71
Infections in the Elderly Jérôme Fennell, Jérôme Fennell, MB, MSc, MB, MSc, PhD, FRCPath PhD, FRCPath [email protected] [email protected]
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | annice-douglas |
| View: | 216 times |
| Download: | 0 times |

Infections in the Elderly
Jérôme Fennell, Jérôme Fennell, MB, MSc, PhD, FRCPathMB, MSc, PhD, FRCPath
[email protected]@amnch.ie

Infections in Old AgeInfections in Old Age
• Risk Factors of Old Age• Common Infections of Old Age
– RTI: Pneumonia, Influenza, TB– Skin and Soft tissue infections
• Shingles• Leg Ulcers
– GIT: C. Difficile– UTI: ESBLs
• Renal function and aminoglycoside and glycopeptide dosing

Risk factors for Infections in the Risk factors for Infections in the ElderlyElderly
Older, weaker, more at risk
• More comorbidities• Gradual deterioration of immune system with
age• May be malnourished, poor accommodation• More likely to harbour resistant organisms as
more likely to have been – Hospitalised– in nursing home– Exposed to multiple antibiotics

Cellular Immunity in the ElderlyCellular Immunity in the Elderly
• Altered T cell phenotype naïve T cells; memory T cells
Reduced T cell responses response to TCR stimulation T cell proliferation expression of IL2-R IL2 production
Ginaldi et al 1999

Case History: December 1999Case History: December 1999
• 67 yr old woman
• PC: cough, left sided chest pain, rigors x 24h
• HPC: productive cough most mornings, but increasingly purulent recently
• PMHx: MI 2 yrs ago, smoked 40/day until then

On Examination:On Examination:
• T: 40oC
• Pulse: 130/min, BP: 145/90
• Tachypnoea
• PMHx: MI 2 yrs ago
smoked 40/day until then
• Resp exam suggestive of consolidation
TestsTests
• FBC, WCC
• Sputum for microscopy and culture
• Blood culture
• CXR
• ABG
• WCC – 22, 90% neutrophils
• Sputum – pus cells, gram positive diplococci
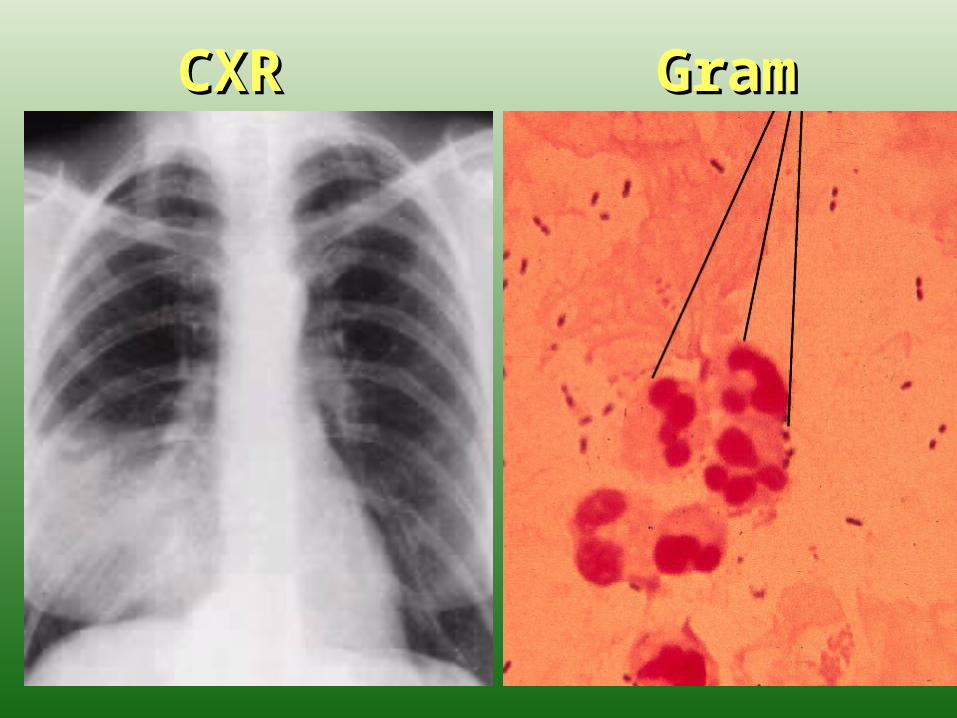
CXRCXR GramGram

Sputum resultSputum resultSputum – pus cells, gram positive
diplococci…What does this tell us?
More than you think –
• No epithelial cells - suggests this is a good specimen from lower RT so should provide a good result on culture
• Gram positive diplococci likely to be?

