INFECTION CONTROL IN THE ICU JOÃO MELO ALVES, MD LISBOA, PORTUGAL -- GENERAL ICU DIRECTOR: PROF. CHARLES SPRUNG, MD DEPARTMENT OF ANESTHESIOLOGY AND INTENSIVE CARE HEAD OF DEP.: PROF. CHARLES WEISSMAN, MD HADASSAH EIN KEREM UNIVERSITARY HOSPITAL JERUSALEM Ignaz Semmelweis (1818 – 1865)
Transcript
INFECTION CONTROL IN THE ICU
JOÃO MELO ALVES, MDLISBOA, PORTUGAL
--
GENERAL ICUDIRECTOR: PROF. CHARLES SPRUNG, MD
DEPARTMENT OF ANESTHESIOLOGY AND INTENSIVE CAREHEAD OF DEP.: PROF. CHARLES WEISSMAN, MD
HADASSAH EIN KEREM UNIVERSITARY HOSPITAL JERUSALEM
Ignaz Semmelweis (1818 – 1865)
21% PSSA0.4% MRSA
Prospective observational study in Canterbury NZ8 years (1998-2006); n=779
Huggan PJ et al. Intern Med J 2010 (40:2)
Sir Alexander Flemming (1881 – 1955)Nobel Prize 1945
ICUsFrikdin SK et al. Infect Dis Clin North Am 1997 (11:2)
<10% HOSPITAL BEDS
>20% NOSOCOMIAL INFECTIONS
EPIC ICRBSI – OR 1.73
Pneumonia – OR 1.91
Sepsis – 3.75
Vincent JL et al. JAMA 1995 (274:8)
EPIC I >1000 ICUs
>10000 patients
17 european countries
EPIC II
60% patients infected
Infection vs mortality OR 1.51
Leading cause of mortality in ICU
40% of all ICU expenditures
Indwelling catheters
Vincent JL et al. JAMA 2009 (302:21)
EPIC II >1000 ICUs
>14000 patients
Worldwide study – 75 countries
Philippe Eggimann, Didier Pittet. Infection control in the ICU. Chest 2001, 120 (6)
Philippe Eggimann, Didier Pittet. Infection control in the ICU. Chest 2001, 120 (6)
“IA: periodically assess knowledge of and adherence to guidelines for all personnel involved in the insertion and maintenance of intravascular catheters”
CDC 2011 Guidelines for the Prevention of Intravascular Catheter-Related Infections
Antibiotics control
Hand hygiene
Contact precautions
DecolonizationBathing
SOD/SDD
Nasal carriage
Device specific strategies
Antibiotics control
Hand hygiene
Contact precautions
DecolonizationBathing
SOD/SDD
Nasal carriage
Device specific strategies
A-LINES (vs. CVC)
BLOOD CULTURES & CRBSI
UTI IN THE UCI
ET & SPUTUM CULTURES
A-LINES (vs. CVC)
A-LINES (vs. CVC)
BLOOD CULTURES & CRBSI
UTI IN THE ICU
ET & SPUTUM CULTURES
A-Lines as source of BSI
49 studies - only one study MSBP vs sterile gloves
O’Horo JC et al. Crit Care Med 2014 (42:6)
IB: aseptic technique for insertion and care of intravascular catheters
IC: clean gloves, rather than sterile, for PVC, after skin antisepsis
IA: sterile gloves for arterial and CVC catheters
IB: maximal sterile barrier precautions (incl cap, mask, sterile gown, sterile gloves, sterile full body drape) for insertion of CVC, PiCC or guidewire exchange
CDC Prevention Intravascular Catheter Related infections 2011
A-Lines as source of BSI
49 studies, 222 BSI, >30000 catheters
1.26 /1000 cath-days
O’Horo JC et al. Crit Care Med 2014 (42:6)
Arterial CRBSI
Prospective cohortn=2500, 2949 catheters
Femoral vs Radial /1000 cath-days:Local: 3.02 vs 0.75BSI: 1.92 vs 0.25
Increased durationPoor aseptic technique on insertion
Lorente L et al. Crit Care 2006 (10)
Rates of CRBSI/1000 cath-days
AL 1.7 vs. CVC 2.7
PVC 0.5
PiCC 1.1 (inpatients = CVC)
PAC 3.7
Maki DG et al. Mayo Clin Proc 2006 (81:9)
106 ICU, >300000 cath-days
18 months – The Provonost checklist
Handwashing
MSBP
Clorhexidine-ethanol
Avoidance of femoral
Removal ASAP
7.7 1.4
Pronovost P at al. NEJM 2006 (355)
n=3154, 2y cohort of catheter care
incidence rate/1000 pt-days
Exit-site infection 9.23.3 (RR 0.36)
CRBSI 11.33.8 (RR 0.33)
VAP/VAT/CAUTI no change
Global NI 52.434.0
Eggimann P et al. Lancet 2000 (355)
Routine replacement has no role
More mechanical complications
No advantage in reducing CRBSI
Cobb DK et al. NEJM 1992 (327)Eyer S et al. Crit Care Med 1990 (18)
Direct vs guidewire techniques
Less likelihood of success
Longer to perform
Used more catheters
Required more punctures
Guidewire 82% vs direct 65% success
Beards SC et al. Anaesthesia 1994 (49)Mangar D et al. Anesth Analg 1993 (76)
Q3d, new place – 3 Q3d, guidewire – 6 Clinical indication, new place – 2 Clinical Indication, guidewire – 3 New sites increased mechanical complications
Cobb DK et al. NEJM 1992 (327:15)
CDC guidelines IB: do not routinely replace CVCs, PiCCs, HD caths,
PACs to prevent CR-infections (new place or guidewire)
II: do not remove CVC/PiCCs on the basis of fever alone. Use clinical judgment.
