63
| Date post: | 02-Nov-2014 |
| Category: |
Documents |
| Upload: | murthy-katari |
| View: | 19 times |
| Download: | 2 times |


NIE 99-17D
January 2000
The Global Infectious DiseaseThreat and Its Implicationsfor the United States

Preface
1
The Global Infectious DiseaseThreat and Its Implicationsfor the United States
I am pleased to share with you this unclassified version of a new NationalIntelligence Estimate on the reemergence of the threat from infectiousdiseases worldwide and its implications for the United States.
This report represents an important initiative on the part of the IntelligenceCommunity to consider the national security dimension of a nontraditionalthreat. It responds to a growing concern by senior US leaders about theimplications—in terms of health, economics, and national security—of thegrowing global infectious disease threat. The dramatic increase in drug-resistant microbes, combined with the lag in development of new antibiot-ics, the rise of megacities with severe health care deficiencies, environmen-tal degradation, and the growing ease and frequency of cross-bordermovements of people and produce have greatly facilitated the spread ofinfectious diseases.
In June 1996, President Clinton issued a Presidential Decision Directivecalling for a more focused US policy on infectious diseases. The StateDepartment’s Strategic Plan for International Affairs lists protecting humanhealth and reducing the spread of infectious diseases as US strategic goals,and Secretary Albright in December 1999 announced the second of twomajor U.S. initiatives to combat HIV/AIDS. The unprecedented UN Secu-rity Council session devoted exclusively to the threat to Africa from HIV/AIDS in January 2000 is a measure of the international community’s con-cern about the infectious disease threat.
As part of this new US Government effort, the National Intelligence Coun-cil produced this National Intelligence Estimate. It examines the mostlethal diseases globally and by region; develops alternative scenarios abouttheir future course; examines national and international capacities to dealwith them; and assesses their national and global social, economic, politi-cal, and security impact. It then assesses the infectious disease threat frominternational sources to the United States; to US military personnel over-seas; and to regions in which the United States has or may develop signifi-cant equities.

2
The Estimate was produced under the auspices of David F. Gordon,National Intelligence Officer for Economics and Global Issues. The pri-mary drafters were Lt. Col. (Dr.) Don Noah of the Armed Forces MedicalIntelligence Center and George Fidas of the NIC. The Estimate also bene-fited from a conference on infectious diseases held jointly with the StateDepartment’s Bureau of Intelligence and Research, and was reviewed byseveral prominent epidemiologists and other health experts in and outsidethe US Government. We hope that it will further inform the debate aboutthis important subject.
John C. GannonChairman, National Intelligence Council

Contents
3
Page
Preface 1Key Judgments 5Discussion 13Patterns of Infectious Diseases 13Factors Affecting Growth and Spread 20Regional Trends and Response Capacity 24International Response Capacity 32Alternative Scenarios and Outlook for Infectious 36DiseasesEconomic, Social, and Political Impacts 46Infectious Diseases and US National Security 53


Key Judgments
5
The Global Infectious DiseaseThreat and Its Implicationsfor the United States
New and reemerging infectious diseases will pose a rising global healththreat and will complicate US and global security over the next 20 years.These diseases will endanger US citizens at home and abroad, threaten USarmed forces deployed overseas, and exacerbate social and political insta-bility in key countries and regions in which the United States has signifi-cant interests.
Infectious diseases are a leading cause of death, accounting for a quarter toa third of the estimated 54 million deaths worldwide in 1998. The spread ofinfectious diseases results as much from changes in human behavior––including lifestyles and land use patterns, increased trade and travel, andinappropriate use of antibiotic drugs––as from mutations in pathogens.
• Twenty well-known diseases––including tuberculosis (TB), malaria, andcholera––have reemerged or spread geographically since 1973, often inmore virulent and drug-resistant forms.
• At least 30 previously unknown disease agents have been identified since1973, including HIV, Ebola, hepatitis C, and Nipah virus, for which nocures are available.
• Of the seven biggest killers worldwide, TB, malaria, hepatitis, and, inparticular, HIV/AIDS continue to surge, with HIV/AIDS and TB likely toaccount for the overwhelming majority of deaths from infectious diseasesin developing countries by 2020. Acute lower respiratory infections––including pneumonia and influenza—as well as diarrheal diseases andmeasles, appear to have peaked at high incidence levels.
Impact Within the United States
Although the infectious disease threat in the United States remains rela-tively modest as compared to that of noninfectious diseases, the trend is up.Annual infectious disease-related death rates in the United States havenearly doubled to some 170,000 annually after reaching an historic low in
6
1980. Many infectious diseases—most recently, the West Nile virus—orig-inate outside US borders and are introduced by international travelers,immigrants, returning US military personnel, or imported animals andfoodstuffs. In the opinion of the US Institute of Medicine, the next majorinfectious disease threat to the United States may be, like HIV, a previouslyunrecognized pathogen. Barring that, the most dangerous known infectiousdiseases likely to threaten the United States over the next two decades willbe HIV/AIDS, hepatitis C, TB, and new, more lethal variants of influenza.Hospital-acquired infections and foodborne illnesses also will pose athreat.
• Although multidrug therapies have cut HIV/AIDS deaths by two-thirdsto 17,000 annually since 1995, emerging microbial resistance to suchdrugs and continued new infections will sustain the threat.
• Some 4 million Americans are chronic carriers of the hepatitis C virus, asignificant cause of liver cancer and cirrhosis. The US death toll from thevirus may surpass that of HIV/AIDS in the next five years.
• TB, exacerbated by multidrug resistant strains and HIV/AIDS co-infec-tion, has made a comeback. Although a massive and costly control effortis achieving considerable success, the threat will be sustained by thespread of HIV and the growing number of new, particularly illegal,immigrants infected with TB.
• Influenza now kills some 30,000 Americans annually, and epidemiolo-gists generally agree that it is not a question of whether, but when, thenext killer pandemic will occur.
• Highly virulent and increasingly antimicrobial resistant pathogens, suchas Staphylococcus aureus, are major sources of hospital-acquired infec-tions that kill some 14,000 patients annually.
• The doubling of US food imports over the last five years is one of thefactors contributing to tens of millions of foodborne illnesses and 9,000deaths that occur annually, and the trend is up.
Regional Trends
Developing and former communist countries will continue to experiencethe greatest impact from infectious diseases—because of malnutrition,

7
poor sanitation, poor water quality, and inadequate health care––but devel-oped countries also will be affected:
• Sub-Saharan Africa—accounting for nearly half of infectious diseasedeaths globally—will remain the most vulnerable region. The death ratesfor many diseases, including HIV/AIDS and malaria, exceed those in allother regions. Sub-Saharan Africa’s health care capacity—the poorest inthe world—will continue to lag.
• Asia and the Pacific, where multidrug resistant TB, malaria, and choleraare rampant, is likely to witness a dramatic increase in infectious diseasedeaths, largely driven by the spread of HIV/AIDS in South and SoutheastAsia and its likely spread to East Asia. By 2010, the region could surpassAfrica in the number of HIV infections.
• The former Soviet Union (FSU) and, to a lesser extent, Eastern Europealso are likely to see a substantial increase in infectious disease incidenceand deaths. In the FSU especially, the steep deterioration in health careand other services owing to economic decline has led to a sharp rise indiphtheria, dysentery, cholera, and hepatitis B and C. TB has reached epi-demic proportions throughout the FSU, while the HIV-infected popula-tion in Russia alone could exceed 1 million by the end of 2000 anddouble yet again by 2002.
• Latin American countries generally are making progress in infectiousdisease control, including the eradication of polio, but uneven economicdevelopment has contributed to widespread resurgence of cholera,malaria, TB, and dengue. These diseases will continue to take a heavytoll in tropical and poorer countries.
• The Middle East and North Africa region has substantial TB and hepa-titis B and C prevalence, but conservative social mores, climatic factors,and the high level of health spending in the oil-producing states tend tolimit some globally prevalent diseases, such as HIV/AIDS and malaria.The region has the lowest HIV infection rate among all regions, althoughthis is probably due in part to above-average underreporting because ofthe stigma associated with the disease in Muslim societies.
• Western Europe faces threats from several infectious diseases, such asHIV/AIDS, TB, and hepatitis B and C, as well as from several economi-cally costly zoonotic diseases (that is, those transmitted from animals tohumans). The region’s large volume of travel, trade, and immigrationincreases the risks of importing diseases from other regions, but its highlydeveloped health care system will limit their impact.

8
Response Capacity
Development of an effective global surveillance and response system prob-ably is at least a decade or more away, owing to inadequate coordinationand funding at the international level and lack of capacity, funds, and com-mitment in many developing and former communist states. Although over-all global health care capacity has improved substantially in recentdecades, the gap between rich and poorer countries in the availabilityand quality of health care, as illustrated by a typology developed by theDefense Intelligence Agency’s Armed Forces Medical Intelligence Center(AFMIC), is widening.
Alternative Scenarios
We have examined three plausible scenarios for the course of the infectiousdisease threat over the next 20 years:
Steady ProgressThe least likely scenario projects steady progress whereby the aging of glo-bal populations and declining fertility rates, socioeconomic advances, andimprovements in health care and medical breakthroughs hasten movementtoward a “health transition” in which such noninfectious diseases as heartdisease and cancer would replace infectious diseases as the overarchingglobal health challenge. We believe this scenario is unlikely primarilybecause it gives inadequate emphasis to persistent demographic and socio-economic challenges in the developing countries, to increasing microbialresistance to existing antibiotics, and because related models have alreadyunderestimated the force of major killers such as HIV/AIDS, TB, andmalaria.
Progress StymiedA more pessimistic—and more plausible––scenario projects little or noprogress in countering infectious diseases over the duration of this Esti-mate. Under this scenario, HIV/AIDS reaches catastrophic proportions asthe virus spreads throughout the vast populations of India, China, theformer Soviet Union, and Latin America, while multidrug treatmentsencounter microbial resistance and remain prohibitively expensive fordeveloping countries. Multidrug resistant strains of TB, malaria, and otherinfectious diseases appear at a faster pace than new drugs and vaccines,wreaking havoc on world health. Although more likely than the “steadyprogress” scenario, we judge that this scenario also is unlikely to prevailbecause it underestimates the prospects for socioeconomic development,international collaboration, and medical and health care advances to con-strain the spread of at least some widespread infectious diseases.

9
Deterioration, Then Limited ImprovementThe most likely scenario, in our view, is one in which the infectious diseasethreat—particularly from HIV/AIDS––worsens during the first half of ourtime frame, but decreases fitfully after that, owing to better prevention andcontrol efforts, new drugs and vaccines, and socioeconomic improvements.In the next decade, under this scenario, negative demographic and socialconditions in developing countries, such as continued urbanization andpoor health care capacity, remain conducive to the spread of infectious dis-eases; persistent poverty sustains the least developed countries as reservoirsof infection; and microbial resistance continues to increase faster than thepace of new drug and vaccine development. During the subsequent decade,more positive demographic changes such as reduced fertility and agingpopulations; gradual socioeconomic improvement in most countries; medi-cal advances against childhood and vaccine-preventable killers such asdiarrheal diseases, neonatal tetanus, and measles; expanded internationalsurveillance and response systems; and improvements in national healthcare capacities take hold in all but the least developed countries. Barringthe appearance of a deadly and highly infectious new disease, a cata-strophic upward lurch by HIV/AIDS, or the release of a highly contagiousbiological agent capable of rapid and widescale secondary spread, thesedevelopments produce at least limited gains against the overall infectiousdisease threat. However, the remaining group of virulent diseases, led byHIV/AIDS and TB, continue to take a significant toll.
Economic, Social, and Political Impact
The persistent infectious disease burden is likely to aggravate and, in somecases, may even provoke economic decay, social fragmentation, and politi-cal destabilization in the hardest hit countries in the developing and formercommunist worlds, especially in the worst case scenario outlined above:
• The economic costs of infectious diseases—especially HIV/AIDS andmalaria—are already significant, and their increasingly heavy toll on pro-ductivity, profitability, and foreign investment will be reflected in grow-ing GDP losses, as well, that could reduce GDP by as much as 20 percentor more by 2010 in some Sub-Saharan African countries, according torecent studies.
• Some of the hardest hit countries in Sub-Saharan Africa—and possiblylater in South and Southeast Asia—will face a demographic upheaval asHIV/AIDS and associated diseases reduce human life expectancy by as

10
much as 30 years and kill as many as a quarter of their populations over adecade or less, producing a huge orphan cohort. Nearly 42 million chil-dren in 27 countries will lose one or both parents to AIDS by 2010; 19 ofthe hardest hit countries will be in Sub-Saharan Africa.
The relationship between disease and political instability is indirect butreal. A wide-ranging study on the causes of state instability suggests thatinfant mortality—a good indicator of the overall quality of life—correlatesstrongly with political instability, particularly in countries that already haveachieved a measure of democracy. The severe social and economic impactof infectious diseases is likely to intensify the struggle for political powerto control scarce state resources.
Implications for US National Security
As a major hub of global travel, immigration, and commerce with wide-ranging interests and a large civilian and military presence overseas, theUnited States and its equities abroad will remain at risk from infectiousdiseases.
• Emerging and reemerging infectious diseases, many of which are likelyto continue to originate overseas, will continue to kill at least 170,000Americans annually. Many more could perish in an epidemic of influenzaor yet-unknown disease or if there is a substantial decline in the effective-ness of available HIV/AIDS drugs.
• Infectious diseases are likely to continue to account for more militaryhospital admissions than battlefield injuries. US military personneldeployed at NATO and US bases overseas, will be at low-to-moderaterisk. At highest risk will be US military forces deployed in support ofhumanitarian and peacekeeping operations in developing countries.
• The infectious disease burden will weaken the military capabilities ofsome countries—as well as international peacekeeping efforts––as theirarmies and recruitment pools experience HIV infection rates rangingfrom 10 to 60 percent. The cost will be highest among officers and themore modernized militaries in Sub-Saharan Africa and increasinglyamong FSU states and possibly some rogue states.

11
• Infectious diseases are likely to slow socioeconomic development in thehardest-hit developing and former communist countries and regions. Thiswill challenge democratic development and transitions and possibly con-tribute to humanitarian emergencies and civil conflicts.
• Infectious disease-related embargoes and restrictions on travel and immi-gration will cause frictions among and between developed and develop-ing countries.
• The probability of a bioterrorist attack against US civilian and militarypersonnel overseas or in the United States also is likely to grow as morestates and groups develop a biological warfare capability. Although thereis no evidence that the recent West Nile virus outbreak in New York Citywas caused by foreign state or nonstate actors, the scare and several ear-lier instances of suspected bioterrorism showed the confusion and fearthey can sow regardless of whether or not they are validated.

