37
Infections in Pregnancy Sudha Jasmine Rajan Medicine 3 Medicine CME 2016 1
| Date post: | 21-Apr-2018 |
| Category: |
Documents |
| Upload: | hoangtuyen |
| View: | 220 times |
| Download: | 4 times |

Infections in Pregnancy Sudha Jasmine Rajan
Medicine 3
Medicine CME 2016
1
Outline
Implications of infections on maternal and fetal outcome
Spectrum of infections in pregnancy and why
Recognizing sepsis in pregnancy
Management of specific acute fevers in pregnancy
Medicine CME 2016
2
ldquoYou can tell the condition of a Nation by looking at
the status of its womenrdquo Jawahar Lal Nehru
134 Billion population
asymp 26 million births year
Mean age at birth of 1st child 199years
Median age at first birth among women
25-29 (200506 est)
MMR174 deaths100000 live births (2015
est)
asymp 45335 deaths of young mothers year
children are 10 times more likely to die
within two years of their mothersrsquo death Medicine CME 2016
3
Maternal mortality data
January 2003 and December 2012
98139 deliveries
212 maternal deaths
Mean age2398plusmn415 y
13rd infections
11 pregnancy related infection Vs Pregnancy unrelated infection
J Turk Ger Gynecol Assoc 2015 Nov 216(4)208-13 doi
105152jtgga20150134 eCollection 2015
Changing perspectives of infectious causes of maternal mortality Halder A1 Vijayselvi R2 Jose R2
Medicine CME 2016
4
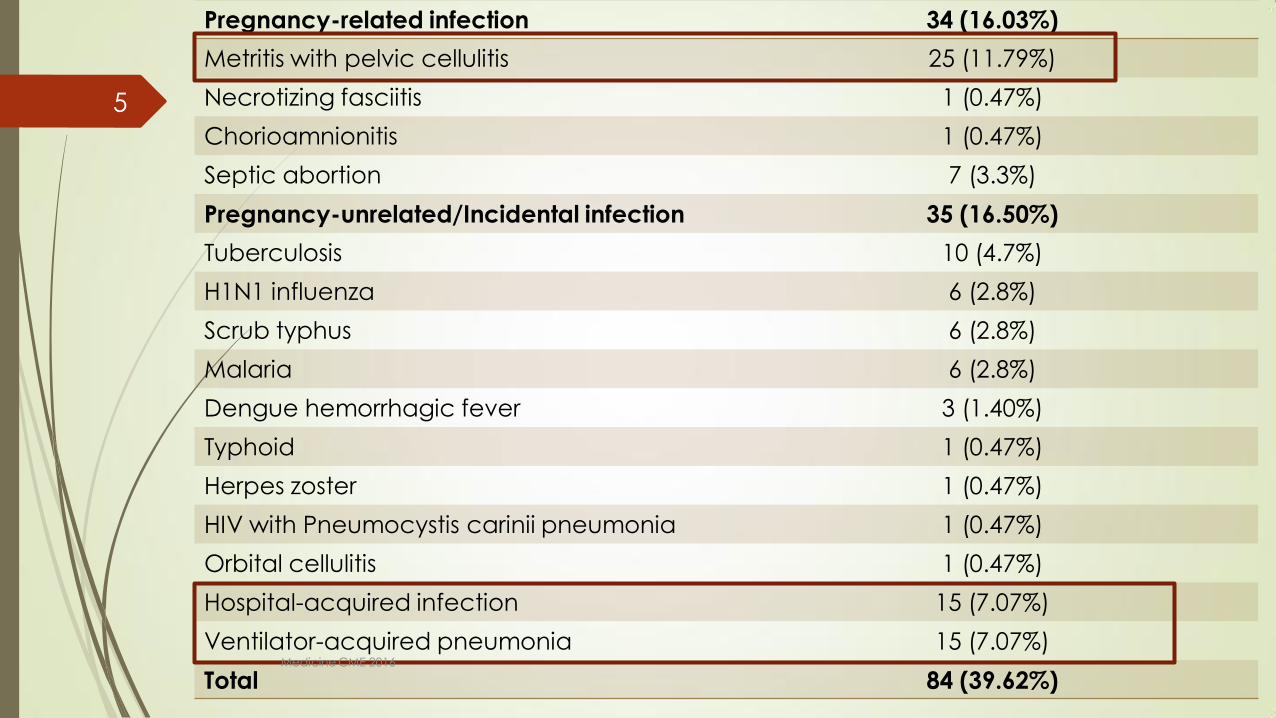
Pregnancy-related infection 34 (1603)
Metritis with pelvic cellulitis 25 (1179)
Necrotizing fasciitis 1 (047)
Chorioamnionitis 1 (047)
Septic abortion 7 (33)
Pregnancy-unrelatedIncidental infection 35 (1650)
Tuberculosis 10 (47)
H1N1 influenza 6 (28)
Scrub typhus 6 (28)
Malaria 6 (28)
Dengue hemorrhagic fever 3 (140)
Typhoid 1 (047)
Herpes zoster 1 (047)
HIV with Pneumocystis carinii pneumonia 1 (047)
Orbital cellulitis 1 (047)
Hospital-acquired infection 15 (707)
Ventilator-acquired pneumonia 15 (707)
Total 84 (3962) Medicine CME 2016
5
Forest plot of case-control studies considering maternal fever and risk of neural tube defects in
the offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Effect of maternal fever on fetal outcome
Neural tube defect
Medicine CME 2016
6
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Outline
Implications of infections on maternal and fetal outcome
Spectrum of infections in pregnancy and why
Recognizing sepsis in pregnancy
Management of specific acute fevers in pregnancy
Medicine CME 2016
2
ldquoYou can tell the condition of a Nation by looking at
the status of its womenrdquo Jawahar Lal Nehru
134 Billion population
asymp 26 million births year
Mean age at birth of 1st child 199years
Median age at first birth among women
