Infections in Oncology Patients: Febrile Neutropenia and Beyond Corey Casper, MD MPH Vaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center Division of Infectious Disease, University of Washington 9 July 2010
Transcript
Infections in Oncology Patients: Febrile Neutropenia and Beyond
Corey Casper, MD MPHVaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center
Division of Infectious Disease, University of Washington
9 July 2010
Overview• Febrile Neutropenia
– Epidemiology– Microbiology– Evidence for Various Prophylactic Strategies– Controversies
• VRE• Prevention and treatment of invasive
fungal infections
Incidence of Infection in Neutropenic Patients with Cancer
• Prior to routine antibiotic prophylaxis, infection was a common complication of cancer therapy– Acute Leukemia
• 20-40 infections per 1000 patient-days• Bodey GP (1966), Ann Intern Med
– Transplant• 71-100 infections per 1000-patient days
• Engels EA (1999), Clin Infect Dis
• Infections frequently associated with high mortality– 75% of mortality in early era of chemotherapeutics was due to
infection• Schimpff SC (1971). N Engl J Med
Risk Factors for Infection in Patients with Neutropenia: Duration
Viscoli C (2005), Clin Infect Dis
Risk Factors for Infection in Patients with Neutropenia: Depth
Engels EA (1999). Clin Infect Dis
No Abx
IV Abx
PO Cipro IV Abx + PO Cirpo
Risk Factors for Infection in Patients with Neutropenia: Other
• Therapy– Type of chemotherapy– Corticosteroids
• Breach of Physical Barriers to Infection
• Skin / mucous membranes• Catheters
• Malignancy– Those which impair Ig function
• Multiple myeloma• CLL
– Those associated with splenectomy
Incidence of Febrile Neutropenia by Cancer Type
Etiology of Fever in Neutropenia• Only 50% of patients with fever during
neutropenia will have a documented infection– Of those 50%, only 20% have blood stream
infection– Not all are bacterial
Etiology of Bacteremia in Neutropenic Cancer Patients (1)
Viscoli C (2005) Clin Infect Dis
Etiology of Bacteremia in Neutropenic Cancer Patients (2)
Wisplinghoff H (2003), Clin Infect Dis
Sites of Infection in Cancer Patients
Yadegarynia D (2003), Clin Infect Dis, MD Anderson
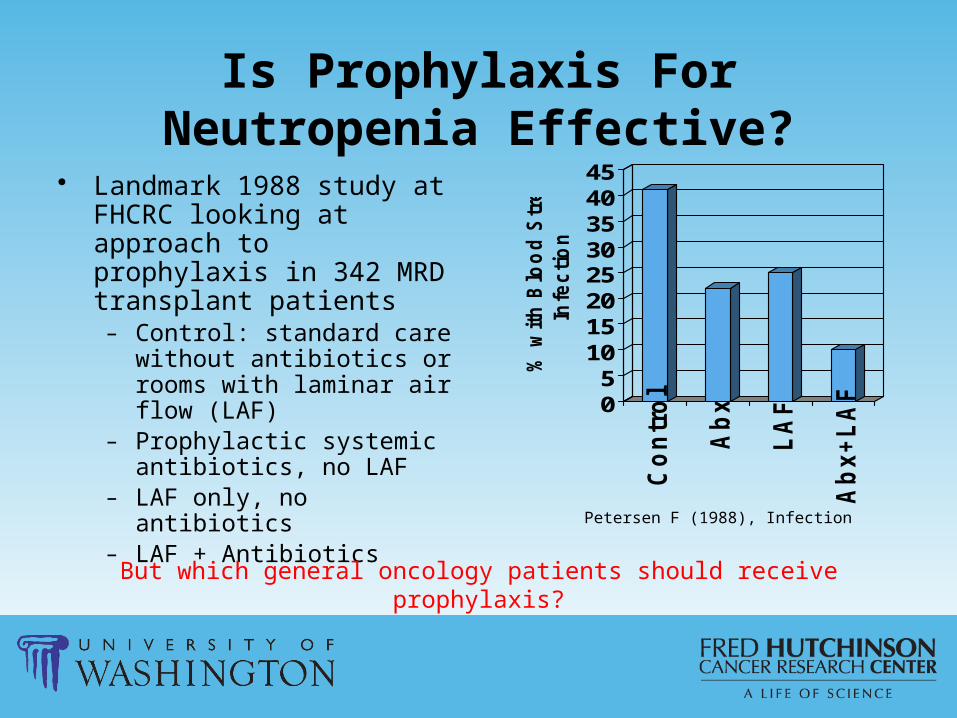
Is Prophylaxis For Neutropenia Effective?