12

Discussion
13
The Global Infectious DiseaseThreat and Its Implicationsfor the United States
Patterns of Infectious Diseases
Broad advances in controlling or eradicating agrowing number of infectious diseases—suchas tuberculosis (TB), malaria, and smallpox––in the decades after the Second World Warfueled hopes that the global infectious diseasethreat would be increasingly manageable. Opti-mism regarding the battle against infectiousdiseases peaked in 1978 when the UnitedNations (UN) member states signed the“Health for All 2000” accord, which predictedthat even the poorest nations would undergo ahealth transition before the millennium,whereby infectious diseases no longer wouldpose a major danger to human health. Asrecently as 1996, a World Bank/World HealthOrganization (WHO)–sponsored study byChristopher J.L. Murray and Alan D. Lopezprojected a dramatic reduction in the infectiousdisease threat. This optimism, however, led tocomplacency and overlooked the role of suchfactors as expanded trade and travel and grow-ing microbial resistance to existing antibioticsin the spread of infectious diseases. Today:
• Infectious diseases remain a leading cause ofdeath (see figure 1). Of the estimated 54 mil-lion deaths worldwide in 1998, about one-fourth to one-third were due to infectious dis-eases, most of them in developing countriesand among children globally.
• Infectious diseases accounted for 41 percentof the global disease burden measured interms of Disability-Adjusted Life Years(DALYS) that gauge the impact of bothdeaths and disabilities, as compared to43 percent for noninfectious diseases and16 percent for injuries.
• Although there has been continuing progressin controlling some vaccine-preventablechildhood diseases such as polio, neonataltetanus, and measles, a White House–appointed interagency working group identi-fied at least 29 previously unknown diseasesthat have appeared globally since 1973, manyof them incurable, including HIV/AIDS,Ebola hemorrhagic fever, and hepatitis C.Most recently, Nipah encephalitis was identi-fied. Twenty well-known diseases such asmalaria, TB, cholera, and dengue haverebounded after a period of decline or spreadto new regions, often in deadlier forms(see table 1).
• These trends are reflected in the United Statesas well, where annual infectious diseasedeaths have nearly doubled to some 170,000since 1980 after reaching historic lows thatyear, while new and existing pathogens, suchas HIV and West Nile virus, respectively,continue to enter US borders.

14
The Deadly SevenThe seven infectious diseases that caused thehighest number of deaths in 1998, according toWHO and DIA’s Armed Forces Medical Intelli-gence Center (AFMIC), will remain threatswell into the next century. HIV/AIDS, TB,malaria, and hepatitis B and C––are eitherspreading or becoming more drug-resistant,while lower respiratory infections, diarrhealdiseases, and measles, appear to have at leasttemporarily peaked (see figure 2).
HIV/AIDS. Following its identification in1983, the spread of HIV intensified quickly.Despite progress in some regions, HIV/AIDSshows no signs of abating globally (see figure3). Approximately 2.3 million people died fromAIDS worldwide in 1998, up dramatically from0.7 million in 1993, and there were 5.8 millionnew infections. According to WHO, some 33.4million people were living with HIV by 1998,up from 10 million in 1990, and the numbercould approach 40 million by the end of 2000.
Source: US Institute of Medicine, 1997; WHO, 1999.
Table 1Examples of Pathogenic Microbes and the DiseasesThey Cause, Identified Since 1973
Year Microbe Type Disease
1973 Rotavirus Virus Infantile diarrhea1977 Ebola virus Virus Acute hemorrhagic fever1977 Legionella pneumophila Bacterium Legionnaires’ disease1980 Human T-lymphotrophic
virus I (HTLV 1)Virus T-cell lymphoma/leukemia
1981 Toxin-producingStaphylococcus aureus
Bacterium Toxic shock syndrome
1982 Escherichia coli O157:H7 Bacterium Hemorrhagic colitis; hemolyticuremic syndrome
1982 Borrelia burgdorferi Bacterium Lyme disease1983 Human Immunodeficiency
Virus (HIV)Virus Acquired Immuno-Deficiency
Syndrome (AIDS)1983 Helicobacter pylori Bacterium Peptic ulcer disease1989 Hepatitis C Virus Parentally transmitted non-A,
non-B liver infection1992 Vibrio cholerae O139 Bacterium New strain associated with
epidemic cholera1993 Hantavirus Virus Adult respiratory distress
syndrome1994 Cryptosporidium Protozoa Enteric disease1995 Ehrlichiosis Bacterium Severe arthritis?1996 nvCJD Prion New variant Creutzfeldt-Jakob
disease1997 HVN1 Virus Influenza1999 Nipah Virus Severe encephalitis

15
Although infection and death rates have slowedconsiderably in developed countries owing tothe growing use of preventive measures andcostly new multidrug treatment therapies, thepandemic continues to spread in much of thedeveloping world, where 95 percent of globalinfections and deaths have occurred. Sub-Saharan Africa currently has the biggestregional burden, but the disease is spreadingquickly in India, Russia, China, and much ofthe rest of Asia. HIV/AIDS probably will causemore deaths than any other single infectiousdisease worldwide by 2020 and may accountfor up to one-half or more of infectious diseasedeaths in the developing world alone.
TB. WHO declared TB a global emergency in1993 and the threat continues to grow, espe-cially from multidrug resistant TB (see figure4). The disease is especially prevalent in Rus-sia, India, Southeast Asia, Sub-Saharan Africa,and parts of Latin America. More than 1.5 mil-lion people died of TB in 1998, excluding those
infected with HIV/AIDS, and there were up to7.4 million new cases. Although the vast major-ity of TB infections and deaths occur in devel-oping regions, the disease also is encroachinginto developed regions due to increased immi-gration and travel and less emphasis on preven-tion. Drug resistance is a growing problem; theWHO has reported that up to 50 percent of peo-ple with multidrug resistant TB may die of theirinfection despite treatment, which can be 10 to50 times more expensive than that used fordrug-sensitive TB. HIV/AIDS also has contrib-uted to the resurgence of TB. One-quarter ofthe increase in TB incidence involves co-infec-tion with HIV. TB probably will rank secondonly to HIV/AIDS as a cause of infectious dis-ease deaths by 2020.
A Word About Data
All data concerning global disease inci-dence, including WHO data, should betreated as broadly indicative of trends ratherthan accurate measures of disease preva-lence. Much disease incidence in developingcountries, in particular, is either unreportedor under-reported due to a lack of adequatemedical and administrative personnel, thestigma associated with many diseases, or thereluctance of countries to incur the trade,tourism, and other losses that such revela-tions might produce. Since much morbidityand mortality are multicausal, moreover,diagnosis and reporting of diseases can vary
and further distort comparisons. WHO andother international entities are dependent onsuch data despite its weaknesses and areoften forced to extrapolate or build modelsbased on relatively small samples, as in thecase of HIV/AIDS. Changes in methodolo-gies, moreover, can produce differing results.The ranking of AIDS mortality ahead of TBmortality in figure 2, for example, partlyowes to the fact that HIV-positive individualsdying of TB were included in the AIDSmortality category in the most recentWHO survey.

16
Malaria, a mainly tropical disease that seemedto be coming under control in the 1960sand 1970s, is making a deadly comeback––especially in Sub-Saharan Africa where infec-tion rates increased by 40 percent from 1970 to
1997 (see figure 5). Drug resistance, histori-cally a problem only with the most severe formof the disease, is now increasingly reported inthe milder variety, while the prospects for aneffective vaccine are poor. In 1998, an esti-mated 300 million people were infected withmalaria, and more than 1.1 million died fromthe disease that year. Most of the deathsoccurred in Sub-Saharan Africa. According tothe US Agency for International Development(USAID), Sub-Saharan Africa alone is likely toexperience a 7- to 20-percent annual increase inmalaria-related deaths and severe illnesses overthe next several years.
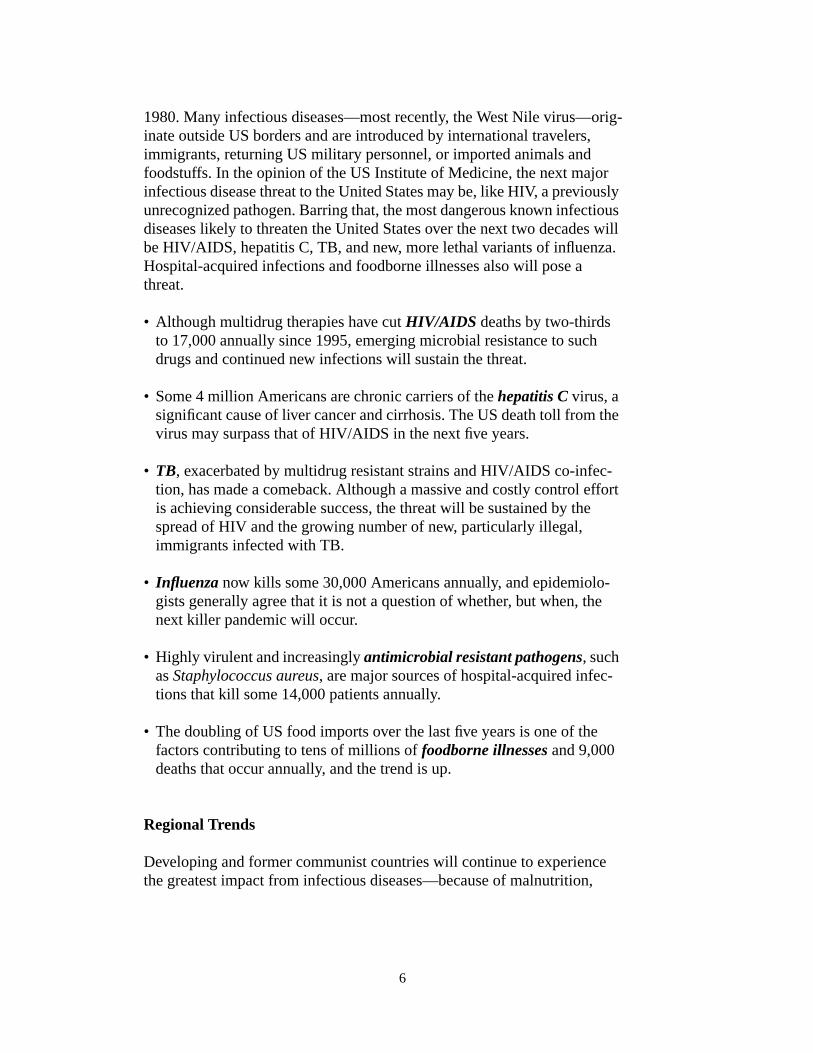
Hepatitis B and C. Hepatitis B, which causedat least 0.6 million deaths in 1997, is highlyendemic in the developing world, and some 350million people worldwide are chronic carriers(see figure 6). The less prevalent but far morelethal hepatitis C identified in 1989 has growndramatically and is a significant contributor tocirrhosis and liver cancer. WHO estimated that3 percent of the global population was infectedwith the hepatitis C virus by 1997 (see figure7), which means that more than 170 millionpeople were at risk of developing the diseasesassociated with this virus. Various studiesproject that up to 25 percent of people withchronic hepatitis B and C will die of cirrhosisof the liver and liver cancer over the next 20 to30 years.
Lower respiratory infections, especially influ-enza and pneumonia, killed 3.5 million peoplein 1998, most of them children in developingcountries, down from 4.1 million in 1993.Owing to immunosuppression from malnutri-tion and growing microbial resistance to com-monly used drugs such as penicillin, these
Glossary
Infectious DiseaseAn illness due to a specific infectiousagent that is spread from an infected per-son, animal, or inanimate reservoir to asusceptible host, either directly or indi-rectly, through an intermediate plant oranimal host, vector, or the inanimate envi-ronment.
EndemicThe constant presence of a disease orinfectious agent within a given geographicarea.
EpidemicThe occurrence in an area of a disease orillness in excess of what may be expectedon the basis of past experience for a givenpopulation (in the case of a new disease,such as AIDS, any occurrence may be con-sidered “epidemic”).
PandemicA worldwide epidemic affecting an excep-tionally high proportion of the global pop-ulation.
PrevalenceThe number of existing cases of a diseaseamong a total or specified population in agiven period of time; usually expressed asa percent or as the number of cases perthousand, 10,000, and so forth.

17
children are especially vulnerable to such dis-eases and will continue to experience highdeath rates.
Diarrheal diseases—mainly spread bycontaminated water or food—accounted for2.2 million deaths in 1998, as compared to 3million in 1993, of which about 60 percentoccurred among children under five years of
age in developing countries. The most commoncause of death related to diarrheal diseases isinfection with Escherichia coli. Other diarrhealdiseases include cholera, dysentery, and rotavi-ral diarrhea, prevalent throughout the develop-ing world and, more recently, in many formercommunist states. Such waterborne and food-borne diseases will remain highly prevalent in

18

19

20
these regions in the absence of improvementsin water quality and sanitation.
Measles. Despite substantial progress againstmeasles in recent years, the disease still infectssome 42 million children annually and killedabout 0.9 million in 1998, down from 1.2 mil-lion in 1993. It is a leading cause of deathamong refugees and internally displaced per-sons during complex humanitarian emergen-cies. Measles will continue to pose a majorthreat in developing countries (see figure 8),particularly Sub-Saharan Africa, until the stillrelatively low vaccination rates are substan-tially increased. It also will continue to causeperiodic epidemics in areas such as SouthAmerica with higher, but still inadequate, vac-cination rates.
Factors Affecting Growth and Spread
With few exceptions, the resurgence of theinfectious disease threat is due as much to dra-matic changes in human behavior and broadersocial, economic, and technological develop-ments as to mutations in pathogens (see table2). Changes in human behavior include popula-tion dislocations, living styles, and sexual prac-tices; technology-driven medical proceduresentailing some risks of infection; and land usepatterns. They also include rising internationaltravel and commerce that hasten the spread ofinfectious diseases; inappropriate use of antibi-otics that leads to the development of microbialresistance; and the breakdown of public healthsystems in some countries owing to war or eco-nomic decline. In addition, climate changesenable diseases and vectors to expand theirrange. Several of these factors interact, exacer-bating the spread of infectious diseases.
Human Demographics and BehaviorPopulation growth and urbanization, particu-larly in the developing world, will continue tofacilitate the transfer of pathogens among peo-ple and regions. Frequent and often suddenpopulation movements within and across bor-ders caused by ethnic conflict, civil war,and famine will continue to spread diseasesrapidly in affected areas, particularly amongrefugees. As of 1999, there were some24 major humanitarian emergencies worldwideinvolving at least 35 million refugees and inter-nally displaced people. Refugee camps, found
Source: Adapted from US Institute of Medicine, 1997.
Table 2Factors Contributing to Infectious DiseaseReemergence and Associated Diseases
Contributing Factor(s) Associated InfectiousDiseases
Human demographics andbehavior
Dengue/dengue hemorrhagicfever, sexually transmitteddiseases, giardiasis
Technology and industry Toxic shock syndrome, noso-comial (hospital-acquired)infections, hemorrhagiccolitis/hemolytic uremicsyndrome
Economic development andland use
Lyme disease, malaria,plague, rabies, yellow fever,Rift Valley fever,schistosomiasis
International travel andcommerce
Malaria, cholera, pneumococ-cal pneumonia
Microbial adaptation andchange
Influenza, HIV/AIDS,malaria, Staphylococcusaureus infections
Breakdown of public healthmeasures
Rabies, tuberculosis, trenchfever, diphtheria, whoopingcough (pertussis), cholera
Climate change Malaria, dengue, cholera,yellow fever
21

