25
INFECTIONS in patients with CANCER ANN MEREDITH U. GARCIA, MD, FPCP, DPSMO, MCMMO Internal Medicine − Medical Oncology
| Date post: | 16-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | ann-meredith-garcia |
| View: | 152 times |
| Download: | 2 times |
INFECTIONS in patients with
CANCER
ANN MEREDITH U. GARCIA, MD, FPCP, DPSMO, MCMMO Internal Medicine − Medical Oncology
INFECTIONS are a common cause of death and an even more common cause of morbidity in cancer patients.
§ Mostdeathsfromacuteleukemiaandhalfofdeathsfromlymphomaarecauseddirectlybyinfec6on.
§ Withmoreintensivechemotherapy,pa6entswithsolidtumorshavealsobecomemorelikelytodieofinfec6on.

An evolving approach to prevention and treatment of infectious complications of cancer has decreased infection-associated mortality rates.
§ “Earlyempirical”an6bio6cs
§ “Empirical”an6fungaltherapy– Administeredtoneutropenicpa6entswho,aAer4–7daysof
an6bio6ctherapy,remainfebrilebuthavenoposi6vecultures
§ Broad-spectrumprophylac6can6bio6csforafebrileneutropenicpa6ents

SPECIFICLESION ORGANISM DISEASE CANCERASSOCIATION
Breaksinskin Staphylococci,streptococci CelluliBs,extensiveskininfecBon
Head&neck,squamouscellCA
NodedissecBon CelluliBs BreastCAsurgery
Occlusionoforifices:ureters,bileduct,colon
Gram-negaBvebacilli Rapid,overwhelmingsepsis;urinarytractinfecBon
Renal,ovarian,biliarytree,metastaBcdiseases
Splenectomy S.pneumoniae,H.influenzae,N.meningi2dis
Rapid,overwhelmingsepsis
Hodgkinlymphoma,leukemia
LackofanBbody
InfecBonswithencapsulatedorganisms,sinusiBs,pneumonia
ChroniclymphocyBcleukemia,mulBplemyeloma
Lackofgranulocytes
Staphylococci,streptococci,entericorganisms,fungi
Bacteremia Acutemyeloid´lymphocyBcleukemias,hairycellleukemia
LackofTcells Mycobacteriumtuberculosis,Listeria,herpesviruses,fungi,intracellularparasites
InfecBonswithintracellularbacteria,fungi,parasites;virusreacBvaBon
Hodgkinlymphoma,leukemia,Tcelllymphoma
Disruption of normal barriers may predispose to infections in patients with cancer.

The level of suspicion of infections with certain organisms should depend on the type of cancer.
CANCER IMMUNEABNORMALITY ORGANISMSCAUSINGINFECTION
MulBplemyeloma Hypogammaglobulinemia S.pneumoniae,H.influenzae,N.meningi2dis
ChroniclymphocyBcleukemia
AcutemyeloidorlymphocyBcleukemia
Granulocytopenia,skin&mucousmembranelesions
ExtracellularGram-posiBve&Gram-negaBvebacteria,fungi
Hodgkinlymphoma AbnormalTcellfuncBon Intracellularpathogens(Mycobacteriumtuberculosis,Listeria,Salmonella,Cryptococcus,Mycobacteriumavium),herpesviruses
Hairycellleukemia
Non-Hodgkinlymphoma,acutelymphocyBcleukemia
GlucocorBcoidtherapy,T&BcelldysfuncBon
Pneumocys2s
Colon&rectaltumors LocalabnormaliBes Streptococcusbovis

Patients with cancer are likely to manifest their infections in characteristic ways. § Fevercon6nuestobeareliableindicatorin
neutropenicpa6ents.
§ Pa6entsreceivingglucocor6coidsandagentsthatimpairTcellfunc6onandcytokinesecre6onmayhaveseriousinfec6onsintheabsenceoffever.
§ Neutropenicpa6entscommonlypresentwithcelluli6swithoutpurulenceandwithpneumoniawithoutsputumorevenX-rayfindings.

SKIN-SPECIFIC SYNDROMES § Skinlesionsarecommonincancerpa6ents,andtheirappearance
maypermitthediagnosisofsystemicbacterialorfungalinfec6on.
SKINLESION ORGANISM/CONDITION REMARKS
CelluliBs –Mostcommon:GroupAStreptococcus,Staphylococcusaureus–UnusualorganismsinneutropenicpaBents:E.coli,Pseudomonas,fungi
–SignsofinfecBonareoYenlacking,butmayspreadrapidlyinneutropenicpaBents
Ecthymagangrenosum
–PseudomonasaeruginosabacteremiainneutropenicpaBents
–Painless,round,necroBclesionwithacentralblackorgray-blackeschar&surroundingerythema
Maculopapularrash
–Candidemia

SKIN-SPECIFIC SYNDROMES § Skinlesionsarecommonincancerpa6ents,andtheirappearance
maypermitthediagnosisofsystemicbacterialorfungalinfec6on.
SKINLESION ORGANISM/CONDITION REMARKS
Sweetsyndromeorfebrileneutrophilicdermatosis
–MostoYenassociatedwithacutemyeloidleukemia&otherneutropenicpaBentswithcancer
–Redorbluish-redpapulesornodulesthatmaycoalesceandformsharplyborderedplaques–Accompaniedbyhighfevers&anelevatederythrocytesedimentaBonrate
ErythemamulBforme
–Herpessimplexvirus –Accompaniedbymucousmebraneinvolvement