Sputum Gram Stain Sputum Gram Stain
• No longer done routinely• Not sensitive or specific enough• Not recommended in IDSA CAP guidelines
• Guidelines now recommend another test instead...

Urinary Antigen TestingUrinary Antigen Testing
• All severe pneumonias should have urine test for – Legionella Urinary Antigen– Pneumococcal Urinary Antigen
• Should also think of CXR, pulse oximetry, ABG,

TreatmentTreatmentPneumococcus
BenzylPen unless allergic or live in area of resistance (Irish rate of resistance-?)
When cause unknown, use augmentin or cefotaxime to cover Haemophilus

later…later…IV BenPenTransferred to ICU for ventilation because of
hypoxiaBCs – positive for S pneumoniae x2WCC – 35CXR – shows increasing consolidation and
pleural effusion24 hrs later – Cardiac arrest – RIPNext day S pneumoniae sensitivity available: R- PenicillinS – Erythromycin, Ceftriaxone

RTI in ElderlyRTI in Elderly
• Strep. Pneumoniae
• Influenza Virus
• Recurrence of TB
• Normal causes of RTI

PneumococcusPneumococcus
• Common cause of community acquired pneumonia• Risk increased by smoking• Often occurs as secondary pneumonia after influenza
infection• More common during winter months• Can also cause ENT, bacteremia and CNS infections• Latest EARSS Resistance Rates for Ireland:
– Pen Non Susceptible 16.2%– Erythromycin Resistant 14.1%– Ceftriaxone/Cefotaxime Resistance Rare
Pneumonia SymptomsPneumonia Symptoms
• Fever (less common in those >75)• Cough with coloured sputum• Pleuritic chest pain, dyspnea• Altered mental function, particularly in the
elderly• Increased or decreased WBC

Strep pneumoniaeStrep pneumoniae
• RTI: Amoxicillin/Clarithromycin if sensitive • If infection severe or previous antibiotic
exposure, use IV Ceftriaxone or Cefotaxime• Augmentin has no added benefit because
resistance is not due to B-lactamase production but do to different Pen binding proteins
• In countries where Ceftriaxone resistance occurs in significant numbers use IV Ceftriaxone and IV Vancomycin empirically

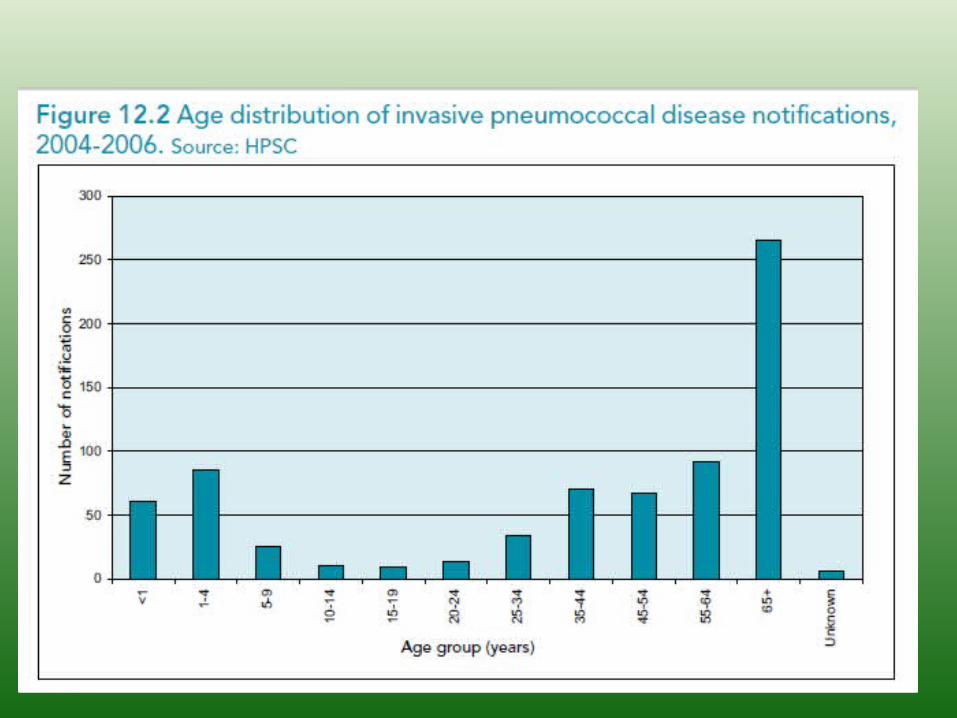
Pneumococcal PneumoniaPneumococcal Pneumonia• Elderly patients often have fewer or less
severe symptoms than younger patients
• Many community-acquired pneumonias are perfectly treatable as outpatients by oral antibiotics
• >90 polysaccharide capsular types
• HPSC Guidelines:
Pneumococcal VaccinesPneumococcal Vaccines2 types of pneumococcal vaccine:
1. Polysaccharide Pneumococcal Vaccine (PPV23)– incorporates 23 of the most common capsular types which together
account for up to 90% of serious pneumococcal infections– Only suitable for use in those ≥ 2 years of age
2. A conjugate 7 valent vaccine (PCV7) containing polysaccharide antigens from the 7 most common serotypes conjugated to a protein (CRM 197) has enhanced immunogenicity compared with the polysaccharide vaccine. – immunogenic even in infancy– active against approximately 70% of isolates causing invasive
disease, and against a significant number of penicillin-resistant strains.

