29
Infectious Mononucleosis Mary Ann Hudson, RN The Ohio State University College of Nursing
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | ethan-barton |
| View: | 217 times |
| Download: | 2 times |

Infectious Mononucleosis
Mary Ann Hudson, RN The Ohio State University College of
Nursing
Overview of presentation
• Presentation of patient where infectious mononucleosis is part of differential
• An establishment of a few clinical pearls that assist the practitioner when infectious mono has entered the differential
• Epidemiology, patho, pediatric differential Dx (including labs), research, clinical Tx guidelines
• Dx of our mystery patient
14-year-old Female
• 4 day Hx sore throat, extreme fatigue, headache, loss of appetite, fever, N/V
• Exam revealed cervical lymphadenopathy and tenderness, pharyngeal inflammation and erythema, fever (101 F), mild left-sided tenderness, nasal congestion, and otitis serous.
• Patient and caregiver reported no previous Hx of mononucleosis. Negative rapid Strep A.

Exudative pharyngitis
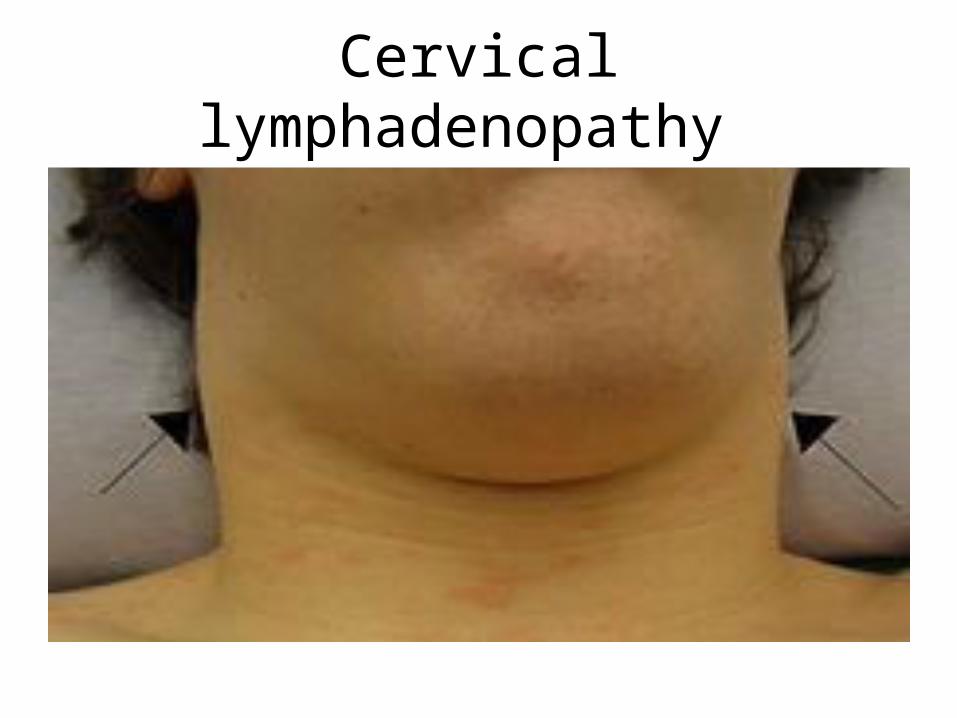
Cervical lymphadenopathy
Epidemiology• Epstein-Barr infectious mononucleosis is
caused by the Epstein-Barr virus, one type of herpes virus to which 90% of adults have been exposed.
• In developing countries, most of the population is exposed in early childhood. In developed countries, most of the population is exposed during adolescence.
• It is characterized by fever, sore throat, and fatigue.
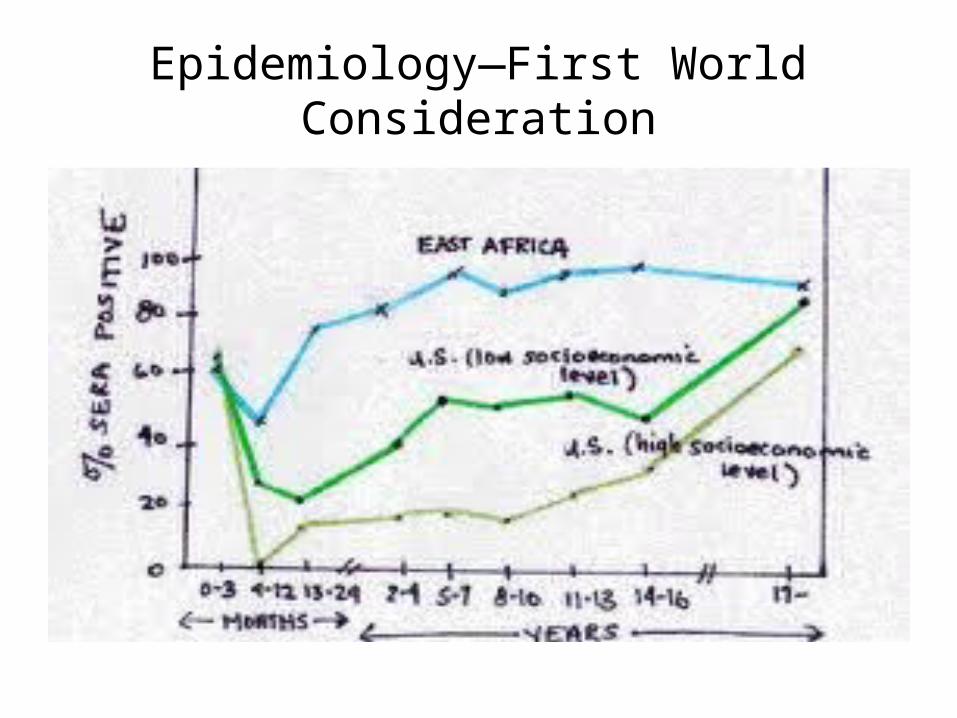
Epidemiology—First World Consideration
Prognosis and Natural Hx
• 4-6 incubation period to appearance of Sx• 2-7 week period of Sx, infectious at anytime from
introduction of virus, and some remain viral reservoirs for life. Reemergence from dormancy with Sx is possible.
• Less than 5% of patients experience complications leading to mortality and morbidity. Lymphomas and carcinomas d/t EBV initiated changes on the lymphocytes are are in the United States.