PART 7Oncology and Hematology
486 TABLE 104-3 INFECTIONS ASSOCIATED WITH SPECIFIC TYPES OF CANCER
CancerUnderlying Immune Abnormality
Organisms Causing Infection
Multiple myeloma Hypogammaglobulinemia Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis
Chronic lympho-cytic leukemia
Hypogammaglobulinemia S. pneumoniae, H. influenzae, N. meningitidis
Acute myeloid or lymphocytic leukemia
Granulocytopenia, skin and mucous membrane lesions
Extracellular gram-positive and gram-negative bacteria, fungi
Hodgkin’s disease Abnormal T cell function Intracellular patho-gens (Mycobacterium tuberculosis, Listeria, Salmonella, Cryptococcus, Mycobacterium avium); herpesviruses
Non-Hodgkin’s lymphoma and acute lympho-cytic leukemia
Glucocorticoid chemo-therapy, T and B cell dysfunction
Pneumocystis
Colon and rectal tumors
Local abnormalitiesa Streptococcus bovis biotype 1 (bacteremia)
Hairy cell leukemia
Abnormal T cell function Intracellular pathogens (M. tuberculosis, Listeria, Cryptococcus, M. avium)
aThe reason for this association is not well defined.
FIGURE 1041 A. Papules related to Escherichia coli bacteremia in a patient with acute lymphocytic leukemia. B. The same lesions on the following day.
A B
Streptococcus or Staphylococcus is common, neutropenic patients—i.e., those with <500 functional polymorphonuclear leukocytes (PMNs)/μL—and patients with impaired blood or lymphatic drainage may develop infections with unusual organisms. Innocent-looking macules or papules may be the first sign of bacterial or fungal sepsis in immu-nocompromised patients (Fig. 104-1). In the neutropenic host, a mac-ule progresses rapidly to ecthyma gangrenosum (see Fig. 25e-35), a usually painless, round, necrotic lesion consisting of a central black or gray-black eschar with surrounding erythema. Ecthyma gangrenosum, which is located in nonpressure areas (as distinguished from necrotic lesions associated with lack of circulation), is often associated with Pseudomonas aeruginosa bacteremia (Chap. 189) but may be caused by other bacteria.
Candidemia (Chap. 240) is also associated with a variety of skin conditions (see Fig. 25e-38) and commonly presents as a maculo-papular rash. Punch biopsy of the skin may be the best method for diagnosis.
Cellulitis, an acute spreading inflammation of the skin, is most often caused by infection with group A Streptococcus or Staphylococcus aureus, virulent organisms normally found on the skin (Chap. 156). Although cellulitis tends to be circumscribed in normal hosts, it may spread rapidly in neutropenic patients. A tiny break in the skin may lead to spreading cellulitis, which is characterized by pain and ery-thema; in the affected patients, signs of infection (e.g., purulence) are often lacking. What might be a furuncle in a normal host may require amputation because of uncontrolled infection in a patient presenting with leukemia. A dramatic response to an infection that might be triv-ial in a normal host can mark the first sign of leukemia. Fortunately, granulocytopenic patients are likely to be infected with certain types of organisms (Table 104-4); thus the selection of an antibiotic regi-men is somewhat easier than it might otherwise be (see “Antibacterial Therapy,” below). It is essential to recognize cellulitis early and to treat it aggressively. Patients who are neutropenic or who have previ-ously received antibiotics for other reasons may develop cellulitis with unusual organisms (e.g., Escherichia coli, Pseudomonas, or fungi). Early treatment, even of innocent-looking lesions, is essential to pre-vent necrosis and loss of tissue. Debridement to prevent spread may sometimes be necessary early in the course of disease, but it can often be performed after chemotherapy, when the PMN count increases.
TABLE 104-4 ORGANISMS LIKELY TO CAUSE INFECTIONS IN GRANULOCYTOPENIC PATIENTS
Gram-Positive CocciStaphylococcus epidermidis Staphylococcus aureus
Viridans Streptococcus Enterococcus faecalis
Streptococcus pneumoniae
Gram-Negative BacilliEscherichia coli Serratia spp.
Klebsiella spp. Acinetobacter spp.a
Pseudomonas aeruginosa Stenotrophomonas spp.
Enterobacter spp. Citrobacter spp.
Non-aeruginosa Pseudomonas spp.a
Gram-Positive BacilliDiphtheroids JK bacillusa
FungiCandida spp. Mucor/Rhizopus
Aspergillus spp.aOften associated with intravenous catheters.
HPIM19_Part07(A)_p0467-p0619.indd 486 2/9/15 6:04 PM