HPSC Groups Requiring VaccinationHPSC Groups Requiring VaccinationAt risk categories:• Asplenia or reduced splenic dysfunction (e.g. splenectomy, sickle cell
disease and coeliac syndrome)• Chronic renal disease or nephrotic syndrome• Chronic heart, lung, or liver disease, including cirrhosis• Diabetes mellitus• Complement deficiency (particularly early component deficiencies C1,
C2, C3, C4)• Immunosuppressive conditions (e.g. HIV, leukaemia, lymphoma,
Hodgkin’s disease) and those receiving immunosuppressive therapies• CSF leaks either congenital or complicating skull fracture or
neurosurgery• Intracranial shunt• Candidate for, or recipient of, a cochlear implant• Children under 5 years of age with a history of invasive pneumococcal
disease, irrespective of vaccine history.

Adults >65Adults >65
• All should be offered single dose of Pneumococcal Polysaccharide Vaccine (PPV23)
• Adults 65 years or older should receive a second dose of PPV23 if they received vaccine more than 5 years before and were less than 65 years of age at the time of the first dose.

CURB-65 ScoreCURB-65 Score• Confusion – new onset• Urea - >7 mmol/l• Respiratory rate >30 breaths/minute• Blood Pressure <90/60• Age>65
Score: 0-1 – Treat as outpatient2 – consider admission or follow closely as outpatient> 3 requires hospitalization, mortality >17%

InfluenzaInfluenza
• H1N1 flu pandemic declared over by WHO• now seen as part of seasonal flu• Current seasonal flu vaccine includes a H1N1
strain• Primary Influenza A infection can present
abruptly as rapidly progressive diffuse pneumonia with pulmonary haemorrhage
• More severe in elderly, may develop meningoencephalitis or encephalitis

InfluenzaInfluenza• Treatment: Neuraminidase inhibitors such as oseltamivir
(PO) and Zanamivir (IV) given early in severe or at risk cases
• Often followed by secondary bacterial pneumonia e.g. S pneumoniae, S aureus
• Vaccine less effective in elderly
• Adults over 50 should have annual vaccination
• Those in nursing homes and other long stay facilities should also have annual vaccination

Another CaseAnother Case
• 82 year old woman with 2 months of cough, fatigue, night sweats
• Poor response to Coamoxiclav, tetracycline


TB in IrelandTB in Ireland
• Common in the 1950s
• Many people who were exposed/treated as children then are now presenting with TB now as their immune system wanes with age
Varicella Zoster VirusVaricella Zoster Virus• Cause of Chicken Pox and later Shingles
• Extremely infectious
• Can be severe and even fatal in immunocompromised
• Shingles not uncommon in elderly hospital patients, can leave severe pain of post-herpetic neuralgia
• Pose an infection control risk to immunocompromised, and non immune staff especially to non immune pregnant staff

Not routinely recommended in ElderlyNot routinely recommended in Elderly

Leg UlcersLeg Ulcers• As patients age, increasing peripheral vascular
disease and diabetes can predispose to venous or arterial leg ulcers
• Wet• Warm• Oxygenated• Below the belt• So swabs will always grow something, often grow
patients bowel flora• Treat only if infected!

