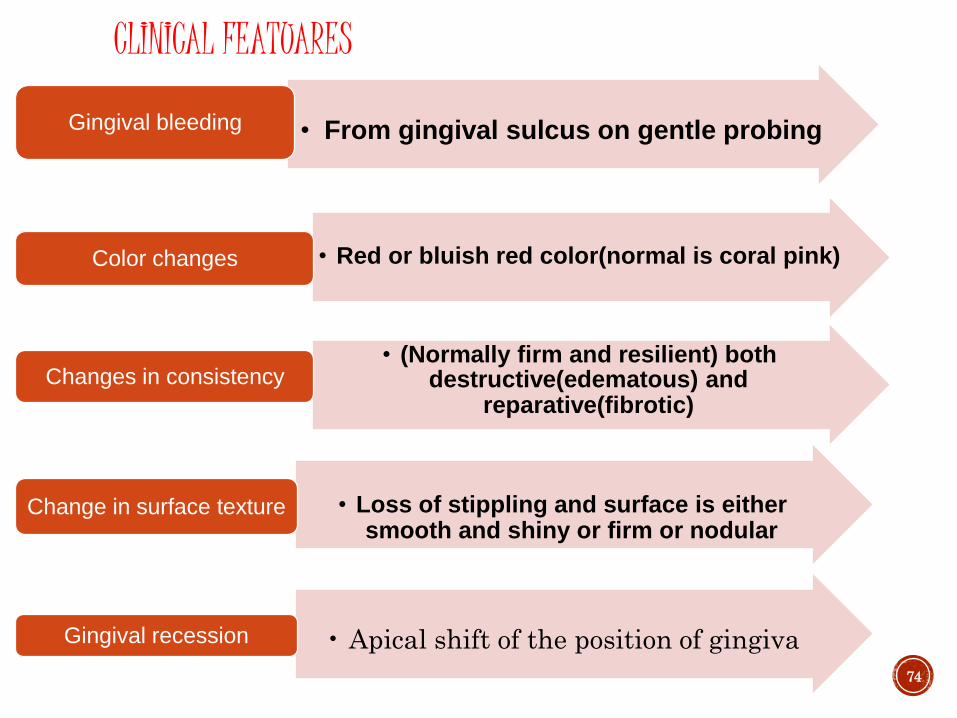
• From gingival sulcus on gentle probingGingival bleeding
• Red or bluish red color(normal is coral pink)Color changes
• (Normally firm and resilient) both destructive(edematous) and
reparative(fibrotic)
Changes in consistency
• Loss of stippling and surface is either smooth and shiny or firm or nodular
Change in surface texture
• Apical shift of the position of gingiva Gingival recession
CLINICAL FEATUARES
75
Conclusion………. Destroy, dilute and wash off any injurious agent & constitutes
the repair. Without inflammation, infections would go unchecked, wounds would never heal, and injured organs may remain as permanent decaying lesions.
In our day to day lives we come across many cases starting from gingivitis to oral cancer wherein inflammation exerts a direct or an indirect effect.
So understanding inflammation helps us to know the various vascular and cellular changes, mediators involved and therefore help us to evaluate the significance of various antibiotics and anti-inflammatory drugs that we do prescribe, for controlling the same.
Thank You . . .
“I choose a lazy person to do a hard job.Because a lazy person will find an easy way to do it.”
― Bill Gates
References……..
77
1. Essential pathology for dental students- Harsh Mohan -3rd edn.
2. Pathologic basis of disease- Robbins & Cotran – 7th edn .
3. Shafer’s text book of oral pathology – 5th edn.
4. Newman, Takei, Klokkevold, Carranza. Carranza’s clinical
periodontology. 12th ed, 2013

78
THANK YOU

