CATHETER-RELATED INFECTIONS § IVcathetersarecommonlyusedincancerchemotherapyandare
pronetocauseinfec6on.§ Somecatheter-associatedinfec6onscanbetreatedwithan6bio6cs,
whereasinothersthecathetermustberemoved.
CHAPTER 104Infections in Patients with Cancer
487Sweet syndrome, or febrile neutrophilic dermatosis, was originally described in women with elevated white blood cell (WBC) counts. The disease is characterized by the presence of leukocytes in the lower dermis, with edema of the papillary body. Ironically, this disease now is usually seen in neutropenic patients with cancer, most often in associa-tion with acute myeloid leukemia (AML) but also in association with a variety of other malignancies. Sweet syndrome usually presents as red or bluish-red papules or nodules that may coalesce and form sharply bordered plaques (see Fig. 25e-41). The edema may suggest vesicles, but on palpation the lesions are solid, and vesicles probably never arise in this disease. The lesions are most common on the face, neck, and arms. On the legs, they may be confused with erythema nodosum (see Fig. 25e-40). The development of lesions is often accompanied by high fevers and an elevated erythrocyte sedimentation rate. Both the lesions and the temperature elevation respond dramatically to glucocorticoid administration. Treatment begins with high doses of glucocorti-coids (prednisone, 60 mg/d) followed by tapered doses over the next 2–3 weeks.
Data indicate that erythema multiforme (see Fig. 25e-25) with mucous membrane involvement is often associated with herpes simplex virus (HSV) infection and is distinct from Stevens-Johnson syndrome, which is associated with drugs and tends to have a more widespread distribution. Because cancer patients are both immu-nosuppressed (and therefore susceptible to herpes infections) and heavily treated with drugs (and therefore subject to Stevens-Johnson syndrome [see Fig. 46e-4]), both of these conditions are common in this population.
Cytokines, which are used as adjuvants or primary treatments for cancer, can themselves cause characteristic rashes, further compli-cating the differential diagnosis. This phenomenon is a particular problem in bone marrow transplant recipients (Chap. 169), who, in addition to having the usual chemotherapy-, antibiotic-, and cytokine-induced rashes, are plagued by graft-versus-host disease.
CATHETERRELATED INFECTIONSBecause IV catheters are commonly used in cancer chemotherapy and are prone to cause infection (Chap. 168), they pose a major problem in the care of patients with cancer. Some catheter-associated infections can be treated with antibiotics, whereas in others the catheter must be removed (Table 104-5). If the patient has a “tunneled” catheter (which consists of an entrance site, a subcutaneous tunnel, and an exit site), a red streak over the subcutaneous part of the line (the tunnel) is grounds
for immediate device removal. Failure to remove catheters under these circumstances may result in extensive cellulitis and tissue necrosis.
More common than tunnel infections are exit-site infections, often with erythema around the area where the line penetrates the skin. Most authorities (Chap. 172) recommend treatment (usually with vancomycin) for an exit-site infection caused by coagulase-negative Staphylococcus. Treatment of coagulase-positive staphylococcal infec-tion is associated with a poorer outcome, and it is advisable to remove the catheter if possible. Similarly, most clinicians remove catheters associated with infections due to P. aeruginosa and Candida species, because such infections are difficult to treat and bloodstream infections with these organisms are likely to be deadly. Catheter infections caused by Burkholderia cepacia, Stenotrophomonas species, Agrobacterium species, Acinetobacter baumannii, Pseudomonas species other than aeruginosa, and carbapenem-resistant Enterobacteriaceae are likely to be very difficult to eradicate with antibiotics alone. Similarly, isola-tion of Bacillus, Corynebacterium, and Mycobacterium species should prompt removal of the catheter.
GASTROINTESTINAL TRACTSPECIFIC SYNDROMESUpper Gastrointestinal Tract Disease INFECTIONS OF THE MOUTH The oral cavity is rich in aerobic and anaero-bic bacteria (Chap. 201) that normally live in a commensal relation-ship with the host. The antimetabolic effects of chemotherapy cause a breakdown of mucosal host defenses, leading to ulceration of the mouth and the potential for invasion by resident bacteria. Mouth ulcerations afflict most patients receiving cytotoxic chemotherapy and have been associated with viridans streptococcal bacteremia. Candida infections of the mouth are very common. Fluconazole is clearly effec-tive in the treatment of both local infections (thrush) and systemic infections (esophagitis) due to Candida albicans. Other azoles (e.g., voriconazole) as well as echinocandins offer similar efficacy as well as activity against the fluconazole-resistant organisms that are associated with chronic fluconazole treatment (Chap. 240).
Noma (cancrum oris), commonly seen in malnourished children, is a penetrating disease of the soft and hard tissues of the mouth and adjacent sites, with resulting necrosis and gangrene. It has a counter-part in immunocompromised patients and is thought to be due to invasion of the tissues by Bacteroides, Fusobacterium, and other nor-mal inhabitants of the mouth. Noma is associated with debility, poor oral hygiene, and immunosuppression.
TABLE 104-5 APPROACH TO CATHETER INFECTIONS IN IMMUNOCOMPROMISED PATIENTSClinical Presentation or Isolated Pathogen Catheter Removal Antibiotics Comments
Evidence of Infection, Negative Blood CulturesExit-site erythema Not necessary if infection
responds to treatmentUsually, begin treatment for gram-positive cocci.
Coagulase-negative staphylococci are most common.
Tunnel-site erythema Required Treat for gram-positive cocci pending culture results.
Failure to remove the catheter may lead to necrosis of the involved area requiring skin grafts in the future.
Blood Culture–Positive InfectionsCoagulase-negative staphylococci Line removal optimal but may
be unnecessary if patient is clinically stable and responds to antibiotics
Usually, start with vancomycin. Linezolid, quinupristin/dalfopristin, and daptomycin are alternative agents.
If there are no contraindications to line removal, this course of action is optimal. If the line is removed, antibiotics may not be necessary.
Other gram-positive cocci (e.g., Staphylococcus aureus, Enterococcus); gram-positive rods (Bacillus, Corynebacterium spp.)
Recommended Treat with antibiotics to which the organism is sensitive, with duration based on the clinical setting.
The incidence of metastatic infections following S. aureus infection and the difficulty of treating enterococcal infection make line removal the recommended course of action. In addition, gram-positive rods do not respond readily to antibiotics alone.
Gram-negative bacteria Recommended Use an agent to which the organism is shown to be sensitive.
Organisms like Stenotrophomonas, Pseudomonas, and Burkholderia are notoriously hard to treat, as are carbapenem-resistant organisms.
Fungi Recommended — Fungal infections of catheters are extremely difficult to treat.
HPIM19_Part07(A)_p0467-p0619.indd 487 2/9/15 6:04 PM
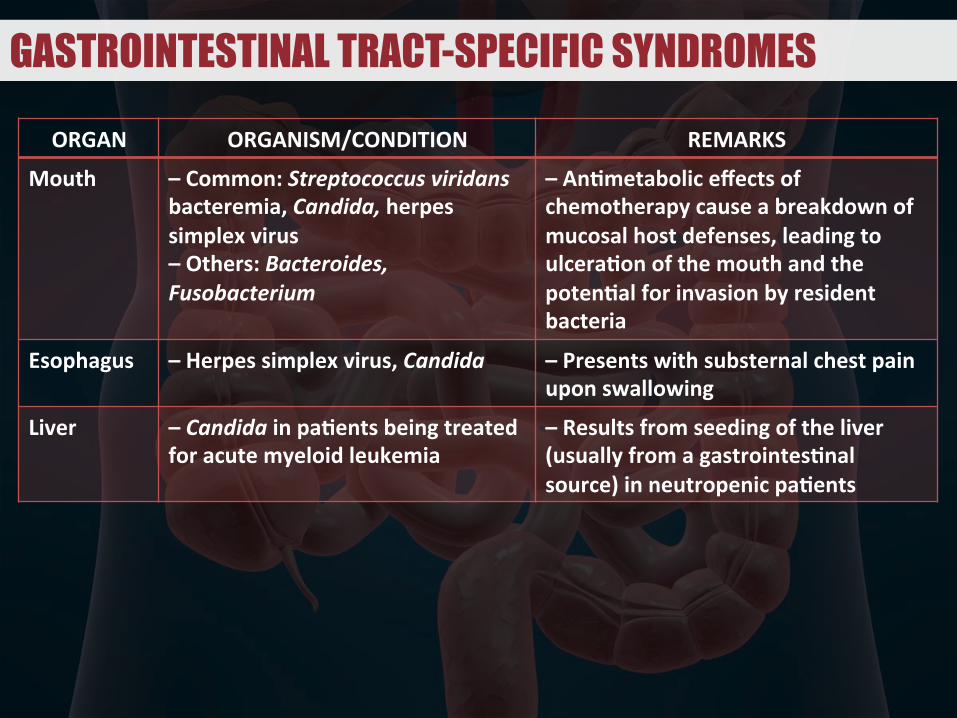
GASTROINTESTINAL TRACT-SPECIFIC SYNDROMES
ORGAN ORGANISM/CONDITION REMARKS
Mouth –Common:Streptococcusviridansbacteremia,Candida,herpessimplexvirus–Others:Bacteroides,Fusobacterium
–AnBmetaboliceffectsofchemotherapycauseabreakdownofmucosalhostdefenses,leadingtoulceraBonofthemouthandthepotenBalforinvasionbyresidentbacteria
Esophagus –Herpessimplexvirus,Candida –Presentswithsubsternalchestpainuponswallowing
Liver –CandidainpaBentsbeingtreatedforacutemyeloidleukemia
–Resultsfromseedingoftheliver(usuallyfromagastrointesBnalsource)inneutropenicpaBents