Case HistoryCase History
• Anne, 74 yr old housewife
• PC: Elective total hip replacement – 3/7 ago• PMHx: Hypertension, Gastric Ca 13 yrs ago• 2/7 post op catheter specimen urine showed
high white cells, Mixed growth predominantly gram negative bacilli
• Given Zinacef po x 5/7

Case HistoryCase History
• 3/7 after Zinacef started, complains of diarrhoeaCauses:• Infectious? – Any other patients on ward
affected?• Non-infective causes?• Hospital food?• Secondary to drugs:
– Antibiotic assoc diarrhoea?– Clostridium difficile?

Case HistoryCase History
Investigations?
Stool Culture sent:
• Culture – NAD, no Salmonella, Shigella, Campylobacter, or E coli 0157
• C diff toxin studies negative
Case HistoryCase History
What next?
Repeat C diff testing: Positive
Treatment?

Case HistoryCase History
• Treatment – po metronidazole 250 mgs qds for 10/7
• Diarrhoea settles – D/C home
• Seen in OPD:

What is C. difficile?What is C. difficile?
Gram positive bacillus
Clostridia = anaerobe
Forms spores
Spread by touch, faecal-oral route
Main sources are: • asymptomatic carriers• Contaminated environment

Resistance to AntibioticsResistance to Antibiotics
No antibiotic – no selection for resistant organisms
sensitive resistant

Resistance to AntibioticsResistance to Antibioticsantibiotic – selects for resistant organisms
sensitive resistant

Clinical PictureClinical Picture
• Clinical ranges from mild diarrhoea to life-threatening colitis
• Occurs 1/7 to 6/52 after antibiotic exposure
• Get watery diarrhoea, lower abdominal pain, blood pr

Clinical PictureClinical Picture
• Systemic symptoms: fever, anorexia, nausea and malaise
• Severely ill may have no diarrhoea due to toxic megacolon
• Complications: perforation, peritonitis – high mortality

Risk FactorsRisk Factors
• Age
• Prior antibiotic use
• Length of hospital stay
• Other severe underlying disease
• C diff strain

Antibiotic culpritsAntibiotic culprits
• Any – including metronidazole
• Main culprits include:– Clindamycin– Cephalosporins– Quinolones e.g. Moxifloxacin, Ciprofloxacin– Broad spectrum antibiotics – e.g. Augmentin,
Meropenem