Burkitt’s Lymphoma--EBV

Pathophysiology
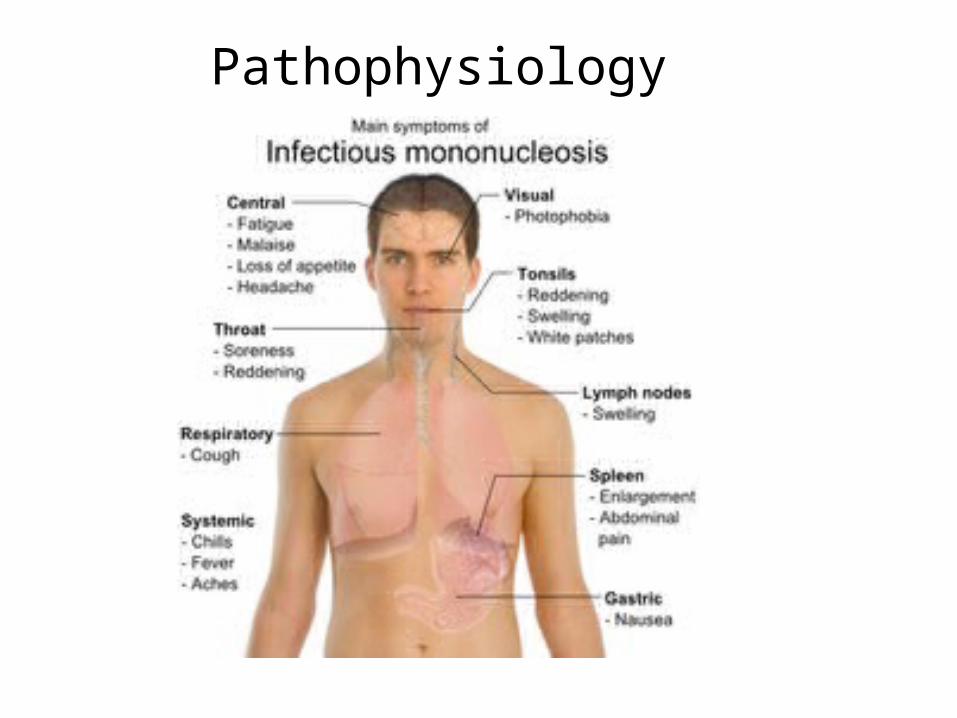
Pathophysiology
Differential—14 y.o. Female• EBV– Fever, malaise, pharyngitis, +N/V, cervical
lymphadenopathy, left-sided tenderness, reports no Hx of IM
– HOWEVER, progressive and additive Sx over 4 days, non-exudative pharyngitis, nasal congestion, otitis serous, lymphadenopathy limited to cervical chain, palpation of left-sided tenderness may be non-sensitive.

