38
INFECTION PREVENTION MANUAL October , 2012 Boston University Henry M. Goldman School of Dental Medicine

INFECTION PREVENTION MANUAL
O c t o b e r , 2 0 1 2
Boston University
Henry M. Goldman
School of Dental
Medicine

INFECTION PREVENTION MANUAL 2012
1 | P a g e
I) PURPOSE OF THE INFECTION PREVENTION MANUAL
This manual describes the Infection Prevention program of the Goldman School of Dental Medicine (GSDM). It presents preventive measures required to reduce the risk of injury and infection to patients, students, employees and staff in the dental health-care setting. These preventive measures fall into two categories. The first are evidenced based policies and procedures designed to prevent the transmission of health-care related infections. The second category of preventive measures – called the Exposure Control Plan - are federally mandated work standards designed to prevent on-the-job exposures of health-care workers to blood-borne pathogens.
The Center for Disease Control and Prevention (CDC ) has issued Guidelines for Infection Control in Dental Health-Care Settings. Those guidelines form the basis for many of the policies and procedures contained in the GSDM Infection Prevention Manual. The Occupational Safety and Health Administration (OSHA) institutes and enforces regulations to promote safe work practices in an effort to minimize the incidence of work-related illness and injury. OSHA has enacted the Blood borne Pathogens Standard (29 CFR 1910.1030) to "reduce occupational exposure to Hepatitis B Virus (HBV), Human Immunodeficiency Virus (HIV) and other blood borne pathogens" that health-care workers may encounter on the job The Exposure Control Plan found in this manual is based on the OSHA Standard. As required by the Federal Needle stick Safety and Prevention Act (November, 2000), revisions to the Standard became effective on April 18, 2001. The revisions focus on developments in exposure control technology and require that Exposure Control Plans reflect how employers comply with the revisions.
The Henry M. Goldman School of Dental Medicine believes that the following principles must be observed by employees and students when working with blood or body fluids:
All blood and certain body fluids are considered to be potentially infected with blood borne pathogens.
All used needles and other sharps are considered to be potentially infectious.
All exposure to blood and body fluids should be minimized.
The purpose of the Henry M. Goldman School of Dental Medicine’s Exposure Control Plan is to describe the school-wide program designed to eliminate or minimize exposure to blood borne pathogens.
The OBJECTIVES of this plan are:
To protect patients, employees, staff and students from infection by blood borne pathogens and pathogens transmitted by certain other bodily fluids.
To assure that at least annually a work group (which will include at least one front-line clinician/dentist in training) is convened to assess for possible use, safety features and

INFECTION PREVENTION MANUAL 2012
2 | P a g e
systems for sharp dental instruments as they are brought to the market, and to assure that a record of their deliberations and recommendations is maintained.
To assure appropriate follow-up care to any GSDM employee, staff member, or student
who experiences an exposure incident with blood or body fluids. Incidents are reported
by the medical center Office of Environmental Medicine (OEM) to the Office of Clinical
Services where documentation is maintained.
Infection prevention procedures
A) Simulation Learning Environment
"Attire and personal protective equipment (PPE) worn in the preclinical setting should prepare students
for the clinic. Thus, students and faculty are required to wear scrubs, shoes that cover the top of the
foot (no sandals or open toed shoes may be worn for safety reasons) and PPE reflective of:
Gloves: GSDM provides non-latex gloves within the Simulation Learning Environment.
Protective Gowns: GSDM provides disposable gowns for students and laundered blue
coats for faculty members.
Eye protection: GSDM provides the following forms of eye protection (deemed
acceptable by OSHA and CDC),: Face shields, Surgical goggles/glasses, side shields which
can be attached to prescription glasses. Users may purchase their own safety eye
protection.
Mask: (dome/ear loop)
B) Patient Care Environment (All GSDM clinical areas)
Before Treatment begins
Operatory preparation:
Prior to seating a patient, the operatory must be thoroughly cleaned, disinfected. Appropriate
surfaces, clinical contact surfaces, must be protected with barriers. The following protocol is to
be followed:
INFECTION PREVENTION MANUAL 2012
3 | P a g e
1) Hand hygiene
Proper hand hygiene is probably the single most effective barrier to infection. Hands must be
thoroughly and properly sanitized:
At the beginning and end of each appointment
Before gloving and after de-gloving.
Soap and water wash –
Remove all jewelry from hands and arms.
Rinse hands under cool running water and apply antimicrobial soap, lather well.
There is a 20 second minimum washing time for hands and fingers.
Work soap around fingers and nails. Do not use a hard bristled scrub brush because it
may cause abrasions.
Rinse thoroughly with cool running water (hot water opens pores and dilates
capillaries).
Dry hands with paper towels and use the towel to turn off the faucet.
Cover cuts and abrasions with Band-Aids or finger cot until fully healed.
Alcohol-based Hand Rub/Rinse (include emollients to protect skin from drying)
If hands are not visibly soiled or sticky, they may be sanitized with an alcohol based
hand rub.
Apply enough product to wet both hands from finger tips to wrists.
Rub in vigorously until dry [about 20 seconds]
Moisturizers can be useful in counteracting the effects of dryness caused by frequent hand
hygiene. Be advised, petroleum based products, including some moisturizers, can weaken latex
gloves and increase permeability. For that reason, lotions that contain petroleum or other oil
emollients should only be used at the end of the work day.

INFECTION PREVENTION MANUAL 2012
4 | P a g e
Wear gloves and all personal protective equipment defined to minimize inhalation and
exposure to chemicals in the disinfectant during operatory preparation. (see #5)
2) Cleaning, disinfecting, and protecting clinical contact surfaces
Liquid disinfectant, a "hospital disinfectant" that has a label claim for mycobactericidal (e.g.,
tuberculocidal) activity, needs to be applied to all clinical contact surfaces prior to seating the
patient.
Example of a"hospital disinfectant" that has a
label claim for mycobactericidal (e.g., tuberculocidal) activity.
-Cleaning: prior to surface disinfection, clean surfaces by wetting surfaces with approved
liquid disinfectant or germicidal disposable wipe, and allowing surfaces to remain wet for 15
seconds; then wipe clean with a clean paper towel. Repeat as necessary, until surface appears
clean. Discard paper towel.
-Disinfection- after properly cleaning surface, reapply approved liquid disinfectant by
spraying surface or using a germicidal disposable wipe. Allow surface to remain wet for 3
minutes, then wipe dry with a clean paper towel. When finished, discard paper towel.
- Protecting clinical contact surfaces- Use surface barriers to protect all clinical contact
surfaces, particularly those that are difficult to clean, and always remember to discard the
barrier after each patient.