25-29 (200506 est)
MMR174 deaths100000 live births (2015
est)
asymp 45335 deaths of young mothers year
children are 10 times more likely to die
within two years of their mothersrsquo death Medicine CME 2016
3
Maternal mortality data
January 2003 and December 2012
98139 deliveries
212 maternal deaths
Mean age2398plusmn415 y
13rd infections
11 pregnancy related infection Vs Pregnancy unrelated infection
J Turk Ger Gynecol Assoc 2015 Nov 216(4)208-13 doi
105152jtgga20150134 eCollection 2015
Changing perspectives of infectious causes of maternal mortality Halder A1 Vijayselvi R2 Jose R2
Medicine CME 2016
4
Pregnancy-related infection 34 (1603)
Metritis with pelvic cellulitis 25 (1179)
Necrotizing fasciitis 1 (047)
Chorioamnionitis 1 (047)
Septic abortion 7 (33)
Pregnancy-unrelatedIncidental infection 35 (1650)
Tuberculosis 10 (47)
H1N1 influenza 6 (28)
Scrub typhus 6 (28)
Malaria 6 (28)
Dengue hemorrhagic fever 3 (140)
Typhoid 1 (047)
Herpes zoster 1 (047)
HIV with Pneumocystis carinii pneumonia 1 (047)
Orbital cellulitis 1 (047)
Hospital-acquired infection 15 (707)
Ventilator-acquired pneumonia 15 (707)
Total 84 (3962) Medicine CME 2016
5
Forest plot of case-control studies considering maternal fever and risk of neural tube defects in
the offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Effect of maternal fever on fetal outcome
Neural tube defect
Medicine CME 2016
6
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
ldquoYou can tell the condition of a Nation by looking at
the status of its womenrdquo Jawahar Lal Nehru
134 Billion population
asymp 26 million births year
Mean age at birth of 1st child 199years
Median age at first birth among women
25-29 (200506 est)
MMR174 deaths100000 live births (2015
est)
asymp 45335 deaths of young mothers year
children are 10 times more likely to die
within two years of their mothersrsquo death Medicine CME 2016
3
Maternal mortality data
January 2003 and December 2012
98139 deliveries
212 maternal deaths
Mean age2398plusmn415 y
13rd infections
11 pregnancy related infection Vs Pregnancy unrelated infection
J Turk Ger Gynecol Assoc 2015 Nov 216(4)208-13 doi
105152jtgga20150134 eCollection 2015
Changing perspectives of infectious causes of maternal mortality Halder A1 Vijayselvi R2 Jose R2
Medicine CME 2016
4
Pregnancy-related infection 34 (1603)
Metritis with pelvic cellulitis 25 (1179)
Necrotizing fasciitis 1 (047)
Chorioamnionitis 1 (047)
Septic abortion 7 (33)
Pregnancy-unrelatedIncidental infection 35 (1650)
Tuberculosis 10 (47)
H1N1 influenza 6 (28)
Scrub typhus 6 (28)
Malaria 6 (28)
Dengue hemorrhagic fever 3 (140)
Typhoid 1 (047)
Herpes zoster 1 (047)