• Landmark 1988 study at FHCRC looking at approach to prophylaxis in 342 MRD transplant patients
– Control: standard care without antibiotics or rooms with laminar air flow (LAF)
– Prophylactic systemic antibiotics, no LAF
– LAF only, no antibiotics– LAF + Antibiotics
05
1015202530354045
% w
ith
Blo
od
Str
ea
m
Infe
cti
on
Co
ntr
ol
Ab
x
LA
F
Ab
x+
LA
F
Petersen F (1988), Infection
But which general oncology patients should receive prophylaxis?
Antibiotic Prophylaxis for General Oncology Patients with Short-Term Neutropenia (1)
Cullen, et. al. NEJM 2005
Antibiotic Prophylaxis for General Oncology Patients with Short-Term Neutropenia (2)
0
10
20
30
40
50
Fever Infection Hospitalization
Levo
Placebo
P value for all comparisons <0.01, Cullen, et. al. NEJM 2005
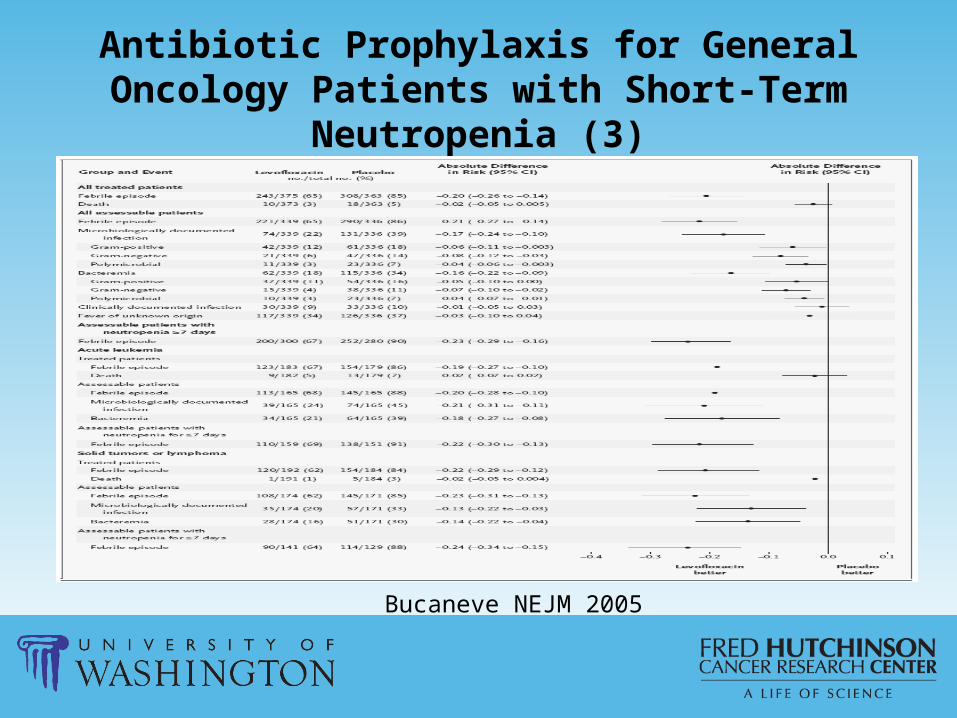
Antibiotic Prophylaxis for General Oncology Patients with Short-Term Neutropenia (3)
Bucaneve NEJM 2005
Antibiotic Prophylaxis for General Oncology Patients with Short-Term Neutropenia (4)
…But Resistance to Fluoroquinolones is Increasing
• Among 823 hematology/oncology patients receiving FQ pphx, risk of FQ resistant bacteremia was 3 fold higher among those receiving prophylaxis– Cattaneo J Antimicrob Chemother. 2008
Prediction Model to Identify Neutropenic Patients Needing Pphx?
