63
Infection Control Practice in ICU

Infection Control Practice in ICU

• What is infection control
• Why is it important in ICU set up
• Basics of infection control prevention
• How do you set up an infection control program in your ICU
What is infection control
• Application of epidemiological principles for infection prevention and reduction
• We have an infection control program in a health care institution mainly to prevent patient acquiring nosocomial infections(Health-care associated infections)

What are hospital associated infections(HAI)? • Infections acquired by the patients while they are in the hospital or
Infections acquired by health care workers while working in the hospital
• Patient should not be incubating them on admission
• Usually appear after 48 hours
• If present on D1 and D2, they are taken as POA(Present On Admission)
• Patient may manifest signs and symptoms of HAI after they are discharged from the hospital

History of Infection control-Father of the Concept

• Ignaz Philipp Semmelweis( july,1818-August,1865)
• Hungarian obstetrician known as the “savior of mothers”,
• There were two maternity units at the Viennese hospital he worked. The First unit had an average maternal mortality rate due to puerperal fever of about 10% and second Clinic’s rate was considerably lower, averaging less than 4%
• women begged to be admitted to the second clinic due to the bad reputation of the first Clinic and some preferred to give births in streets but infection rates were low even in street births

• Semmelweise discovered crucial difference, the first clinic was attended to by medical students who did autopsies just before they came to the clinic while the second clinic was attended to by midwives who did not do autopsies
• He implemented a practice of mandating that his obstetric students wash their hands with “chlorinated lime solutions”
• Death rate became zero 2 months after this measure since the introduction of anatomical orientation in the unit

• Semmelweis’s hypothesis, that there was only one cause, that all that mattered was cleanliness, was extreme at the time, and was largely ignored, rejected or ridiculed.
• He was dismissed from the hospital for political reasons and harassed by the medical community in Vienna
• His contemporaries, including his wife, believed he was losing his mind, and in 1865 he was committed to an asylum. He died there of septicaemia only 14 days later, at age 47, possibly after being severely beaten by guards

Only after Pasteur, and Lister had produced more evidence of the germ theory and antiseptic techniques was the value of hand washing appreciated two decades later

Why is it necessary
Epidemiology of health care associated infections • One in 25 Patients End Up with Hospital-Acquired Infections, CDC
Warns (April 09, 2014)
• Of every 100 hospitalized patients at any given time, 7 in developed and 10 in developing countries will acquire at least one health care-associated infection(WHO)(5-10%)
• In high-income countries, approximately 30% of patients ICUs are affected by at least one HAI
• In low- and middle-income countries the frequency of ICU-acquired infection is at least 2 to 3 fold higher than this
• Newborns are at higher risk of acquiring health care-associated infection in developing countries, with infection rates 3 to 20 times higher than in high-income countries.
Source: WHO

This population at a higher risk?
• Sickest of the sick(multiple diagnosis, multiple organ failure,immunocompromized,severe sepsis,trauma)
• Restricted to the bed
• Nutritional status low
• Obdunted-low glassglow coma scale
• Underlying associated conditions
• Multiple antibiotic usage

ICU care is more invasive
• Having invasive devices-Central venous catheters, Urinary catheters, invasive mechanical ventilation, tracheostomies, stomas-multiple portals of entries
• On IV medication, total parenteral nutrition, multiple blood transfusions
• Long stays

Acquisition of a HAI
Infected patient Microorganism Non infected patient Direct transmission Indirect transmission

Patient, Patient care zone and Health care zone • Patient
Patient and the and anything attached to the patient
E.G. ECG leads,IV line
• Patient care zone
patient and his/her immediate surrounding
E.G. bed rails, bed linen, infusion tubing
• Health care zone
The ward or the special unit patient is being treated

Patient care zone and Health care zone

• When a patient is being treated in an ICU setting for a while invariably they get colonized with resistant microorganisms and they shed them to the patient care zone and health care zone in greater/ lesser quantities
• Health care worker and patient care instrument are the carriers that move them between patient and patient zones

If it is so, how can we prevent Hospital Associated Infections?
Develop a safety culture in our working environment
Bear this question in the mind
• Is our work surrounding safe to our patient and to us ?
If not
• How to change our attitudes and behavior towards a safety culture - through standard precautions
And
• Break the chain of infection

What are standard precautions
A set of guidelines which should be followed to help to prevent the transmission of HAIs in hospitals, which should be followed by all health care providers at all times when attending to all patients regardless of their diagnosis and presumed infectious status

• They are the basic level of infection control precautions which are to be used as a minimum ,in the care of all patients


What are standard precautions
• Hand hygiene
• Use of Personal Protective Equipment (PPE)
• Safe injection practices
• Safe handling of potentially contaminated equipment or surfaces in the patient environment
Cleaning and proper handling of equipment
Environmental cleaning
Proper handling and cleaning of linen
Proper disposal of waste
• Respiratory hygiene and cough etiquette

