Infectious Complications of Biologic Therapies: Preventive and Therapeutic Strategies Kevin L. Winthrop, MD, MPH Assistant Professor, Divisions of Infectious Diseases, Public Health, and Preventive Medicine Oregon Health & Science University
Transcript
Infectious Complications of Biologic Therapies:
Preventive and Therapeutic Strategies
Infectious Complications of Biologic Therapies:
Preventive and Therapeutic Strategies
Kevin L. Winthrop, MD, MPH Assistant Professor, Divisions of Infectious Diseases, Public Health, and
Preventive Medicine Oregon Health & Science University
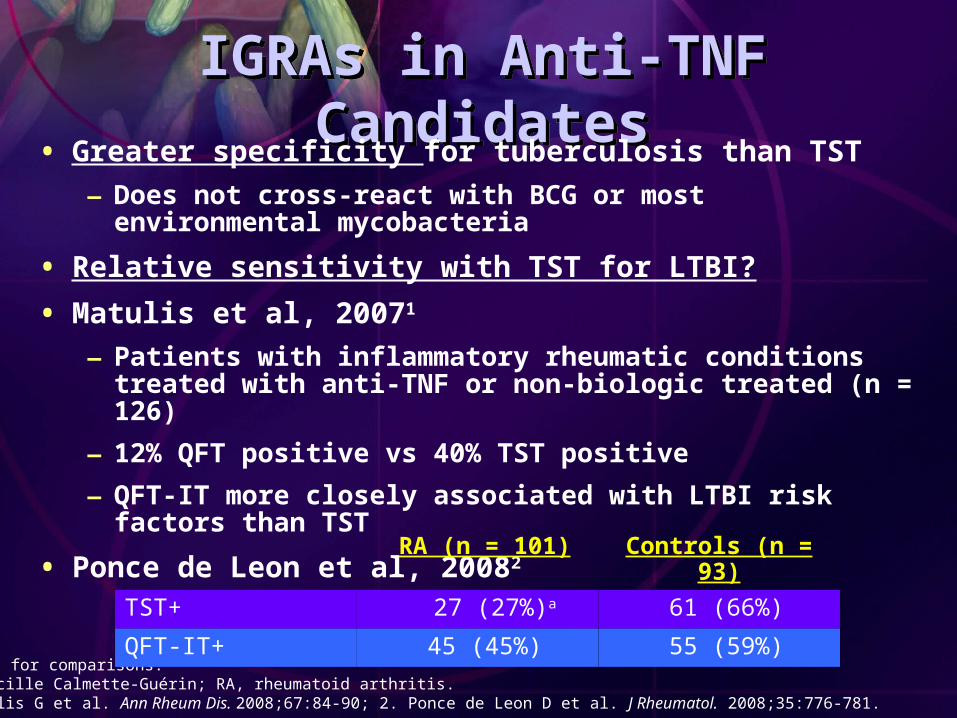
IGRAs in Anti-TNF CandidatesIGRAs in Anti-TNF Candidates• Greater specificity for tuberculosis than TST
– Does not cross-react with BCG or most environmental mycobacteria
• Relative sensitivity with TST for LTBI?
• Matulis et al, 20071
– Patients with inflammatory rheumatic conditions treated with anti-TNF or non-biologic treated (n = 126)
– 12% QFT positive vs 40% TST positive
– QFT-IT more closely associated with LTBI risk factors than TST
• Ponce de Leon et al, 20082
aP < .05 for comparisons.BCG, bacille Calmette-Guérin; RA, rheumatoid arthritis.1. Matulis G et al. Ann Rheum Dis. 2008;67:84-90; 2. Ponce de Leon D et al. J Rheumatol. 2008;35:776-781.
RA (n = 101) Controls (n = 93)
TST+ 27 (27%)a 61 (66%)
QFT-IT+ 45 (45%) 55 (59%)
IGRAs in the Immunocompromised
IGRAs in the Immunocompromised
• Anergy with TST and IGRAs
– IGRAs less affected by prednisone
– False negative with IGRA in patients already receiving anti-TNF therapy1
• Indeterminate results2
– QFT-IT and T-SPOT.TB < QFT-Gold
• LTBI sensitivity2
– QFT-IT similar to T.SPOT.TB (and probably similar to or greater than TST)
– QFT-Gold is less sensitive
1. Hamdi H et al. Arthritis Res Ther. 2006;8:R114.2. Lalvani A, Millington KA. Autoimmun Rev. 2008. Epub ahead of print.
LTBI TreatmentLTBI Treatment
• Begin treatment before starting anti-TNF therapy
– 9 months isoniazid (INH) preferred in US
– 4 months rifampin is alternative
• Start INH 1 month prior to anti-TNF initiation
– 83% reduction in INF-associated cases in Spain1
– Ensure INH compliance and tolerance
• Liver function testing
– Many patients taking MTXMTX, methotrexate.1. Carmona L et al. Arthritis Rheum. 2005;52:1766-1772.
New Biologics for RANew Biologics for RA
• Rituximab
– CD20+ B-cell antibody
– Depletes peripheral B cells
– No TB in RA clinical trials or in lymphoma use
– B cell importance to granuloma/survival in murine model of TB*
• EIN Survey
– 8 TB/NTM cases with rituximab
– All cases also on prednisone
*Maglione et al. J Immunol 2007
AbataceptAbatacept• Tuberculosis risk unknown
– Screened in clinical trials
– Should screen in practice
• Murine chronic TB not affected by abatacept*
– Mortality, T cell, B cell, INF-γ production in lung, and bacillary load
*Bigbee et al. Arth Rheum 2007
TocilizumabTocilizumab
• 10 cases TB in 10,000 patients
– 5 pulmonary
• Should we be screening?
– YES
ConclusionsConclusions
• Anti-TNF–associated mycobacterial cases
– NTM likely more common than TB in US
– M. avium complex is most common
– High mortality
– Severe lung destruction despite anti-NTM therapy
• Screening and prevention
– Chest CT?
– Sputum when appropriate
CT, computed tomography.
Patients Receiving TNF- Antagonists
Patients Receiving TNF- Antagonists
• Physicians should maintain high index of suspicion for TB disease


















































![in.. biologic]. - ed](https://static.documents.pub/doc/80x56/621ad33da61fe5242163542e/in-biologic-ed.jpg)