HIV with Pneumocystis carinii pneumonia 1 (047)
Orbital cellulitis 1 (047)
Hospital-acquired infection 15 (707)
Ventilator-acquired pneumonia 15 (707)
Total 84 (3962) Medicine CME 2016
5
Forest plot of case-control studies considering maternal fever and risk of neural tube defects in
the offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Effect of maternal fever on fetal outcome
Neural tube defect
Medicine CME 2016
6
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Maternal mortality data
January 2003 and December 2012
98139 deliveries
212 maternal deaths
Mean age2398plusmn415 y
13rd infections
11 pregnancy related infection Vs Pregnancy unrelated infection
J Turk Ger Gynecol Assoc 2015 Nov 216(4)208-13 doi
105152jtgga20150134 eCollection 2015
Changing perspectives of infectious causes of maternal mortality Halder A1 Vijayselvi R2 Jose R2
Medicine CME 2016
4
Pregnancy-related infection 34 (1603)
Metritis with pelvic cellulitis 25 (1179)
Necrotizing fasciitis 1 (047)
Chorioamnionitis 1 (047)
Septic abortion 7 (33)
Pregnancy-unrelatedIncidental infection 35 (1650)
Tuberculosis 10 (47)
H1N1 influenza 6 (28)
Scrub typhus 6 (28)
Malaria 6 (28)
Dengue hemorrhagic fever 3 (140)
Typhoid 1 (047)
Herpes zoster 1 (047)
HIV with Pneumocystis carinii pneumonia 1 (047)
Orbital cellulitis 1 (047)
Hospital-acquired infection 15 (707)
Ventilator-acquired pneumonia 15 (707)
Total 84 (3962) Medicine CME 2016
5
Forest plot of case-control studies considering maternal fever and risk of neural tube defects in
the offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Effect of maternal fever on fetal outcome
Neural tube defect
Medicine CME 2016
6
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Pregnancy-related infection 34 (1603)
Metritis with pelvic cellulitis 25 (1179)
Necrotizing fasciitis 1 (047)
Chorioamnionitis 1 (047)
Septic abortion 7 (33)
Pregnancy-unrelatedIncidental infection 35 (1650)
Tuberculosis 10 (47)
H1N1 influenza 6 (28)
Scrub typhus 6 (28)
Malaria 6 (28)
Dengue hemorrhagic fever 3 (140)
Typhoid 1 (047)
Herpes zoster 1 (047)
HIV with Pneumocystis carinii pneumonia 1 (047)
Orbital cellulitis 1 (047)
Hospital-acquired infection 15 (707)
Ventilator-acquired pneumonia 15 (707)
Total 84 (3962) Medicine CME 2016
5
Forest plot of case-control studies considering maternal fever and risk of neural tube defects in
the offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Effect of maternal fever on fetal outcome
Neural tube defect
Medicine CME 2016
6
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
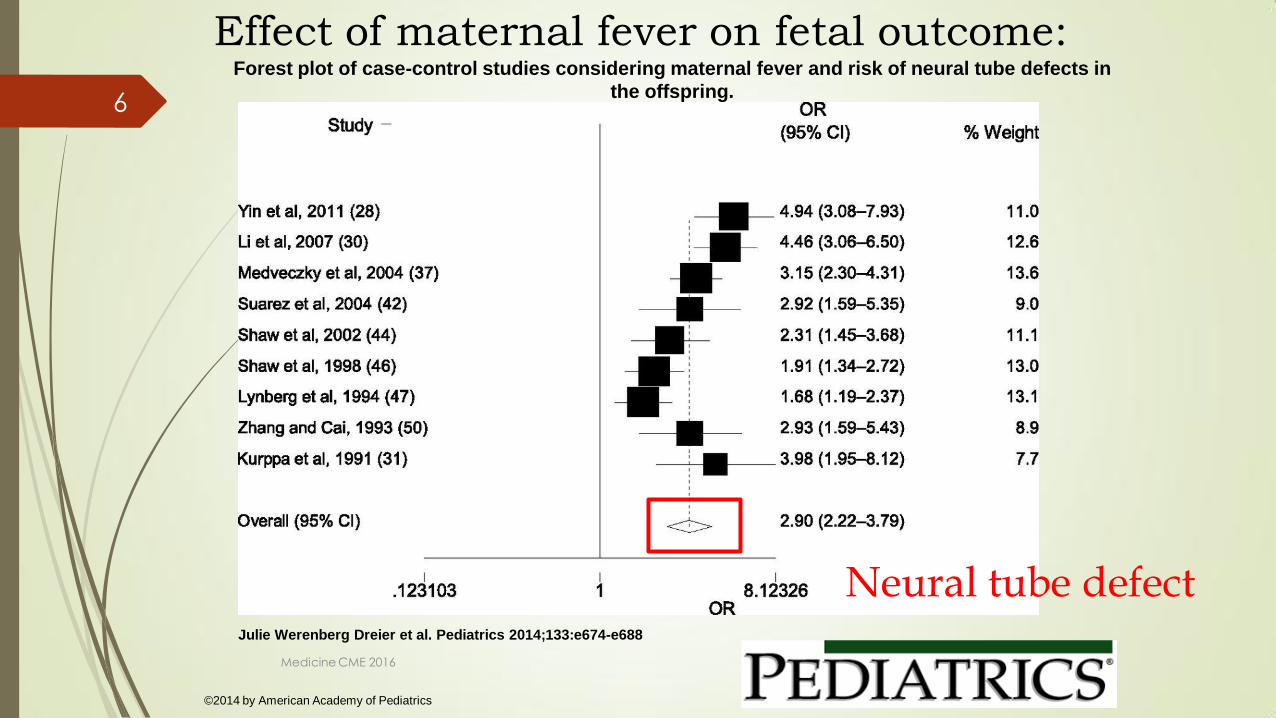
Forest plot of case-control studies considering maternal fever and risk of neural tube defects in
the offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Effect of maternal fever on fetal outcome
Neural tube defect
Medicine CME 2016
6
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
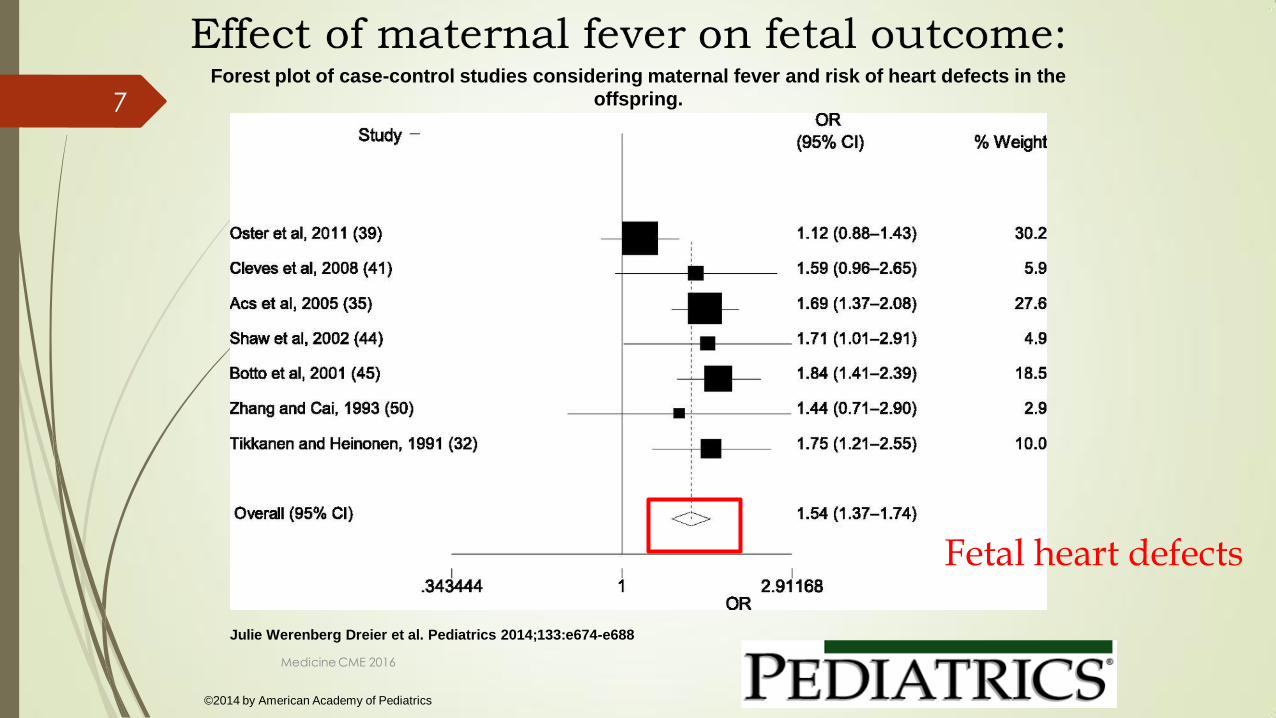
Forest plot of case-control studies considering maternal fever and risk of heart defects in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Fetal heart defects
Medicine CME 2016
7
Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Forest plot of case-control studies considering maternal fever and risk of oral clefts in the
offspring
Julie Werenberg Dreier et al Pediatrics 2014133e674-e688
copy2014 by American Academy of Pediatrics
Oral clefts
Effect of maternal fever on fetal outcome
Medicine CME 2016
8
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Effect of intrapartum fever on fetal outcome
intrapartum fever was a strong predictor of infection-related death
early neonatal death (OR 129 95 CI 101 164)
Intrapartum fever is an important predictor of neonatal morbidity and infection-related mortality
meconium aspiration syndrome
hyaline membrane disease
neonatal seizures
assisted ventilation
Obstet Gynecol 2001 Jul98(1)20-7
Association of maternal fever during labor with neonatal and infant morbidity and
mortality Petrova A1 Demissie K Rhoads GG Smulian JC Marcella S Ananth CV
Medicine CME 2016
9
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
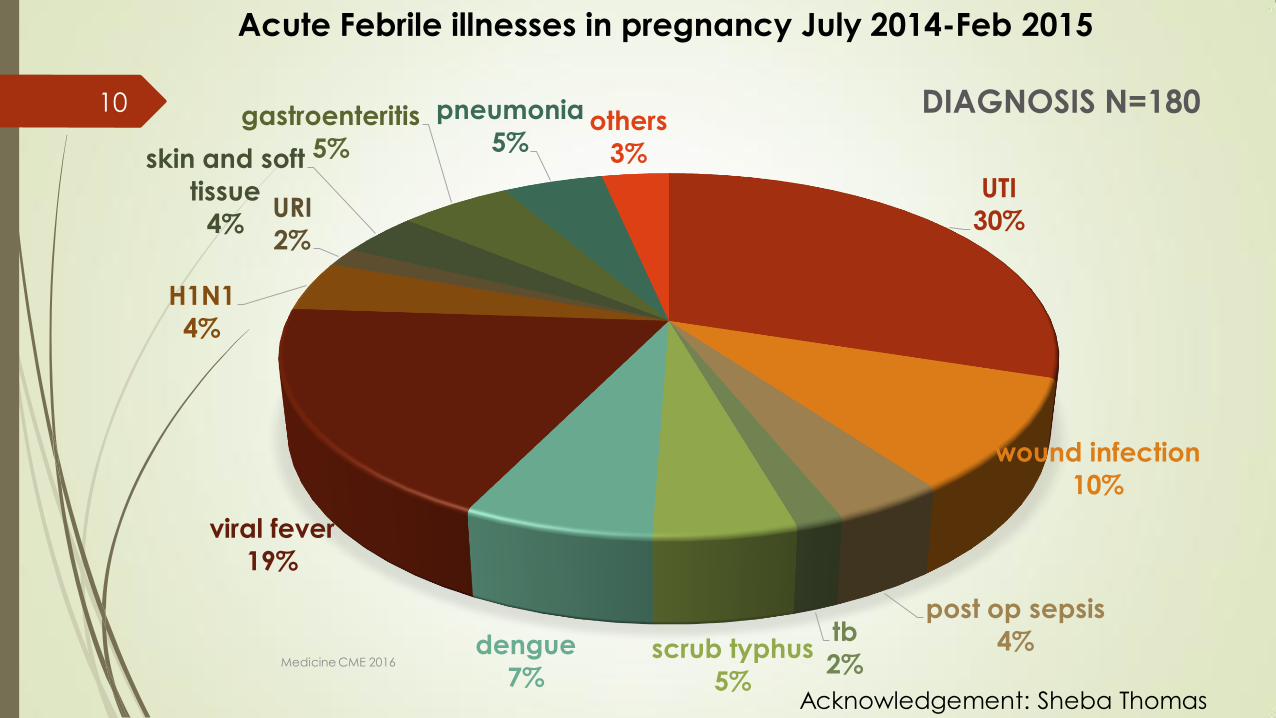
UTI
30
wound infection
10
post op sepsis
4 tb
2 scrub typhus
5
dengue
7
viral fever
19
H1N1
4
URI
2
skin and soft
tissue
4
gastroenteritis
5
pneumonia
5 others
3
DIAGNOSIS N=180
Acute Febrile illnesses in pregnancy July 2014-Feb 2015
Acknowledgement Sheba Thomas
Medicine CME 2016
10
Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Medicine CME 2016
11
0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

0
5
10
15
20
25
30
35
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
oth
ers
Fetal outcome
alive dead not known
0
10
20
30
40
50
60
UTI
wo
un
d in
fec
tio
n
ga
stro
en
teritis
pn
eu
mo
nia
scru
b t
yp
hu
s
de
ng
ue
vira
l fe
ve
r
tb
skin
an
d s
oft
hellip
po
st o
p hellip
H1
N1
UR
I
ch
orio
am
nio
nitis
oth
ers
Maternal outcome
alive dead and DAMA
Acknowledgement Sheba Thomas
Medicine CME 2016
12
Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Pregnancy asso plusmn
related surgical
procedures
Unrelated to pregnancy
uarr frequency in
pregnancy
Incidental infections
during pregnancy
Hospital-acquired
infections
Infection of LSCS wound
Episiotomy infection
Mastitis
Chorioamnionitis
Postpartum endometritis
Septic abortion
Septic thrombophlebitis