22
mainly in Sub-Saharan Africa and the MiddleEast, facilitate the spread of TB, HIV, cholera,dysentery, and malaria. Well over 120 millionpeople lived outside the country of their birth in1998, and millions more will emigrate annu-ally, increasing the spread of diseases globally.Behavioral patterns, such as unprotected sexwith multiple partners and intravenous druguse, will remain key factors in the spread ofHIV/AIDS.
Technology, Medicine, and IndustryAlthough technological breakthroughs willgreatly facilitate the detection, diagnosis, andcontrol of certain infectious and noninfectiousillnesses, they also will introduce new dangers,especially in the developed world where theyare used extensively. Invasive medical proce-dures will result in a variety of hospital-acquired infections, such as Staphylococcusaureus. The globalization of the food supplymeans that nonhygienic food production, prep-aration, and handling practices in originatingcountries can introduce pathogens endangeringforeign as well as local populations. Diseaseoutbreaks due to Cyclospora spp, Escherichiacoli, and Salmonella spp. in several countries,along with the emergence, primarily in Britain,of Bovine Spongiform Encephalopathy, or“mad cow” disease, and the related new variantCreutzfeldt-Jakob disease (nvCJD) affectinghumans, result from such food practices.
Economic Development and Land UseChanges in land and water use patterns willremain major factors in the spread of infectiousdiseases. The emergence of Lyme disease in theUnited States and Europe has been linked toreforestation and increases in the deer tick pop-ulation, which acts as a vector, while conver-sion of grasslands to farming in Asia
encourages the growth of rodent populationscarrying hemorrhagic fever and other viral dis-eases. Human encroachment on tropical forestswill bring populations into closer proximitywith insects and animals carrying diseases suchas leishmaniasis, malaria, and yellow fever, aswell as heretofore unknown and potentiallydangerous diseases, as was the case with HIV/AIDS. Close contact between humans and ani-mals in the context of farming will increase theincidence of zoonotic diseases––those trans-mitted from animals to humans. Water manage-ment efforts, such as dambuilding, willencourage the spread of water-breeding vectorssuch as mosquitoes and snails that have con-tributed to outbreaks of Rift Valley fever andschistosomiasis in Africa.
International Travel and CommerceThe increase in international air travel, trade,and tourism will dramatically increase the pros-pects that infectious disease pathogens such asinfluenza—and vectors such as mosquitoes androdents—will spread quickly around the globe,often in less time than the incubation period ofmost diseases. Earlier in the decade, for exam-ple, a multidrug resistant strain of Streptococ-cus pneumoniae originating in Spain spreadthroughout the world in a matter of weeks,according to the director of WHO’s infectiousdisease division. The cross-border movementof some 2 million people each day, including1 million between developed and developingcountries each week, and surging global tradeensure that travel and commerce will remainkey factors in the spread of infectious diseases.
23
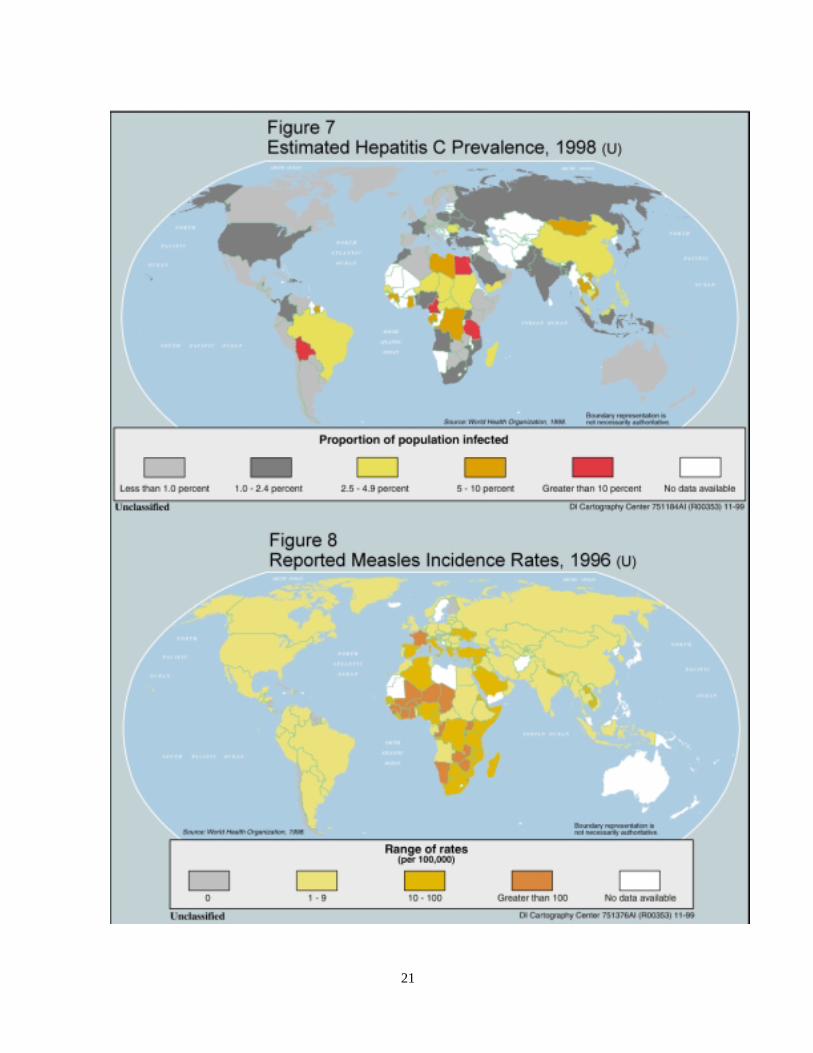
Microbial Adaptation and ResistanceInfectious disease microbes are constantlyevolving, oftentimes into new strains that areincreasingly resistant to available antibiotics.As a result, an expanding number of strains ofdiseases—such as TB, malaria, and pneumo-nia—will remain difficult or virtually impossi-ble to treat. At the same time, large-scale use ofantibiotics in both humans and livestock willcontinue to encourage development of micro-bial resistance. The firstline drug treatment formalaria is no longer effective in over 80 of the92 countries where the disease is a major healthproblem. Penicillin has substantially lost itseffectiveness against several diseases, such aspneumonia, meningitis, and gonorrhea, in
many countries. Eighty percent of Staphylococ-cus aureus isolates in the United States, forexample, are penicillin-resistant and 32 percentare methicillin-resistant. A US Centers for Dis-ease Control and Prevention (USCDC) studyfound a 60-fold increase in high-level resis-tance to penicillin among one group of Strepto-coccus pneumoniae cases in the United Statesand significant resistance to multidrug therapyas well. Influenza viruses, in particular, are par-ticularly efficient in their ability to survive andgenetically change, sometimes into deadlystrains. HIV also displays a high rate of geneticmutation that will present significant problemsin the development of an effective vaccine ornew, affordable therapies.
Note: Antimicrobial resistance occurs when a disease-carryingmicrobe (bacteria, virus, parasite, or fungus) is no longer affectedby a drug that previously was able to kill the microbe or prevent itfrom growing. Even among populations of microorganisms thatare susceptible to a particular antimicrobial agent, at least a smallpercentage of those organisms are naturally resistant, and theirproportion will grow as the others succumb to the antimicrobialagent. Eventually this process renders the agent ineffective againstthe microorganism.
Source: US Institute of Medicine, 1997; WHO, 1999.
Table 3Examples of Drug-Resistant Infectious Agents andPercentage of Infections That Are Drug Resistant,by Country or Region
Pathogen Drug Country/Region Percentage of Drug-ResistantInfections
Streptococcus pneumoniae Penicillin United StatesAsia, Chile, Spain,Hungary
10 to 352058
Staphylococcus aureus MethicillinMultidrug
United StatesJapan
3260
Mycobacterium tuberculosis Any drugAny drugMultidrug
United StatesNew York CityEastern Europe
131620
Plasmodium falciparummalaria
Chloroquine
Mephloquine
KenyaGhanaZimbabweBurkina FasoThailand
6545591745
Shigella dysenteride Multidrug Burundi, Rwanda 100

24
Breakdown in Public Health CareAlone or in combination, war and natural disas-ters, economic collapse, and human compla-cency are causing a breakdown in health caredelivery and facilitating the emergence orreemergence of infectious diseases. While Sub-Saharan Africa is the area currently mostaffected by these factors, economic problems inRussia and other former communist states arecreating the context for a large increase ininfectious diseases. The deterioration of basichealth care services largely accounts for thereemergence of diphtheria and other vaccine-preventable diseases, as well as TB, as fundsfor vaccination, sanitation, and water purifica-tion have dried up. In developed countries, pastinroads against infectious diseases led to arelaxation of preventive measures such as sur-veillance and vaccination. Inadequate infectioncontrol practices in hospitals will remain amajor source of disease transmission in devel-oping and developed countries alike.
Climate ChangeClimatic shifts are likely to enable some dis-eases and associated vectors––particularlymosquito-borne diseases such as malaria, yel-low fever, and dengue––to spread to new areas.Warmer temperatures and increased rainfallalready have expanded the geographic range ofmalaria to some highland areas in Sub-SaharanAfrica and Latin America and could add sev-eral million more cases in developing countryregions over the next two decades. The occur-rence of waterborne diseases associated withtemperature-sensitive environments, such ascholera, also is likely to increase.
Regional Trends and Response Capacity
The overall level of global health care capacityhas improved substantially in recent decades,but in most poorer countries the availability of
various types of health care––ranging frombasic pharmaceuticals and postnatal care tocostly multidrug therapies––remains very lim-ited. Almost all research and developmentfunds allocated by developed country govern-ments and pharmaceutical companies, more-over, are focused on advancing therapies anddrugs relevant to developed country maladies,and those that are relevant to developing coun-try needs usually are beyond their financialreach. This is generating a growing controversybetween rich and poorer nations over suchissues as intellectual property rights, as somedeveloping countries seek to meet their phar-maceutical needs with locally produced genericproducts. Malnutrition, poor sanitation, andpoor water quality in developing countries alsowill continue to add to the disease burden thatis overwhelming health care infrastructures inmany countries. So too, will political instabilityand conflict and the reluctance of many govern-ments to confront issues such as the spread ofHIV/AIDS. A global composite measure ofhealth care infrastructure devised by DIA’sArmed Forces Medical Intelligence Center(AFMIC) assesses factors such as the priorityattributed to health care, health expenditures,the quality of health care delivery and access todrugs, and the extent of surveillance andresponse systems. The AFMIC typology high-lights the disparities in health care capacity (seefigure 9), as do various WHO, UNAIDS, andWorld Bank studies.
Sub-Saharan AfricaSub-Saharan Africa will remain the regionmost affected by the global infectious diseasephenomenon––accounting for nearly half ofinfectious disease-caused deaths worldwide.Deaths from HIV/AIDS, malaria, cholera, andseveral lesser known diseases exceed those in

25

27
all other regions. Sixty-five percent of alldeaths in Sub-Saharan Africa are caused byinfectious diseases. Rudimentary health caredelivery and response systems, the unavailabil-ity or misuse of drugs, the lack of funds, andthe multiplicity of conflicts are exacerbating thecrisis. According to the AFMIC typology, withthe exception of southern Africa, most of Sub-Saharan Africa falls in the lowest category.Investment in health care in the region is mini-mal, less than 40 percent of the people in coun-tries such as Nigeria and the DemocraticRepublic of the Congo (DROC) have access tobasic medical care, and even in relatively welloff South Africa, only 50 to 70 percent havesuch access, with black populations at the lowend of the spectrum.
Four-fifths of all HIV-related deaths and 70 per-cent of new infections worldwide in 1998occurred in the region, totaling 1.8-2 millionand 4 million, respectively. Although only atenth of the world’s population lives in theregion, 11.5 million of 13.9 million cumulativeAIDS deaths have occurred there. Eastern andsouthern African countries, including SouthAfrica, are the worst affected, with 10 to 26percent of adults infected with the disease. Sub-Saharan Africa has high TB prevalence, as wellas the highest HIV/TB co-infection rate, withTB deaths totaling 0.55 million in 1998. Thehardest hit countries are in equatorial and espe-cially southern Africa. South Africa, in particu-lar, is facing the biggest increase in the region.
Sub-Saharan Africa accounts for an estimated90 percent of the global malaria burden (seefigure 10). Ten percent of the regional diseaseburden is attributed to malaria, with roughly 1million deaths in 1998. Cholera, dysentery, andother diarrheal diseases also are major killers inthe region, particularly among children, refu-gees, and internally displaced populations.
Forty percent of all childhood deaths fromdiarrheal diseases occur in Sub-Saharan Africa.The region also has a high rate of hepatitis Band C infections and is the only region with aperennial meningococcal meningitis problemin a “meningitis belt” stretching from west toeast. Sub-Saharan Africa also suffers from yel-low fever, while trypanasomiasis or “sleepingsickness” is making a comeback in the DROCand Sudan, and the Marburg virus alsoappeared in DROC for the first time in 1998.Ebola hemorrhagic fever strikes sporadically incountries such as the DROC, Gabon, Coted’Ivoire, and Sudan (see figure 11).
Asia and the PacificAlthough the more developed countries of Asiaand the Pacific, such as Japan, South Korea,Australia, and New Zealand, have strongrecords in combating infectious diseases, infec-tious disease prevalence in South and SoutheastAsia is almost as high as in Sub-SaharanAfrica. The health care delivery system of theAsia and Pacific region––the majority of whichis privately financed––is particularly vulnerableto economic downturns even though this is off-set to some degree by much of the region’s reli-ance on traditional medicine from localpractitioners. According to the AFMIC typol-ogy, 90 to 100 percent of the populations in themost developed countries, such as Japan andAustralia, have access to high-quality healthcare. Forty to 50 percent have such accessamong the large populations of China andSouth Asia, while southeast Asian health careis more varied, with less than 40 percent enjoy-ing such access in Burma and Cambodia, and50 to 70 percent in Thailand, Malaysia, and thePhilippines. In South and Southeast Asia,reemergent diseases such as TB, malaria, chol-era, and dengue fever are rampant, while HIV/AIDS, after a late start, is growing faster than inany other region.