Cullen, JCO 2007
Predicting Risk of Infection During Neutropenia : Risk Groups
NCCN, “Prevention and Treatment of Cancer-Related Infections”
Principals of Antibiotics for Febrile Neutropenia
• Antibiotics are not antipyretics• Look for sources
– Risk factors– Exam– Studies
• Know antibiotic resistance patterns at UWMC / FHCRC and inherent susceptibilities of organisms to antibiotics
Evaluation of Patients with Febrile Neutropenia
Empiric Therapy for Febrile Neutropenia
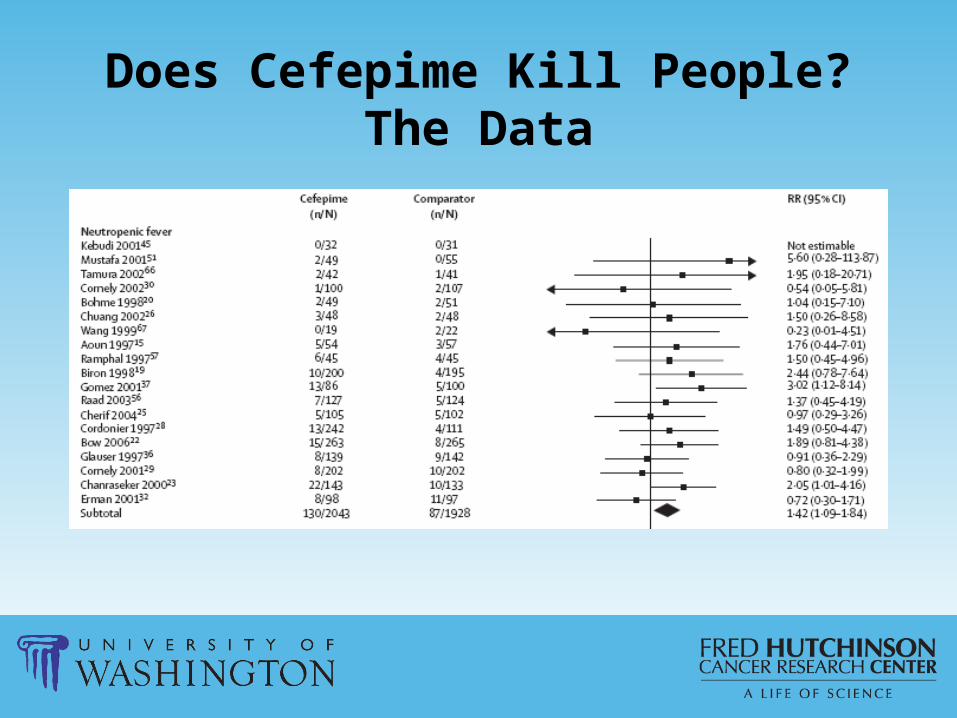
Does Cefepime Kill People? The Story
Cefepime Meta-analysis• Lancet meta-analysis indicated that use of
Cefepime was associated with a 26% increased risk of death compared with other antibiotics– Not due to microbiologic failure
• NCCN hired biostatistician to review data, found methodology to be sound
Does Cefepime Kill People?The Data
Cefepime FDA Re-review• FDA asked for additional primary data from company
and found no increased risk for death– Quality / comprehensiveness of additional data provided?– Subgroup analysis found significantly increased risk of
death in solid tumor patients (but small numbers) and trend in hematologic malignancy patients
• My conclusion (only partially evidenced-based): use another agent in cancer patients when possible!
Tally of Infection-Related Deaths in Transplant, Q1 2008
Infection Count
VRE 8
Aspergillus 4
CMV 4
RSV 3
BK 2
Influenza A 1
Adenovirus 1
Non-infectious 8
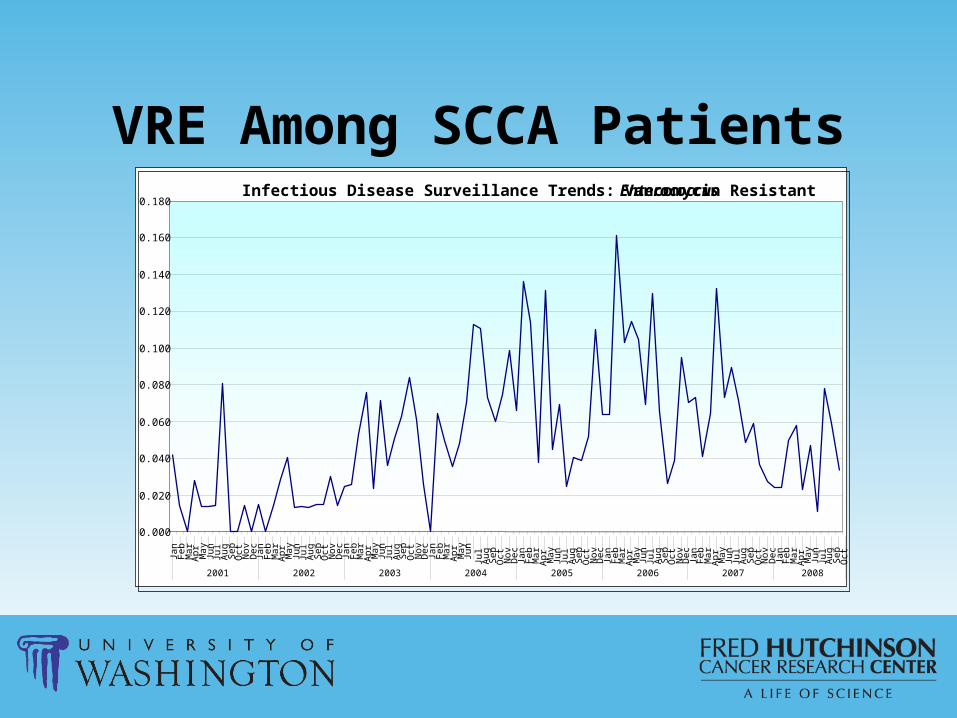
VRE Among SCCA PatientsInfectious Disease Surveillance Trends: Vancomycin Resistant Enterococcus
0.000
0.020
0.040
0.060
0.080
0.100
0.120
0.140
0.160
0.180
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr May
Jun
Jul
Aug
Sep
Oct
2001 2002 2003 2004 2005 2006 2007 2008
Prevalence / Significance of VRE Among SCCA Transplant Patients
• All transplant patients receive “welcome” culture to survey for VRE– 25% of transplant patients arrive at SCCA colonized with VRE– Additional 25% of susceptible patients develop VRE over course
of treatment at SCCA• Presence of VRE colonization predicts the development
of bacteremia in up to 1/3rd of cancer patients. – Matar MJ, et. al.. Am J Infect Control 2006; Zaas AK, et. al. Clin Infect Dis 2002
• VRE bacteremia portends a poor prognosis in persons undergoing treatment of malignancies with a high mortality rate