Hand Hygiene
•Accepted by the whole world as the most effective way in reducing health care-associated infections
• It is not optional but mandatory
•Master this and it is a sign of respect and professionalism

Effective Hand Washing

Simple infrastructure development
• Use liquid soap or small pieces of bar soap
• A source of running water
• Hand drying facilities-single use towels
Or
• A bottle of alcohol based hand rub

My Five Moments (WHO/CDC)
• Before touching a patient
• Before a sterile procedure
• After touching a patient
• After body fluid contact
• After touching patient surrounding

• 1 BEFORE PATIENT CONTACT
WHEN? Clean your hands before touching a patient when approaching him or her WHY? To protect the patient against harmful germs carried on your hands
• 2 BEFORE AN ASEPTIC TASK
WHEN? Clean your hands immediately before any aseptic task WHY? To protect the patient against harmful germs, including the patient’s own germs, entering his or her body
• 3 AFTER BODY FLUID EXPOSURE RISK
WHEN? Clean your hands immediately after an exposure risk to body fluids (and after glove removal) WHY? To protect yourself and the health-care environment from harmful patient germs
• 4 AFTER PATIENT CONTACT
WHEN? Clean your hands after touching a patient and his or her immediate surroundings when leaving WHY? To protect yourself and the health-care environment from harmful patient germs
• 5 AFTER CONTACT WITH PATIENT SURROUNDINGS
WHEN? Clean your hands after touching any object or furniture in the patient’s immediate surroundings, when leaving - even without touching the patient WHY? To protect yourself and the health-care environment from harmful patient germs


7 Steps in hand washing
•Practice !practice! and re-practice!
•Until it becomes a routine



Alcohol Hand Rub
• Can be used as an alternative to washing with soap and water
• Can use at point of care
• Less time consuming
• Does not require drying with a towel
• Available as in-house preparation or commercial products
• Do not use for visibly soiled hands
• Hand washing is the preferred method for spore forming bacteria for example Clostridium difficile



Additional precautions/transmission based precautions
• Needed for instances transmission is not completely interrupted using standard precautions
• Transmission-based precautions are taken while ensuring standard precautions are maintained
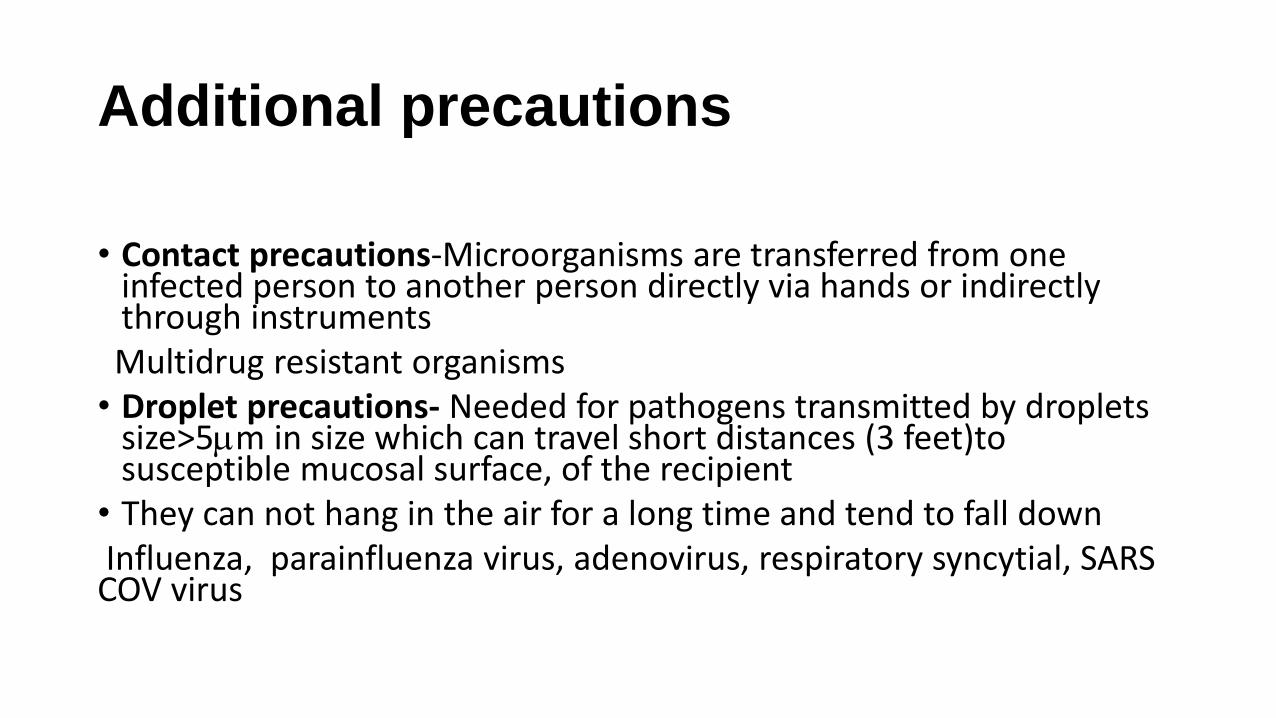
Additional precautions
• Contact precautions-Microorganisms are transferred from one
infected person to another person directly via hands or indirectly through instruments
Multidrug resistant organisms • Droplet precautions- Needed for pathogens transmitted by droplets
size>5m in size which can travel short distances (3 feet)to susceptible mucosal surface, of the recipient
• They can not hang in the air for a long time and tend to fall down Influenza, parainfluenza virus, adenovirus, respiratory syncytial, SARS COV virus