INFECTION PREVENTION MANUAL 2012
5 | P a g e
Clinical Contact Surfaces: Clinical contact surfaces can be directly contaminated from patient materials either by direct spray or spatter generated during dental procedures or by contact with the dental health care provider's gloved hands. These surfaces can subsequently contaminate other instruments, devices, hands, or gloves. All clinical contact surfaces must be covered with a barrier. Examples of such surfaces include: Light handles, Switches, Dental radiograph equipment Dental chair Operator chair Dental chairside computers, Signature pad Reusable containers of dental materials, Drawer handles, Faucet handles, Countertops,(liquid disinfectant only, no barrier) Pens, Door- knobs. Microscopes, CEREC unit, Impregum dispenser (pentamix)
INFECTION PREVENTION MANUAL 2012
6 | P a g e
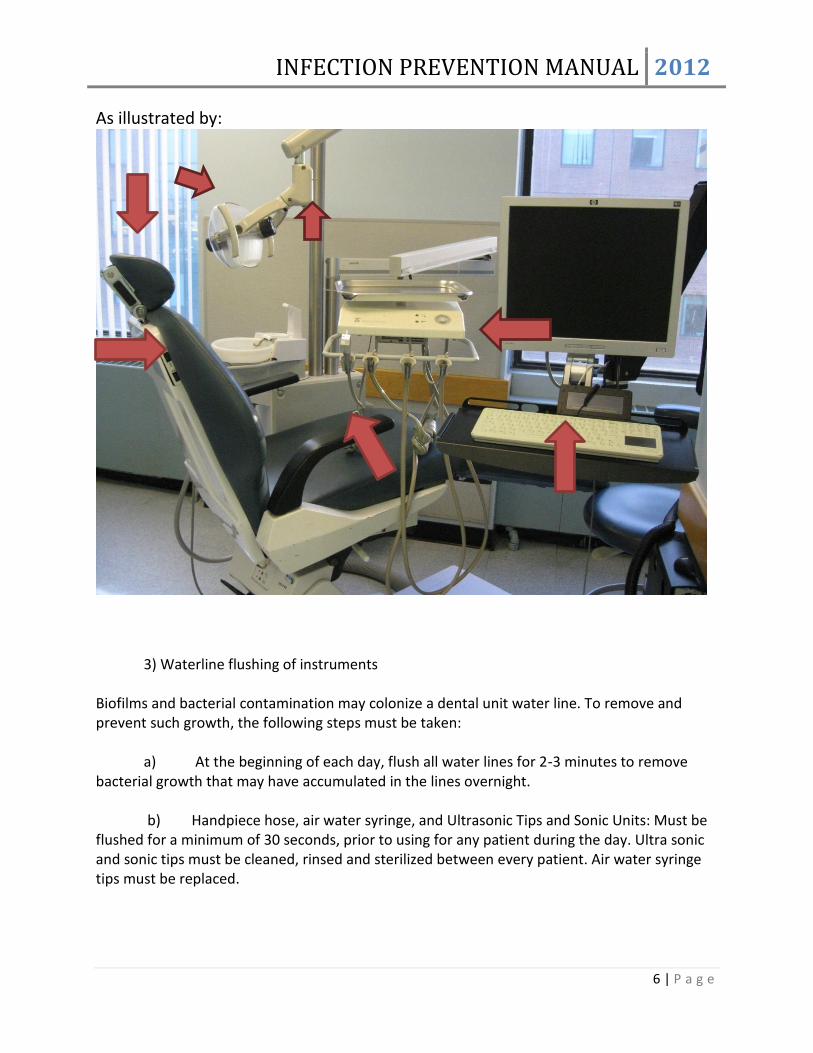
As illustrated by:
3) Waterline flushing of instruments
Biofilms and bacterial contamination may colonize a dental unit water line. To remove and prevent such growth, the following steps must be taken:
a) At the beginning of each day, flush all water lines for 2-3 minutes to remove bacterial growth that may have accumulated in the lines overnight.
b) Handpiece hose, air water syringe, and Ultrasonic Tips and Sonic Units: Must be flushed for a minimum of 30 seconds, prior to using for any patient during the day. Ultra sonic and sonic tips must be cleaned, rinsed and sterilized between every patient. Air water syringe tips must be replaced.
INFECTION PREVENTION MANUAL 2012
7 | P a g e
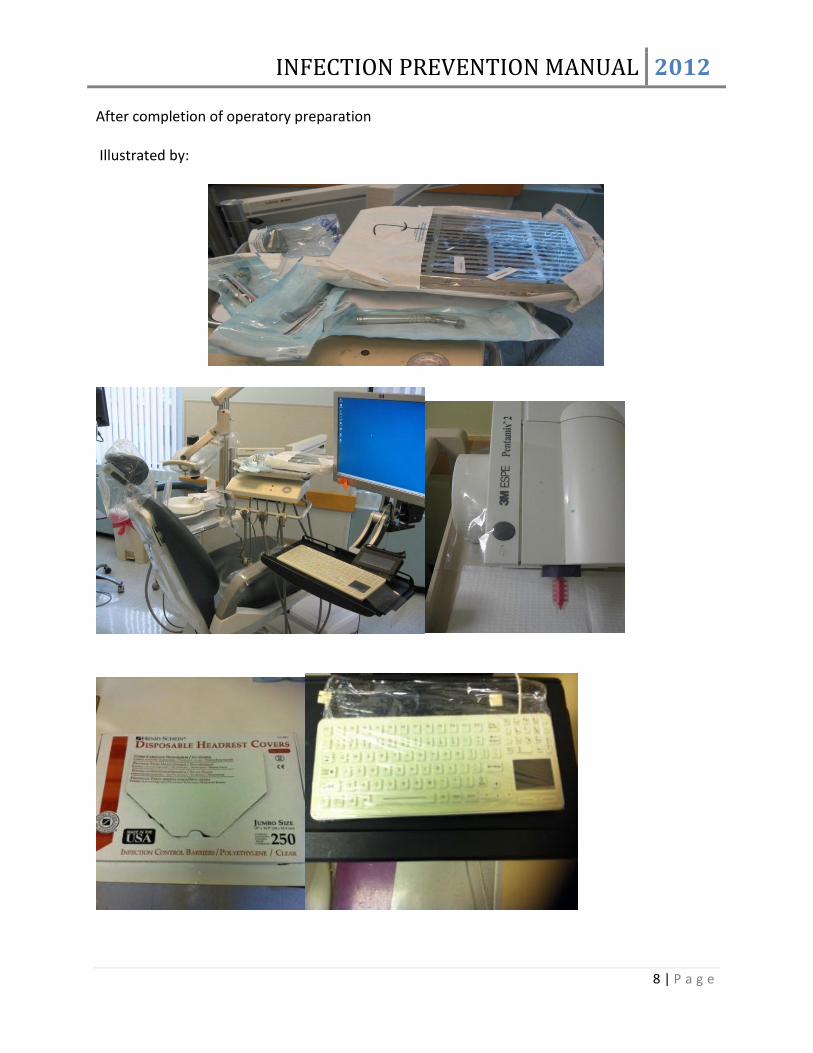
4) Set-up operatory for the session’s procedure Arrange unopened sterile cassettes, burs and hand -pieces on the bracket tray and/or shelf. For pre-doctoral students cassettes, burs and hand pieces are to be opened in front of Pre-Doctoral faculty giving the start, or staff to insure sterility. Pre-doctoral faculty will sign attendance sheet verifying compliance. Be prepared: set up all materials, instruments, burs and equipment before starting the procedure. In this way, you limit the number of visits to the dispensary (time management) Aseptic Technique: Once sterile packages have been opened and the procedure has begun, it is critical to follow the basic principles of aseptic technique to prevent the introduction of pathogens or contaminants, that may harm the patient, into the treatment field:
- The field and opened instruments may not be left unattended - Do not introduce non-sterile/clean items (e.g.chart, phone) into the field - Do not pass non-sterile items over the field - Assure that anyone who joins the procedure underway, has performed hand hygiene and dons fresh gloves/gear - Any item that falls to the floor, or becomes contaminated may not be returned to the field.
Burs: The majority of burs are sterilized pre-packaged single use only, disposable burs. GSDM bur blocks will be provided at the dispensary windows in sterilized bags together with restorative instrument cassettes upon request. All carbide burs, other than finishing burs, are considered "single use." A variety of carbide burs are stocked in the dispensary and may be requested for clinical use. No carbide bur other than those provided through the dispensary may be used in the treatment centers. All carbide burs, other than finishing burs, must be discarded in the "Sharps Container" at the end of a clinic session. GSDM bur blocks must be returned to the dispensary at the end of each session.
High-speed and low-speed hand pieces: All components of all handpieces must be sterilized at the conclusion of each patient use. All student hand pieces must be picked up after sterilization at the dispensary window at the beginning of the clinic session.
Although a student may not intend to use his/her hand-pieces during a particular session, a cassette will not be given to a student unless it is accompanied by the student's sterile hand- pieces.
INFECTION PREVENTION MANUAL 2012
8 | P a g e
After completion of operatory preparation Illustrated by:
INFECTION PREVENTION MANUAL 2012
9 | P a g e
5) Personal Protective equipment When there is danger of exposure to hazardous material, Personal Protective Equipment (PPE) must be used. The school provides, at no cost to dental health care workers, the Personal Protective Equipment that they need to protect themselves against exposure incidents. This equipment includes, but is not limited to the following:
Personal Protective Equipment (PPE): Garment and physical barriers to be worn as a standard precaution to prevent cross-contamination, work-related injuries and to avoid contact with chemical substances used to disinfect surfaces. Proper PPE/clinical attire includes:
Gloves: GSDM provides latex and non-latex gloves at all clinical and lab areas. - Gloves must be worn during operatory disinfection. They must be disposed of and replaced
with a new pair of gloves prior to handling sterile instruments or disposable barriers and
supplies.
- Gloves are to be worn during all instances of patient care - Wear a new pair of gloves for each patient, remove them promptly after use, and wash hands immediately to avoid transfer of microorganisms to other patients or environments. - Remove gloves that are torn, cut or punctured as soon as feasible and wash hands before re-gloving. -Never wash gloves during use, or for reuse; if indicated, always replace with a new pair of gloves. - Always remove gloves and wash hands prior to leaving the operatory. Re-glove as necessary.
Jewelry-Some studies have indicated that skin under a hand ring will be more heavily colonized with bacteria than comparable areas without a ring. Hand rings can also make donning gloves more difficult, and can cause gloves to tear more easily. Rings should not be worn while treating patients.
Protective Gowns: GSDM provides disposable gowns for students and laundered blue coats for faculty members. - disposable gowns must be worn during disinfection of the operatory and discarded
prior to placement of clean barriers and disposable supplies - Protective Gowns must be worn at all times in the clinical areas (operatories) - Protective Gowns may not be worn outside of the clinical areas of the treatment
center (past the doorway entrance to the treatment area) - A new Protective Gown is worn for each patient. Faculty should wear a disposable
gown if contamination is expected. - Protective Gowns are worn inside treatment and Lab areas only. - Protective Gowns must be changed when visibly soiled.
INFECTION PREVENTION MANUAL 2012
10 | P a g e
Eye protection: As defined by OSHA and CDC, the following are acceptable forms of eye
protection: Face shields, Surgical goggles/glasses, Prescription glasses with side shields
- Eyewear should be disinfected at the beginning and end of each appointment
- Eye protection is required during all patient care events and lab procedures
- Eye protection must be used when providing care using a dental microscope
Patient must wear protective eyewear when receiving dental care or examinations. Reusable
eye protection for patients must be disinfected between patient uses.
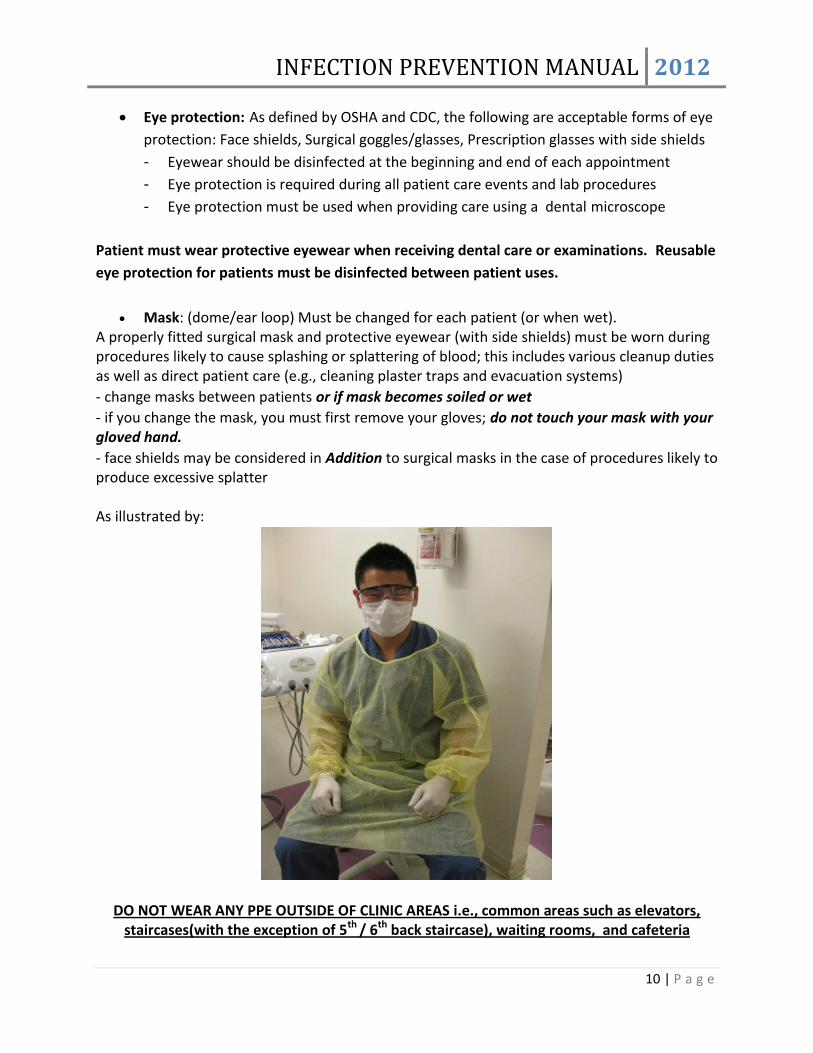
Mask: (dome/ear loop) Must be changed for each patient (or when wet). A properly fitted surgical mask and protective eyewear (with side shields) must be worn during procedures likely to cause splashing or splattering of blood; this includes various cleanup duties as well as direct patient care (e.g., cleaning plaster traps and evacuation systems)
- change masks between patients or if mask becomes soiled or wet
- if you change the mask, you must first remove your gloves; do not touch your mask with your gloved hand.
- face shields may be considered in Addition to surgical masks in the case of procedures likely to produce excessive splatter As illustrated by:
DO NOT WEAR ANY PPE OUTSIDE OF CLINIC AREAS i.e., common areas such as elevators, staircases(with the exception of 5th / 6th back staircase), waiting rooms, and cafeteria
INFECTION PREVENTION MANUAL 2012
11 | P a g e
During patient care USE AND CARE OF SHARP INSTRUMENTS AND NEEDLES: 1. Used sharp items (needles, scalpel blades, and other sharp instruments) should be considered “potentially infectious” and must be handled with extraordinary care to prevent unintentional injuries. 2. After use, disposable syringes and needles, scalpel blades, and other sharp items must be discarded into puncture-resistant containers located as close as practical to the area in which they were used.
To prevent accidental need stick injury, used needles should never be recapped or otherwise manipulated by using both hands, or any other technique that involves directing the point of a needle toward any part of the body. A one-handed technique with a mechanical device designed for holding the needle cap to facilitate one-handed recapping could be used for recapping needles between uses and before disposal. Dental Health Care Workers should never bend or break needles before disposal because this practice requires unnecessary manipulation. Before attempting to remove needles from non-disposable aspirating syringes, providers should recap them to prevent injuries. For procedures involving multiple injections with a single needle, the practitioner should recap the needle between injections by using a one-handed technique with a mechanical device designed for holding the needle cap to facilitate one-handed recapping. Passing a syringe with an unsheathed needle should be avoided because of the potential for injury. Consistent with CDC guidelines, GSDM continually evaluates new safety devices as they become available. Reports of these evaluations are available in the Office of Clinical Services. Local Anesthetic Armamentarium Use a sterile syringe, a new disposable needle, and new anesthetic solutions for every patient. Multidose vials are not used in the GSDM treatment centers. At all times avoid operator exposure to contaminated sharps. Disposable needles should not be purposely bent or broken; removed from disposable syringes; or otherwise manipulated by hand after use. Do not leave the syringe on the bracket tray with the needle hanging off the side.
INFECTION PREVENTION MANUAL 2012
12 | P a g e
DECONTAMINATION OF LABORATORY SUPPLIES AND MATERIALS:
Blood and saliva should be thoroughly and carefully cleaned from laboratory supplies and materials that have been used in the mouth, (e.g., impression materials, bite registration), especially before polishing and grinding intra-oral devices. Be sure to use a dedicated, clinical sink (cuspidor) decontamination may not be performed in hand washing sinks.
Materials, impressions, and intra-oral appliances should be cleaned and disinfected before being handled, adjusted, or sent to a dental laboratory. These items should also be cleaned and disinfected when returned from the dental laboratory and before placement in the patient's mouth. Use a dedicated, clinical sink, decontamination/disinfection may not be performed in hand washing sinks. Because of the ever-increasing variety of dental materials used intra-orally, DHCWs are advised to consult with manufacturers as to the stability of specific materials relative to disinfection procedures. A chemical germicide that is registered with the EPA as a "hospital disinfectant" that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, is preferred..
Communication between a dental office and a dental laboratory with regard to handling and decontamination of supplies and materials is of the utmost importance. Laboratory Asepsis and Disinfection of Impression Materials Clinic Protocol For safety reasons, NO laboratory work is to be performed by students outside of GSDM clinics and laboratories. All impressions and bite registrations must be thoroughly rinsed with cold running tap water as soon as they are removed from the mouth to remove saliva, blood, and debris. They must be disinfected using the appropriate techniques described below before they leave the operatory to be poured in plaster or stone, or sent to the laboratory. A dedicated sink,cuspidor, must be used for this purpose. Decontamination/disinfection may not be performed in a hand washing sink. Nature of Material/Method of Disinfection: Impression compound: Rinse under cold water. Spray thoroughly with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and place in an airtight and leak-proof plastic bag for 10 minutes. Rinse again with cold water. Dry and pour. Alginate impressions: Rinse, gently tap away excess water, spray with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, activity, and place
INFECTION PREVENTION MANUAL 2012
13 | P a g e
while still wet into an airtight and leak-proof plastic bag for 10 minutes. Do NOT allow to dry. Remove, rinse, and pour immediately. Reusable trays must be sterilized. Polysulfide rubber impressions: Rinse thoroughly and dry. Spray thoroughly with “hospital disinfectant” and that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and place in an airtight and leak-proof plastic bag for 10 minutes. Rinse, dry, and pour within 30 minutes to preserve dimensional stability. Polyvinyl siloxane impressions; Rinse. Spray thoroughly with a “hospital disinfectant” and that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and place in an airtight and leak-proof plastic bag for 10 minutes. Rinse again and either send to laboratory or pour at your convenience. Polyethers impressions: Rinse thoroughly with cold water and blow dry. Spray thoroughly with “hospital disinfectant” and that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and place in an airtight and leak-proof plastic bag for 10 minutes. Rinse well with cold water. Air dry for 30 minutes. Pour at your convenience. For all intra-oral devices before delivery (new or repaired dentures, night guards, retainers, frameworks): Thoroughly clean. Rinse well. All prosthetic devices and appliances that are taken from the patient’s mouth: frameworks, partial dentures, provisional dentures, complete dentures, temporary crowns and bridges, permanent crowns and bridges, retainers, nightguards, etc; must be rinsed immediately under running tap water. Spray thoroughly, with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity and place in an airtight and leak-proof plastic bag for 10 minutes. Only new prostheses (i.e., those that have NEVER been inserted) should be trimmed, pumiced, and polished in the 6th floor student laboratory. All other prostheses should be trimmed or finished chair-side with burs and rubber points (black, green, yellow) that are then dry heat sterilized. Equipment such as articulators, alcohol torches, shade guides, mold guides must be disinfected after use. The white handled Buffalo knife can be autoclaved.
After Patient Treatment Sterilization: All reusable instruments, including all hand-piece components, that can be sterilized, must be sterilized after every patient appointment. Instruments: Wear gloves and protective eyewear, to rinse (not scrub) instruments in order to remove blood, tissue, cement, wax and amalgam (remove from the carrier and place in labeled containers). Rinse instruments in dedicated instrument processing sinks. Instrument