GASTROINTESTINAL TRACT-SPECIFIC SYNDROMES
ORGAN ORGANISM/CONDITION REMARKS
IntesBne –TyphliBs,necroBzing/neutropeniccoliBs,necroBzingenteropathy,ileocecalsyndrome,ceciBs:MorecommoninpaBentswithacutemyeloidorlymphocyBcleukemia,especiallyinneutropenicpaBentsaYerchemotherapy
–Presentsasfever&rightlowerquadrant(orgeneralizedabdominal)tenderness–OYenaccompaniedbybloodydiarrhea
–Clostridiumdifficile-induceddiarrhea
–ShouldalwaysbeconsideredasapossiblecauseofdiarrheaincancerpaBentswhohavereceivedeitherchemotherapyoranBbioBcs
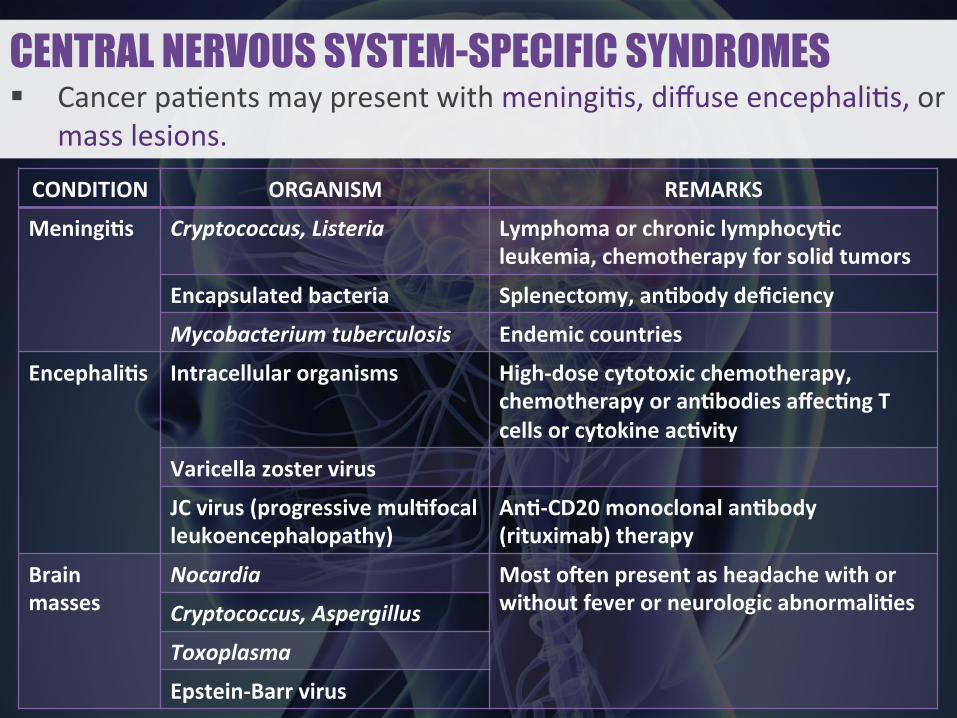
CENTRAL NERVOUS SYSTEM-SPECIFIC SYNDROMES § Cancerpa6entsmaypresentwithmeningi6s,diffuseencephali6s,or
masslesions.
CONDITION ORGANISM REMARKS
MeningiBs Cryptococcus,Listeria LymphomaorchroniclymphocyBcleukemia,chemotherapyforsolidtumors
Encapsulatedbacteria Splenectomy,anBbodydeficiency
Mycobacteriumtuberculosis Endemiccountries
EncephaliBs Intracellularorganisms High-dosecytotoxicchemotherapy,chemotherapyoranBbodiesaffecBngTcellsorcytokineacBvity
Varicellazostervirus
JCvirus(progressivemulBfocalleukoencephalopathy)
AnB-CD20monoclonalanBbody(rituximab)therapy
Brainmasses
Nocardia MostoYenpresentasheadachewithorwithoutfeverorneurologicabnormaliBesCryptococcus,Aspergillus
Toxoplasma
Epstein-Barrvirus
PART 7Oncology and Hematology
488 Viruses, particularly HSV, are a prominent cause of morbidity in immunocompromised patients, in whom they are associated with severe mucositis. The use of acyclovir, either prophylactically or thera-peutically, is of value.ESOPHAGEAL INFECTIONS The differential diagnosis of esophagitis (usu-ally presenting as substernal chest pain upon swallowing) includes herpes simplex and candidiasis, both of which are readily treatable.
Lower Gastrointestinal Tract Disease Hepatic candidiasis (Chap. 240) results from seeding of the liver (usually from a gastrointestinal source) in neutropenic patients. It is most common among patients being treated for AML and usually presents symptomatically around the time the neutropenia resolves. The characteristic picture is that of persistent fever unresponsive to antibiotics, abdominal pain and tenderness or nausea, and elevated serum levels of alkaline phosphatase in a patient with hematologic malignancy who has recently recovered from neutro-penia. The diagnosis of this disease (which may present in an indolent manner and persist for several months) is based on the finding of yeasts or pseudohyphae in granulomatous lesions. Hepatic ultrasound or CT may reveal bull’s-eye lesions. MRI scans reveal small lesions not visible by other imaging modalities. The pathology (a granulomatous response) and the timing (with resolution of neutropenia and an eleva-tion in granulocyte count) suggest that the host response to Candida is an important component of the manifestations of disease. In many cases, although organisms are visible, cultures of biopsied material may be negative. The designation hepatosplenic candidiasis or hepatic candi-diasis is a misnomer because the disease often involves the kidneys and other tissues; the term chronic disseminated candidiasis may be more appropriate. Because of the risk of bleeding with liver biopsy, diag-nosis is often based on imaging studies (MRI, CT). Treatment should be directed to the causative agent (usually C. albicans but sometimes Candida tropicalis or other less common Candida species).
Typhlitis Typhlitis (also referred to as necrotizing colitis, neutropenic colitis, necrotizing enteropathy, ileocecal syndrome, and cecitis) is a clinical syndrome of fever and right-lower-quadrant (or generalized abdominal) tenderness in an immunosuppressed host. This syndrome is classically seen in neutropenic patients after chemotherapy with cytotoxic drugs. It may be more common among children than among adults and appears to be much more common among patients with AML or ALL than among those with other types of cancer. Physical examination reveals right-lower-quadrant tenderness, with or without rebound tenderness. Associated diarrhea (often bloody) is common, and the diagnosis can be confirmed by the finding of a thickened cecal wall on CT, MRI, or ultrasonography. Plain films may reveal a right-lower-quadrant mass, but CT with contrast or MRI is a much more sensitive means of diagnosis. Although surgery is sometimes attempted to avoid perforation from ischemia, most cases resolve with medical therapy alone. The disease is sometimes associated with positive blood cultures (which usually yield aerobic gram-negative bacilli), and therapy is recommended for a broad spectrum of bacteria (particularly gram-negative bacilli, which are likely to be found in the bowel flora). Surgery is indicated in the case of perforation.
Clostridium difficile–Induced Diarrhea Patients with cancer are predis-posed to the development of C. difficile diarrhea (Chap. 161) as a consequence of chemotherapy alone. Thus, they may test positive for C. difficile even without receiving antibiotics. Obviously, such patients are also subject to C. difficile–induced diarrhea as a result of antibiotic pressure. C. difficile should always be considered as a possible cause of diarrhea in cancer patients who have received either chemotherapy or antibiotics.
CENTRAL NERVOUS SYSTEMSPECIFIC SYNDROMESMeningitis The presentation of meningitis in patients with lymphoma or CLL and in patients receiving chemotherapy (particularly with glucocorticoids) for solid tumors suggests a diagnosis of cryptococ-cal or listerial infection. As noted previously, splenectomized patients are susceptible to rapid, overwhelming infection with encapsulated bacteria (including S. pneumoniae, H. influenzae, and N. meningitidis).
Similarly, patients who are antibody-deficient (e.g., those with CLL, those who have received intensive chemotherapy, or those who have undergone bone marrow transplantation) are likely to have infections caused by these bacteria. Other cancer patients, however, because of their defective cellular immunity, are likely to be infected with other pathogens (Table 104-3). Central nervous system (CNS) tuberculosis should be considered, especially in patients from countries where tuberculosis is highly prevalent in the population.
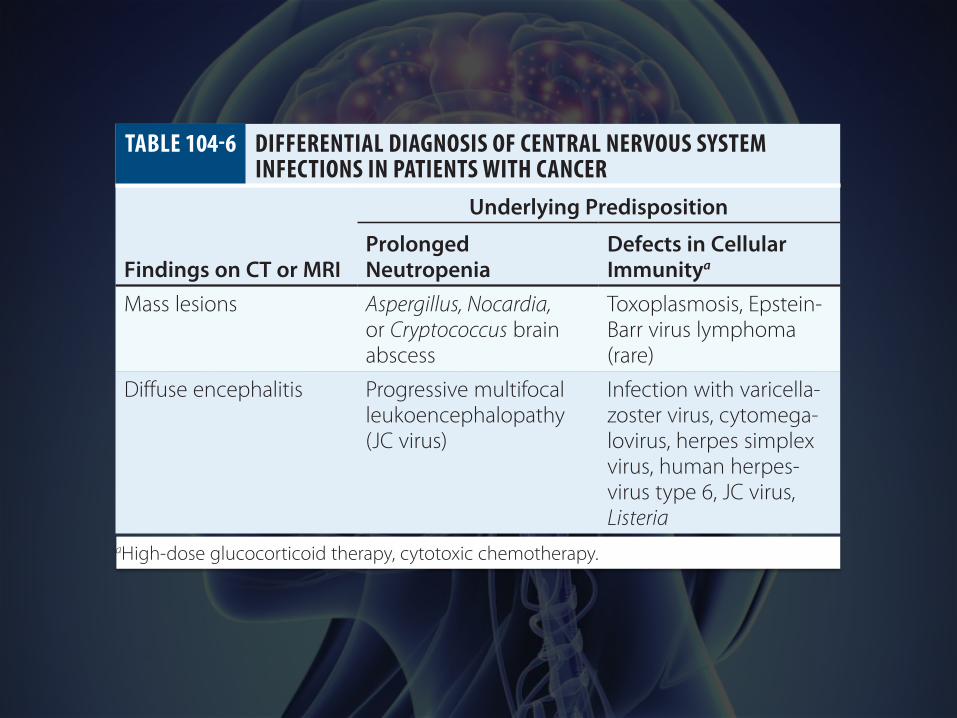
Encephalitis The spectrum of disease resulting from viral encephalitis is expanded in immunocompromised patients. A predisposition to infections with intracellular organisms similar to those encountered in patients with AIDS (Chap. 226) is seen in cancer patients receiving (1) high-dose cytotoxic chemotherapy, (2) chemotherapy affecting T cell function (e.g., fludarabine), or (3) antibodies that eliminate T cells (e.g., anti-CD3, alemtuzumab, anti-CD52) or cytokine activity (anti–tumor necrosis factor agents or interleukin 1 receptor antagonists). Infection with varicella-zoster virus (VZV) has been associated with encephalitis that may be caused by VZV-related vasculitis. Chronic viral infections may also be associated with dementia and encepha-litic presentations. A diagnosis of progressive multifocal leukoen-cephalopathy (Chap. 164) should be considered when a patient who has received chemotherapy (rituximab in particular) presents with dementia (Table 104-6). Other abnormalities of the CNS that may be confused with infection include normal-pressure hydrocephalus and vasculitis resulting from CNS irradiation. It may be possible to differ-entiate these conditions by MRI.
Brain Masses Mass lesions of the brain most often present as head-ache with or without fever or neurologic abnormalities. Infections associated with mass lesions may be caused by bacteria (particularly Nocardia), fungi (particularly Cryptococcus or Aspergillus), or parasites (Toxoplasma). Epstein-Barr virus (EBV)–associated lymphoma may also present as single—or sometimes multiple—mass lesions of the brain. A biopsy may be required for a definitive diagnosis.
PULMONARY INFECTIONSPneumonia (Chap. 153) in immunocompromised patients may be dif-ficult to diagnose because conventional methods of diagnosis depend on the presence of neutrophils. Bacterial pneumonia in neutropenic patients may present without purulent sputum—or, in fact, without any sputum at all—and may not produce physical findings suggestive of chest consolidation (rales or egophony).
In granulocytopenic patients with persistent or recurrent fever, the chest x-ray pattern may help to localize an infection and thus to deter-mine which investigative tests and procedures should be undertaken and which therapeutic options should be considered (Table 104-7). In this setting, a simple chest x-ray is a screening tool; because the impaired host response results in less evidence of consolidation or infiltration, high-resolution CT is recommended for the diagnosis of pulmonary infections. The difficulties encountered in the man-agement of pulmonary infiltrates relate in part to the difficulties of performing diagnostic procedures on the patients involved. When platelet counts can be increased to adequate levels by transfusion,
TABLE 104-6 DIFFERENTIAL DIAGNOSIS OF CENTRAL NERVOUS SYSTEM INFECTIONS IN PATIENTS WITH CANCER
Underlying Predisposition
Findings on CT or MRIProlonged Neutropenia
Defects in Cellular Immunitya
Mass lesions Aspergillus, Nocardia, or Cryptococcus brain abscess
Toxoplasmosis, Epstein-Barr virus lymphoma (rare)
Diffuse encephalitis Progressive multifocal leukoencephalopathy (JC virus)
Infection with varicella-zoster virus, cytomega-lovirus, herpes simplex virus, human herpes-virus type 6, JC virus, Listeria
aHigh-dose glucocorticoid therapy, cytotoxic chemotherapy.
HPIM19_Part07(A)_p0467-p0619.indd 488 2/9/15 6:04 PM