Puerperal sepsis
Necrotizing fasciitis
Pelvic abscess
Infected cerclage
Amniocentesis
Lower UTI
Pyelonephritis
Malaria
Listeriosis
Viral hepatitis (E)
Varicella pneumonia
Coccidioidomycosis
Aspiration pneumonia
Community-acquired
pneumonia
Vector borne Scrub typhus Dengue
Gastrointestinal
infections
HIV-related infections Toxoplasmosis Cytomegalovirus
Catheter-related UTI
Thrombophlebitis
Wound infection
Pneumonia nosocomial
Ventilator-associated
pneumonia
Central line-associated
infection
Spectrum of infections in the obstetric patient
Medicine CME 2016
13
Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Immunity during pregnancy
Cytokines
Complement
cascade NK cells Macrophages
Monocytes
Eosinophils
Neutrophils
PRRs Extracellular
antigens
bacteria virus
Intracellular antigens cells
infected with viruses rickettsia
mycoplasma
+ +
Acquired immunity
Pathogenantigen
Immediate effect
Result
Soluble antigen activated B cell Cell killing by CTLs
Humoral immunity Cell mediated immunity
B cell TH2 CTL TH1
Medicine CME 2016
14
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
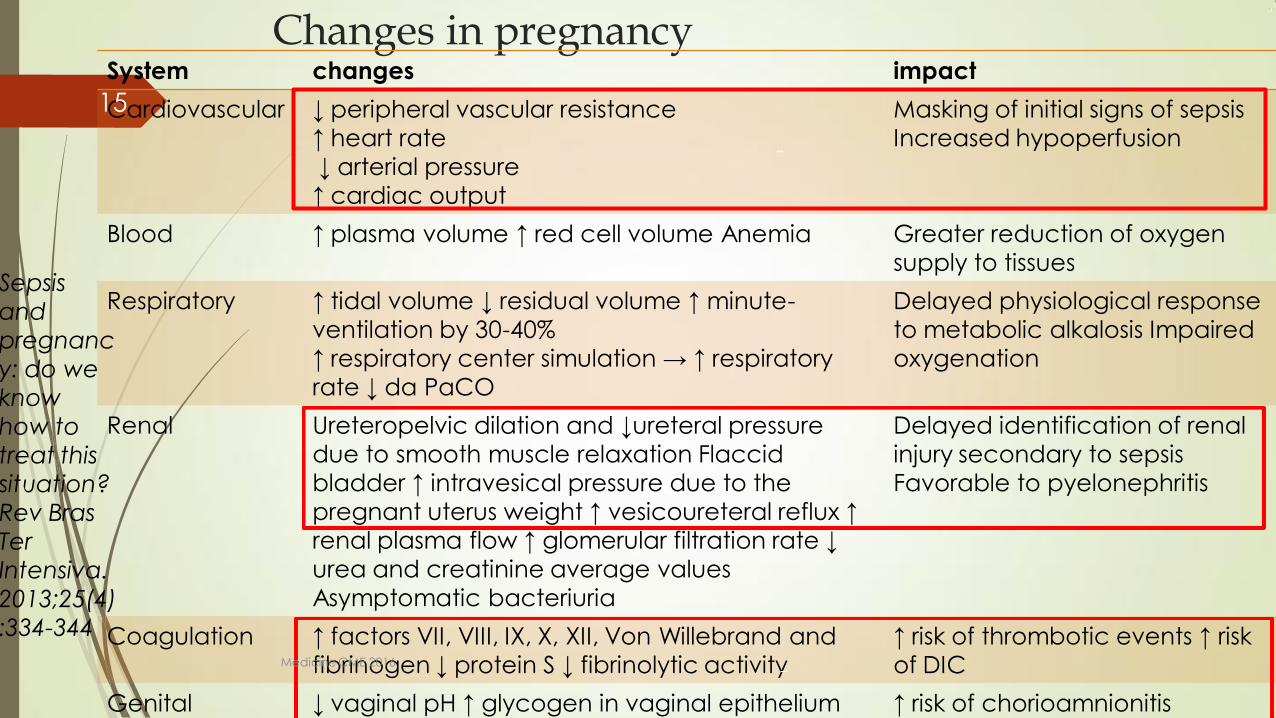
Changes in pregnancy System changes impact
Cardiovascular darr peripheral vascular resistance
uarr heart rate
darr arterial pressure
uarr cardiac output
Masking of initial signs of sepsis
Increased hypoperfusion
Blood uarr plasma volume uarr red cell volume Anemia Greater reduction of oxygen
supply to tissues
Respiratory uarr tidal volume darr residual volume uarr minute-
ventilation by 30-40
uarr respiratory center simulation rarr uarr respiratory
rate darr da PaCO
Delayed physiological response
to metabolic alkalosis Impaired
oxygenation
Renal Ureteropelvic dilation and darrureteral pressure
due to smooth muscle relaxation Flaccid
bladder uarr intravesical pressure due to the
pregnant uterus weight uarr vesicoureteral reflux uarr
renal plasma flow uarr glomerular filtration rate darr
urea and creatinine average values
Asymptomatic bacteriuria
Delayed identification of renal
injury secondary to sepsis
Favorable to pyelonephritis
Coagulation uarr factors VII VIII IX X XII Von Willebrand and
fibrinogen darr protein S darr fibrinolytic activity
uarr risk of thrombotic events uarr risk
of DIC
Genital darr vaginal pH uarr glycogen in vaginal epithelium uarr risk of chorioamnionitis
Sepsis
and
pregnanc
y do we
know
how to
treat this
situation
Rev Bras
Ter
Intensiva
201325(4)
334-344
-
Medicine CME 2016
15
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
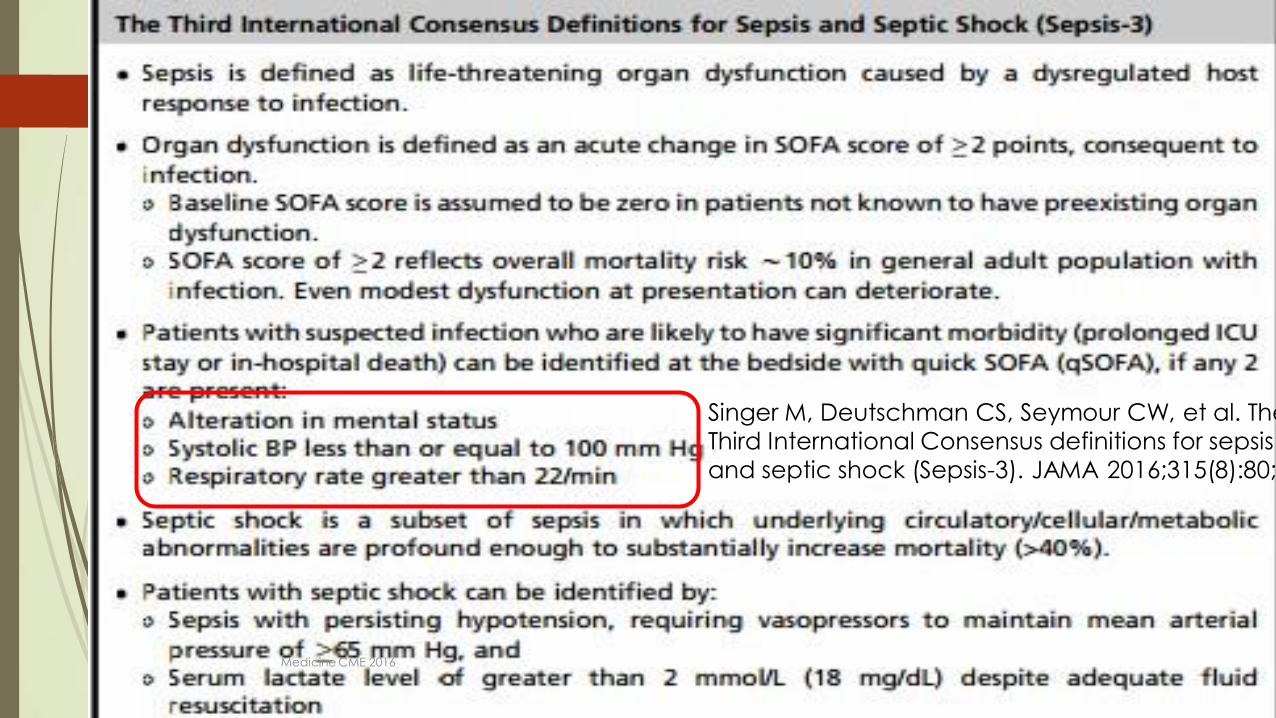
Singer M Deutschman CS Seymour CW et al The
Third International Consensus definitions for sepsis