INFECTION PREVENTION MANUAL 2012
14 | P a g e
decontamination may not be performed in a hand washing sinks. Carefully dispose of sharps (needles, scalpel blades, etc.) in the puncture proof needle boxes located in every operatory. After instruments have been rinsed and packaged for sterilization, the protective gown may be removed and discarded. While still in the operatory and wearing gloves, fit the contaminated instruments into the cassette so that none are sticking outside of the kit. If not done correctly, this can result in puncture wounds. Close and lock the cassette. Wrap soiled cassette in a new sterilization pouch, secure and place a BIOHAZARD label, remove your gloves, wash hands and carry cassette package to Central Sterilization. All instruments to be sterilized should be carried to the sterilization area. Gloves are not to be worn outside the operatory. High Level Disinfection: Reusable instruments that cannot be sterilized between uses and must undergo high level disinfection, must:
- Undergo decontamination with detergent in an instrument processing sink, (by a person wearing appropriate PPE)
- Be rinsed with tap water and dried - Be fully immersed in GSDM approved high level disinfectant for the amount of time
required by the manufacturer’s instructions - The container must be able to be securely closed to prevent off-gassing of fumes in
an area approved and monitored for this purpose by the Office of Environmental Health and Safety
- If the chemical has been poured into the container from the primary package, the secondary container must be clearly marked with the complete name of the chemical.
- After soaking, the instruments must be rinsed and handled according to the disinfectant manufacturer’s directions.
Hand-piece care and sterilization:
The protocol at the end of a clinic session requires the student to clean, and bag any hand piece used or taken out of a sterile sealed pouch.
1) Flush hand piece over the cuspidor for 60 seconds to remove adherent
material and oil residue. Dry the exterior of the hand piece and place in autoclave bag.
2) Use a separate autoclave bag for each hand-piece.
3) Remove your gloves and sanitize hands.
4) Print your name and date using an indelible pen (not magic marker) on
sterilization pouches.
One pouch for your slow-speed, all components