Differential—14 y.o. Female
• Strep A Pharyngitis – Inflammatory and painful pharyngitis, fever,
cervical lymphadenopathy, possible exposure from younger siblings.–HOWEVER, nasal congestion, otitis serous,
and negative rapid strep A
Differential—14 y.o. Female
• Adenovirus infection–Pharyngitis, nasal congestion, cervical
lymphadenopathy, fever, progressive symptomology, +N/V (adenovirus), otitis serous, negative rapid strep A.–HOWEVER, left-sided tenderness, extreme
fatigue, report of negative EBV Hx.

General Differential
• Group A Strep• Adenovirus• Cytomegalovirus (few clinical correlates,
serology r/o)• HIV (clinically and historically correlate)• Viral Hepatitis A, B, C (clinically correlate with
hepatomegaly, jaundice, Hx)• Leukemia, Lymphomas (will r/o with CBC)

Laboratory Orders
• CBC with differential• Liver Enzymes• Mononucleosis Rapid Slide Agglutination Test
(MonoSpot. Detects 90% of cases in teens and adults by identifying heterophile antibodies)
• EBC Serology detects past and present EBV infection
• Optional: CMV serology, HIV serology, Hepatitis panel serology
Laboratory Results
• CBC will show leukocyte count up to 20,000/mm3 and >10% atypical (Downey’s) lymphocytes. If this is result and clinically correlates to patient Sx, this is early positive IM result.
• Serology should confirm CBC. If not, may need to add differentials.
Laboratory Results—14 y.o. Female
• CBC WDL• EBV Serology revealed previous, but not
current EBV infection
Dx—Adenovirus. Clinically correlates with symptomology as adenovirus accounts for all UR and GI symptoms. Remember that left-sided tenderness can be non-sensitive and that patient had GI Sx.

Infectious Mononucleosis Treatment
Acetaminophen or Ibuprofen for fever reduction and analgesia
Prednisone 1mg/kg divided into 2 doses BID for severe lymphatic inflammation
Our 14 y.o. Female
• Adenovirus is also self-limiting and requires self-care that supports the symptomology (fluids, rest, analgesics or NSAIDs)
• Patient presented in the context of IM because she was an excellent example of correct differential for her age and symptoms and importance of understanding and ruling out IM. Her exposure to IM is an important part of her medical Hx.
Complications of IM
• Meningitis, Guillain-Barre, transverse myelitis• Ctyo and thrombo penias• Jaundice• UA restriction• Myocarditis • Splenic rupture (surgical emergency and a
point of education for families)
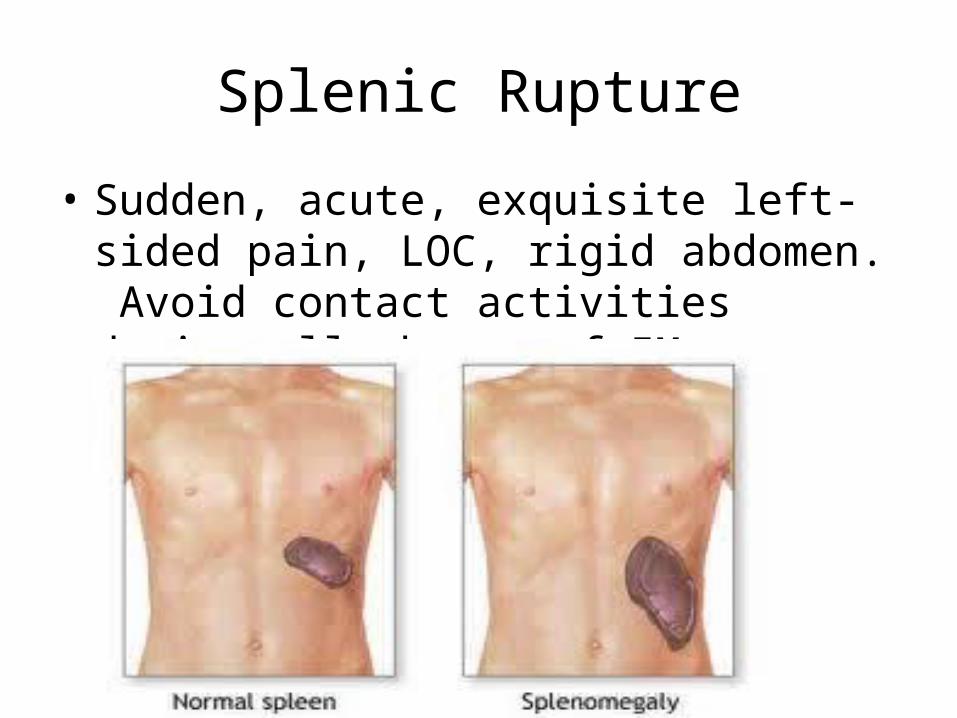
Splenic Rupture
• Sudden, acute, exquisite left-sided pain, LOC, rigid abdomen. Avoid contact activities during all phases of IM.