PathogenesisPathogenesis
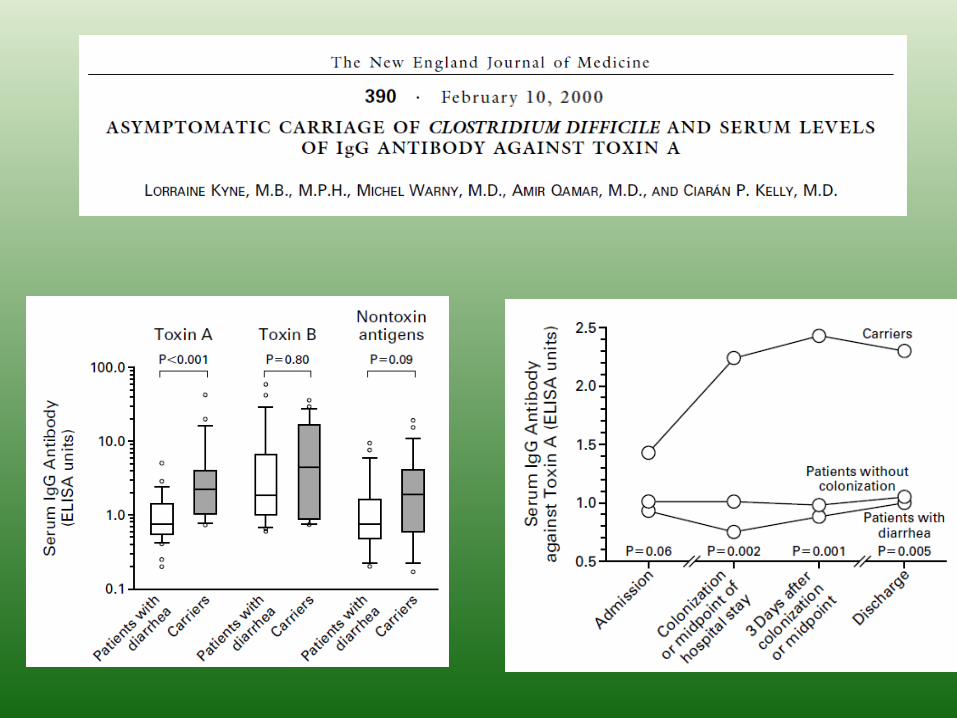
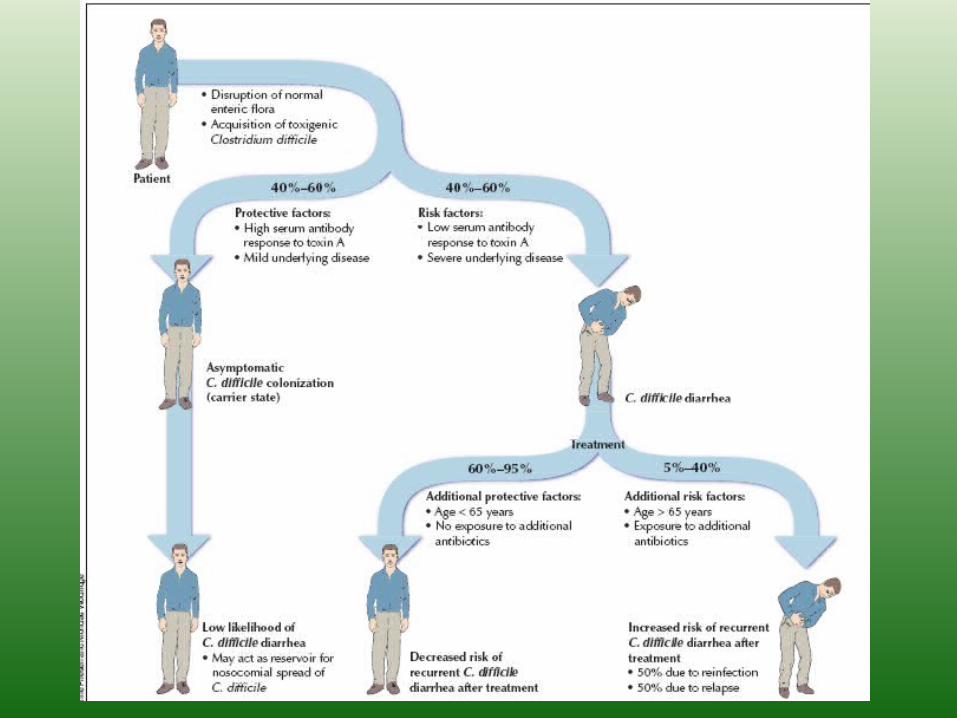
• Disrupts normal bowel flora• Many people especially neonates are colonised
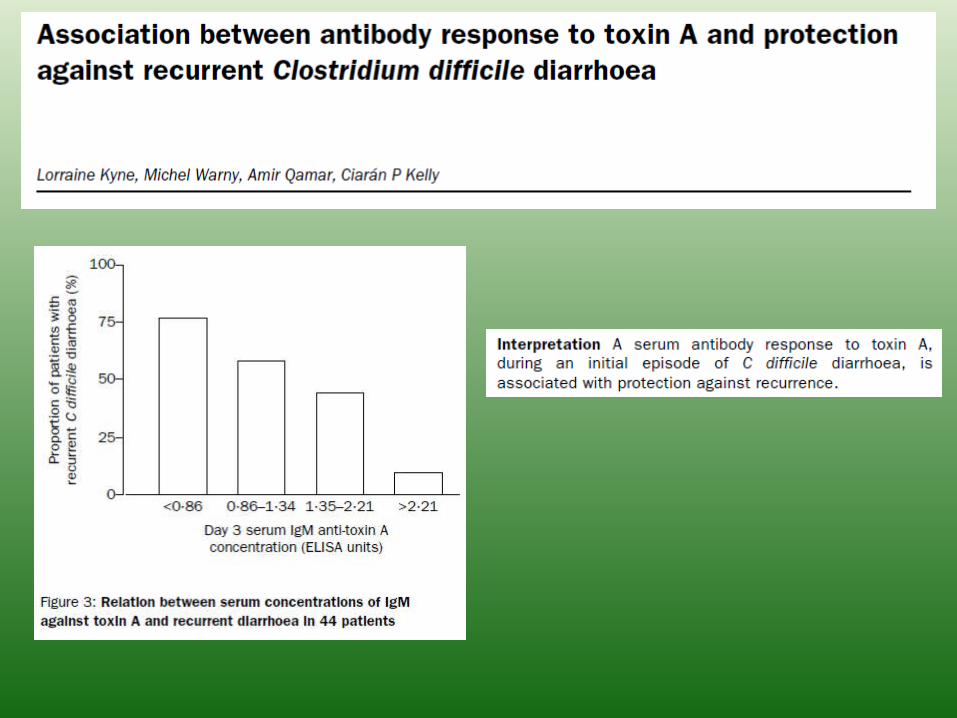
but not infected.• Carriers thought to have better immune
response, infected tend to have lower Ab response
• Two potent cytotoxins, toxins A and B• Can have colitis without pseudomembranes
Spore FormationSpore Formation• Spores provide a method of survival when
environmental conditions are unsuitable
• Protect against ethanol, phenol, formaldehyde, heat
• Killed by iodine, glutaraldehyde, hydrogen peroxide, autoclaving