INFECTION PREVENTION MANUAL 2012
15 | P a g e
Two pouches for your high-speed. The two high-speed pouches will be utilized as follows: one with your high-speed sealed inside and the other, empty, for sterilization staff to place your high-speed in after lubrication.
5) Neatly fill out the Student Hand piece Receipt. Make sure you get the staff's signature and be sure to save your copy. It's your only proof and you will need it to claim your sterilized hand pieces. NOTE: When you pick up your property, check that the serial numbers match. Don't forget to lubricate your hand pieces immediately before your next patient.
Prior to sterilization, high-speed hand-pieces will be lubricated, by central sterilization personnel, following manufactures recommendations,(See link to the Midwest Slow Speed hand-piece and ADEC high Speed Hand-piece maintenance instruction manual, including the use of the ASSISTINA).
Hand pieces required for clinical use must be returned to the dispensary no later than 5 p.m. the preceding day. However, student scheduled to see a patient during an evening session and also a patient the following day may return the hand pieces to the dispensary by 7:45 a.m. the morning following the evening appointment.
When students need the use of their hand pieces for nonclinical purposes, they may
request them from the dispensary. However, hand pieces used for nonclinical purposes must be returned to the dispensary for sterilization prior to clinical use. Minimum turnaround time for hand piece sterilization is 45 minutes. Loaner Hand pieces If your own hand piece is being sterilized or is out for repair, you can check out a sterilized loaner hand piece from Central Sterilization. - Hand-pieces must be sterilized before servicing or shipping. Air/Water Syringe, Ultrasonic Tips and Sonic Units: Must be flushed for 15-30 seconds. All Ultrasonic and sonic tips must be cleaned, rinsed and sterilized between patients. Air/Water syringe tips must be replaced. Instrument decontamination may not be performed in hand washing sinks. Single Use Disposables: Protective barriers, suction tips, saliva ejector, prophy angle, pre-packaged single use only burs, must be discarded and not reused Operatory: Check the area/floor for blood, splatter, debris, impression material, cotton rolls,

INFECTION PREVENTION MANUAL 2012
16 | P a g e
etc. on and around the unit, cuspidor and sink. Remove contaminated barriers with gloves on. Barriers must be changed between patients. Clean and decontaminate all clinical contact surfaces. Equipment: Clean and disinfect reusable equipment like the water bath, curing light, shade guides, etc. CLEAN AND DISINFECT ALL CLINICAL CONTACT SURFACES IN PREPARATION FOR THE NEXT PATIENT
At the End of the Day Raise the chair, to prevent possible water damage make sure that you shut off the master switch, the suction and the running water in the cuspidor. Place the black foot pedal on the rubber mat to facilitate cleaning. Evacuation system will be flushed with disinfectant stored for that purpose under the sink, by central sterilization personnel on a daily basis. EVERYTHING THAT CAN BE STERILIZED MUST BE STERILIZED! Central Sterilization prepares, sterilizes and monitors instrument processing according to AAMI and CDC guidelines and OSHA regulations. Staff who reprocesses instruments must wear appropriate PPE for tasks that include potential for exposure to blood or body fluids. Heavy duty gloves are worn for handling sharps; fluid resistant gowns/aprons and mask/goggles or full face shields are worn when there is risk of contaminated fluid splash. PPE must be removed and hands sanitized before moving from the decontamination area to the clean side of the Central Sterilization area. Reusable Equipment and Supplies Sign up to request supplies/equipment. Return items clean and disinfected.(cavitrons, sensors, water baths) Disposal of Waste Materials The following items identified by OSHA are to be treated as "regulated waste" and must be placed in the container lined with the red biohazard bag.
Liquid or semi-liquid blood or body fluids such as saliva; Items contaminated with blood or saliva that would release these substances in a liquid
or semi-liquid state if compressed (e.g., gauze squares or cotton rolls saturated or dripping wet);

INFECTION PREVENTION MANUAL 2012
17 | P a g e
Items that are caked with dried blood or body fluids that are capable of releasing these materials when handled.
Pathological and microbiological wastes. Amalgam: Located in each operatory is a plastic container labeled: Hazardous Waste: Working Container Waste Mercury Amalgam
- all excess or discarded amalgam is to be placed in one of these sealed containers.
Use, Care, and Disposal of Sharps In addition to physical harm, emotional trauma may be a consequence of injuries sustained as a result of careless handling of contaminated sharps. Sharps include syringe needles, scalpel blades, burs, orthodontic wires, endodontic files and reamers, metal matrix material, suture needles, local anesthetic carpules and broken glass. All instruments and materials classified as sharps should be handled carefully to prevent injury. All sharps must be placed in the puncture resistant sharps container located in each operatory. It is illegal to dispose of sharps in the regular trash! Burs and Ultrasonic Scaler Tips Remove burs from the hand piece and sonic scaler tips immediately after use. These sharp items, when not in use and placed in the holder, can be a source of injury. When the dental health care worker or assistant reaches back to the tray for other instruments, there is the potential risk that they may scratch themselves on the bur or ultrasonic tip. Matrix Bands When placing metal matrix bands on a tooth, a cotton roll or 2x2 gauze can be placed on top of the band when using finger pressure to seat the band. Gauze or pliers should be used when removing matrix bands.