PULMONARY INFECTIONS § Bacterialpneumoniasingranulocytopenichostspresentwitha
paucityofsigns,symptoms,orradiographicabnormali6es.§ Ingranulocytopenicpa6entswithpersistentorrecurrentfever,the
chestX-raypaRernmayhelptolocalizeaninfec6on.§ Becausetheimpairedhostresponseresultsinlessevidenceof
consolida6onorinfiltra6on,high-resolu6onCTisrecommendedforthediagnosisofpulmonaryinfec6ons.
CHAPTER 104Infections in Patients with Cancer
489
microscopic and microbiologic evaluation of the fluid obtained by endoscopic bronchial lavage is often diagnostic. Lavage fluid should be cultured for Mycoplasma, Chlamydia, Legionella, Nocardia, more common bacterial pathogens, fungi, and viruses. In addition, the pos-sibility of Pneumocystis pneumonia should be considered, especially in patients with ALL or lymphoma who have not received prophylactic trimethoprim-sulfamethoxazole (TMP-SMX). The characteristics of the infiltrate may be helpful in decisions about further diagnostic and therapeutic maneuvers. Nodular infiltrates suggest fungal pneumonia (e.g., that caused by Aspergillus or Mucor). Such lesions may best be approached by visualized biopsy procedures. It is worth noting that while bacterial pneumonias classically present as lobar infiltrates in normal hosts, bacterial pneumonias in granulocytopenic hosts present with a paucity of signs, symptoms, or radiographic abnormalities; thus, the diagnosis is difficult.
Aspergillus species (Chap. 241) can colonize the skin and respira-tory tract or cause fatal systemic illness. Although this fungus may cause aspergillomas in a previously existing cavity or may produce allergic bronchopulmonary disease in some patients, the major prob-lem posed by this genus in neutropenic patients is invasive disease, primarily due to Aspergillus fumigatus or Aspergillus flavus. The organ-isms enter the host following colonization of the respiratory tract, with subsequent invasion of blood vessels. The disease is likely to present as a thrombotic or embolic event because of this ability of the fungi to invade blood vessels. The risk of infection with Aspergillus correlates directly with the duration of neutropenia. In prolonged neutropenia, positive surveillance cultures for nasopharyngeal colonization with Aspergillus may predict the development of disease.
Patients with Aspergillus infection often present with pleuritic chest pain and fever, which are sometimes accompanied by cough. Hemoptysis may be an ominous sign. Chest x-rays may reveal new focal infiltrates or nodules. Chest CT may reveal a characteristic halo consist-ing of a mass-like infiltrate surrounded by an area of low attenuation. The presence of a “crescent sign” on chest x-ray or chest CT, in which the mass progresses to central cavitation, is characteristic of invasive Aspergillus infection but may develop as the lesions are resolving.
In addition to causing pulmonary disease, Aspergillus may invade through the nose or palate, with deep sinus penetration. The appear-ance of a discolored area in the nasal passages or on the hard palate should prompt a search for invasive Aspergillus. This situation is likely to require surgical debridement. Catheter infections with Aspergillus usually require both removal of the catheter and antifungal therapy.
Diffuse interstitial infiltrates suggest viral, parasitic, or Pneumocystis pneumonia. If the patient has a diffuse interstitial pattern on chest x-ray, it may be reasonable, while considering invasive diagnostic procedures, to institute empirical treatment for Pneumocystis with TMP-SMX and for Chlamydia, Mycoplasma, and Legionella with a quinolone or azithromycin. Noninvasive procedures, such as stain-ing of induced sputum smears for Pneumocystis, serum cryptococcal antigen tests, and urine testing for Legionella antigen, may be help-ful. Serum galactomannan and β-d-glucan tests may be of value in diagnosing Aspergillus infection, but their utility is limited by their lack of sensitivity and specificity. The presence of an elevated level of β-d-glucan in the serum of a patient being treated for cancer who is not receiving prophylaxis against Pneumocystis suggests the diagnosis
of Pneumocystis pneumonia. Infections with viruses that cause only upper respiratory symptoms in immunocompetent hosts, such as respiratory syncytial virus (RSV), influenza viruses, and parainfluenza viruses, may be associated with fatal pneumonitis in immunocom-promised hosts. CMV reactivation occurs in cancer patients receiving chemotherapy, but CMV pneumonia is most common among HSCT recipients (Chap. 169). Polymerase chain reaction testing now allows rapid diagnosis of viral pneumonia, which can lead to treatment in some cases (e.g., influenza). Multiplex studies that can detect a wide array of viruses in the lung and upper respiratory tract are now avail-able and will lead to specific diagnoses of viral pneumonias.
Bleomycin is the most common cause of chemotherapy-induced lung disease. Other causes include alkylating agents (such as cyclo-phosphamide, chlorambucil, and melphalan), nitrosoureas (carmus-tine [BCNU], lomustine [CCNU], and methyl-CCNU), busulfan, procarbazine, methotrexate, and hydroxyurea. Both infectious and noninfectious (drug- and/or radiation-induced) pneumonitis can cause fever and abnormalities on chest x-ray; thus, the differential diagnosis of an infiltrate in a patient receiving chemotherapy encom-passes a broad range of conditions (Table 104-7). The treatment of radiation pneumonitis (which may respond dramatically to glucocor-ticoids) or drug-induced pneumonitis is different from that of infec-tious pneumonia, and a biopsy may be important in the diagnosis. Unfortunately, no definitive diagnosis can be made in ∼30% of cases, even after bronchoscopy.
Open-lung biopsy is the gold standard of diagnostic techniques. Biopsy via a visualized thoracostomy can replace an open procedure in many cases. When a biopsy cannot be performed, empirical treat-ment can be undertaken; a quinolone or an erythromycin derivative (azithromycin) and TMP-SMX are used in the case of diffuse infil-trates, and an antifungal agent is administered in the case of nodular infiltrates. The risks should be weighed carefully in these cases. If inap-propriate drugs are administered, empirical treatment may prove toxic or ineffective; either of these outcomes may be riskier than biopsy.
CARDIOVASCULAR INFECTIONSPatients with Hodgkin’s disease are prone to persistent infections by Salmonella, sometimes (and particularly often in elderly patients) affecting a vascular site. The use of IV catheters deliberately lodged in the right atrium is associated with a high incidence of bacterial endo-carditis, presumably related to valve damage followed by bacteremia. Nonbacterial thrombotic endocarditis (marantic endocarditis) has been described in association with a variety of malignancies (most often solid tumors) and may follow bone marrow transplantation as well. The presentation of an embolic event with a new cardiac murmur suggests this diagnosis. Blood cultures are negative in this disease of unknown pathogenesis.
ENDOCRINE SYNDROMESInfections of the endocrine system have been described in immuno-compromised patients. Candida infection of the thyroid may be dif-ficult to diagnose during the neutropenic period. It can be defined by indium-labeled WBC scans or gallium scans after neutrophil counts increase. CMV infection can cause adrenalitis with or without result-ing adrenal insufficiency. The presentation of a sudden endocrine anomaly in an immunocompromised patient can be a sign of infection in the involved end organ.
MUSCULOSKELETAL INFECTIONSInfection that is a consequence of vascular compromise, resulting in gangrene, can occur when a tumor restricts the blood supply to mus-cles, bones, or joints. The process of diagnosis and treatment of such infection is similar to that in normal hosts, with the following caveats:
1. In terms of diagnosis, a lack of physical findings resulting from a lack of granulocytes in the granulocytopenic patient should make the clinician more aggressive in obtaining tissue rather than more willing to rely on physical signs.
2. In terms of therapy, aggressive debridement of infected tissues may be required. However, it is usually difficult to operate on patients
TABLE 104-7 DIFFERENTIAL DIAGNOSIS OF CHEST INFILTRATES IN IMMUNOCOMPROMISED PATIENTS
Cause of Pneumonia
Infiltrate Infectious NoninfectiousLocalized Bacteria (including Legionella,
mycobacteria)Local hemorrhage or embolism, tumor
Nodular Fungi (e.g., Aspergillus or Mucor), Nocardia
Recurrent tumor
Diffuse Viruses (especially cytomegalovirus), Chlamydia, Pneumocystis, Toxoplasma gondii, mycobacteria
Congestive heart failure, radiation pneumonitis, drug-induced lung injury, lymphangitic spread of cancer
HPIM19_Part07(A)_p0467-p0619.indd 489 2/9/15 6:04 PM