and septic shock (Sepsis-3) JAMA 2016315(8)80
Medicine CME 2016
16
Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Caveats with pregnant women
Pregnant women are young Reach the limits of physiological compensation before they collapse
Count heart rate and respiratory rate
Normals are different
Fever may not always be present and are not necessarily related to the severity of sepsis
BP Measure lactates UO Fetal heart rate
Gravid uterus ventilation CVP
Tests urine RE SPC cultures postpartum
Antibiotics greater distribution volume altered absorption excretion and reduced drug levels
Medicine CME 2016
17
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
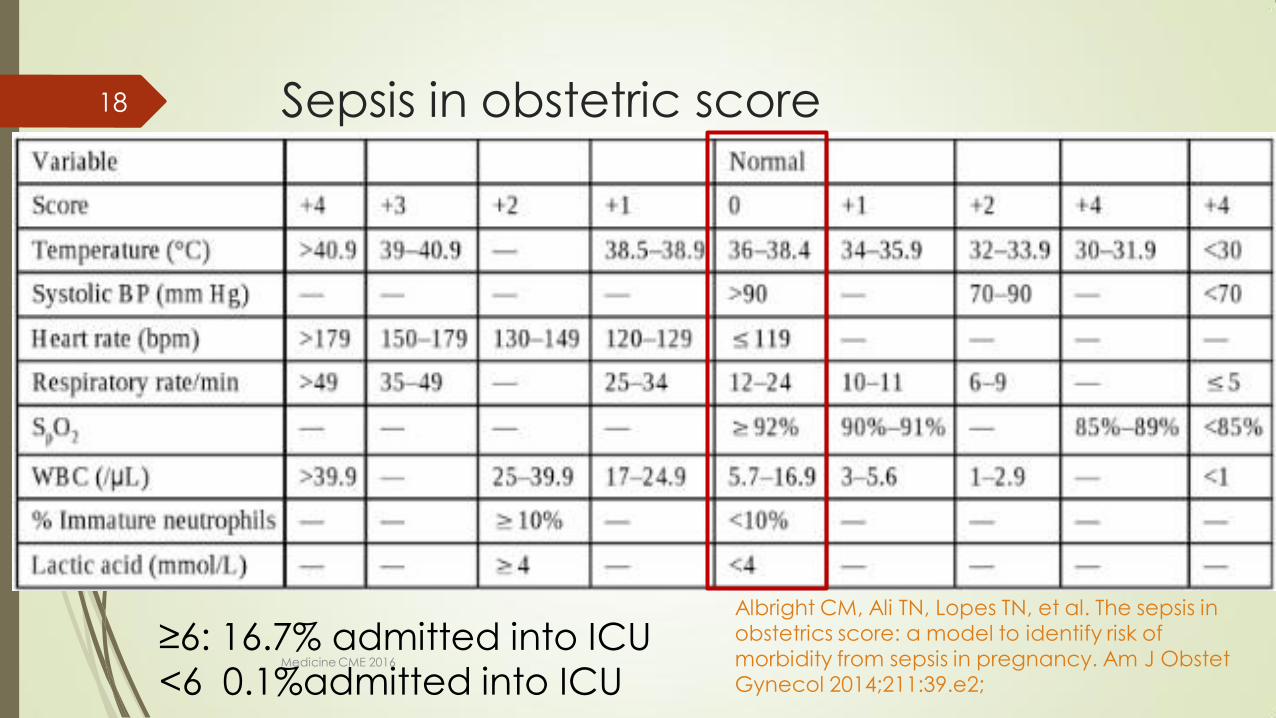
Sepsis in obstetric score
ge6 167 admitted into ICU lt6 01admitted into ICU
Albright CM Ali TN Lopes TN et al The sepsis in obstetrics score a model to identify risk of morbidity from sepsis in pregnancy Am J Obstet Gynecol 201421139e2
Medicine CME 2016
18
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Overall goals
Treat the mother Resuscitating the mother will resuscitate
the fetus
Delivery attempts increase maternal and fetal mortality assuming the source is not intrauterine
Improve functional intravascular volume
Establish and maintain an adequate airway
Determine the septic foci
Empiric antibiotic therapy know the most common pathogens Medicine CME 2016
19
Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Tasks lt6hrs of the identification of severe sepsis
Complete History and Clinical examination
Obtain blood cultures prior to antibiotic administration
Administer broad-spectrum antibiotic within one hour of recognition of severe sepsis
Measure serum lactate
If hypotension plusmn a serum lactate gt4mmoll fetal heart rate
urine output(05mlkghr)
start initial minimum 20mlkg of crystalloid or an equivalent 1st hour
Apply vasopressors for hypotension that is not responding to
initial fluid resuscitation
to maintain mean arterial pressure (MAP) gt65mmHg Medicine CME 2016
20
Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Need for ICU transfers Cardiovascular Hypotension or raised serum lactate
persisting despite fluid resuscitation suggesting the need for inotrope support
Respiratory Pulmonary oedema Mechanical ventilation Airway protection
Renal Renal dialysis
Neurological Significantly decreased conscious level
Miscellaneous Multi-organ failure
Uncorrected acidosis Hypothermia
Medicine CME 2016
21
Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Risk factors for maternal sepsis by
confidential enquiry
Obesity
Impaired glucose tolerance Diabetes
Impaired immunity immunosuppressant medication
Anaemia