Research—Safe Return to Play After Infectious Mononucleosis
• Waninger, K., , & Harcke, H. (2005). Determination of safe return to play for athletes recovering from infectious mononucleosis: a review of the literature. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine, 15(6), 410-6.
• Important clinical consideration!
Research—Sensitivity of CBC as initial IM diagnostic tool
• Lennon, P., O' Neill, J., Fenton, J., , & O' Dwyer, T. (2010). Challenging the use of the lymphocyte to white cell count ratio in the diagnosis of infectious mononucleosis by analysis of a large cohort of Monospot test results. Clinical otolaryngology : official journal of ENT-UK ; official journal of Netherlands Society for Oto-Rhino-Laryngology & Cervico-Facial Surgery, 35(5), 397-401. doi:10.1111/j.1749-4486.2010.02187.x

Research—Adenovirus vs IM
• Mel, ón, S., M, éndez, S., Iglesias, B., Boga. (2005). Involvement of adenovirus in clinical mononucleosis-like syndromes in young children. European Journal of Clinical Microbiology & Infectious Diseases, 24(5), 314-8. doi:10.1007/s10096-005-1333-7
• Good overview of why labs are important and establish medical history (important in future differentials of EBV complications).
American Family Physician Clinical Guidelines for the Management of Infectious Mononucleosis
• Complete guidelines include a grade B for clinical findings that include generalized lymphadenopathy, fatigue, and exudative pharyngitis.
• Grade Cs are given for CBC correlation, use of prednisone, and avoidance of contact sports until patient is completely asymptomatic
• Guidelines include complete EBV serology, other serologies as clinically indicated, and Strep A rapid testing.
• Symptomatic and supportive treatment of symptoms including rest, fluids, and monitoring are also recommended.
Complete AFP Guidelines Available via Free PDF
• http://www.aafp.org/afp/2004/1001/p1279.pdf
14 y.o. Female—Critique of Care
• This patient received a complete physical that included IM in the differential.
• The patient was swabbed for Strep A and it was a negative rapid strep.
• The patient was sent for lab work that included a CBC and complete EBV serology.
• Lab results were correlated with clinical picture.
• This patient’s management was an exemplar case according to AFP clinical guidelines.

















![WORKSHOP SESSIONS DAY 2(October 29[Mon]) · Institute of Infectious Diseases W2-2-08 Oral Neomycin prevents hepatitis of severe infectious mononucleosis-like disease in murine](https://static.documents.pub/doc/80x56/6033401d452e3a74a96d5ee1/workshop-sessions-day-2ioctober-29moni-institute-of-infectious-diseases-w2-2-08.jpg)