CARDIOVASCULAR INFECTIONS § Pa6entswithHodgkinlymphomaarepronetopersistentinfec6ons
bySalmonella.§ TheuseofIVcathetersdeliberatelylodgedintherightatriumis
associatedwithahighincidenceofbacterialendocardi6s.§ Nonbacterialthrombo6cendocardi6s(maran6cendocardi6s)has
beendescribedmostoAeninassocia6onwithsolidtumorsandmayalsofollowbonemarrowtransplanta6on.Thepresenta6onofanemboliceventwithanewcardiacmurmursuggeststhisdiagnosis.

MUSCULOSKELETAL INFECTIONS § Infec6onthatisaconsequenceofvascularcompromise,resul6ngin
gangrene,canoccurwhenatumorrestrictsthebloodsupplytomuscles,bones,orjoints.
§ Alackofphysicalfindingsinthegranulocytopenicpa6entshouldmaketheclinicianmoreaggressiveinobtaining6ssueratherthanmorewillingtorelyonphysicalsigns.
§ Aggressivedebridementofinfected6ssuesmayberequired.§ Examples:Clostridiumperfringens,Clostridiumsep5cum,
Streptococcusbovis
RENAL & URETERAL INFECTIONS § Infec6onsoftheurinarytractarecommonamongpa6entswhose
ureteralexcre6oniscompromised.§ Candida,whichhasapredilec6onforthekidney,caninvadeeither
fromthebloodstreamorinaretrogrademannerinimmunocom-promisedpa6ents.
§ Certainvirusesaretypicallyseenonlyinimmunosuppressedpa6ents,suchastheBKvirusandadenovirus.