INFECTION PREVENTION MANUAL 2012
18 | P a g e
Broken Glassware Broken glass should never be picked up by hand. Use a dustpan and broom or a piece of cardboard to recover the broken glass. Dispose in the sharps container DISPOSAL OF WASTE MATERIALS Sharps Container Regulated Waste
All sharp items (especially needles), tissues, or blood should be considered potentially infective and should be handled and disposed of with special precautions. Disposable needles, scalpels, or other sharp items should be placed intact into puncture-resistant containers before disposal. Sharps Container (Puncture resistant, orange/red, with biohazard symbol affixed) Once the contents of a sharps container reaches the FULL line (scribed on the label) or the container is approximately ¾ full, the clinician is responsible for closing and securing the safety lock. The locked top alerts the Environmental Services staff to replace the container.
Blood, suctioned fluids, or other liquid waste may be carefully poured into a drain
connected to a sanitary sewer system. Other solid waste contaminated with blood, saliva, or other body fluids should be placed in sealed, sturdy impervious bags to prevent leakage of the contained items. Such contained liquid or solid wastes can then be disposed of according to requirements established by local or state environmental regulatory agencies and published recommendations. Developed by Dental Disease Prevention Activity, Center for Prevention Svcs, Hospital Infections Program, Center for Infectious Diseases, CDC.
INFECTION PREVENTION MANUAL 2012
19 | P a g e
C) Laboratory Environment
Laboratory Protocol All materials brought from the dental operatory to the dental laboratory must be disinfected appropriately before entry. Just as impressions must be disinfected, so too must any laboratory or prosthetic materials which come into contact with oral fluids be disinfected.
Metal frameworks for fixed and removable partial dentures or copings for crowns must be carefully rinsed of blood and debris and disinfected according to prescribed protocol before transfer from the operatory to the laboratory.
Disinfection – All clinical work (Removable, Fixed, Operative) must be sprayed, with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity and placed in an airtight and leak-proof plastic bag BEFORE leaving the operatory and transporting the prosthesis to the laboratories. They must be kept in the airtight and leak-proof plastic bag for 10 minutes before any work can be instituted. Larger items, like facebow forks with their mounting jigs (which must remain together) must be placed into the large size airtight and leak-proof plastic bags.
Large airtight and leak-proof plastic bags are dispensed in central sterilization for larger items such as face bow transfers.
Chemical Spill Remove any affected personnel from the area.
Attend to injured personnel.
Call the Control Center at 8-6666
Contain the spill and alert others in the immediate area.
Before attempting to clean up spill, know what the chemical is and locate the appropriate
MSDS.
DO NOT attempt to clean up a MERCURY SPILL. Call the Control Center at 8-6666
Hazardous Waste Information
The following waste materials are regulated waste and must be disposed of according to
protocol.
Material Satellite Accumulation area/responsible
Scrap amalgam 5th
floor/Central Sterilization
Monomer 6th
floor/Ms. Rosenthal
INFECTION PREVENTION MANUAL 2012
20 | P a g e
Sharps; Needles, scalpel blades, burs etc. Sharps Container/Housekeeping
Blood or Saliva contaminated items Red Bags/housekeeping
Burning alcohol 6th
Floor Central Sterilization
MONOMER/ALCOHOL PROTOCOL
PURPOSE
To establish a mechanism so that employees and students use, dispose of, and store formatray
monomer in a safe manner.
PROCEDURE
Formatray monomer will be turned into Central Sterilization on the fifth floor and stored in
the chemical storage room.
Formatray monomer will be available for use on the sixth floor in the flammable storage
cabinet. The amount of monomer will be checked daily by Leila Rosenthal.
Formatray monomer must be used, transferred, and stored in the appropriate containers.
Unused monomer, if not recycled, must be placed in appropriate containers located in
hazardous materials accumulation area on the sixth floor.
When container is full, please call the Office of Environmental Health and Safety for a
hazardous waste pick-up 8-8830.
Alcohol: “Burning alcohol” commonly used in Hanau torches is a special ðenatured”
mixture of ethanol and methanol alcohols. It is specially formulated to burn with a controlled
flame. To use safely follow these general guidelines.
1. Use only approved fuels. Never substitute other non-approved fuels
such as isopropyl alcohol.
2. Unused burning alcohol should be returned to Central Sterilization.
6th Floor Student Laboratory
Only new prostheses that have not yet been in the patient’s mouth are treated here.
Attire
Attire (scrubs) worn in the clinical setting should carry over into the student laboratories; however, PPE
should be modified in the following way: students will be required to cover their scrubs with pink
protective gowns provided in the lab. Nitrile gloves are used when handling raw (i.e., freshly
mixed) acrylic. Eye protection and mask protocols remain the same.

INFECTION PREVENTION MANUAL 2012
21 | P a g e
Counters & Sinks
Please keep all work areas clean. Pick up and discard trash from the floor and counters. This includes the sink area! Do not pour alcohol, monomer, alginate, or gypsum down the sink.
Flammable materials such as brown paper are not to serve as coverings in areas where open flames such as alcohol torches and Bunsen burners are used.
Model Trimmers After use, wait for the water to run clean before shutting off the machine. Flush the metal plate with a cup of water.
INFECTION PREVENTION MANUAL 2012
22 | P a g e
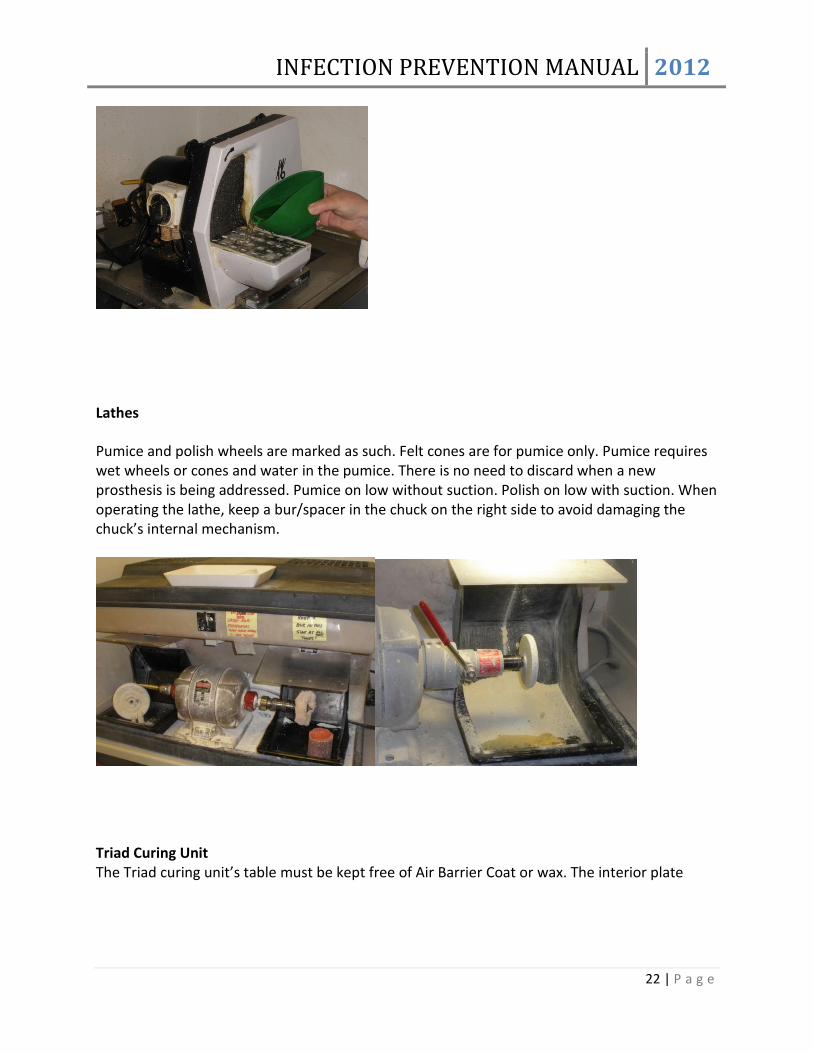
Lathes
Pumice and polish wheels are marked as such. Felt cones are for pumice only. Pumice requires wet wheels or cones and water in the pumice. There is no need to discard when a new prosthesis is being addressed. Pumice on low without suction. Polish on low with suction. When operating the lathe, keep a bur/spacer in the chuck on the right side to avoid damaging the chuck’s internal mechanism.
Triad Curing Unit The Triad curing unit’s table must be kept free of Air Barrier Coat or wax. The interior plate
INFECTION PREVENTION MANUAL 2012
23 | P a g e
must be wiped down after each use.
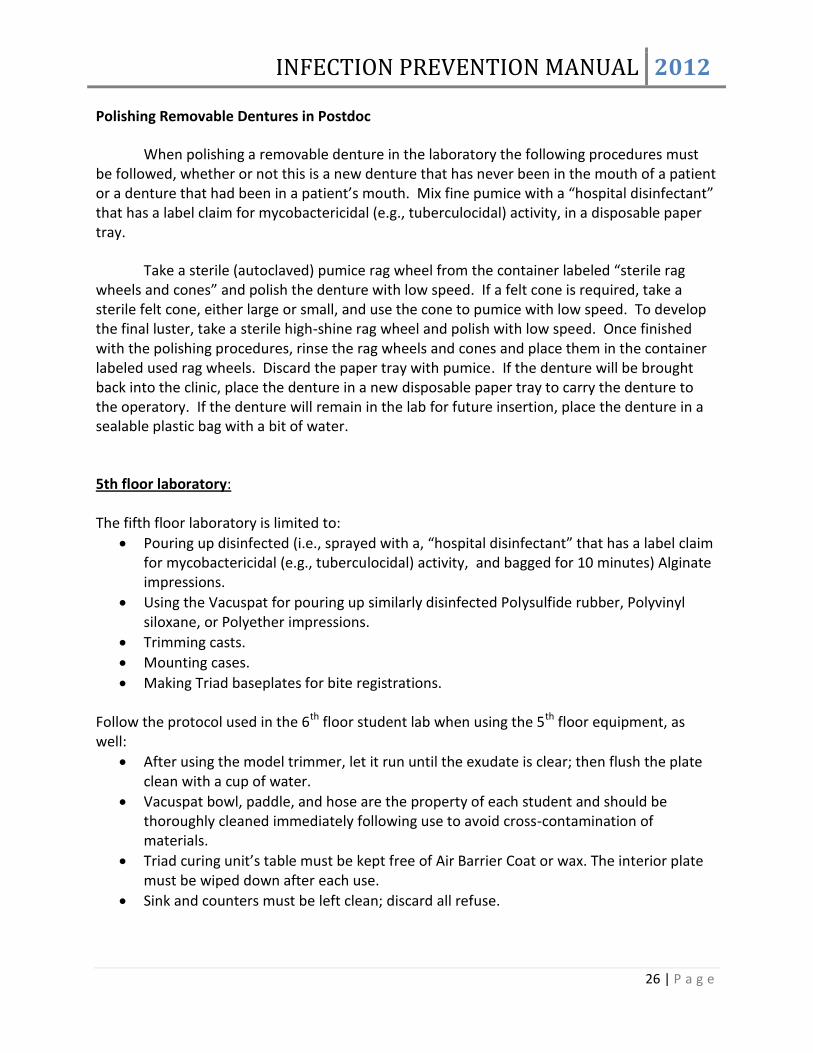
Vacuspat The Vacuspat bowl, paddle, and hose are the property of each student and should be thoroughly cleaned immediately following use to avoid cross-contamination of materials.
Vibrators: The vibrators are pre-covered. Additionally, cover the vibrator with a paper towel before using it and discard the towel afterward.