28
TB caused 1 million deaths in the Asia andPacific region in 1998, more than any other sin-gle disease, with India and China accountingfor two-thirds of the total. Several million newcases occur annually—most in India, China andIndonesia—representing as much as 40 percentof the global TB burden. HIV/AIDS is increas-ing dramatically, especially in India, whichleads the world in absolute numbers of HIV/AIDS infections, estimated at 3-5 million.China is better off than most of the countriesto its south, but it too has a growing AIDSproblem, with HIV infections variously esti-mated at 0.1-0.4 million and spreading rapidly.
Regionwide, the number of people infectedwith HIV could overtake Sub-Saharan Africa inabsolute numbers before 2010.
There were 19.5 million new malaria infectionsestimated in the Asia and Pacific region in1998, many of them drug resistant, and 100,000deaths due to malaria. Acute respiratory infec-tions, such as pneumonia, cause about 1.8 mil-lion childhood deaths annually––over half ofthem in India––while dengue (including den-gue hemorrhagic fever/dengue shock syn-drome) outbreaks have spread throughout theregion in the last five years. Waterborne

29
illnesses such as dysentery and cholera alsotake a heavy toll in poor and crowded areas.Asian, particularly Chinese, agricultural prac-tices place farm animals, fowl, and humans inclose proximity and have long facilitated theemergence of new strains of influenza thatcause global pandemics. Hepatitis B is widelyprevalent in the region, while hepatitis C isprevalent in China and in parts of southeastAsia. In 1999 the newly recognized Nipah virusspread throughout pig populations in Malaysia,causing more than 100 human deaths there anda smaller number in nearby Singapore.
Latin AmericaLatin American countries are making consider-able progress in infectious disease control,including the eradication of polio and major
reductions in the incidence and death rates ofmeasles, neonatal tetanus, some diarrheal dis-eases, and acute respiratory infections. None-theless, infectious diseases are still a majorcause of illness and death in the region, and therisk of new and reemerging diseases remainssubstantial. Widening income disparities, peri-odic economic shocks, and rampant urbaniza-tion have disrupted disease control efforts andcontributed to widespread reemergence of chol-era, malaria, TB, and dengue, especially in thepoorer Central American and Caribbean coun-tries and in the Amazon basin of SouthAmerica. According to the AFMIC typology,Latin America’s health care capacity is sub-stantially more advanced than that of Sub-Saharan Africa and somewhat better thanmainland Asia’s, with 70 to 90 percent of

30
populations having access to basic health carein Chile, Costa Rica, and Cuba on the upperend of the scale. Less than 50 percent have suchaccess in Haiti, most of Central America, andthe Amazon basin countries, including the ruralpopulations in Brazil.
Cholera reemerged with a vengeance in theregion in 1991 for the first time in a centurywith 400,000 new cases, and while dropping to100,000 cases in 1997, it still comprises two-thirds of the global cholera burden. TB is agrowing problem regionwide, especially inBrazil, Peru, Argentina, and the DominicanRepublic where drug-resistant cases also are onthe rise. Haiti does not provide data but proba-bly also has a high infection rate. HIV/AIDSalso is spreading rapidly, placing Latin Amer-ica third behind Sub-Saharan Africa and Asiain HIV prevalence. Prevalence is high in Braziland especially in the Caribbean countries(except Cuba), where 2 percent of the popula-tion is infected. Malaria is prevalent in theAmazon basin. Dengue reemerged in the regionin 1976, and outbreaks have taken place in thelast few years in most Caribbean countries andparts of South America. Hepatitis B and Cprevalence is greatest in the Amazon basin,Bolivia, and Central America, while denguehemorhagic fever is particularly prevalent inBrazil, Colombia, and Venezuela. Yellow feverhas made a comeback over the last decadethroughout the Amazon basin, and there havebeen several recent outbreaks of gastrointesti-nal disease attributed to E. coli infection inChile and Argentina. Hemorrhagic fevers arepresent in almost all South American countries,and most hantavirus pulmonary syndromeoccurs in the southern cone.
Middle East and North AfricaThe region’s conservative social mores, cli-matic factors, and high levels of health spend-ing in oil-producing states tend to limit some
globally prevalent diseases, such as HIV/AIDSand malaria, but others, such as TB and hepati-tis B and C, are more prevalent. The region’sadvantages are partially offset by the impact ofwar-related uprooting of populations, over-crowded cities with poor refrigeration and sani-tation systems, and a dearth of water, especiallyclean drinking water. Health care capacity var-ies considerably within the region, according tothe AFMIC typology. Israel and the ArabianPeninsula states minus Yemen are in far bettershape than Iraq, Iran, Syria, and most of NorthAfrica. Ninety to 100 percent of the Israelipopulation and 70 to 90 percent of the Saudipopulation have good access to health care.Elsewhere, access ranges from less than 40 per-cent in Yemen to 50 to 70 percent in the smallerGulf states, Jordan and Tunisia, while mostNorth African states fall into the 40- to50-percent category.
The HIV/AIDS impact is far lower than inother regions, with 210,000 cases, or 0.13 per-cent of the population, including 19,000 newcases, in 1998. This owes in part to above-aver-age underreporting because of the stigma asso-ciated with the disease in Muslim societies andthe authoritarian nature of most governments inthe region. TB, including multidrug resistantvarieties, is more problematic, especially inIran, Iraq, Yemen, Libya, and Morocco, with anestimated 140,000 deaths in 1998. Malaria issignificant only in Iran, Iraq, and Yemen, butdiarrheal and childhood diseases caused 0.3million deaths each in 1998. Other prominentor reemerging diseases in the region include alltypes of hepatitis, with Egypt reporting thehighest prevalence worldwide of the C variety.Brucellosis now infects some 90,000 people;leishmaniasis and sandfly fever also areendemic in the region; and various hemorrhagicfevers occur, as well.

31
The Former Soviet Union and EasternEuropeThe sharp decline in health care infrastructurein Russia and elsewhere in the former SovietUnion (FSU) and, to a lesser extent, in EasternEurope—owing to economic difficulties—arecausing a dramatic rise in infectious diseaseincidence. Death rates attributed to infectiousdiseases in the FSU increased 50 percent from1990 to 1996, with TB accounting for a sub-stantial number of such deaths. According tothe AFMIC typology, access to health careranges from 50 to 70 percent in most EuropeanFSU states, including Russia and Ukraine, andfrom 40 to 50 percent in FSU states located inCentral Asia. This is generally supported byWHO estimates indicating that only 50 to 80percent of FSU citizens had regular access toessential drugs in 1997, as compared to morethan 95 percent a decade earlier as health carebudgets and government-provided health ser-vices were slashed. Access to health care isgenerally better in Eastern Europe, particularlyin more developed states such as Poland, theCzech Republic, and Hungary, where it rangesfrom 70 to 90 percent, while only 50 to 70 per-cent have access in countries such as Bulgariaand Romania. More than 95 percent of the pop-ulation throughout the East European regionhad such access in 1987, according to WHO.
Crowded living conditions are among thecauses fueling a TB epidemic in the FSU, espe-cially among prison populations––while surg-ing intravenous drug use and rampantprostitution are substantially responsible for amarked increase in HIV/AIDS incidence. Therewere 111,000 new TB infections in Russiaalone in 1996, a growing number of them mul-tidrug resistant, and nearly 25,000 deaths dueto TB––numbers that could increase signifi-cantly following periodic releases of prisonersto relieve overcrowding. The number of newinfections for the entire FSU in 1996 was
188,000, while East European cases totaled54,000. More recent data indicate that the TBinfection rate in Russia more than tripled from1990 to 1998, with 122,000 new cases reportedin 1998 and the total number of cases expectedto reach 1 million by 2002. After a slow andlate start, HIV/AIDS is spreading rapidlythroughout the European part of the FSUbeyond the original cohort of intravenous drugusers, though it is not yet reflected in officialgovernment reporting. An estimated 270,000people were HIV-positive in 1998, up morethan five-fold from 1997. Although Ukrainehas been hardest hit, Russia, Belarus, andMoldova have registered major increases. Vari-ous senior Russian Health Ministry officialspredict that the HIV-positive population in Rus-sia alone could reach 1 million by the end of2000 and could reach 2 million by 2002. EastEuropean countries will fare better as renewedeconomic growth facilitates recovery of theirhealth care systems and better enables them toexpand preventive and treatment programs.
Diphtheria reached epidemic proportions in theFSU in the first half of the decade, owing tolapses in vaccination. Reported annual casetotals grew from 600 cases in 1989 to morethan 40,000 in 1994 in Russia, with another50,000 to 60,000 in the rest of the FSU. Chol-era and dysentery outbreaks are occurring withincreasing frequency in Russian cities, such asSt. Petersburg and Moscow, and elsewhere inthe FSU, such as in T’bilisi, owing to deterio-rating water treatment and sewerage systems.Hepatitis B and C, spread primarily by intrave-nous drug use and blood transfusions, are onthe rise, especially in the non-European part ofthe FSU. Polio also has reappeared owing tointerruptions in vaccination, with 140 newcases in Russia in 1995.
32
Western EuropeWestern Europe faces threats from a number ofemerging and reemerging infectious diseasessuch as HIV/AIDS, TB, and hepatitis B and C,as well as several zoonotic diseases. Its statusas a hub of international travel, commerce, andimmigration, moreover, dramatically increasesthe risks of importing new diseases from otherregions. Tens of millions of West Europeanstravel to developing countries annually,increasing the prospects for the importation ofdangerous diseases, as demonstrated by theimportation of typhoid in 1999. Some 88 per-cent of regional population growth in the firsthalf of the decade was due to immigration;legal immigrants now comprise about 6 percentof the population, and illegal newcomers num-ber an estimated 6 million. Nonetheless, theregion’s highly developed health care infra-structure and delivery system tend to limit theincidence and especially the death rates of mostinfectious diseases, though not the economiccosts. Access to high-quality care is availablethroughout most of the region, although gov-ernments are beginning to limit some hereto-fore generous health benefits, and a growingantivaccination movement in parts of WesternEurope, such as Germany, is causing a rise inmeasles and other vaccine-preventable dis-eases. The AFMIC typology gives somewhathigher marks to northern over some southernEuropean countries, but the region as a whole isranked in the highest category, along withNorth America.
After increasing sharply for most of the 1980sand 1990s, HIV infections, and particularlyHIV/AIDS deaths, have slowed considerablyowing to behavioral changes among high-riskpopulations and the availability and funding formultidrug treatment. Some 0.5 million peoplewere living with HIV/AIDS in 1998, down
slightly from 510,000 the preceding year, andthere were 30,000 new cases and 12,000deaths, with prevalence somewhat higher inmuch of southern Europe than in the north. TB,especially its multidrug resistant strains, is onthe upswing, as is co-infection with HIV, par-ticularly in the larger countries, with some50,000 TB cases reported in 1996. Hepatitis Cprevalence is growing, especially in southernEurope. Western Europe also continues to suf-fer from several zoonotic diseases, amongwhich is the deadly new variant Creutzfeldt-Jakob disease (nvCJD), linked to the bovinespongiform encephalopathy or “mad cow dis-ease” outbreak in the United Kingdom in 1995that has since ebbed following implementationof strict control measures. Other recent diseaseconcerns include meningococcal meningitisoutbreaks in the Benelux countries andleishmaniasis-HIV co-infection, especially insouthern Europe.
International Response Capacity
International organizations such as WHO andthe World Bank, institutions in several devel-oped countries such as the US CDC, and Non-governmental Organizations (NGOs) willcontinue to play an important role in strength-ening both international and national surveil-lance and response systems for infectiousdiseases. Nonetheless, progress is likely to beslow, and development of an integrated globalsurveillance and response system probably is atleast a decade or more away. This owes to themagnitude of the challenge; inadequate coordi-nation at the international level; and lack offunds, capacity, and, in some cases, coopera-tion and commitment at the national level.
33
Some countries hide or understate their infec-tious disease problems for reasons of interna-tional prestige and fear of economic losses.Total international health-related aid to low-and middle-income countries—some $2-3 bil-lion annually––remains a fraction of the $250billion health bill of these countries.
WHOWHO has the broadest health mandate underthe UN system, including establishing healthpriorities, coordinating global health surveil-lance, and emergency assistance in the event ofdisease outbreaks. Health experts give WHOcredit for major successes, such as the eradica-tion of smallpox, near eradication of polio, andsubstantial progress in controlling childhooddiseases, and in facilitating the expansion ofprimary health care in developing countries. Italso has come under criticism for becoming topheavy, unfocused in its mission, and overlyoptimistic in its health projections. WHOdefenders blame continued member state parsi-mony that has kept WHO’s regular biennialbudget to roughly $850 million for severalyears and forced it to rely more on voluntarycontributions that often come with stringsattached as the cause of its shortcomings.
The election last year of Gro Harlem Bruntlandas Secretary General, along with a series ofreforms, including expansion of the Emergingand other Communicable Diseases Surveillanceand Control (EMC) Division, has placed WHOin a better position to revitalize itself. Internaloversight and transparency have beenexpanded, programs and budgets are undergo-ing closer scrutiny, and management account-ability is looming larger. Bruntland has movedquickly to streamline upper-level managementand has installed new top managers, mostly
from outside the organization, including fromthe private sector. She also is working tostrengthen country offices and to make theregional offices more responsive to centraldirection. WHO is increasing its focus on thefight against resurgent malaria, while a better-funded EMC is expanding efforts to establish aglobal surveillance and response system incooperation with UNAIDS, UNICEF, andnational entities such as the US CDC, the USDoD, and France’s Pasteur Institute.
Other UN Agencies Involved inHealth Care
WHO competes for resources with themany other UN agencies that are increas-ingly involved in health care. The UnitedNations Children’s Fund (UNICEF)focuses on children’s health. The UnitedNations AIDS Program (UNAIDS) focuseson improving the response capacitytoward HIV/AIDS at the country, regional,and global levels in cooperation withWHO and other UN agencies. Other UNagencies involved in health care issuesinclude the UN Development Program(UNDP); the UN Family Planning Agency(UNFPA); the UN High Commissioner forRefugees (UNHCR); the UN Educational,Scientific and Cultural Organization(UNESCO); the International LaborOrganization (ILO); the Food and Agri-cultural Organization (FAO); and theWorld Food Program (WFP).