IB: use guidewire exchange to replace malfunctioning catheter if no evidence of infection is present
IB: do not use guidewire exchanges to replace suspected infected catheterCDC Prevention Intravascular Catheter Related infections 2011
REMOVAL Severe sepsis/shock Endocarditis or metastatic infection Suppurative thromboplebitis >72h persistent bacteremia under atb Specific pathogens (SA, enteococci, GNR, fungi,
mycobacterium)
SALVAGE – no role in ICU Uncomplicated CRBSI with long-term catheters Salvage therapy (e.g. antibiotic lock) Except specific pathogens (…)
MONITOR, DO NOT TREAT Positive tip, no clinical signs Positive CVC BC, negative peripheral
Staphylococcus aureus 25-32% BSI develop INFECTIVE ENDOCARDITIS TEE 5-7d after +BC >72h is an ominous sign
Abraham J et al. Am Heart J 2004 (147:3)Fowler VG Jr et al. J Am Coll Cardiol 1997 (30:4)
Sullenberger AL et al. J Heart Valve Dis 2005 (14:1)
URINARY TRACT INFECTIONS IN THE ICU
A-LINES (vs. CVC)
BLOOD CULTURES & CRBSI
UTI IN THE ICU
ET & SPUTUM CULTURES
When to treat?
<5% of bacteriuric cases bacteremia
Leading cause of nosocomial BSI 17% of all HA-BSI (lower proportion in ICU)
CA-urosepsis 10% mortality
Gould CV et al. Infect Control Hosp Epidemiol 2010 (31)
Diagnosis: cultures and symptoms
Asymptomatic CA-bacteriuria: ≥105 CFU/mL of uropathogenic bacteria Pyuria >10 WBC/uL has low sensitivity but >90% specificity – doesn’t make the diagnosis Cloudy appearance and foul smell are NOT correlated with bacteriuria
Bacteriuria: 3-10%/day of catheterization
Hooton TM et al. Clin Infect Dis 2010 (50:5)Nicolle LE. Infect Dis Clin North Am 2012 (26:1)
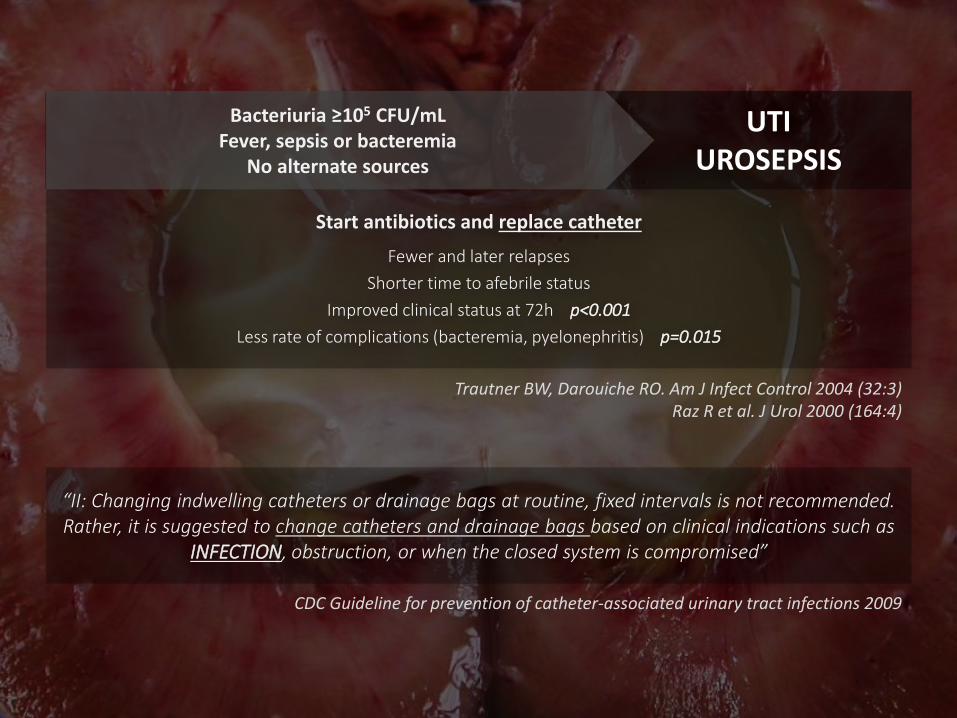
“II: Changing indwelling catheters or drainage bags at routine, fixed intervals is not recommended. Rather, it is suggested to change catheters and drainage bags based on clinical indications such as
INFECTION, obstruction, or when the closed system is compromised”
CDC Guideline for prevention of catheter-associated urinary tract infections 2009
Trautner BW, Darouiche RO. Am J Infect Control 2004 (32:3)Raz R et al. J Urol 2000 (164:4)
Start antibiotics and replace catheter
Fewer and later relapses
Shorter time to afebrile status
Improved clinical status at 72h p<0.001
Less rate of complications (bacteremia, pyelonephritis) p=0.015
UTIUROSEPSIS
Bacteriuria ≥105 CFU/mLFever, sepsis or bacteremia
No alternate sources
ENDOTRACHEAL TUBES & SPUTUM CULTURES
A-LINES (vs. CVC)
BLOOD CULTURES & CRBSI
UTI IN THE ICU
ET & SPUTUM CULTURES
Ventilator associated tracheobronchitis
Horan TC et al. CDC/NHSN surveillance definition. Am J Infect Control 2008 (36:5)
Fever>38ºC
No other recognizable source of infection
New/increased sputum production
Positive culture of tracheal aspirates
No radiographic infiltrate or evidence of pneumonia