• Stomach acid kills 99% bacteria but doesn’t affect spores

Pseudomembranous ColitisPseudomembranous Colitis• Due to Clostridium difficile toxins, rarely due to S. aureus
• Symptoms: diarrhoea +/- mucus or blood, abdominal pain, tenderness, fever, dehydration, electrolyte disturbances
• Dx by toxin detection or by endoscopy (risk of perforation)
• Tx: Stop causative agent, give metronidazole or Vancomycin PO for 10/7

DiagnosisDiagnosis
• Culture too slow and those that grow may not express toxins
• Therefore do toxin testing by ELISA• Pseudomembranes can be seen on
endoscopy• Nursing nose!• No point in testing if clinically well or still on
treatment
• O27 strain• Increasingly common• Associated with quinolone use• Higher mortality• Higher infectivity

TreatmentTreatment• Hydration, electrolytes
• Contra-indicated: Antiperistaltics, e.g. imodium
• Severe illness may require surgery esp if perforation or toxic megacolon suspected.
• Probiotics??
Half of recurrences thought to be due to reinfection rather than relapse.
Metronidazole resistance rare.
TX. MUST BE PO!

C difficileC difficile Treatment Guide – IDSA 2010 Treatment Guide – IDSA 2010


UTIsUTIs
• Men often have some degree of prostatic obstruction
• As patients age greater risk of urinary and faecal incontinence
• Nursing home/Hospital/Antibiotic exposure predispose to resistant organisms
• Temptation to catheterise many of these patients indefinitely, this sacrifices patient outcomes for convenience

Epidemiology of Extended Spectrum B-Epidemiology of Extended Spectrum B-Lactamases - IrelandLactamases - Ireland
0
5
10
15
20
25
30
35
40
45
Apr
May Jun
Jul
Aug Sep Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep
2007 2008 2009 2010
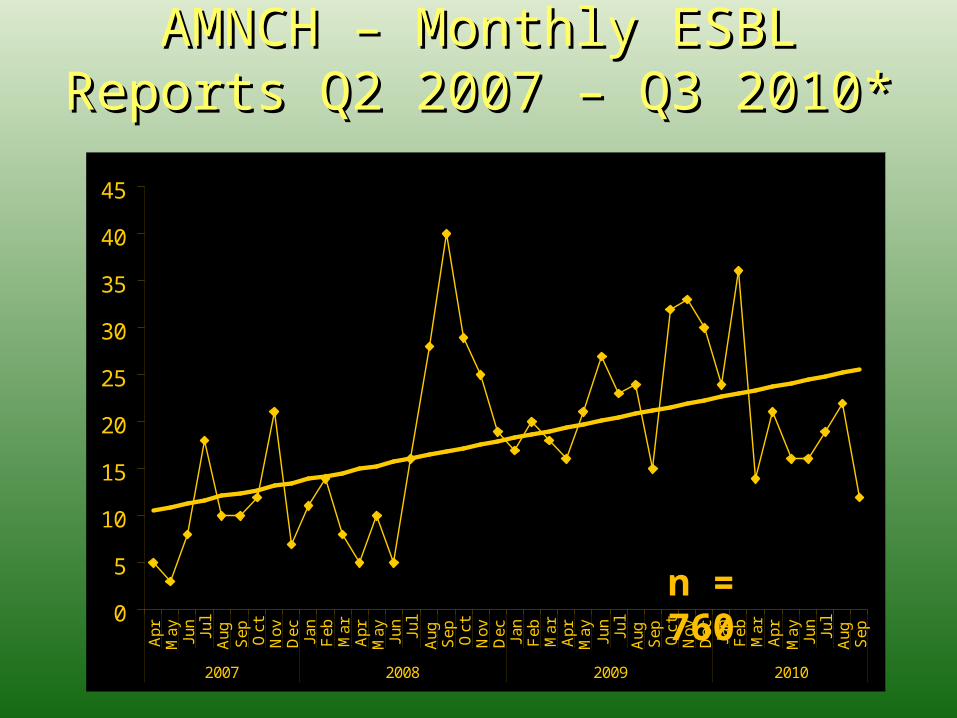
AMNCH – Monthly ESBL Reports Q2 AMNCH – Monthly ESBL Reports Q2 2007 – Q3 2010* 2007 – Q3 2010*
n = 760