Vaginal discharge
History of pelvic infection
History of group B streptococcal
infection
Amniocentesis and other invasive
procedures
Cervical cerclage
Prolonged spontaneous rupture of
membranes
GAS infection in close contacts
family members
Of black or other minority ethnic
group origin Centre for Maternal and Child Enquiries (CMACE) Saving Motherrsquos Lives reviewing maternal deaths to make motherhood safer 2006-2008 BJOG 2011 118(suppl 1)1-203
Medicine CME 2016
22
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Gram-negative
Escherichia coli
Hemophilus influenzae
Klebisiellaspecies
Enterobacter species
Proteusspecies
Pseudomonas species
Serratiaspecies
Gram-positive
Pneumococcus
Streptococcus groups A B and D
Enterococus
Staphylococcus aureus
Listeria monocytogenes
Anaerobic
Bacteroides species
Clostridium perfringens
Fusobacterium species
Peptococcus
Peptostreptococcus Medicine CME 2016
23
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Choice of antibiotics
Lancefield group A beta-haemolytic Streptococcus
EColi
Mixed infections Gram-positive and Gram-negative
chorioamnionitis endometritis
Coliform infection urinary sepsis preterm premature
rupture of membranes and cerclage
Anaerobes Peptostreptococcus and Bacteroides spp
Medicine CME 2016
24
Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Medicine CME 2016
25
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
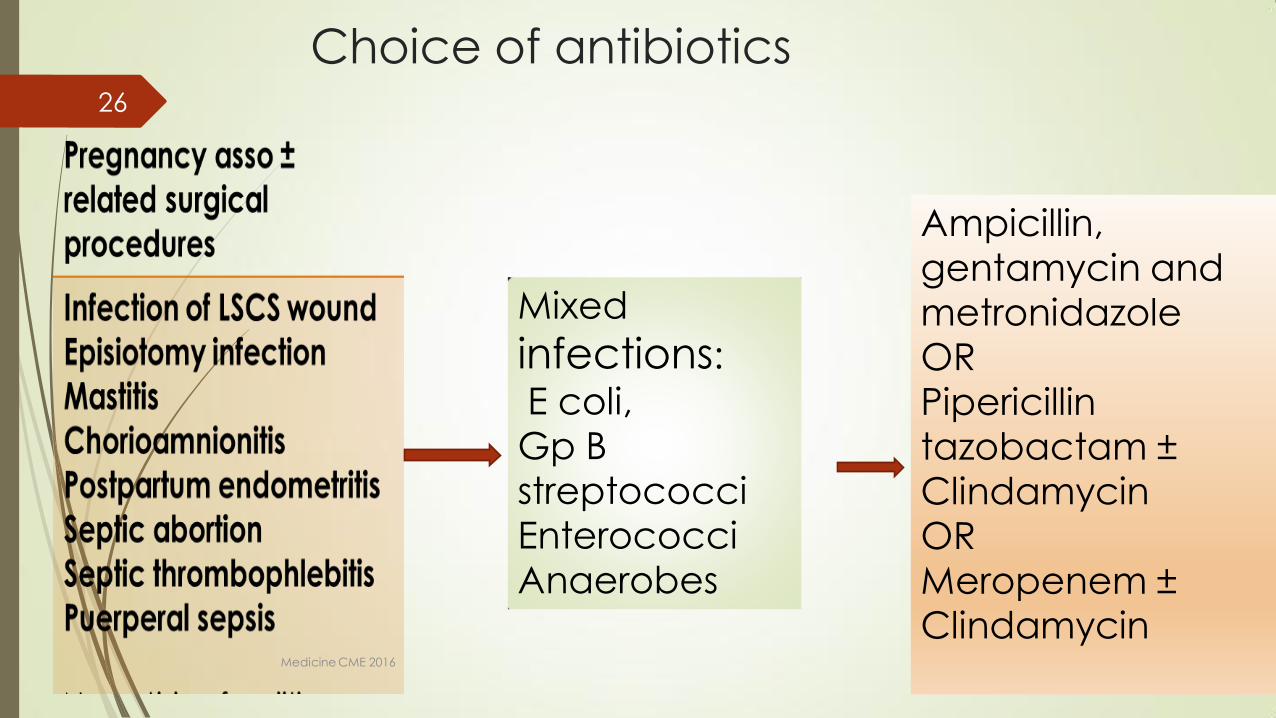
Choice of antibiotics
Mixed
infections
E coli Gp B streptococci Enterococci Anaerobes
Ampicillin
gentamycin and metronidazole OR
Pipericillin tazobactam plusmn Clindamycin OR Meropenem plusmn Clindamycin Medicine CME 2016
26
Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Choice of antibiotics
E Coli(70 Klebsiella and Enterobacter species (3 ) Proteus (2 )
gram-positive organisms including group B
Streptococcus (10 )
Meropenem
1 g IV Q8H
Medicine CME 2016
27
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
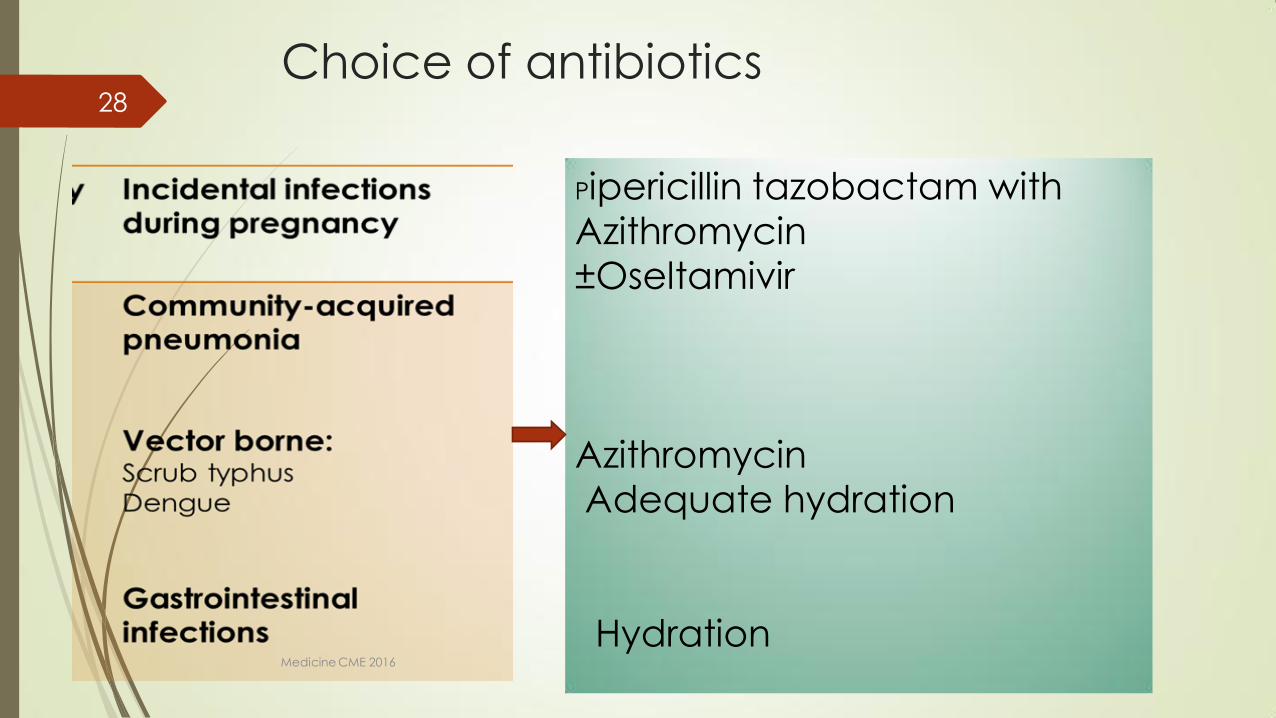
Choice of antibiotics
Pipericillin tazobactam with Azithromycin plusmnOseltamivir
Azithromycin
Adequate hydration Hydration
Medicine CME 2016
28
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
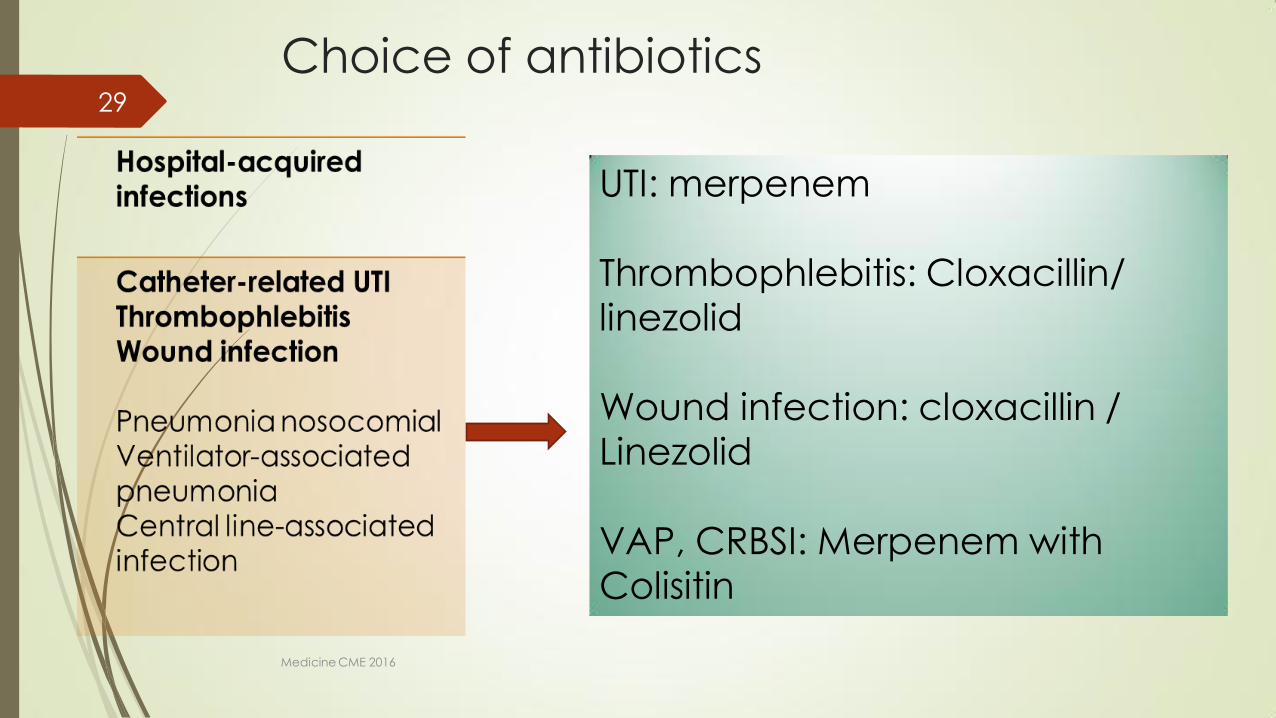
Choice of antibiotics
UTI merpenem Thrombophlebitis Cloxacillin linezolid
Wound infection cloxacillin Linezolid
VAP CRBSI Merpenem with Colisitin
Medicine CME 2016
29
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
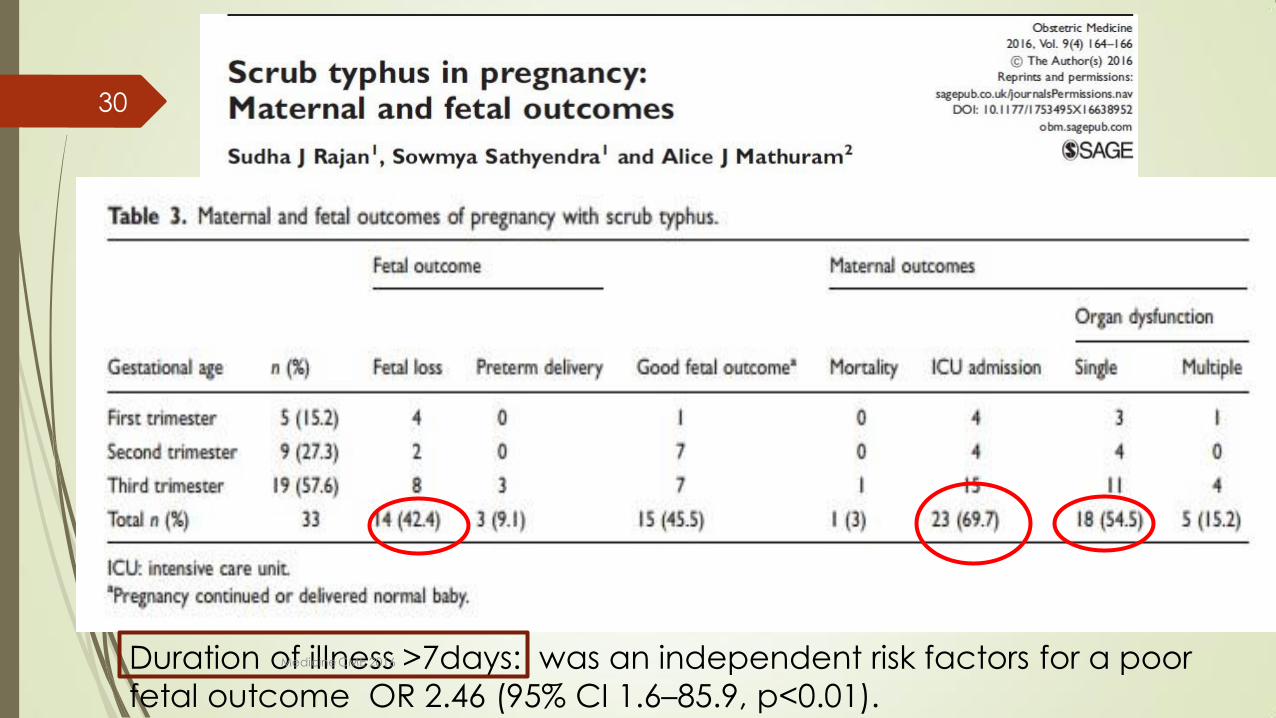
Scrub typhus in pregnancy
Duration of illness gt7days was an independent risk factors for a poor
fetal outcome OR 246 (95 CI 16ndash859 plt001)