34
The World BankThe growing sense that health is linked inexo-rably to socioeconomic development, hasprompted the World Bank to expand its healthactivities. According to a 1997 study by the USInstitute of Medicine, the most significantchange in the global health arena over the pastdecade has been the growth in both financialand intellectual influence of the World Bank,whose health loans have grown to $2.5 billionannually, including $800 million for infectiousdiseases. Health experts generally welcome theBank’s greater involvement in the health sector,viewing it as efficient and responsive in areassuch as health sector financial reform. Someremain concerned that the Bank’s emphasis onfiscal balance can sometimes have a negativehealth and social impact in developing coun-tries. Some developing countries resent whatthey perceive as the domination of Bank deci-sionmaking and priority setting by the richercountries.
Nongovernmental OrganizationsAnother major change in the global healtharena over the last decade is the increasinglyimportant role of NGOs, which provide directassistance, including emergency shelter andaid, as well as long-term domestic health caredelivery. NGOs also build community aware-ness and support for WHO and other interna-tional and bilateral surveillance and responseefforts. At the same time, health experts notethat NGOs, like their governmental counter-parts, are driven in part by their own self inter-ests, which sometimes conflict with those ofhost and donor governments.
Bilateral AssistanceThe United States, through USAID, the CDC,the National Institutes for Health (NIH), and the
Defense Department’s overseas laboratories, isa major contributor to international efforts tocombat infectious diseases. It is joined increas-ingly by other developed nations and regionalgroupings, such as the European Union (EU),that provide assistance bilaterally, as well asthrough international organizations and NGOs.The Field Epidemiology Training Programs––run jointly by the CDC and WHO—as well asthe EU-US Task Force on Emerging Diseasesand the US-Japan Common Scientific Agenda,are key examples of developed-country pro-grams focusing on infectious diseases.
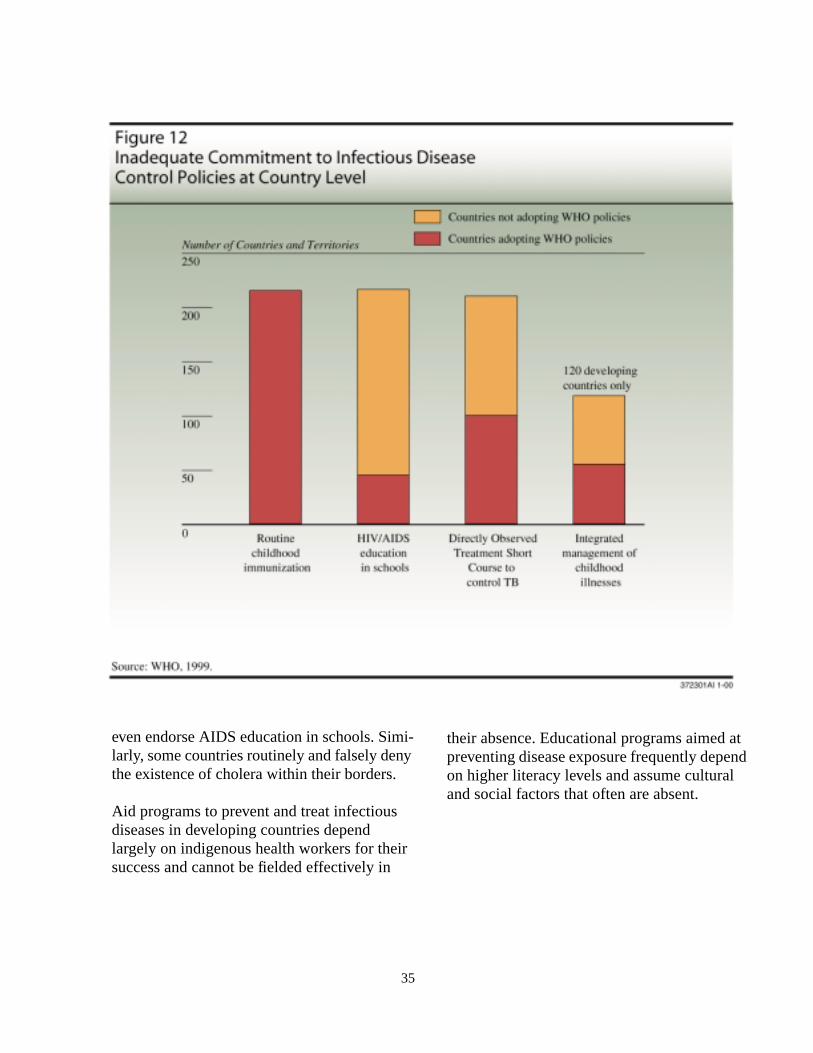
National LimitationsA major obstacle to effective global surveil-lance and control of infectious diseases willcontinue to be poor or inaccurate nationalhealth statistical reporting by many developingcountries and lack of both capacity and will toproperly direct aid (see figure 12) and to followWHO and other recommended health carepractices. Those areas of the world most sus-ceptible to infectious disease problems are leastable to develop and maintain the sophisticatedand costly communications equipment neededfor effective disease surveillance and reporting.In addition to the barriers dictated by low levelsof development, revealing an outbreak of adreaded disease may harm national prestige,commerce, and tourism. For example, nearlyevery country initially denied or minimized theextent of the HIV/AIDS virus within its bor-ders, and even today, some countries known tohave significant rates of HIV infection refuse tocooperate with WHO, which can only publishthe information submitted by surveyingnations. Only a few, such as Uganda, Senegal,and Thailand, have launched major preventa-tive efforts, while many WHO members do not
35
even endorse AIDS education in schools. Simi-larly, some countries routinely and falsely denythe existence of cholera within their borders.
Aid programs to prevent and treat infectiousdiseases in developing countries dependlargely on indigenous health workers for theirsuccess and cannot be fielded effectively in
their absence. Educational programs aimed atpreventing disease exposure frequently dependon higher literacy levels and assume culturaland social factors that often are absent.

36
Alternative Scenarios and Outlook forInfectious Diseases
The impact of infectious diseases over the next20 years will be heavily influenced by three setsof variables. The first is the relationshipbetween increasing microbial resistance andscientific efforts to develop new antibiotics andvaccines. The second is the trajectory of devel-oping and transitional economies, especiallyconcerning the basic quality of life of the poor-est groups in these countries. The third is thedegree of success of global and national effortsto create effective systems of surveillance andresponse. The interplay of these drivers willdetermine the overall outlook.
On the positive side, reduced fertility and theaging of the population, continued economicdevelopment, and improved health care capac-ity in many countries, especially the moredeveloped, will increase the progress toward ahealth transition by 2020 whereby the impactof infectious diseases ebbs, as compared tononinfectious diseases. On the negative side,continued rapid population growth, urbaniza-tion, and persistent poverty in much of thedeveloping world, and the paradox in whichsome aspects of socioeconomic development––such as increased trade and travel––actuallyfoster the spread of infectious diseases, couldslow or derail that transition. So, too, willgrowing microbial resistance among resurgentdiseases, such as malaria and TB, and the pro-liferation or intensification of new ones, such asHIV/AIDS.
Two scenarios—one optimistic and one pessi-mistic—reflect differences in the internationalhealth community concerning the global
outlook for infectious diseases. We present andcritically assess these scenarios, elaborate onthe pessimistic scenario, and develop a third,combining some elements of each, that wejudge as more likely to prevail over the periodof this Estimate.
The Optimistic Scenario: Steady ProgressAccording to a key 1996 World Bank/WHOstudy cited earlier that articulated the optimisticscenario, a health transition––resulting fromkey drivers, such as aging populations, socio-economic development, and medicaladvances—already is under way in developedcountries and also in much of Asia and LatinAmerica that is likely to produce a dramaticreduction in the infectious disease threat. Thestudy projects that deaths caused primarily byinfectious diseases will fall steadily from 34percent of the total disease burden in 1990 to15 percent in 2020. Those from noninfectiousdiseases are likely to climb from 55 percent ofthe total disease burden to 73 percent, with theremainder of deaths due to accidents and othertypes of injuries. According to the study’s rank-ing of major disease threats over this 30-yeartime frame, noninfectious diseases generallywill rise in importance, led by heart disease andmental illness, as will accidental injuries. TBwill remain in 7th place in 2020, and HIV/AIDS will move from 28th place to 10th, withthe two combined accounting for more than 90percent of infectious disease-caused deathsamong adults, almost all of them in developingcountries. Lower respiratory infections will fallfrom the top spot to sixth place, however, while

37
measles and malaria will drop precipitouslyfrom 8th and 11th place to 24th and 25th,respectively (see figures 13 and 14).
Aging Populations. Demographic changes areone key to this scenario, which projects thatdeclining fertility and infant mortality, alongwith increased life expectancy, will result in anaging global population more apt to be felledby noninfectious diseases and by accidental
injury than by infectious diseases, which tendto occur among the very young. While thesetrends are generally evident on a global scale,there is considerable variance by region andlevel of development. Fertility has been cut bya half over the last 50 years in most regions ofthe world, infant mortality worldwide droppedfrom 129 to 60 per 1,000 live births from 1960to 1996, and life expectancy worldwideincreased from 50 to 64 years, according to the
Toward a Global Surveillance andResponse System
Although a formal, fully integrated surveil-lance and response system does not yet existat the global level, the WHO’s Emerging andother Communicable Diseases Surveillanceand Control (EMC) Division, working withUNAIDS and more than 200 collaboratingcenters and laboratories, is making someprogress.
• Independent networks of laboratories mon-itoring specific diseases and the microbialresistance phenomenon are beingexpanded or established, while networksfor reporting and exchanging informationabout infectious disease outbreaks arebeing enhanced. These networks includeone on influenza encompassing more than100 worldwide laboratories; a network forHIV/AIDS and other sexually transmitteddiseases; several new or smaller networksfocusing on hepatitis C and yellow fever;and one on microbial resistance in general.The EMC has taken the lead in revising
international health reporting requirementsto encompass a broader array of diseases.
• Member states’ capacities to monitorinfectious diseases are being enhanced byincreasing the number of developing coun-try health professionals capable of moni-toring and responding to diseaseoutbreaks.
• Global infectious disease control effortsare being improved by better assistingcountries to deal with disease outbreaks,such as ensuring that trained experts, vac-cines, and therapeutics are available todeal with such outbreaks.
• The global exchange of information amongand within surveillance networks is beingimproved by expanding the availability ofequipment for electronic communicationthrough the Internet and World Wide Websites, such as PROMED.

38
1998 UN Human Development Report. Theoverall population growth rate, meanwhile, willslow to 1.2 percent annually by 2015, as com-pared to 1.7 percent between 1970 and 1995.
Socioeconomic Progress. Under this scenario,continued improved access to safe food andwater in developing countries, better nutrition,and improved literacy will sharply reduceinfant and adult mortality, already cut by morethan half in developing countries since 1965.The number of people with an average per cap-ita caloric intake of 2,700 per day is projectedto increase from 1.8 billion in 1990-92 to 2.7billion by 2010—or roughly 50 percent––andadult literacy in the least developed countries isexpected to grow from 49 percent in 1995 to 61percent in 2010. All of these factors would thusproduce better health and health practices foryoung and old alike.
Economic Gains. The optimistic scenarioassumes that worldwide economic growth andrising incomes will further reduce poverty andprovide funding for improvements in healthcare infrastructure, though it will be uneven inscope and by region. Real per capita incomelevels from 1970 to 1995, for example,increased by 200 percent in east Asia, 60 per-cent in south Asia, and 25 to 50 percent in LatinAmerica.
Improved Health Care Capacity. Improve-ments in health care delivery in accordancewith WHO’s “health for all” goal are projectedto continue in such areas as prenatal care forwomen, contraception, childhood and adultimmunization, and availability of essentialdrugs. Already more than 90 percent of womenin developed and transitional countries and 50percent in the least developed countries receivesome prenatal care. The number of women indeveloping countries using contraceptives
increased from 9 percent in 1965 to 60 percentin 1998. Immunization rates against six com-mon vaccine-preventable diseases haveincreased from 5 percent to 80 percent of therelevant population over the last two decades.
aOf the six infectious diseases ranked in 1990, only lower res-piratory infections, diarrheal diseases, and measles are trendingdownward as projected, while malaria is increasing and tuber-culosis and HIV are growing far faster than projected. Nonethe-less, more pessimistic experts have not developed an alternativemodel and generally adopt the projections of the Murray andLopez model.
Source: Adapted from World Bank, WHO, 1996, edited byChristopher J. L. Murray and Alan D. Lopez.
Table 4Projected Change in the Rank Order of GlobalDisease Burden for Leading Causes, Worldwide1990-2020, According to the OptimisticScenarioa
1990Rank Order
Disease or Injury 2020Rank Order
1 Lower respiratory infections 62 Diarrheal diseases 93 Conditions arising during
perinatal period11
4 Unipolar major depression 25 Ischemic heart disease 16 Cerebrovascular disease 47 Tuberculosis 78 Measles 259 Road traffic deaths 3
10 Congenital abnormalities 1311 Malaria 2412 Chronic obstructive
pulmonary disease5
13 Falls 1914 Iron-deficiency anemia 3915 Protein-energy malnutrition 3716 War 817 Self-inflicted injuries 1419 Violence 1228 HIV 1033 Trachea, bronchus, and
lung cancers15

39
And access to drugs continues to expand,except in the former communist states in East-ern Europe and in the former Soviet Union. Allof these factors will combine to reduce child-hood diseases and mortality.
Medical Advances. The optimistic scenarioalso notes that several diseases are on the vergeof elimination or close to it, such as polio, neo-natal tetanus, and leprosy, while measles inci-dence also will be reduced dramatically asvaccination rates increase in the least devel-oped countries. Research efforts are projectedto result in the development of more effective,safer, and in some cases, less expensive vac-cines. Disease agents against which vaccineshave been developed recently include Lymedisease, while several others––such as formalaria, dengue fever, and Ebola––are in vari-ous stages of development. As the humangenetic code is deciphered, additional genesthat influence infectious disease risk are likelyto be discovered.
Scenario Assessment. Our overall judgment isthat the “steady progress” scenario is veryunlikely to transpire over the time period of thisEstimate. Although the scenario captures somereal trends, it overstates the progress achiev-able, while underestimating the risks.
• The global life expectancy increases pro-jected by the optimists are likely to be sub-stantially offset by HIV/AIDS and relateddiseases, such as TB, which are already caus-ing a major reduction in life expectancy in themost heavily affected Sub-Saharan Africancountries and will be spreading extensivelythroughout heavily populated Asia during thetime period of the Estimate. Optimistsacknowledge that HIV/AIDS and TB will be
the overarching infectious disease threats by2020, but they understate the magnitude ofthat threat, while their projections of a steepdecline in malaria deaths is belied by the dis-ease’s resurgence and growing death toll.
• The picture of steady socioeconomic progressis not consistent with the most recent surveysof conditions in developing countries under-taken by the United Nations, the World Bank,and other international agencies. These stud-ies point to a slowing of progress in basicsocial indicators in much of the developingworld, even before the recent global financialcrisis.
• Although we judge that economic growth islikely to continue, we are less confident thatthe dramatic reductions in poverty achievedin many countries in the last generation willbe sustained. Growth is likely to be halting inmany countries, owing to structural economicproblems and the impact of recurring devel-oping world economic crises.
• The rapidly expanding costs of many drugs,especially those that attack critical infectiousdiseases, such as HIV/AIDS and multidrugresistant TB and malaria, threaten to limit thesustainability of improved health care. Fur-thermore, despite economic growth, pres-sures on government budgets, especially fromrising pension and other costs, may limit theprospects for increased health financing.
• The optimists may place too much emphasison the steady progress of science, which isinconsistent with the demonstrated difficultyof developing new drugs and vaccines forcomplex pathogens such as HIV and malaria.