– Avery R, et. al.. Bone Marrow Transplant 2005; Bach PB, et. al.. Infect Control Hosp Epidemiol 2002
Antimicrobials for VRE: No Magic Bullet
Antibiotic Limitation (s)
Linezolid •Bacteriostatic•Bone marrow suppression
Quinupristin/Dalfopristin (Synercid)
•Bacteriostatic•Only active against E. faecium•Relatively poor penetration to urine•Infusional Toxicity
Daptomycin •Poor alveolar penetration•Resistance relatively easy to engender
Tigecycline •Questionable efficacy in bacteremia•Significant toxicities / drug-drug interactions
New SCCA Strategy for VRE• Empiric use of daptomycin in all patients
with known VRE colonization prior to or subsequent to transplant when vancomycin would ordinarily be used
Sepsis Stat Pack - Rationale• Anecdotal observations found opportunities for
improvement in providing antibiotics to septic patients with febrile neutropenia presenting to SCCA outpatient clinic– No antibiotics given in clinic because they would slow
transfer to acute setting– Inappropriate antibiotics given in clinic
• Convenience• Failure to appreciate spectrum of resistant organisms
Sepsis Stat Pack - Implementation[ ] Adult Sepsis
Protocol Standard Imipenem 500 mg
IVPB STAT over 20 minutes
Tobramycin 80 mg IVPB STAT over 20 minutes
Linezolid 600 mg IVPB STAT over 30 minutes
[ ] Adult Sepsis Protocol PENICILLIN ALLERGIC
Aztreonam 2 gm IVPB STAT over 20 minutes
Tobramycin 80 mg IVPB STAT over 20 minutes
Linezolid 600 mg IVPB STAT over 30 minutes
Improved Survival of Cancer Patients with Sepsis with Use of “Stat Pack”
• Among patients meeting criteria for severe sepsis, 90% thirty-day survival– More than double
compared with other published studies
• No toxicities noted• 81% had follow-up ID
consultation and tailoring of antibiotics
Larche J, Intensive Care Med 2003Pene F, Crit Care Med 2008
Invasive Fungal Infections (IFI)Infection Count
VRE 8
Aspergillus 4
CMV 4
RSV 3
BK 2
Influenza A 1
Adenovirus 1
Non-infectious 8
IFI Prevention:New Triazole on the Block
• Fluconazole– Cheap (<$1 per generic dose)– Effective against yeast– Safe
• Voriconazole– Expensive ($68 per dose)– Increased toxicities / drug interactions– Effective against yeast and mould