EARSS Ireland 02-10 – EARSS Ireland 02-10 – E. coliE. coli
EARSS Quarterly Surveillance Reports – Quarter 1 2010, HPSC

ESBL Sample Type - AMNCHESBL Sample Type - AMNCHFemale: Male 3:2

AMNCH ESBL Age DistributionAMNCH ESBL Age Distribution
Average Age: 60.1Median Age: 66
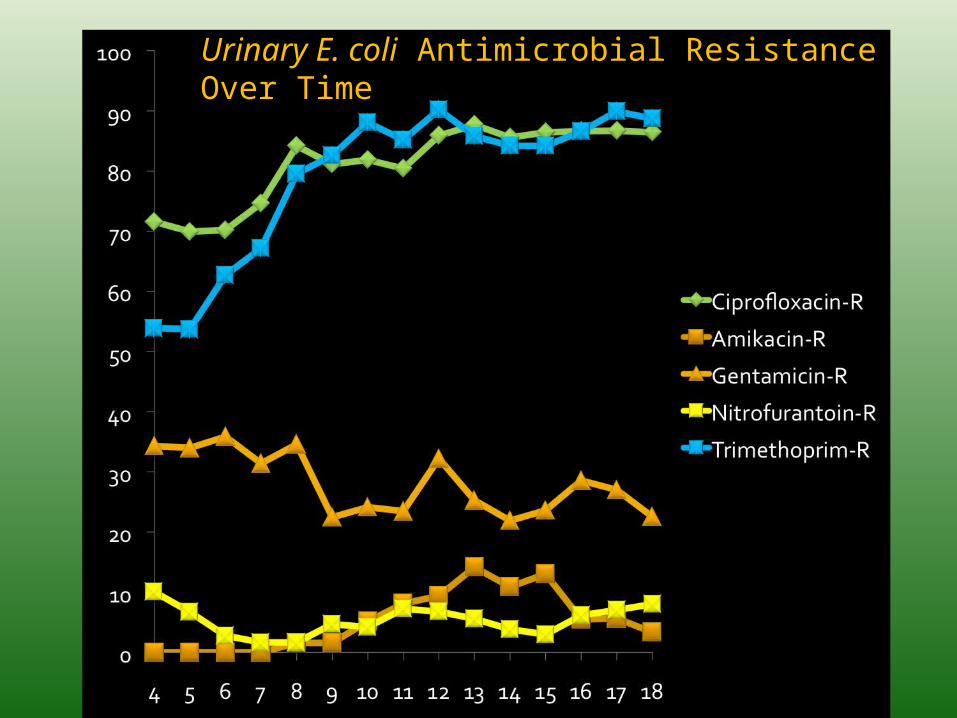
Urinary E. coli Antimicrobial Resistance Over Time

ESBL Resistance Rates
Susceptible (%)Susceptible (%) Intermediate (%)Intermediate (%) Resistant (%)Resistant (%)
BloodBlood UrineUrine BloodBlood UrineUrine BloodBlood UrineUrine
AmikacinAmikacin 11 (78.6)11 (78.6) 312 (86.4)312 (86.4) 2 (14)2 (14) 29 (8.0)29 (8.0) 1 (7.1)1 (7.1) 20 (5.5)20 (5.5)
GentamicinGentamicin 9 (60.0)9 (60.0) 254 (70.2)254 (70.2) 1 (7)1 (7) 3 (0.8)3 (0.8) 5 (33.3)5 (33.3) 105 (29.0)105 (29.0)
CiprofloxacinCiprofloxacin 0 (0)0 (0) 62 (17.0)62 (17.0) 0 (0)0 (0) 1 (0.3)1 (0.3) 15 (100)15 (100) 302 (82.7)302 (82.7)
MeropenemMeropenem 15 (100)15 (100) -- 0 (0)0 (0) -- 0 (0)0 (0) --
TrimethoprimTrimethoprim -- 68 (18.6)68 (18.6) -- 0 (0)0 (0) -- 297 (81.4)297 (81.4)
Nalidixic AcidNalidixic Acid -- 43 (11.8)43 (11.8) -- 1 (0.3)1 (0.3) -- 319 (87.9)319 (87.9)
NitrofurantoinNitrofurantoin -- 323(88.5)323(88.5) -- 20 (5.5)20 (5.5) -- 22 (6.0)22 (6.0)