40

41

42
The Pessimistic Scenario: Progress StymiedSurprisingly, even the most pessimistic epide-miologists have done little to project the long-term implications of their analysis and simplyadopt the longer term projections of the WorldBank/WHO model in the absence of a worstcase model. We have developed a worst casescenario culled from a variety of epidemiologi-cal and broader health studies. This scenariohighlights the dangers posed by microbialresistance among reemergent diseases such asTB and malaria. It takes a more concerned viewof new diseases and of the HIV/AIDS pan-demic, in particular, and is skeptical about theadequacy of world health care capacity to con-front these challenges. It emphasizes continu-ing and difficult-to-address poverty challengesin developing countries and projects an incom-plete health transition that prolongs the heavyinfectious disease burden in the least developedcountries and sustains their role as reservoirs ofinfection for the rest of the world.
A Not-So-Benign Demographic Picture.Although the global population growth rate isslowing, world population still will expand by80 million annually through 2015, mostly indeveloping countries, where especially theyoungest population cohorts will remain highlysusceptible to infectious diseases. Infant mor-tality in the least developed countries is runningat nearly double the global average and is eighttimes that of developed countries, while lifeexpectancy is 23 years below that of developedcountries and 13 years below the global aver-age. These trends will be especially evident inurban areas where poverty, overcrowding, poorsanitation, and polluted drinking water createconditions in which infectious diseases andrelevant vectors, such as mosquitoes androdents, thrive. The problem will only worsenwhen the number of people living in cities
exceeding 10 million more than doubles to 450million by 2015, with almost all of the increaseoccurring in developing world cities.
Disparate Socioeconomic Development.Although the broad long-term trend in globaleconomic growth is likely to be upward, thisscenario posits a growing prosperity gapbetween the developed and developing coun-tries and within developing countries, particu-larly the poorest cohort. Despite the neardoubling of real per capita income from 1970to 1995 globally, for example, it declined inSub-Saharan Africa, and income gaps withinthese countries are widening substantially, aswell. One-fifth of developing country popula-tions remain malnourished––the biggest riskfactor for infectious diseases––3 billion lackadequate sanitation, and 1 billion still have noaccess to safe drinking water. Recurring eco-nomic crises in developing countries, more-over, are likely to have a negative impact onforeign and domestic investor willingness toinvest in them, slowing their economic growthrates further and widening the gap with devel-oped countries.
Inadequate Health Care Delivery and DiseaseSurveillance. Tightening of health care eligi-bility requirements, privatization, and the grow-ing costs of health care, particularly for HIV/AIDS patients, are likely to continue to squeezehealth care delivery worldwide, but the impactwill be greatest in Sub-Saharan Africa as wellas in China––where 80 percent of the rural pop-ulation no longer has subsidized health care––and in the former communist states. Under thisscenario access to essential drugs and basicmedical care in these regions will remain pooror deteriorate, and many Sub-Saharan Africancountries, in particular, will continue to relyon international and NGO assistance for a

43
modicum of health care and surveillance capa-bility. Although current global surveillance andresponse capabilities are likely to improve, theemergence of an integrated global network is atleast a decade or more away, owing to inade-quate capacity and cooperation and resourceconstraints.
Toward a Postantibiotic Era? The growth andintensity of antimicrobial resistance amonginfectious pathogens increases, due both topathogen mutation and to inappropriate andindiscriminate use of therapeutic drugs in bothdeveloped and developing countries. Two-thirds of all oral antibiotics worldwide areobtained without a prescription and are inap-propriately used against diseases such as TB,malaria, pneumonia, and more routine child-hood infections. These practices contribute toantimicrobial resistance and the severe, nearlyimpossible to treat hospital-acquired infections.Even vancomycin, the last defense against anumber of such infections, is losing effective-ness. According to WHO, “In the struggle forsupremacy, the microbes are sprinting aheadand the gap between their ability to mutate intoresistant strains and man’s ability to counterthem is widening fast.” Some epidemiologistsand health experts have even suggested that wemay be entering a postantibiotic era in whichexisting antimicrobials, in general, will losetheir effectiveness against the most commoninfectious diseases.
Inadequate Drug and Vaccine Development.The development of new antimicrobial drugsand vaccines does not keep pace with new andresistant pathogens owing to the complexity ofpathogens such as HIV and malaria, the slowpace of new antimicrobial development andapproval, and in many cases a lack of commer-cial incentives for drug companies to developnew antibiotics for diseases prevalent in devel-oping countries. Most recent efforts to develop
new or more effective drugs and vaccinesagainst dengue, malaria, E. coli, TB, and sev-eral other infectious diseases are likely to beprolonged. WHO estimates that development ofan effective vaccine against malaria, for exam-ple, is at least seven to 15 years away, while acure for HIV/AIDS is likely to be even moredistant. The majority of new drugs and vac-cines, moreover, are likely to be beyond thereach of most developing country populationsbecause of their cost.
Continued Threat From HIV/AIDS. Thethreat from HIV/AIDS and related diseasesover the next two decades continues to surge.Although behavioral changes and multidrugtreatments will slow infection and death rates indeveloped countries, these advances are likelyto be more than offset by the rapid spread of thedisease among the vast populations of India,Russia, China, and Latin America. HIV/AIDSburden projections since the start of the pan-demic have consistently been surpassed, whilethe slow pace of behavioral changes in thedeveloping world, high costs of available treat-ment, and the obstacles to developing a cureportend more increases in the future. The 1996joint World Bank/WHO model’s projectionsthat HIV/AIDS deaths would peak in 2006 with1.7 million deaths, for example, were alreadyexceeded by the 2.3 million deaths in1998. Twoother models likewise have underestimated theHIV/AIDS threat, albeit less so. Similarly, theWorld Bank/WHO model’s baseline projectionof roughly 2.2 million TB deaths in 2020 islikely to be exceeded in the next decade, asmay its worst case scenario of 3.2 milliondeaths if HIV co-infection surges. According toUNAIDS epidemiologists, Asia alone is likelyto outstrip Sub-Saharan Africa in the absolutenumber of HIV carriers by 2010. When cou-pled with the poor prospects for developing acure and likely growing resistance to the

44
multidrug therapies now in use, the HIV/AIDSburden could reach catastrophic proportionsover the next 20 years (see figure 14).
The “Infectiousness” of Noninfectious Dis-eases. Prospects that the infectious diseasethreat may not diminish, as compared to non-communicable diseases, are further butressedby the growing body of evidence that infectiouspathogens cause or contribute to many dis-eases––such as diabetes, cancer, heart disease,and ulcers––previously thought to be caused byenvironmental or lifestyle factors. WHO andother institutions estimate that up to 15 percentof cancers, for example, could be avoided bypreventing the infectious diseases associatedwith them, including more than 50 percent ofstomach and cervical cancers and 80 percent ofliver cancers.
Scenario Assessment. Our overall judgment isthat the “progress stymied” scenario, whilemore plausible than the optimistic scenario, isalso unlikely to develop over the period of thisEstimate. Although the pessimistic scenarioprovides an important counterpoint to theassumptions in the “steady progress” scenario,it understates the likely longer term impact ofeconomic development, scientific progress, andpolitical pressures in responding to the infec-tious disease threat.
• The demographic projections understate thelikely impact of continued progress in reduc-ing infant mortality.
• Improvements in the economic conditions ofpoor countries and the poorest within coun-tries are probably more important for theinfectious disease outlook than the widening“prosperity gap” both between countries andwithin countries. Although the outlook forSub-Saharan Africa remains bleak, for therest of the world progress against infectious
diseases would stall only under the most direglobal economic scenario.
• The negative impact on health care deliveryof privatization and the transitions in formercommunist states is likely to be most heavilyfelt in the immediate future. Free marketreforms eventually will improve health caredelivery.
• The current success of the “mutatingmicrobes” in the race against scientific inno-vation will, in and of itself, call forth a greaterresearch effort that will, over time, increasethe likelihood of a reversal of this trend.
• The rapid spread of HIV/AIDS in developingand former communist countries is likely toreinvigorate international efforts to addressthe virus through both medical and behav-ioral approaches. It will especially give impe-tus to the search for a more cost-effectiveapproach than at present.
• While growth in surveillance and responsecapabilities are slow, they are real and areunlikely to be reversed.
The Most Likely Scenario: Deterioration,Then Limited ImprovementAccording to this scenario, continued deteriora-tion during the first half of our time frame—ledby hard core killers such as HIV/AIDS, TB,and malaria—is followed by limited improve-ment in the second half, owing primarily togains against childhood and vaccine-prevent-able diseases such as diarrheal diseases, neona-tal tetanus, and measles. The scale and scope ofthe overall infectious disease threat diminishes,but the remaining threat consists of especiallydeadly or incurable diseases such as HIV/AIDS, TB, hepatitis C and possibly, heretofore,unknown diseases, with HIV/AIDS and TB
45
likely comprising the overwhelming majorityof infectious disease deaths in developingcountries alone by 2020.
Scenario AssessmentBecause some elements of both the optimisticand pessimistic scenarios cited above are likelyto appear during the 20-year time frame of thisEstimate, we are likely to witness neithersteady progress against the infectious diseasethreat nor its unabated intensification. Instead,progress is likely to be slow and uneven, withadvances, such as the recent development of anew type of antibiotic drug against certain hos-pital-acquired infections, frequently offset byrenewed setbacks, such as new signs of grow-ing microbial resistance among available HIV/AIDS drugs and withdrawal of a promisingnew vaccine against rotavirus because ofadverse side effects. On balance, negative driv-ers, such as microbial resistance, are likely toprevail over the next decade, but given time,positive ones, such as gradual socioeconomicdevelopment and improved health care capac-ity, will likely come to the fore in the seconddecade.
• The negative trends cited in the pessimisticscenario above, such as persistent poverty inmuch of the developing world, growingmicrobial resistance and a dearth of newreplacement drugs, inadequate disease sur-veillance and control capacity, and the highprevalence and continued spread of majorkillers such as HIV/AIDS, TB, and malaria,are likely to remain ascendant and worsen theoverall problem during the first half of ourtime frame.
• Sub-Saharan Africa, India, and SoutheastAsia will remain the hardest hit by these dis-eases. The European FSU states and Chinaare likely to experience a surge in HIV/AIDSand related diseases such as TB. The devel-oped countries will be threatened principally
by the real possibility of a resurgence of theHIV/AIDS threat owing to growing microbialresistance to the current spectrum of multi-drug therapies and to a wide array of otherdrugs used to combat infectious diseases.
The broadly positive trends cited in the moreoptimistic scenario, such as aging populations,global socioeconomic development, improvedhealth care capacity, and medical advances, arelikely to come to the fore during the secondhalf of our time frame in all but the least devel-oped countries, and even the least developedwill experience a measure of improvement.
• Aging populations and expected continueddeclines in fertility throughout Asia, LatinAmerica, the former FSU states, and Sub-Saharan Africa will sharply reduce the size ofage cohorts that are particularly susceptible toinfectious diseases owing to environmental orbehavioral factors.
• Socioeconomic development, however fitful,and resulting improvements in water quality,sanitation, nutrition, and education in mostdeveloping countries will enable the mostsusceptible population cohorts to better with-stand infectious diseases both physically andbehaviorally.
• The worsening infectious disease threat weposit for the first decade of our time frame islikely to further energize the internationalcommunity and most countries to devotemore attention and resources to improvedinfectious disease surveillance, response, andcontrol capacity. The WHO’s new campaignagainst malaria, recent developed countryconsideration of tying debt forgiveness forthe poorest countries in part to their undertak-ing stronger commitments to combat disease,self-initiated efforts by Sub-Saharan Africangovernments to confront HIV/AIDS, and

46
greater pharmaceutical industry willingnessto provide more drugs to poor countries ataffordable prices are likely to be harbingersof more such efforts as the infectious diseasethreat becomes more acute.
• The likely eventual approval of new drugsand vaccines—now in the developmentalstage—for major killers such as dengue, diar-rheal diseases, and possibly even malaria willfurther ease the infectious disease burden andhelp counter the microbial resistance phe-nomenon.
Together, these developments are likely to setthe stage for at least a limited improvement ininfectious disease control, particularly againstchildhood and vaccine-preventable diseases,such as respiratory infections, diarrheal dis-eases, neonatal tetanus, and measles in mostdeveloping and former communist countries.Given time––and barring the appearance of adeadly and highly infectious new disease, a cat-astrophic expansion of the HIV/AIDS pan-demic, or the release of a highly contagiousbiological agent capable of rapid and widescalesecondary spread—such medical advances,behavioral changes, and improving nationaland international surveillance and responsecapacities will eventually produce substantialgains against the overall infectious diseasethreat. In the event that HIV/AIDS takes a cata-strophic turn for the worse in both developedand developing countries, even the authors ofthe optimistic World Bank/WHO model concurthat all bets are off.
Economic, Social, and Political Impacts
The persistent infectious disease burden islikely to aggravate and, in extreme cases, mayeven provoke social fragmentation, economic
decay, and political polarization in the hardesthit countries in the developing and former com-munist worlds in particular, especially in theworst case scenario outlined above. This, inturn, will hamper progress against infectiousdiseases. Even under the most likely scenariothat posits some attenuation of the infectiousdisease threat in the second half of our timeframe, new and reemergent infectious diseasesare likely to have a disruptive impact on globaleconomic, social, and political dynamics.
Economic Impact Likely To GrowMacroeconomic ImpactThe macroeconomic costs of the infectious dis-ease burden are increasingly significant for themost seriously affected countries despite thepartially offsetting impact of declines in popu-lation growth, and they will take an evengreater toll on productivity, profitability, andforeign investment in the future. A seniorWorld Bank official considers AIDS to be thesingle biggest threat to economic developmentin Sub-Saharan Africa. A growing number ofstudies suggest that AIDS and malaria alonewill reduce GDP in several Sub-Saharan Afri-can countries by 20 percent or more by 2010.
• The impact of infectious diseases on annualGDP growth in heavily affected countriesalready amounts to as much as a 1-percentagepoint reduction in the case of HIV/AIDS onaverage and 1 to 2 percentage points formalaria, according to World Bank studies. Arecent Namibian study concluded that AIDScost the country nearly 8 percent of GDP in1996, while a study of Kenya projected thatGDP will be 14.5 percent smaller in 2005than it otherwise would have been without thecumulative impact of AIDS. The annual costof malaria to Kenya’s GDP was estimated at 2to 6 percent and at 1 to 5 percent for Nigeria.