Medicine CME 2016
30
Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Dengue in pregnancy
Maternal outcome
high rates of cesarean deliveries
(440)
pre-eclampsia (120)
50 DHF
30 DSS
30 mortality
Fetal outcome
preterm birth (161)
low birth weight
Vertical transmission was
described in 640 case reports
and (126) case series
25 fetal loss
375NICU admission
19 case reports 9 case series and 2 comparison studies
Obstet Gynecol Surv 2010 Feb65(2)107-18 doi 101097OGX0b013e3181cb8fbc
Maternal dengue and pregnancy outcomes a systematic review
Pouliot SH1 Xiong X Harville E Paz-Soldan V Tomashek KM Breart G Buekens P
Infect Dis Obstet Gynecol 201620165046091 doi 10115520165046091 Epub 2016 Mar 16
Spectrum of Maternofetal Outcomes during Dengue Infection in Pregnancy An Insight
Sharma S1 Jain S1 Rajaram S1
Medicine CME 2016
31
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
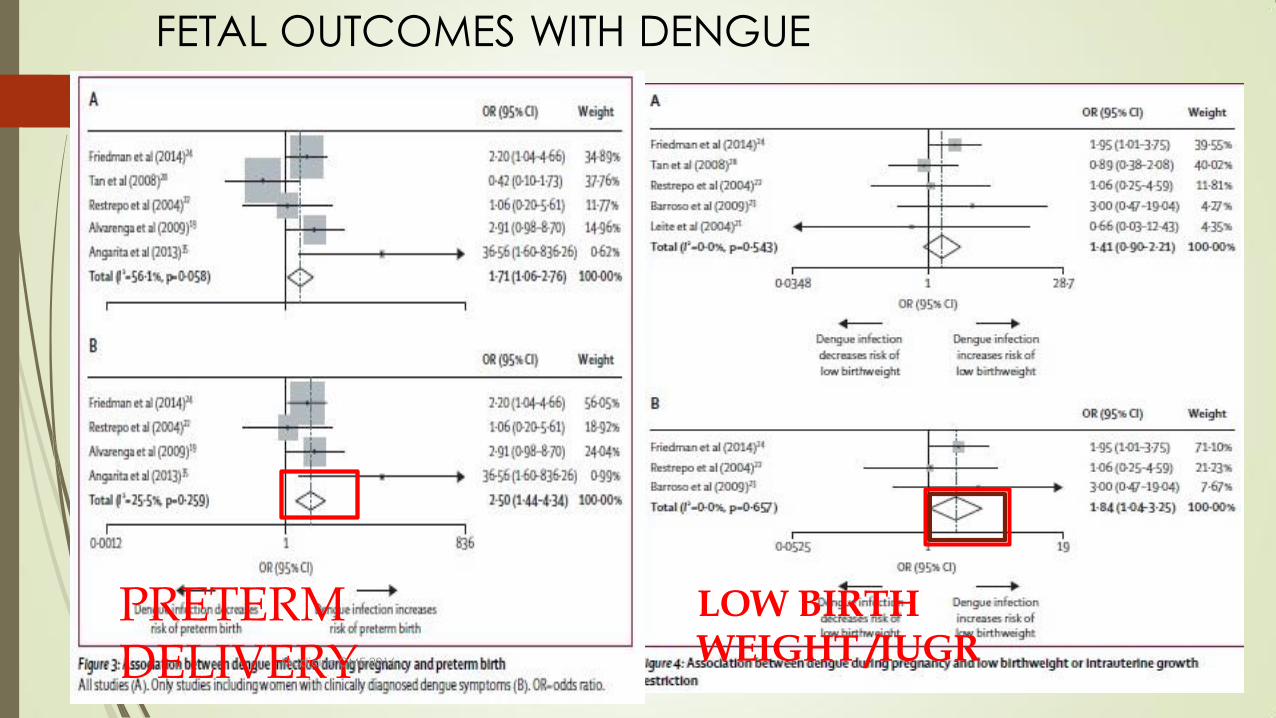
PRETERM DELIVERY
LOW BIRTH WEIGHT IUGR
FETAL OUTCOMES WITH DENGUE
Medicine CME 2016
32
FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

FETAL OUTCOMES WITH DENGUE
Miscarriage
Dengue during pregnancy and adverse fetal outcomes
a systematic review and meta-analysis Enny S Paixatildeo Maria Gloria Teixeira Maria da Conceiccedilatildeo N Costa Laura C Rodrigues
wwwthelancetcominfection Published online March 3 2016
httpdxdoiorg101016S1473-3099(16)00088-8
Medicine CME 2016
33
UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

UTI in pregnancy the most common severe medical complication of pregnancy
Asymptomatic bacteruria 2-7 and 13rd would develop UTI
asymptomatic bacteriuria at the first prenatal visit (12-16 weeks) (ACOGamp US preventive task force)
lower the incidence of pyelonephritis (OR 023 95 CI 013-041)
Risk factors
history of UTI
presence of urinary tract anomalies
diabetes mellitus
hemoglobin S
preterm labor
Medicine CME 2016
34
Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Take home message
The pregnant woman is a different host
Impact of maternal mortality
Medicine CME 2016
35
Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

Acknowledgements
Colleagues in Department of Obstetrics
Sowmya Satyendra and friends in Medicine 3
Patients in OG OMC and students
Teachers and mentors
Lord Jesus Christ
Thank you
Medicine CME 2016
36
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore
Copyright of this educational material rests with the author and
Christian Medical College Vellore Duplication revision and
redistribution are not permitted For any further clarification please
contact the concerned author
copy reserved to author and Christian Medical College Vellore

