• Posaconazole– Expensive ($88 per dose)– Equally safe as fluconazole– Proven efficacy against IFI (and in vitro activity against
Zygomycetes)
Posaconazole:Acute Leukemia and MDS with Prolonged
Neutropenia
Cornely, NEJM 2007
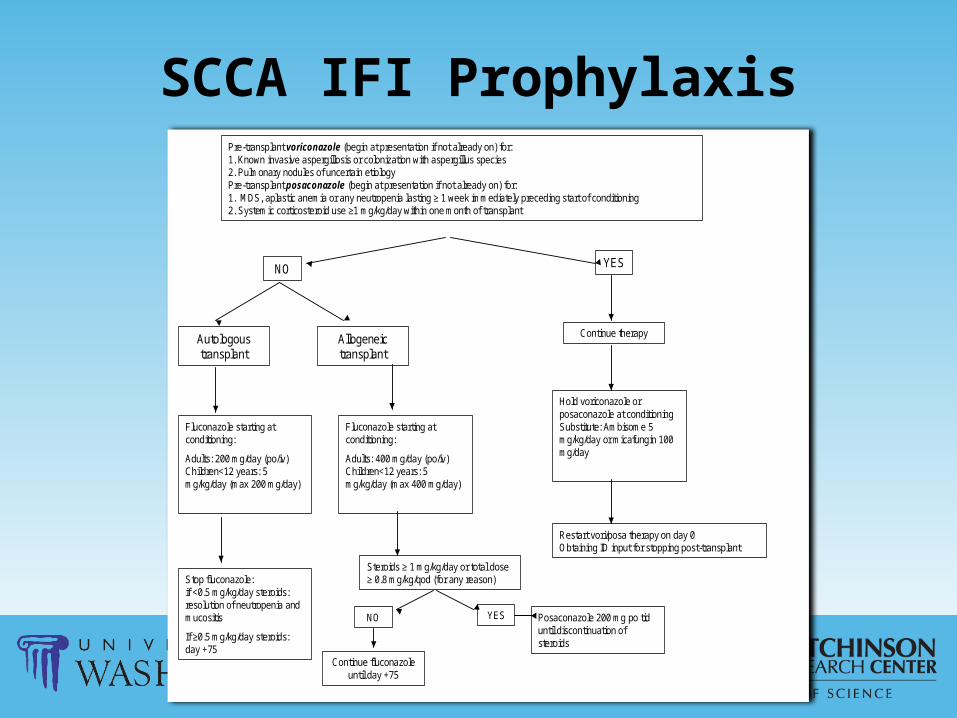
SCCA IFI ProphylaxisPre-transplant voriconazole (begin at presentation if not already on) for:1. Known invasive aspergillosis or colonization with aspergillus species2. Pulmonary nodules of uncertain etiologyPre-transplant posaconazole (begin at presentation if not already on) for:1. MDS, aplastic anemia or any neutropenia lasting ≥ 1 week immediately preceding start of conditioning2. Systemic corticosteroid use ≥1 mg/kg/day within one month of transplant
Steroids ≥ 1 mg/kg/day or total dose ≥ 0.8 mg/kg/qod (for any reason)
NO
Continue fluconazoleuntil day +75
Posaconazole 200 mg po tiduntil discontinuation of steroids
YES
Continue therapy
Hold voriconazole or posaconazole at conditioningSubstitute: Ambisome 5 mg/kg/day or micafungin 100 mg/day
Restart vori/posa therapy on day 0Obtaining ID input for stopping post-transplant
Reduction of Invasive Aspergillosis
• Despite constant construction at SCCA Outpatient Clinic and UWMC, number of aspergillus cases has dropped nearly 5-fold over last 7 years
• May be attributable to improved early diagnostics or prophylactic antifungal strategies
Conclusions (1)• Infections are a significant cause of morbidity and
mortality among neutropenic patients with cancer• Several well-defined risk factors help to identify
neutropenic patients at highest risk of infection and death
• Neutropenic patients are susceptible to many types of infection, including blood stream infections, pneumonia, urinary tract infections and intra-abdominal infections
• Antibiotic prophylaxis significantly reduces infections in neutropenic patients
Conclusions (2)• VRE is an increasing problem in cancer patients
and aggressive empiric therapy is warranted• Prevention and treatment of mould infections is
an emerging area of research• Rational use of antibiotics is essential to prevent
toxicities, resistance and unnecessary costs– Understand antimicrobial spectrum– Change antibiotics for well-defined and validated
reasons– Follow FHCRC Standard Practice Algorithms and
consult FHCRC Infectious Disease attendings with questions