INFECTION PREVENTION MANUAL 2012
24 | P a g e
Ultrasonic Machines
FOR BRAND NEW PROSTHESES (i.e., that have NEVER been inserted): To remove any residual gypsum: Place the prosthesis into the beaker filled with pink Plaster-Stone Remover that sits in the ultrasonic machine in the 6th floor Removable laboratory and set the machine to “10”. To remove residual polishing material:

INFECTION PREVENTION MANUAL 2012
25 | P a g e
Place the prosthesis into the beaker filled with blue Ultrasonic Cleaner that sits in the ultrasonic machine in the 6th floor Removable laboratory and set the machine to “10” . To remove calculus: Place the disinfected prosthesis in an airtight and leak-proof plastic bag with Tartar-Stain Remover then set it into a dry beaker in the ultrasonic machine either in the 6th floor Removable laboratory or in central sterilization and set the machine to “10”. For cement removal: To use cement removers or general cleaner, place the prosthesis in an airtight and leak-proof plastic bag with some of the liquid from the appropriate beaker. Use the ultrasonic machine in the Fixed laboratory. In postdoc pros where the ultrasonic does not have provision for beakers, items are place in airtight and leak-proof plastic bags filled with the following liquids: To remove plaster or stone: Place the prosthesis in pink liquid (Plaster-Stone Remover). To remove high luster polishing material: Place the prosthesis in blue liquid (Ultrasonic Cleaner). And then placed it in the ultrasonic and set the machine to “10” FOR REMOVABLE PROSTHESES THAT HAVE BEEN IN THE MOUTH: To trim or re-polish small areas of a prosthesis: Burs and rubber points (black, green, yellow) are used in the students’ handpieces chairside and then dry heat sterilize. Black and green rubber points are to be used between 10,000-15,000 RPM. Yellow points are to be used at 6000-7000 RPM. The Midwest Shorty handpieces operate at 40,000 RPM and has a dial down feature to 20,000 RPM. Use the rheostat judiciously to keep the rubber points spinning at lower speeds. Postdoc Laboratory:
All material brought from the clinic that has been in a patient’s mouth (such as a prosthesis, baseplates and occlusion rims, wax trial denture, impression, or facebow fork) must be sprayed with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and placed in an airtight and leak-proof plastic bag BEFORE leaving the operatory. This airtight and leak-proof plastic bag must then be placed in a disposable paper tray. Gloves must be removed and discarded. The tray with the airtight and leak-proof plastic bag is then carried to the laboratory. The bag must remain closed for 10 minutes before any work can be initiated. Articles such as facebow forks with their mounting jigs (which must remain together) must be placed into the larger size airtight and leak-proof plastic bags.
Larger airtight and leak-proof plastic bags are available from the dispensary.
INFECTION PREVENTION MANUAL 2012
26 | P a g e
Polishing Removable Dentures in Postdoc
When polishing a removable denture in the laboratory the following procedures must be followed, whether or not this is a new denture that has never been in the mouth of a patient or a denture that had been in a patient’s mouth. Mix fine pumice with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, in a disposable paper tray.
Take a sterile (autoclaved) pumice rag wheel from the container labeled “sterile rag wheels and cones” and polish the denture with low speed. If a felt cone is required, take a sterile felt cone, either large or small, and use the cone to pumice with low speed. To develop the final luster, take a sterile high-shine rag wheel and polish with low speed. Once finished with the polishing procedures, rinse the rag wheels and cones and place them in the container labeled used rag wheels. Discard the paper tray with pumice. If the denture will be brought back into the clinic, place the denture in a new disposable paper tray to carry the denture to the operatory. If the denture will remain in the lab for future insertion, place the denture in a sealable plastic bag with a bit of water.
5th floor laboratory: The fifth floor laboratory is limited to:
Pouring up disinfected (i.e., sprayed with a, “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and bagged for 10 minutes) Alginate impressions.
Using the Vacuspat for pouring up similarly disinfected Polysulfide rubber, Polyvinyl siloxane, or Polyether impressions.
Trimming casts.
Mounting cases.
Making Triad baseplates for bite registrations. Follow the protocol used in the 6th floor student lab when using the 5th floor equipment, as well:
After using the model trimmer, let it run until the exudate is clear; then flush the plate clean with a cup of water.
Vacuspat bowl, paddle, and hose are the property of each student and should be thoroughly cleaned immediately following use to avoid cross-contamination of materials.
Triad curing unit’s table must be kept free of Air Barrier Coat or wax. The interior plate must be wiped down after each use.
Sink and counters must be left clean; discard all refuse.

INFECTION PREVENTION MANUAL 2012
27 | P a g e
All material brought from the clinic that has been in a patient’s mouth (such as a prosthesis, baseplates and occlusion rims, wax trial denture, impression, or facebow fork) must be sprayed with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity, and placed in an airtight and leak-proof plastic bag BEFORE leaving the operatory. This airtight and leak-proof plastic bag must then be placed in a disposable paper tray. Gloves must be removed and discarded. The tray with the airtight and leak-proof plastic bag is then carried to the laboratory. The bag must remain closed for 10 minutes before any work can be initiated. Articles such as facebow forks with the mounting jigs (which must remain together) must be placed into the larger size airtight and leak-proof plastic bags.
Airtight and leak-proof plastic bags and disposable trays are available in each operatory. Larger airtight and leak-proof plastic bags are available from the dispensary.
Further information pertaining to Infection Control and Safety in Health Care Environment can be found at: http://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
D) Radiographic environment :
A clinical examination should precede all radiographic procedures. Standard/universal precautions and other appropriate infection control procedures must be regularly applied for all patients.
Clean clinic attire and full PPE (mask, eye protection, protective gown) must be donned for each radiology clinic procedure, and removed afterwards. Clinic gowns must be changed at least daily or more often when visibly soiled. Hand hygiene must be performed at the beginning and end of each appointment as well as before gloving and after de-gloving.
It is important to prepare the operatory prior to seating the patient. The countertop work area should to be draped with a plastic-backed towel; the x-ray tube-head with a plastic cover, the chair headrest should be covered with a disposable plastic cover. The control panel, chair controls, and the door- knobs should be covered with a clear adhesive barrier. The Rinn kit, disposable bite blocks and cotton rolls should be placed on the countertop work area prior to the procedure.
Every attempt must be made to minimize surfaces touched by contaminated hands during procedures. All surfaces touched during the procedure must be disinfected with a “hospital disinfectant” that has a label claim for mycobactericidal (e.g., tuberculocidal) activity.