Air-born precautions
• Airborne transmission occurs by dissemination of either airborne droplet nuclei or small particles in the respirable size range (<5 m) containing infectious agents that remain infective over time and distance
Open pulmonary cases of Mycobacterum tuberculosis infection, chicken pox ,Measles, aerosol generating procedures in patients needing droplet transmission
Isolation room for 3 ICU beds is recommended

How do you set up an infection control program in your ICU?
Director Infecti
on control team
Microbiologist
Infection control Medical officer
Infection Control nursing
officers
Liaison nurses of
wards and unit

Have a system in operation for surveillance
Surveillance of HAIs/MDROs
• Def:The continuing scrutiny of all aspects of occurrence and spread of a disease that are pertinent to effective control (Benson, 1990)
• Shows the trends
• can recognize any unusual level or change in level of incidence and the existence or impending spread of an outbreak
• able assess the efficacy of the regular preventive measures in use

How to do
• Daily scrutiny of lab reports
• Maintaining a HAI chart by ward/ICU staff
• Prevalence surveys- all patients are visited on one occasion only- can do an annual survey to supplement the other methods of survey

HAI surveillance
• Surveillance criteria should be introduced with working definitions that suit our setting
• To calculate rates standard denominators should be introduced
• Education of all categories of staff-Health care staff get opportunities to detect events:
fever spikes in the QHT, signs f infection at the cannula site or in the surgical sites, new shadows in the chest X-ray
Need to identify as well as report or record it as a HAI

Calculating rates
•SSI rates per 1000 theatre cases
•VAP rates per 1000 ventilator days
•CLABSI rates per 1000 line days
•CAUTI rates per 1000 catheter days

Written guidelines/policies
• Environment cleaning
• Spill management
• Instrument cleaning
• Sterilization/disinfection
• Isolation
• Risk assessment and use of PPE
• Practice of hand hygiene
• Waste disposal
• Antibiotic use

Sterile procedures • CVC insertion
• Urinary catheter insertion
• Ventilation asepsis/procedure
• Tacheostomy care
• Care of IC tubes and stomas
• Collection of blood cultures
• Doing a lumbar puncture

Bundle approach
What is an Infection Control Care bundle?
• A set of evidence based practices that each individually improve patient outcome which should be performed for every patient
• When performed collectively, reliably and continuously, have been proven to improve patient outcome
• The science behind the bundle is so well established that it should be considered standard of care.
• Bundles require “all or none” approach rather than piecemeal application.

• Prevention of central line infections (CLABSI)
• Prevention of ventilator-associated pneumonia (VAP)
• Prevention of catheter associated UTI’s (CAUTI)
• 3.Prevention of surgical site infection (SSI)

CA-UTI Prevention Bundle
• Use urethral catheters only when necessary.
• Catheter inserters should be educated and competent.
• Use aseptic technique for catheter insertion and manipulation.
• Use a closed drainage system.
• Require a urinary catheter insertion indication/order and
consider using an administrative urinary catheter “stop
order” to limit inappropriate catheterization.
• PREVENTION POSSIBILITY: 20%-70%

Monitoring process to see whether the guidelines are implemented • Cleaning chart
• Sterilization chart
• Instrument cleaning check list
• Tracheostomy care checklist
• CVC maintenance check list
Audits • The key component of clinical audit is that performance is reviewed
(or audited) to ensure that what should be done is being done, and if not it provides a framework to enable improvements to be made.
The practice is compared with the standard and suggest changes for improvement

1. Identify problem or
issue
2. Set criteria & standards
3. Observe practice/
data collection
4. Compare performance
with criteria & standards
5. Implementing
change
Audit cycle

You can start with hand hygiene audits
• permissions need to be taken from Hospital administration, Consultant in charge of the unit, Unit Sister Etc
• Should not argue or advice on practices of HCWs during the audit sessions