PART 7Oncology and Hematology
490 who have recently received chemotherapy, both because of a lack of platelets (which results in bleeding complications) and because of a lack of WBCs (which may lead to secondary infection). A blood culture positive for Clostridium perfringens—an organism commonly associated with gas gangrene—can have a number of meanings (Chap. 179). Clostridium septicum bacteremia is associ-ated with the presence of an underlying malignancy. Bloodstream infections with intestinal organisms such as Streptococcus bovis biotype 1 and C. perfringens may arise spontaneously from lower gastrointestinal lesions (tumor or polyps); alternatively, these lesions may be harbingers of invasive disease. The clinical setting must be considered in order to define the appropriate treatment for each case.
RENAL AND URETERAL INFECTIONSInfections of the urinary tract are common among patients whose ureteral excretion is compromised (Table 104-1). Candida, which has a predilection for the kidney, can invade either from the bloodstream or in a retrograde manner (via the ureters or bladder) in immunocom-promised patients. The presence of “fungus balls” or persistent candi-duria suggests invasive disease. Persistent funguria (with Aspergillus as well as Candida) should prompt a search for a nidus of infection in the kidney.
Certain viruses are typically seen only in immunosuppressed patients. BK virus (polyomavirus hominis 1) has been documented in the urine of bone marrow transplant recipients and, like adenovirus, may be associated with hemorrhagic cystitis.
ABNORMALITIES THAT PREDISPOSE TO INFECTION(Table 104-1)
THE LYMPHOID SYSTEMIt is beyond the scope of this chapter to detail how all the immuno-logic abnormalities that result from cancer or from chemotherapy for cancer lead to infections. Disorders of the immune system are discussed in other sections of this book. As has been noted, patients with antibody deficiency are predisposed to overwhelming infection with encapsulated bacteria (including S. pneumoniae, H. influenzae, and N. meningitidis). Infections that result from the lack of a functional cellular immune system are described in Chap. 226. It is worth men-tioning, however, that patients undergoing intensive chemotherapy for any form of cancer will have not only defects due to granulocyto-penia but also lymphocyte dysfunction, which may be profound. Thus, these patients—especially those receiving glucocorticoid-containing regimens or drugs that inhibit either T cell activation (calcineurin inhibitors or drugs like fludarabine, which affect lymphocyte function) or cytokine induction—should be given prophylaxis for Pneumocystis pneumonia.
Patients receiving treatment that eliminates B cells (e.g., with anti-CD20 antibodies or rituximab) are especially vulnerable to intercurrent viral infections. The incidence of progressive multifocal leukoencephalopathy (caused by JC virus) is elevated in these patients.
THE HEMATOPOIETIC SYSTEMInitial studies in the 1960s revealed a dramatic increase in the incidence of infections (fatal and nonfatal) among cancer patients with a granulocyte count of <500/μL. The use of
prophylactic antibacterial agents has reduced the number of bacterial infections, but 35–78% of febrile neutropenic patients being treated for hematologic malignancies develop infections at some time during chemotherapy. Aerobic pathogens (both gram-positive and gram-negative) predominate in all series, but the exact organisms isolated vary from center to center. Infections with anaerobic organisms are uncommon. Geographic patterns affect the types of fungi isolated. Tuberculosis and malaria are common causes of fever in the develop-ing world and may present in this setting as well.
Neutropenic patients are unusually susceptible to infection with a wide variety of bacteria; thus, antibiotic therapy should be initiated
promptly to cover likely pathogens if infection is suspected. Indeed, early initiation of antibacterial agents is mandatory to prevent deaths. Like most immunocompromised patients, neutropenic patients are threatened by their own microbial flora, including gram-positive and gram-negative organisms found commonly on the skin and mucous membranes and in the bowel (Table 104-4). Because treatment with narrow-spectrum agents leads to infection with organisms not covered by the antibiotics used, the initial regimen should target all pathogens likely to be the initial causes of bacterial infection in neutropenic hosts. As noted in the algorithm shown in Fig. 104-2, administra-tion of antimicrobial agents is routinely continued until neutropenia resolves—i.e., the granulocyte count is sustained above 500 μL for at least 2 days. In some cases, patients remain febrile after resolution of neutropenia. In these instances, the risk of sudden death from over-whelming bacteremia is greatly reduced, and the following diagnoses should be seriously considered: (1) fungal infection, (2) bacterial abscesses or undrained foci of infection, and (3) drug fever (includ-ing reactions to antimicrobial agents as well as to chemotherapy or cytokines). In the proper setting, viral infection or graft-versus-host disease should be considered. In clinical practice, antibacterial therapy is usually discontinued when the patient is no longer neutropenic and all evidence of bacterial disease has been eliminated. Antifungal agents are then discontinued if there is no evidence of fungal disease. If the patient remains febrile, a search for viral diseases or unusual pathogens is conducted while unnecessary cytokines and other drugs are system-atically eliminated from the regimen.
TREATMENT INFECTIONS IN CANCER PATIENTSANTIBACTERIAL THERAPYHundreds of antibacterial regimens have been tested for use in patients with cancer. The major risk of infection is related to the degree of neutropenia seen as a consequence of either the disease or the therapy. Many of the relevant studies have involved small populations in which the outcomes have generally been good, and most have lacked the statistical power to detect differences among the regimens studied. Each febrile neutropenic patient should be approached as a unique problem, with particular attention given to previous infections and recent antibiotic exposures. Several general
Continue treatment until neutropenia resolves (granulocyte count > 500/μL).
Add a broad- spectrum antifungal agent.
FebrileAfebrile
Initialevaluation
Initialtherapy
Follow-up
Subsequenttherapy
Physical examination: skin lesions, mucous membranes, IV catheter sites, perirectal areaGranulocyte count: absolute count < 500/μL; expected duration of neutropeniaBlood cultures; chest radiogram; other appropriate studies based on history (sputum, urine, skin biopsy)
Treat with antibiotic(s) effective against both gram-negative and gram-positive aerobes.
Treat the infection with the best available antibiotics. Do not narrow the spectrum unnecessarily. Continue to treat for both gram-positive and gram-negative aerobes.
Obvious infectious site found
No obvious infectious site
Continue regimen.
FIGURE 1042 Algorithm for the diagnosis and treatment of fever and neutropenia.
HPIM19_Part07(A)_p0467-p0619.indd 490 2/9/15 6:04 PM