INFECTION PREVENTION MANUAL 2012
28 | P a g e
All Rinn instruments (metal arms and rings) must be rinsed and autoclaved between patients. Disposable bite blocks should be used for all digital intra-oral sensors.
Panoramic bite guides should be covered by protective barriers for each patient.
All intra-oral digital sensors must be covered by FDA-cleared disposable plastic barriers. Use disinfecting wipes to clean and disinfect sensors between patients. The computer keyboard should also be wiped clean with disinfecting wipes between patients. Clinical contact surfaces should have barriers placed, to include keyboards.
The lead apron should be wiped clean with disinfectant and hung on the wall without
creases.
E) Professional Attire STUDENTS AND RESIDENTS: Students and residents participating in patient treatment (or simulated patient treatment) must wear scrub tops and scrub bottoms of matching color. The particular color is coded to the student’s or resident’s class. For example, all D2 students will wear the same color scrubs. This allows faculty and staff to visually identify the class level of any student in the clinic (or simulated clinical setting). Students wearing scrubs in public areas of the dental school, such as the classroom, meeting rooms or the cafeteria must wear a long white lab coat over their scrubs. Students who are not attending clinic (or simulated clinic) may wear any appropriate personal clothing that they choose. However, if they choose to wear scrubs then they must also wear a long white lab coat in public areas of the school. FACULTY AND STAFF: Faculty and staff participating in clinical (or simulated clinical) activities must wear scrub tops and scrub bottoms of matching color. All faculty wear black scrubs. The color of staff scrubs is coded to their particular clinical responsibilities. For example, all dental hygienists will wear the same color scrubs or the color of scrubs assigned to their postdoctoral department. Faculty and staff wearing scrubs in public areas of the dental school must wear a long white lab coat over their scrubs. Faculty and staff who are not attending clinic (or simulated clinic) may wear any appropriate personal clothing that they choose. However, if they choose to wear scrubs they must also wear the long white lab coat in public areas of the school.

INFECTION PREVENTION MANUAL 2012
29 | P a g e
Illustrated by:
III) Post-Exposure Evaluation and Follow-up Needlestick and Sharps Exposure Protocol If you have been exposed to potentially infectious blood or saliva via a needlestick or a sharp dental instrument, or via a splash or spill to eyes, mouth, or non-intact skin, IMMEDIATELY:
WASH THE AREA thoroughly with soap and water. If eyes or mouth are contaminated, flush vigorously with water for 15 minutes. Two eye
wash stations are located in each treatment center corridor on the South side of the building. There is one eye wash station located in Oral Surgery by the front desk.
Your instructor/supervisor should EXPLAIN THE ACCIDENT TO THE PATIENT and request the patient’s permission for blood testing. The patient should be asked to report to Occupational and Environmental Medicine for HBV, HCV and HIV testing with counseling and follow-up.
REPORT IMMEDIATELY for counseling, assessment of risk and testing to: 1. Occupational and Environmental Medicine
Yawkey Building, ACC Ground Floor, 850 Harrison Ave. Monday - Friday, 7:30 am - 4:pm (617)- 638-8400
2. Occupational and Environmental Medicine Satellite Office Doctors Office Building, room 202, 720 Harrison Ave. Monday – Friday, 7:30am to 4:pm

INFECTION PREVENTION MANUAL 2012
30 | P a g e
(617)-638-8401 3. Occupational and Environment Medicine 90 Commonwealth Avenue Charles River Campus Monday – Friday, 8:30 a.m. to 5:00 p.m. 617-353-6630
At all other times, report to the Boston Medical Center Emergency Room, Menino Pavilion 770 Albany St. (617) 414-4075. The OEM or Emergency Department will initiate two procedures.
An investigation of the circumstances surrounding the exposure incident; and Post-exposure follow up of the employee or student with medical consultation and
treatment (as required). Immediate reporting is extremely important. DO NOT WAIT! If antiretroviral medication is indicated, it should be started AS SOON AS POSSIBLE, ideally not more than an hour or two after the exposure.
An exposed employee should report the exposure with any paperwork from OEM to his/her
supervisor as soon as possible. As in the case of all accidents with actual or potential for injury, an ART form (Accident Reporting and Treatment Report) must be filled out by the supervisor within 24 hours. The supervisor keeps a copy of the ART form and sends the original to Human Resources (HR). HR must report the incident to Risk Management within 5 days per Worker’s Compensation Board requirements. ART forms are available at: http:www.bu.edu/cfo/files/2010/01/accreport.pdf LINK WOULD NOT WORK – Internet reports that Item COULD NOT BE FOUND IV) Immunizations
Infection control policies are instituted to protect all personnel, students, patients and volunteers from communicable diseases and cross contamination related to dental procedures. One method to achieve this goal is for all clinical personnel and volunteers to be currently immunized against Hepatitis B and other appropriate diseases.
Records: Records of compliance with required immunizations and tests are maintained by Occupation and Environmental Medicine (OEM) for faculty and staff and Student Health Services (SHS) for students and residents. For all licensed personnel, compliance is part of the credentialing process. Non-compliance is reported to Departmental Chairs and Clinical Directors for action. The Office of Clinical Services maintains logs of the compliance reports.
Effective June 2011 Immunization Compliance
INFECTION PREVENTION MANUAL 2012
31 | P a g e
Requirements for Henry M. Goldman School of Dental Medicine, GSDM Employees and Volunteers Direct and Indirect Patient Care:
The following immunizations and screening are required and apply to GSDM employees and volunteers who have clinical responsibilities for the care and treatment of patients, i.e., direct patient care. This includes clinical faculty, assistant and associate deans, department chairs and directors, hygienists, dental assistants, and volunteer faculty. Indirect patient care responsibilities may also involve potential exposure to blood or infectious body fluids or airborne contagions; this category includes other faculty without direct clinical roles, patient coordinators, clinic supervisors, administrative managers, administrative coordinators, secretaries and front desk personnel, all central sterilization staff, dental technicians and ceramists, records room staff, Office of Finance Staff, as well as facilities and maintenance staff. Proof of Immunity (provider documentation or lab report) for the following:
Measles, Mumps Rubella (MMR) –vaccine #1 and #2 dates or titers indicating immunity
Hepatitis B - vaccine #1, #2, and #3 dates AND Hep B Surface Antibody titer indicatingimmunity, signed declination, or lab results indicating disease history.
Varicella-zoster (Chicken Pox) - vaccine #1 and #2 dates; or provider documentation of disease (not by parent or self-report); or titer indicating immunity,
Adacel (Tdap; tetanus, diphtheria, acellular pertussis) given since 2005; strongly preferred as gives immunity to whooping cough which can be an airborne contagion
Tuberculosis (TB) skin test results. Two TB skin tests (TST), one within 12 months and the second within 12 weeks of your start date. Documentation of TST results must include dates given and read, and the millimeter (mm) of induration. The form should be signed by the health professional reading the test with printed name, title, and contact number on his or her letterhead.
o For those with prior positive TB skin tests, please provide documentation of
the positive TB test date with size (mm) of skin reaction induration, a copy of a chest X-Ray report obtained for positive TB skin test, and documentation of TB prophylactic medication counseling or treatment.
o Other tests for TB such as the QFT or T-Spot obtained via blood draws will be
accepted or utilized on a case by case basis Annual Screening:
Tuberculosis screening
Influenza vaccine or signed declination
INFECTION PREVENTION MANUAL 2012
32 | P a g e
Vaccination Records - These documents can be found in your doctor's office records, student health or previous employee health records, immigration documents, military service documents and/or travelvaccination records. Requirements defined by job – Examples include healthcare workers with potential direct patient contact (e.g., to blood/body fluids) should have titer proven immunity to Hepatitis B and staff working in patient care areas should have vaccines to prevent illness spread by cough or respiratory secretions. Non-patient Care: Effective June 2011
The following immunizations and screening are required, unless otherwise stated. This applies to teaching and research faculty and staff; all departmental support staff such as coordinators, managers, assistant and associate directors, directors, and supply store staff who share airspace with patients and clinical staff and are at risk of getting or spreading airborne contagions. All employees and volunteers located at 100 E. Newton Street and 930 Commonwealth Avenue Proof of Immunity (provider documentation or lab report) for the following:
Measles, Mumps Rubella (MMR) –vaccine #1 and #2 dates or live vaccine or titers indicating immunity
Varicella-zoster (Chicken Pox) vaccine #1 and #2 dates; or provider documentation of disease (not by parent or self-report); or titer indicating immunity,
Adacel (Tdap; tetanus, diphtheria, acellular pertussis) given since 2005; strongly preferred as gives immunity to whooping cough which can be an airborne contagion
Tuberculosis (TB) skin test results. Two skin tests (TST), one within 12 months and the second within 12 weeks of your start date. Documentation of TST results must include dates given and read and the millimeter (mm) of induration. The form should be signed by the health professional reading the test with printed name, title, and contact number on his or her letterhead.
o For those with prior positive TB skin tests, please provide documentation of
the positive TB test date with size (mm) of skin reaction induration, a copy of a chest X-Ray report obtained for positive TB skin test, and documentation of prophylactic TB medication counseling or treatment.
o Other tests for TB such as the QFT or T-Spot obtained via blood draws will be
accepted or utilized on a case by case basis