Audit rules
• An auditor should record only observations seen by the auditor. Should not imagine or guess the actions of HCWs
• An auditor should not attempt to audit health care workers attending an emergency.
• Try to avoid bias upon entering the data on a form

• Hand Hygiene Action needs to be entered either as rub, wash or missed in the form
• Each Audit Session needs to be observed for at least a period of 20 minutes and should not exceed 20 observations per session
• The Observer may follow a single health care worker till his/her actions are completed or may follow several health care workers together. However selection should be random



Calculating rates
• Compliance rates
Number of Opportunities performed x 100
Number of Opportunities existed
You can evaluate and compare it as health care workers, as moment wise as well
E.G. Number of Opportunities performed by nursing staff x 100
Number of Opportunities existed for nursing staff

Hand Hygiene audit-ICU
• Date:10.04.2014
Adequate Inadequate Not available
Availability of running water Yes
Availability of soap Yes
Availability of tissue/hand towel Yes
Alcohol hand rub Yes
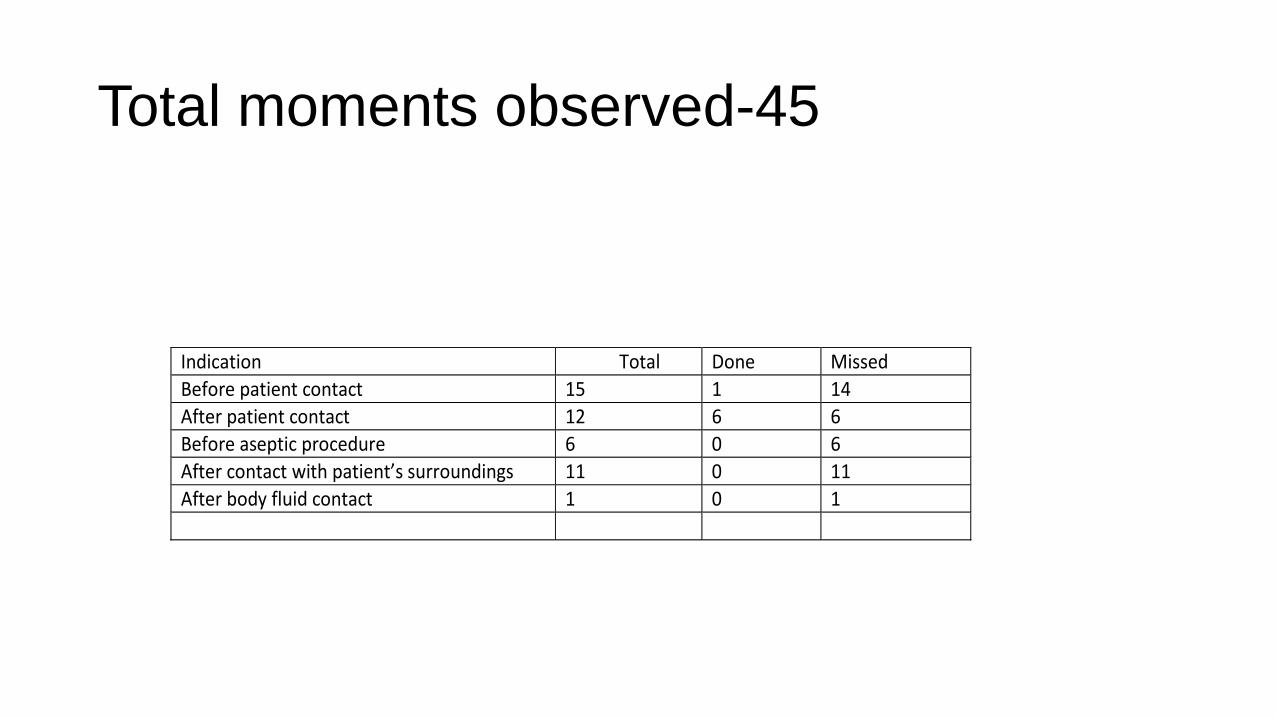
Total moments observed-45
Indication Total Done Missed
Before patient contact 15 1 14
After patient contact 12 6 6
Before aseptic procedure 6 0 6
After contact with patient’s surroundings 11 0 11
After body fluid contact 1 0 1

Missed by staff category
Total Done Missed Percentage
Doctors 7 1 6 14% Benchmark
Nursing officers 38 6 32 16% Benchmark

• Any questions?
Thank you
![Fungal infection in ICU patientshksccm.org/.../Fungal_infection_in_ICU_patients.pdffungal infection (IFI) in critically ill patients[1] •In recent years, Invasive aspergillosishas](https://static.documents.pub/doc/80x56/5eda128fb3745412b570b6ba/fungal-infection-in-icu-fungal-infection-ifi-in-critically-ill-patients1-ain.jpg)
