MortalityMortality
30 day mortality (all causes) = 9.7%
Irish Data (paper in production)
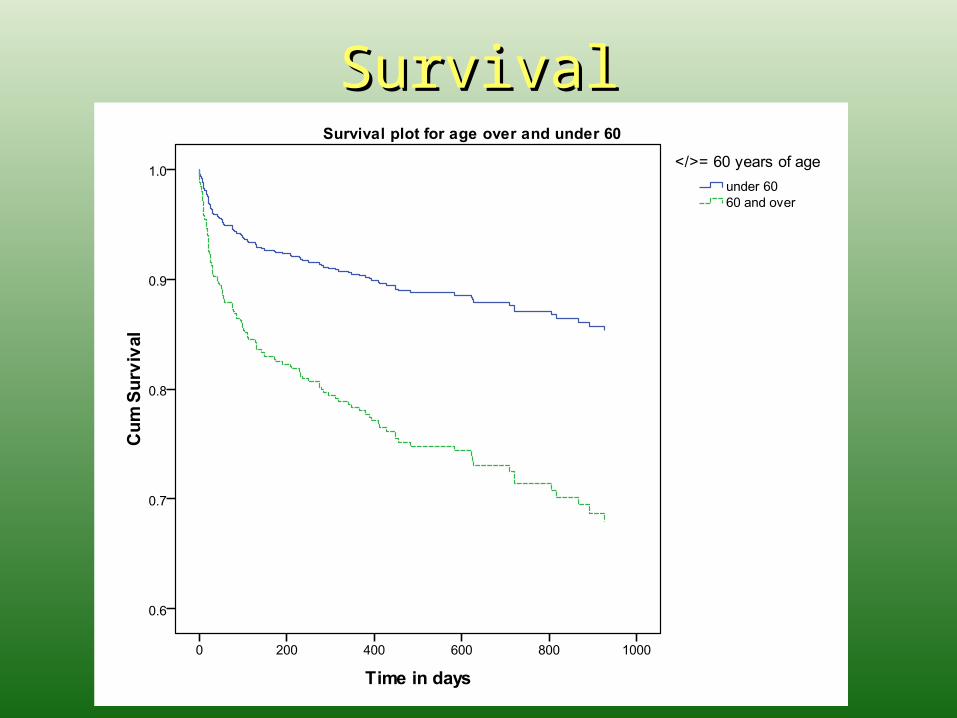
SurvivalSurvival


Treatment by ClassTreatment by Class• Penicillins
• Cephalosporins
• Penicillins +B-lactamase inhibitor
• Quinolones
• Aminoglycosides
• Carbapenems
Useless
Useless
Unreliable
If sensitive
If sensitive
Most reliable...for now

CarbapenemsCarbapenems• E.g. Meropenem, 1E.g. Meropenem, 1stst line choice for line choice for
treatment of serious ESBL infectionstreatment of serious ESBL infections
• stability to all the currently recognised, stability to all the currently recognised, frequently occurring ESBLsfrequently occurring ESBLs
• extensive clinical experienceextensive clinical experience
• Ertapenem also useful for UTIs, home IV Ertapenem also useful for UTIs, home IV tx (once daily)tx (once daily)
• Excess carbapenem use will result in Excess carbapenem use will result in resistanceresistance Paterson DL and Bonomo RA. Clin Microbiol Rev 2005; 18 (4): 657-686

A glimpse of the future...
Other antibioticsOther antibiotics
• Nitrofurantoin po– outpatient settingNitrofurantoin po– outpatient setting
• Tigecycline IV– with caution in Tigecycline IV– with caution in E coliE coli and and Klebsiella Klebsiella (Pseudomonas and (Pseudomonas and Proteus inherently resistant)Proteus inherently resistant)
• Fosfomycin, Temocillin, Pivmecillinam Fosfomycin, Temocillin, Pivmecillinam
• Trimethoprim, Aminoglycosides, Trimethoprim, Aminoglycosides, Quinolones Quinolones when susceptiblewhen susceptible
Paterson DL and Bonomo RA. Clin Microbiol Rev 2005; 18 (4): 657-686

Vancomycin and Gentamicin DosingVancomycin and Gentamicin Dosing• Vancomycin and Gentamicin are nephrotoxic and
ototoxic• Important not to overdose in this age group• Elderly often have some degree of renal impairment• Assess renal function by urea and creatinine levels• If normal, treat normally but watch levels after 24 h
of treatment • If levels high will have to reduce dose

