47
Microeconomic ImpactThe impact of infectious diseases—especiallyHIV/AIDS––at the sector and firm levelalready appears to be substantial and growingand will be reflected eventually in higher GDPlosses (see figure 15), especially in the moreadvanced developing countries with specializedwork force needs.
• A recent study by the Zimbabwe CommercialFarmers’ Union estimated that productionlosses due to HIV/AIDS in the communal andresettlement areas—the African farm-holdersector—is close to 50 percent.
• WHO estimates that small farmers in Nigeriaand Kenya spend 13 and 5 percent, respec-tively, of total household income on malariatreatment that would otherwise go to otherforms of consumption of more benefit to theeconomy.
Although a 1996 World Bank–sponsored studyof nearly 1,000 firms in four African countriesfocusing solely on the impact of AIDS-relatedemployee turnover concluded that it was notlikely to substantially affect firm profits, sev-eral individual firms and their AIDS consult-ants paint a much bleaker picture by 1999.Using broader measures of AIDS-related costs,such as absenteeism, productivity declines,health and insurance payments, and recruit-ment and training, they projected profits todrop by 6 to 8 percent or more and productiv-ity to decline by 5 percent. They are especiallytroubled by the high rate of loss of middle- andupper-level managers to AIDS and the dearthof replacements, as well as the loss of largenumbers of skilled workers to AIDS in themining and other key sectors. According toone expert, South African companies willbegin to feel the full impact of the AIDS epi-demic by 2005. One study of the projectedimpact of AIDS on employee benefit costs in
South Africa concludes that benefit costswould nearly triple to 19 percent of salariesfrom 1995 to 2005, substantially eroding cor-porate profits.
Fiscal Impact. Infectious diseases will increasepressure on national health bills that alreadyconsume some 7 to 14 percent of GDP in devel-oped countries, up to 5 percent in the better offdeveloping countries, but currently less than2 percent in least developed states.
• By 2000, the cumulative direct and indirectcosts of AIDS alone are likely to have topped

48
$500 billion, according to estimates by theGlobal AIDS Policy Coalition at HarvardUniversity. In Latin America, the Pan-Ameri-can Health Organization in 1994 estimated itwould take a decade and $200 billion to bringthe cholera pandemic in the region under con-trol through a massive water cleanup effort,or nearly 80 percent of total developing
country health spending for that year. Thedirect costs of fighting malaria in Sub-Saharan Africa increased from $800 millionin 1989 to $2.2 billion in 1997, largely owingto the far higher cost of treating the growingnumber of drug-resistant cases, and the trendtoward higher costs is likely to continue.
Infectious Disease-Related TradeDisruptions
Infectious diseases will continue to causecostly periodic disruptions in trade and com-merce in every region of the world.
• Avian flu in Hong Kong. The avian influ-enza outbreak in 1997 cost the former col-ony hundreds of millions of dollars in lostpoultry production, commerce, and tour-ism, with airport arrivals in November ofthat year alone down by 22 percent fromthe preceding year.
• BSE and nvCJD in Britain. The outbreakof BSE and new variant Creutzfeldt-Jakobdisease in the United Kingdom in 1995prompted a mass slaughter of cattle, drasti-cally cut beef consumption, and led to theimposition of a three-year EU embargoagainst British beef. The losses to the Brit-ish economy were estimated by the WHO at$5.75 billion, including $2 billion in lostbeef exports.
• Cyclospora in Guatemalan raspberries.The outbreak of cyclospora-related illnessin the United States and Canada associ-ated with raspberries from Guatemala ledto curbs in imports that cost Guatemalaseveral million dollars in lost revenue.
• Cholera in Peru. The outbreak of cholerain 1991 cost the Peruvian fishing industryan estimated $775 million in lost tourismand trade because of a temporary ban onseafood exports.
• Foot and mouth disease in Taiwan. In1997 an outbreak of foot and mouth dis-ease (FMD) devastated Taiwan’s porkindustry—one of the largest in the world––shutting down exports for a full year.
• Nipah in Malaysia. In 1999, the Nipahvirus caused the shutdown of over half ofthe country’s pig farms and an embargoagainst pork exports.
• Plague in India. The plague outbreak inSurat, India, in 1994 and ensuing panicsparked a sudden exodus of 0.5 millionpeople from the region and led to abruptshutdowns of entire industries, includingaviation, and tourism, as several countriesfroze trade, banned travel from India, andsent some Indian migrants home. TheWHO estimated the outbreak cost Indiasome $2 billion.

49
AIDS, along with TB and malaria—particu-larly the drug-resistant varieties––makes largebudgetary claims on national health systems’resources (see figure 16). Policy choices willcontinue to be required along at least threedimensions: spending for health versus spend-ing for other objectives; spending more on pre-vention in order to spend less on treatment; andtreating burgeoning AIDS-infected popula-tions versus treating other illnesses.
• Although prevention is cost-efficient––theeradication of smallpox has shaved $20 bil-lion off the global health bill, and polio eradi-cation would save as much as $3 billionannually by 2015––most countries will not beable to afford even basic care for thoseinfected with diseases such as TB and HIV/AIDS. In Zimbabwe, for example, more thanhalf the meager health budget is spent ontreating AIDS. Yet, treating one AIDS patientfor a year in Sub-Saharan Africa costs asmuch as educating 10 primary school stu-dents for one year.
• Public health spending on AIDS and relateddiseases threatens to crowd out other types ofhealth care and social spending. In India, forexample, simulated annual governmenthealth expenditures in the context of a severeAIDS epidemic in which total expenditures,including AIDS costs, are subsidized at21 percent would add $2 billion annually tothe government’s health bill through 2010and $5 billion with a government subsidy of51 percent. In Kenya, HIV/AIDS treatmentcosts are projected to account for 50 percentof health spending by 2005. In South Africa,such costs could account for 35 to 84 percentof public health expenditures by 2005,according to one projection.
• Even given the budgetary dominance ofAIDS, care is likely to be limited to the mostbasic of therapies. Few countries will be ableto afford the high cost of multidrug treatmentfor HIV/AIDS—or for drug-resistant TB andmalaria—ensuring that such diseases willcontinue to be highly prevalent. Only about1 percent of HIV/AIDS patients even in rela-tively well off South Africa currently undergomultidrug treatment, for example, while itwould cost Russia several billion dollarsannually to provide such treatment for its

50
surging HIV/AIDS case load—which isunlikely given its fiscal difficulties. In addi-tion to the cost of the drugs, few countries canafford to build and maintain the health careinfrastructure that makes effective treatmentpossible.
Disruptive Social ImpactAt least some of the hardest-hit countries, ini-tially in Sub-Saharan Africa and later in otherregions, will face a demographic catastrophe asHIV/AIDS and associated diseases reducehuman life expectancy dramatically and kill upto a quarter of their populations over the periodof this Estimate (see table 5). This will furtherimpoverish the poor and often the middle classand produce a huge and impoverished orphancohort unable to cope and vulnerable to exploi-tation and radicalization.
Life Expectancy and Population Growth.Until the early 1990s, economic developmentand improved health care had raised the lifeexpectancy in developing countries to 64 years,with prospects that it would go higher still. Thegrowing number of deaths from new andreemergent diseases such as AIDS, however,will slow or reverse this trend toward longerlife spans in heavily affected countries by asmuch as 30 years or more by 2010, accordingto the US Census Bureau. For example, lifeexpectancy will be reduced by 30 years inBotswana and Zimbabwe, by 20 years in Nige-ria and South Africa, by 13 years in Honduras,by eight years in Brazil, by four years in Haiti,and by three years in Thailand.
Family Structure. The degradation of nuclearand extended families across all classes willproduce severe social and economic disloca-tions with political consequences, as well.Nearly 35 million children in 27 countries willhave lost one or both parents to AIDS by 2000;
by 2010, this number will increase to 41.6 mil-lion. Nineteen of the hardest hit countries are inSub-Saharan Africa, where HIV/AIDS hasbeen prevalent across all social sectors. Chil-dren are increasingly acquiring HIV from theirmothers during pregnancy or through breast-feeding, ensuring prolongation and intensifica-tion of the epidemic and its economic reverber-ations. With as much as a third of the childrenunder 15 in hardest-hit countries expected tocomprise a “lost orphaned generation” by 2010with little hope of educational or employmentopportunities, these countries will be at risk offurther economic decay, increased crime, andpolitical instability as such young peoplebecome radicalized or are exploited by variouspolitical groups for their own ends; the perva-sive child soldier phenomenon may be oneexample.
Destabilizing Political and Security ImpactIn our view, the infectious disease burden willadd to political instability and slow democraticdevelopment in Sub-Saharan Africa, parts ofAsia, and the former Soviet Union, while alsoincreasing political tensions in and amongsome developed countries.
• The severe social and economic impact ofinfectious diseases, particularly HIV/AIDS,and the infiltration of these diseases into theruling political and military elites and middleclasses of developing countries are likely tointensify the struggle for political power tocontrol scarce state resources. This will ham-per the development of a civil society andother underpinnings of democracy and willincrease pressure on democratic transitions inregions such as the FSU and Sub-SaharanAfrica where the infectious disease burdenwill add to economic misery and politicalpolarization.

51
• A study by Ted Robert Gurr, et al., on thecauses of state instability in 127 cases over a40-year period ending in 1996 suggests thatinfant mortality is a good indicator of theoverall quality of life, which correlates
strongly with political instability. Accordingto the research, three variables out of 75––high infant mortality—which in developingcountries owes substantially to infectious dis-eases; low openness to trade; and incomplete
Source: Adapted from United States Bureau of the Census, 1998.
Table 5Projected Demographic Indicators for 2010 in Selected CountriesWith and Without AIDS
Country Projected Child Mortalitya
Per 1,000 Live Births, 2010
a. Probable deaths before age 5.
Projected LifeExpectancy, 2010
With AIDS Without With AIDS WithoutSub-Saharan AfricaBotswana 120 38 38 66Burkina Faso 145 109 46 61Burundi 129 91 45 61Cameroon 108 78 50 63Cote d’Ivoire 121 84 47 62Dem. Rep. of Congo 116 97 52 60Ethiopia 183 137 39 55Kenya 105 45 44 69Lesotho 122 71 45 66Malawi 203 136 35 57Namibia 119 38 39 70Nigeria 113 68 46 65Rwanda 166 106 38 59South Africa 100 49 48 68Swaziland 152 78 37 63Tanzania 131 96 46 61Uganda 121 92 48 60Zambia 161 97 38 60Zimbabwe 116 32 39 70Latin AmericaBrazil 31 21 68 76Haiti 129 119 54 59Honduras 55 29 60 73Southeast AsiaBurma 80 70 59 63Cambodia 134 124 53 57Thailand 25 21 73 75

52
democratization accounted for two-thirds ofdemonstrated instability. The study defined“instability” as revolutionary wars, ethnicwars, genocides, and disruptive regime transi-tions. High infant mortality has a particularlystrong correlation with the likelihood of statefailure in partial democracies.
Infectious diseases also will affect nationalsecurity and international peacekeeping effortsas militaries and military recruitment poolsexperience increased deaths and disabilitiesfrom infectious diseases. The greatest impactwill be among hard-to-replace officers, non-commissioned officers, and enlisted soldierswith specialized skills and among militarieswith advanced weapons and weapons platformsof all kinds.
• HIV/AIDS prevalence in selected militaries,mostly in Sub-Saharan Africa, generallyranges from 10 to 60 percent (see table 6).This is considerably higher than their civilianpopulations and owes to risky lifestyles anddeployment away from home. Commence-ment of testing and exclusion of HIV-positiverecruits in the militaries of a few countries, isreducing HIV prevalence but it continues togrow in most militaries.
• Militaries in key FSU states are increasinglyexperiencing the impact of negative healthdevelopments within their countries, such asdeteriorating health infrastructure andreduced funding. One in three Russian draft-ees currently is rejected for various healthreasons, as compared to one in 20 in 1985,according to one Russian newspaper report.
• Mounting infectious disease-caused deathsamong the military officer corps in military-dominated and democratizing polities also
may contribute to the deprivation, insecurity,and political machinations that incline someto launch coups and counter-coups aimed,more often than not, at plundering statecoffers.
It is difficult to make a direct connectionbetween high HIV/AIDS and other infectiousdisease prevalence in military forces and per-formance in battle. But, given that a large num-ber of officers and other key personnel aredying or becoming disabled, combat readinessand capability of such military forces is boundto deteriorate.
• Infectious disease-related deaths and disabili-ties are likely to have the greatest impact onthe capabilities of Sub-Saharan militaries,particularly those that have achieved at least amodest level of modernization in weaponssystems and platforms. Over the longer term,the consequences of the continuing spread ofdeadly diseases such as HIV/AIDS on thecapabilities of the more modernized militar-ies in FSU states and possibly China and cer-tain rogue states with large armies andmodern weapons arsenals may be severe aswell.
The negative impact of high infectious diseaseprevalence on national militaries also is likelyto be felt in international and regional peace-keeping operations, limiting their effectivenessand also making them vectors for the furtherspread of diseases among coalition peacekeep-ers and local populations.
• Although the United Nations officiallyrequires that prospective peacekeeping troopsbe “disease free,” it is difficult to enforce this