INFECTION PREVENTION MANUAL 2012
33 | P a g e
Annual Screening: • Influenza vaccine or signed declination • TB Screening All employees and volunteers located at other GSDM buildings where they will NOT have the possibility of patient contact (see list below) Annual Screening: • Influenza vaccine or signed declination (strongly preferred) Other GSDM Buildings:
801 Albany Street
700 Albany Street
650 Albany Street (Evans Biomedical Research Center)
Evans Building 4th Floor
Robinson Building 3rd Floor
930 Commonwealth Ave.
560 Harrison Avenue
Hepatitis B Immunization It has been shown that dental health care workers (DHCW) have a much higher rate of Hepatitis B infection than the general population. Based on studies of health care personnel, the risk of acquiring an HBV infection following a single puncture with a needle contaminated with the virus, ranges from 6% - 30%. Under similar circumstances, the risk of an HIV infection is less than 1.0%! Additionally, transmission of HBV infection from DHCW to patients has been documented. The vaccines currently used are safe and highly effective and stimulate the production of protective antibodies in at least 96% of those vaccinated. OSHA requires that Hepatitis B vaccines be offered to ALL employees at risk for contracting HBV infection, followed by Hepatitis B surface antibody testing after vaccination. These services must be offered FREE of charge.
The American Dental Associations' Council on Scientific Affairs, the Public Health Service's Immunization Practices Advisory Committee and The Center for Disease Control recommend that all dental personnel involved in patient care receive the Hepatitis B Vaccination, if they do not already have immunity as a result of a previous exposure to the virus. The three-part Hepatitis B Vaccination series is administered intramuscularly over 6 months. The vaccine is free to all Category I and II employees. It is available at Occupational Environmental Medicine (OEM) of the Medical Campus, 1st floor Yawkey ACC Building, 850 Harrison Ave. No appointment is necessary.

INFECTION PREVENTION MANUAL 2012
34 | P a g e
Serological testing is required after completion of the vaccination series and should be performed four to six weeks after the last vaccination. Boosters of Hepatitis B vaccine are not needed for individuals who have demonstrated serological immunity after vaccination. Tuberculosis (TB) Plan for the Control of TB Infection at GSDM
GDSM defers dental care of patients diagnosed with or suspected of having active pulmonary or laryngeal TB, until they are declared to be no longer contagious by their pulmonologist or the Dept of Public Health.
Assess each patient for a history of TB as well as for symptoms of active pulmonary or laryngeal TB.
o TB should be considered in all patients who present with the following symptoms: Persistent cough for > 2 weeks duration or other symptoms compatible with TB such as bloody sputum, fever and night sweats, or unexplained weight loss in addition to the aforementioned respiratory symptoms.
Patients suspected of active TB must leave the building as quickly as possible and should proceed to the emergency department or to the TB clinic for further evaluation.
Faculty, students, and volunteers providing clinical care will receive annual training regarding the TB Prevention Plan.
VI) Training Program
All employees/students/residents and volunteers, who have the potential for exposure to
human blood or body fluids, receive comprehensive training in infection control and exposure
prevention prior to any potential exposure. New employees receive this training within 10 days
of their start or before the first potential exposure. Refresher training is required and is given
at least annually. For faculty and staff, the training is part of the credentialing program. For
students, the training is part of their clinical competency XV. Documentation is maintained by
the department of Clinical Services and is shared with Department Chairs and Clinical Directors
for enforcement.
The program shall consist of the following:

INFECTION PREVENTION MANUAL 2012
35 | P a g e
Training
Covering the BUSDM exposure control plan and based on the CDC 2003 “Guidelines for Infection Control in the Dental Healthcare Setting” and OSHA’s “Blood Borne Pathogen Standard”, IC&S training begins shortly after matriculation for all students and residents, and shortly after hiring for faculty and staff. The training is based on the premise that unlike with most other skills, there is no learning curve when it comes to infection control and safety. Everyone must be competent the first time they face the potential to exposure to blood borne pathogens. To provide students with the knowledge necessary to achieve competence, a multi-hour training program is given to first year students as part of their General Dentistry course. Soon after, DMD and Advance Standing students are given an opportunity to apply this knowledge in a mock clinical setting in the simulation learning center (SLC). Competency is then demonstrated by DMD students and recorded by faculty in the clinical portion of the first year General Dentistry course. Advance Standing students similarly demonstrate clinical competency as part of their first year periodontal preclinical course.
Preclinical and clinical experiences are gradually increased in complexity consistent with the students training and experience, and adherence to infection control policies and protocols is constantly monitored and enforced. (Summative Evaluation Plan Competency XV Appendix 5-1.12o) Training continues as the students’ progress through the curriculum with refreshers given at least annually, often coupled with important events in the student schedule, i.e. prior to entering clinic, going on an extramural rotation, etc. (Training schedule Appendix 5-1.12p) Annual training consists of an online module developed by BMC consultants in safety and infection prevention and the GSDM Department of Oral Surgery. Included in this training is a section on management of medical emergencies. The online training is followed by a live lecture by an infection prevention consultant and GSDM faculty. This training is focused on the prevention of exposures to blood borne pathogens. Annual completion of the online training module is required for all faculty and staff with potential for exposure to blood borne pathogens.
Record of training for students are maintained by the Department of Clinical Services. (Sample record in Appendix 5-1.12q) Faculty and staff compliance is part of the clinical credentialing program. Compliance is reported to Department Chairs and Clinical Directors for enforcement.
Staff in specialty areas, such as central sterilization and equipment repair, receive additional training germane to their work responsibilities from their supervisor or director.(Sample plan Appendix5-1.12s) Documentation of this training is maintained by departmental supervisors.
Objectives
Upon completion of the training program, the student/employee will be able to
recognize/describe the following:
INFECTION PREVENTION MANUAL 2012
36 | P a g e
Core Infection Prevention Measures used to protect patients and health-care workers
from care related infections
Epidemiology and symptoms of blood borne diseases (HBV/HCV, HIV)
Modes of transmission of blood borne pathogens (HBV/HCV, HIV)
GSDM Exposure Control Plan
The tasks and other activities involving exposure to blood and/or body fluids.
"Universal (Standard) Precautions"
Engineering controls, work practices, and personal protective equipment (including use
and limitations) that will prevent or reduce exposures.
Types, proper use, location, removal, handling, decontamination and disposal of
personal protective equipment and rationale for product selection
Hepatitis B Vaccination:
Method and site of administration
Safety, efficacy and advantages
Side effects/reactions
Protocol for an emergency or accidental exposure involving blood or body fluids,
including the required post-exposure evaluation and follow-up protocol
Signs, labels and color-coding of containers of infectious/hazardous waste or storage
containers of any infectious materials (Sharps)
References:
OSHA Bloodborne Pathogens Standard 1910.1030
http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=standards&p_id=10051
CDC Guidelines for Infection Control in Dental Healthcare Settings – 2003
http://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
A) PROGRAM ADMINISTRATION
The Henry M. Goldman School of Dental Medicine Infection Control and Safety
Subcommittee is responsible for the overall management and support of the Infection
Prevention Program which includes the OSHA mandated, Blood borne Pathogens Exposure
Control Plan. The GSDM Infection Control and Safety Subcommittee will maintain, review and
update the Plan at least annually, and whenever necessary to include new or modified tasks
and procedures with exposure risk and to account for innovations in procedures and
technological developments that reduce the risk of exposure.
INFECTION PREVENTION MANUAL 2012
37 | P a g e
Members of the Infection Control and Safety Subcommittee
Dr. Bruce Robinson, Chair, 8-7632, [email protected]
Ms. Meg Loadholt, 8-4669, [email protected]
Maria DaSilva, 8-4032, [email protected]
Roslyn George, 8-4527, [email protected]
Andy Burke, 8-5129, [email protected]
Leila Joy Rosenthal, 8-4757, [email protected]
Mike Haddad, 4-1096, [email protected]
Student Representatives: Treasurers of each class
Advisers
Dr. Larry Culpepper, 8-8400
Dr. Jeffrey Hutter, 8-4780, [email protected]
Dr. Stephen DuLong, 8-5127, [email protected]
Dr. John Burress, 8-8400
Bob Burke, RN, CIC (Infection Prevention), 8-8815, [email protected]
Eric Johnson (Safety), 8-8841, [email protected]
Connie Packard (Security), 4-4412
Jim Munroe (Facilities), 8-4211

