CHAPTER 104Infections in Patients with Cancer
491guidelines are useful in the initial treatment of neutropenic patients with fever (Fig. 104-2):
1. In the initial regimen, it is necessary to use antibiotics active against both gram-negative and gram-positive bacteria (Table 104-4).
2. Monotherapy with an aminoglycoside or an antibiotic lacking good activity against gram-positive organisms (e.g., ciprofloxa-cin or aztreonam) is not adequate in this setting.
3. The agents used should reflect both the epidemiology and the antibiotic resistance pattern of the hospital.
4. If the pattern of resistance justifies its use, a single third-genera-tion cephalosporin constitutes an appropriate initial regimen in many hospitals.
5. Most standard regimens are designed for patients who have not previously received prophylactic antibiotics. The development of fever in a patient who has received antibiotics affects the choice of subsequent therapy, which should target resistant organisms and organisms known to cause infections in patients being treated with the antibiotics already administered.
6. Randomized trials have indicated the safety of oral antibiotic regimens in the treatment of “low-risk” patients with fever and neutropenia. Outpatients who are expected to remain neutrope-nic for <10 days and who have no concurrent medical problems (such as hypotension, pulmonary compromise, or abdominal pain) can be classified as low risk and treated with a broad-spectrum oral regimen.
7. Several large-scale studies indicate that prophylaxis with a fluo-roquinolone (ciprofloxacin or levofloxacin) decreases morbidity and mortality rates among afebrile patients who are anticipated to have neutropenia of long duration.
Commonly used antibiotic regimens for the treatment of febrile patients in whom prolonged neutropenia (>7 days) is anticipated include (1) ceftazidime or cefepime, (2) piperacillin/tazobactam, or (3) imipenem/cilastatin or meropenem. All three regimens have shown equal efficacy in large trials. All three are active against P. aeruginosa and a broad spectrum of aerobic gram-positive and gram-negative organisms. Imipenem/cilastatin has been associ-ated with an elevated rate of C. difficile diarrhea, and many centers reserve carbapenem antibiotics for treatment of gram-negative bacteria that produce extended-spectrum β-lactamases; these limi-tations make carbapenems less attractive as an initial regimen. Despite the frequent involvement of coagulase-negative staphy-lococci, the initial use of vancomycin or its automatic addition to the initial regimen has not resulted in improved outcomes, and the antibiotic does exert toxic effects. For these reasons, only judicious use of vancomycin is recommended—for example, when there is good reason to suspect the involvement of coagulase-negative staphylococci (e.g., the appearance of erythema at the exit site of a catheter or a positive culture for methicillin-resistant S. aureus or coagulase-negative staphylococci). Because the sensitivities of bac-teria vary from hospital to hospital, clinicians are advised to check their local sensitivities and to be aware that resistance patterns can change quickly, necessitating a change in approach to patients with fever and neutropenia. Similarly, infection control services should monitor for basic antibiotic resistance and for fungal infections. The appearance of a large number of Aspergillus infections, in particular, suggests the possibility of an environmental source that requires further investigation and remediation.
The initial antibacterial regimen should be refined on the basis of culture results (Fig. 104-2). Blood cultures are the most relevant basis for selection of therapy; surface cultures of skin and mucous membranes may be misleading. In the case of gram-positive bacteremia or another gram-positive infection, it is important that the antibiotic be optimal for the organism isolated. Once treatment with broad-spectrum antibiotics has begun, it is not desirable to discontinue all antibiotics because of the risk of failing to treat a potentially fatal bacterial infection; the addition of more and more
antibacterial agents to the regimen is not appropriate unless there is a clinical or microbiologic reason to do so. Planned progressive therapy (the serial, empirical addition of one drug after another without culture data) is not efficacious in most settings and may have unfortunate consequences. Simply adding another antibi-otic for fear that a gram-negative infection is present is a dubious practice. The synergy exhibited by β-lactams and aminoglycosides against certain gram-negative organisms (especially P. aeruginosa) provides the rationale for using two antibiotics in this setting, but recent analyses suggest that efficacy is not enhanced by the addi-tion of aminoglycosides, while toxicity may be increased. Mere “double coverage,” with the addition of a quinolone or another antibiotic that is not likely to exhibit synergy, has not been shown to be of benefit and may cause additional toxicities and side effects. Cephalosporins can cause bone marrow suppression, and vanco-mycin is associated with neutropenia in some healthy individuals. Furthermore, the addition of multiple cephalosporins may induce β-lactamase production by some organisms; cephalosporins and double β-lactam combinations should probably be avoided alto-gether in Enterobacter infections.
ANTIFUNGAL THERAPYFungal infections in cancer patients are most often associated with neutropenia. Neutropenic patients are predisposed to the devel-opment of invasive fungal infections, most commonly those due to Candida and Aspergillus species and occasionally those caused by Mucor, Rhizopus, Fusarium, Trichosporon, Bipolaris, and others. Cryptococcal infection, which is common among patients taking immunosuppressive agents, is uncommon among neutropenic patients receiving chemotherapy for AML. Invasive candidal disease is usually caused by C. albicans or C. tropicalis but can be caused by C. krusei, C. parapsilosis, and C. glabrata.
For decades, it has been common clinical practice to add ampho-tericin B to antibacterial regimens if a neutropenic patient remains febrile despite 4–7 days of treatment with antibacterial agents. The rationale for this empirical addition is that it is difficult to culture fungi before they cause disseminated disease and that mortal-ity rates from disseminated fungal infections in granulocytopenic patients are high. Before the introduction of newer azoles into clini-cal practice, amphotericin B was the mainstay of antifungal therapy. The insolubility of amphotericin B has resulted in the marketing of several lipid formulations that are less toxic than the amphotericin B deoxycholate complex. Echinocandins (e.g., caspofungin) are use-ful in the treatment of infections caused by azole-resistant Candida strains as well as in therapy for aspergillosis and have been shown to be equivalent to liposomal amphotericin B for the empirical treatment of patients with prolonged fever and neutropenia. Newer azoles have also been demonstrated to be effective in this setting. Although fluconazole is efficacious in the treatment of infections due to many Candida species, its use against serious fungal infections in immunocompromised patients is limited by its narrow spectrum: it has no activity against Aspergillus or against several non-albicans Candida species. The broad-spectrum azoles (e.g., voriconazole and posaconazole) provide another option for the treatment of Aspergillus infections (Chap. 241), including CNS infection. Clinicians should be aware that the spectrum of each azole is somewhat dif-ferent and that no drug can be assumed to be efficacious against all fungi. Aspergillus terreus is resistant to amphotericin B. Although voriconazole is active against Pseudallescheria boydii, amphoteri-cin B is not; however, voriconazole has no activity against Mucor. Posaconazole, which is administered orally, is useful as a prophylac-tic agent in patients with prolonged neutropenia. Studies in progress are assessing the use of these agents in combinations. For a full discussion of antifungal therapy, see Chap. 235.
ANTIVIRAL THERAPYThe availability of a variety of agents active against herpes-group viruses, including some new agents with a broader spectrum of activity, has heightened focus on the treatment of viral infections,
HPIM19_Part07(A)_p0467-p0619.indd 491 2/9/15 6:04 PM

COMMONLY USED ANTIBIOTIC REGIMENS FORTHETREATMENTOFFEBRILEPATIENTSINWHOMPROLONGEDNEUTROPENIA(>7DAYS)ISANTICIPATED
§ CeAazidimeorcefepime§ Piperacillin/tazobactam§ Imipenem/cilasta6normeropenem

PERSISTENT FEVER AFTER RESOLUTION OF NEUTROPENIA § Theriskofsuddendeathfromoverwhelmingbacteremiaisgreatly
reduced.§ Thefollowingdiagnosesshouldbeconsidered:
1. Fungalinfec6on2. Bacterialabscessesorundrainedfociofinfec6on3. Drugfever(includingreac6onstoan6microbialagentsaswellas
tochemotherapyorcytokines)4. Viraldiseasesorunusualpathogens5. GraA-versus-hostdisease

ANTIBIOTIC PROPHYLAXIS IN CANCER PATIENTS
§ Severalstudiesindicatethattheuseoforalfluoroquinolonespreventsinfec6onanddecreasesmortalityratesamongseverelyneutropenicpa6ents.
§ ProphylaxisforPneumocys5sismandatoryforpa6entswithacutelymphocy6cleukemiaandforallcancerpa6entsreceivingglucocor6coid-containingchemotherapyregimens.

VACCINATION OF CANCER PATIENTS
§ Pa6entsundergoingchemotherapyrespondlesswelltovaccinesthandonormalhosts.
§ Purifiedproteinsandinac6vatedvaccinesarealmostnevercontraindicatedandshouldbegiventopa6entsevenduringchemotherapy.
§ Themeningococcalandpneumococcalpolysaccharidevaccinesshouldbegiventopa6entsbeforesplenectomy.TheH.influenzaetypebconjugatevaccineshouldbeadministeredtoallsplenectomizedpa6ents.
§ Livevirus(orlivebacterial)vaccinesshouldnotbegiventopa6entsduringintensivechemotherapybecauseoftheriskofdisseminatedinfec6on.

THANK YOU!

