53
rule with such methods as HIV testing, giventhe paucity of available troops and the poten-tial noncompliance of many contributingstates.
• Healthy peacekeeping forces will remain atrisk of being infected by disease-carryingforces and local populations, as well as byhigh-risk behavior and inadequate medicalcare.
In developed countries, the political debateover AIDS and other infectious diseases islikely to focus on budgetary issues andnegligence in the handling of blood and food-stuffs, as well as on treatment of infectious dis-eases.
• HIV blood and other controversies in severalEuropean countries have sparked politicaluproars and led to the dismissal or prosecu-tion of government officials, and have evencontributed to the fall of some governments.
Infectious diseases also will loom larger in glo-bal interstate relations as related embargoes andboycotts to prevent their spread create tradefrictions and controversy over culpability, suchas in the recently ended three-year EU embargoof British beef, which was imposed to stop thespread of mad cow disease. Developed coun-tries, moreover, will come under pressure frominternational and nongovernmental organiza-tions, as well as from developing countries, todeal with infectious disease-related instabilityand economic and medical needs in the hard-est-hit countries. A growing controversy, in thisregard, will be over drug-related intellectualproperty rights, in which developing countrieswill press for more and cheaper drugs fromdeveloped country pharmaceutical firms andresort to producing their own generic brands ifthey are rebuffed. States will remain concerned,as well, about the growing biological warfarethreat from rogue states and terrorist groups.
Infectious Diseases and US NationalSecurity
As a major hub of global travel, immigration,and commerce, along with having a large civil-ian and military presence and wide-ranginginterests overseas, the United States willremain at risk from global infectious diseaseoutbreaks, or even a bioterrorist incident usinginfectious disease microbes. Infectious diseaseswill continue to kill nearly 170,000 Americansannually and many more in the event of an epi-demic of influenza or yet-unknown disease or a
Source: DIA/AFMIC, 1999.
Table 6HIV Prevalence in Selected Militaries inSub-Saharan Africa
Country Estimated HIVPrevalence(percent)
Angola 40 to 60Congo (Brazzaville) 10 to 25Cote d’Ivoire 10 to 20Democratic Republic of the Congo 40 to 60Eritrea 10Nigeria 10 to 20Tanzania 15 to 30

54
steep decline in the effectiveness of availableHIV/AIDS drugs. Although several emerginginfectious diseases, such as HIV/AIDS, werefirst identified in the United States, most,including HIV/AIDS, originate outside US bor-ders, with the entry of the West Nile virus in1999 a case in point (see inset).
Threats to the US Civilian PopulationThe US civilian population will remain directlyvulnerable to a wide variety of infectiousdiseases, from resurgent ones such as multidrugresistant TB to deadly newer ones such as HIV/AIDS and hepatitis C. Infectious disease-related deaths in the United States haveincreased by about 4.8 percent per year since1980 to 59 deaths per 100,000 people by 1996,or roughly 170,000 deaths annually, as com-pared to an annual decrease of 2.3 percent inthe preceding 15 years and an alltime low of 36deaths per 100,000 in 1980 (see figure 17). TheUSCDC estimates that the total direct and indi-rect medical costs from infectious diseasescomprise some 15 percent of all US health careexpenditures or $120 billion in 1995 dollars.
In the opinion of the US Institute of Medicine,the next major infectious disease threat to theUnited States may be, like HIV, a previouslyunrecognized pathogen. Barring that, the mostlikely known infectious diseases to directly andsignificantly impact the United States over thenext decade will be HIV/AIDS, hepatitis C, andmultidrug resistant TB, or a new, more lethalvariant of influenza. Foodborne illnesses andhospital-acquired infections also pose a threat:
• HIV/AIDS was first identified in the UnitedStates in 1983 but originated in Sub-SaharanAfrica. In the United States, HIV/AIDSdeaths surged from 7,000 in 1985 to 50,000in 1995 before dropping dramatically to17,000 in 1997 as a result of behavioral and
therapeutic changes among the most at riskpopulations. The total number of thoseinfected reached 890,000 for all of NorthAmerica in 1998, including 44,000 newinfections, most of them in the United States.Although HIV/AIDS-related death rates havedeclined sharply, the poor prospects that avaccine will be available over the next decadeor more, along with the likelihood that thevirus will develop growing resistance to theprotease-inhibitor drugs now in use, portend acontinued rise in the infection rate and arenewed rise in the death rate.
• Hepatitis C. Some 4 million Americans arechronic carriers of hepatitis C, which wasfirst identified in the United States in 1989.The hepatitis C burden will continue to growfor at least another decade due to the dis-ease’s long incubation period, with the num-ber of deaths possibly surpassing HIV/AIDSdeaths by 2005 even though the rate of newinfections is dropping, owing to improvedblood supply testing. About 15 percent ofthose infected will develop life-threateningcirrhosis of the liver, and many more willexperience a more slowly developing chronicliver disease, including cancer. The diseasealso will remain the leading cause of livertransplantation.
• Foodborne illnesses. According to theUSCDC, tens of millions of foodborne illnesscases, including 9,000 deaths, occur eachyear in the United States. The threat fromfoodborne illnesses will persist given chang-ing consumption patterns and further global-ization of the food supply.

55
• The threat from highly virulent, antimicro-bial-resistant pathogens such as Staphylo-coccus aureus, Streptococcus pneumoniae,and enterrococci––which kill some 14,000hospital patients annually––is likely to grow,particularly if the remaining small arsenal ofeffective drugs, such as vancomycin,becomes ineffective.
• TB. After declining dramatically for severaldecades, TB in the first half of the 1990smade a comeback in urban areas and in some13 states with large refugee and immigrantpopulations, where some 23,000 to 27,000cases were reported annually, up from a lowof 22,000 in 1984. More alarming was therise of multidrug resistant TB from 10 per-cent of total cases before 1984 to 52 percentof cases resistant to at least one drug and 32percent resistant to two or more of the fivefrontline anti-TB drugs a decade later. Somehigh-risk populations in prisons and thosewith HIV/AIDS have experienced death ratesfrom TB as high as 70 to 90 percent.Although a massive and costly interventionby state and local authorities reversed theoverall infection rate to 18,000 by 1998, themultidrug resistant TB threat persists, and TBincidence continues to grow among immi-grant populations. About 40 percent of allactive TB cases in the United States—upfrom 16 percent in 1982—currently occuramong immigrants, particularly illegal onesfrom countries where TB is highly endemic.
• Influenza. Although the deadly 1918 influ-enza pandemic that caused more than 0.5 mil-lion US deaths appears to have started in theUnited States, almost all others have origi-nated in China and Southeast Asia. Epidemi-ologists generally agree that the threat ofanother “killer” influenza pandemic is highand that it is not a question of whether, butwhen, it will occur. Even in the absence of awidespread “killer” pandemic, influenza has
caused 30,000 US deaths annually in recentyears––nearly double the annual average inthe 1972-84 period, owing in part to the highvulnerability to the disease of the growingcohort of older Americans and HIV-infectedpersons. Influenza will remain essentially anuncontrolled disease because the viruses arehighly efficient in their ability to survive andchange into more virulent strains. USCDCresearchers predict that, in an influenza epi-demic infecting 15 percent of the US popula-tion, the mean number of expected deathswould be approximately 97,000 in one year,regardless of immunization status. The num-ber of hospitalizations would total 314,000,and the number of outpatient cases wouldreach 18 million. If the attack rate were 35percent, the number of expected deaths wouldbe 227,000 in one year and all other illnessrates would be correspondingly higher.
Other Infectious Disease ThreatsOther diseases that are periodically importedand are more likely to be costly in economicterms rather than in lives lost include malaria,cholera, and various animal diseases:
• Malaria. Malaria was domestically elimi-nated in the 1960s but has reemerged over thelast two decades due to the increase in immi-gration and international travel. Currently,some 1,200 cases of malaria are reported tothe USCDC annually, with about half occur-ring among US travelers to highly endemiccountries in the tropics and the other halfamong foreign nationals entering the UnitedStates, primarily agricultural workers andillegal migrants. Although malaria outbreakshave been relatively isolated and have beenbrought under control quickly, the disease hasthe potential to become reestablished in theUnited States because of the abundance ofmosquito vectors, especially in southernstates.

56
Mechanisms of Disease Entry Into theUnited States
The following are a few prominent methodsof pathogen entry into the United States:
• International travel. More than 57 millionAmericans traveled outside the UnitedStates for recreational and business pur-poses in 1998—often to high risk coun-tries—more than double the number just adecade before. In addition, tens of millionsof foreign-born travelers enter the UnitedStates every year. Travelers on commercialflights can reach most US cities from anypart of the world within 36 hours—which isshorter than the incubation periods ofmany infectious diseases.
• Immigration. Approximately 1 millionimmigrants and refugees enter the UnitedStates legally each year, often from coun-tries with high infectious disease preva-lence, while several hundred thousandenter illegally. The USCDC has the author-ity to detain, isolate, or provisionallyrelease persons at US ports of entry show-ing symptoms of any one of seven diseases(yellow fever, cholera, diphtheria, infec-tious TB, plague, suspected smallpox, andviral hemorrhagic fevers). Although eachindividual must undergo a medical exami-nation before entering the country, poten-tially excludable conditions may be in theincubating and therefore less detectablestages.
• Moreover, US law prohibits the Immigra-tion and Naturalization Service fromreturning refugees who have credible rea-sons to fear political persecution, includingthose refugees afflicted with infectiousdiseases.
• Returning US military forces. AlthoughUS military populations are immunizedagainst many infectious diseases and areespecially sensitized to detecting any symp-toms before or after their return to theUnited States, not all cases are likely to bedetected, especially among NationalGuardsmen and Reservists, who are farmore likely to enter the civilian health caresystem and may not associate a later-devel-oping illness with their overseas travel.
• The globalization of food supplies. Food-borne illnesses have become more commonas the number of food imports has doubledover the past five years, owing to changingconsumer preferences and increased trade.At certain times of the year, more than 75percent of the fruits and vegetables avail-able in grocery stores and restaurants areimported and, therefore, potentially morelikely to be infected with pathogenic micro-organisms, according to a foodborne dis-ease expert.

57

58
• Fears that cholera, which has becomeendemic in Latin America over the pastdecade, would find its way into the UnitedStates have not been realized, but isolatedcases have been occurring at a more frequentrate than at any time since 1962 when cholerasurveillance commenced. Thus, the diseaselooms as a potential threat.
• Dengue. Dengue, along with the far moreserious dengue hemorrhagic fever and dengueshock syndrome, was reintroduced into theUnited States in the mid-1980s by foreigntravelers; the mosquito vector is now wide-spread throughout the southeast. There were90 cases in 1998, all of which were acquiredoverseas.
• Foreign animal diseases. In addition to themore obvious human impacts, imported ani-mal diseases present considerable potentialrisks to the domestic economy, trade, andcommerce. Those potentially capable of sig-nificantly harming US agriculture includefoot and mouth disease (FMD), avian influ-enza, bovine spongiform encephalopathy,and African swine fever. An outbreak of footand mouth disease in the US livestock indus-try could cost as much as $20 billion over 15years in increased consumer costs, reducedlivestock productivity, and restricted trade,according to USDA estimates. AnotherUSDA study revealed that, if African swinefever were to become reestablished in the USswine population, the cost over a 10-yearperiod would be $5.4 billion.
Threats to Deployed Military ForcesDeployed US military forces have historicallyexperienced higher rates of hospital admissionfrom infectious diseases than from battlefieldcombat and noncombat injuries (see figure 18
and table 7). In addition to disease transmissionbetween deployed troops and indigenouspopulations, warfare-related social disruptionoften creates refugees and internally displacedpersons that can pass infections along to USmilitary forces. Allied coalition forces maythemselves bring infectious diseases into anarea for the first time and transmit them to USforces and the indigenous population.
Threats to deployed US forces will vary bycountry, region, and the nature of the deploy-ment and its mission:
• Least threatened will be US forces deployedin longstanding US, NATO, and other alliedbases in Europe, especially northern Europe,and in Japan, where base medical facilities,food sources and handling, as well as localhealth care infrastructures are on a par withUS standards.
• At highest risk will be those forces deployedto less developed regions for contingencyoperations such as humanitarian, peacekeep-ing, and peace enforcement missions. Localmedical care in such regions often is poor,and infectious disease prevalence is high,both among the local population and some-times among coalition peacekeeping forces.
• Specific examples of diseases that have andmay continue to appear in association withmilitary and peacekeeping operations includerespiratory diseases such as TB and influ-enza, diarrheal diseases, malaria, hepatitisA and E, sexually transmitted diseases,dengue and dengue hemorrhagic fever, andleishmaniasis.

59
Impact on US Interests AbroadIn addition to their impact on the US popula-tion, infectious diseases will add to the social,economic, and political strains in key regionsand countries in which the United States hassignificant interests or may be called upon toprovide assistance:
• Infectious diseases are likely to slow socio-economic development in developing andformer communist countries and regions ofinterest to the United States. This will chal-lenge democratic development and transitionsand possibly contribute to humanitarianemergencies and military conflicts to whichthe United States may need to respond.
• Infectious disease-related trade embargoesand restrictions on travel and immigrationalso will cause frictions among and with keytrading partners and other selected states.
The Biological Warfare ThreatThe biological warfare and terrorism threat toUS national security is on the rise as roguestates and terrorist groups also exploit the easeof global travel and communication in pursuitof their goals:
• The ability of such foreign-based groups andindividuals to enter and operate within the

60
United States has already been demonstratedand could recur. The West Nile virus scare,and several earlier instances of suspected bio-terrorism, showed, as well, the confusion andfear they can sow regardless of whether or notthey are validated.
• The threat to US forces and interests overseasalso will continue to increase as more nationsdevelop a capability to field at least limitednumbers of biological weapons, and nihilisticand religiously motivated groups contemplateopting for them to cause maximum casualties.
a Usual level of disease occurrence in an area.
Source: DIA/AFMIC, 1997.
Table 7Disease Threats to US Forces in the Gulf
Disease Category Examples Endemic Levelsa
Diarrheal Bacterial, protozoal, viral Moderately-to-highly endemicOther foodborne or waterborne Hepatitis A and E, typhoid/paratyphoid
feversModerately-to-highly endemic
Vectorborne Malaria
Sandfly fever, Leishmaniasis, other arbovi-ral (including dengue, West Nile, Sindbis,Crimean-Congo hemorrhagic fevers)
Focally endemic in Oman, Saudi Arabia,UAE
Endemic
Person-to-person/close contact Tuberculosis, meningococcal meningitis Low-to-moderately endemicSexually transmitted and/orbloodborne contact
Hepatitis B/D and C, Gonorrhea Moderately-to-highly endemic
Other endemic Brucellosis, Q fever, leptospirosis, tra-choma, intestinal parasites, anthrax
Endemic, especially in lower socioeco-nomic groups
















