401 U Clinical Progress Series Inferior Myocardial Infarction High-Risk Subgroups Peter B. Berger, MD, and Thomas J. Ryan, MD I nferior myocardial infarctions account for 40- 50% of all acute myocardial infarctions1l2 and are generally viewed as having a more favorable prognosis than anterior wall infarctions. Data from a number of recent trials of thrombolytic therapy in acute infarction appear to support this view, with mortality rates of 2-9% reported among patients with inferior infarctions assigned to the "standard care" or control groups within these studies.1-3 It is, thus, not surprising that many of these trials have failed to demonstrate reduced mortality after throm- bolytic therapy in the subset of patients with inferior infarction.1"3'4 It is important to note, however, that nearly 50% of patients suffering inferior infarction will have complications or distinguishing features associated with an increased mortality that will sub- stantially alter an otherwise favorable prognosis. It is the purpose of this review to identify the complica- tions most likely to occur during acute inferior infarc- tion as defined electrocardiographically by ST- segment elevation in leads II, III, and aVF. Specifically, heart block, concomitant precordial ST- segment depression, and right ventricular infarction are discussed, their pathogenesis is reviewed, and their impact on prognosis is considered. Also, the data that exist on the impact of thrombolytic therapy on these high-risk subgroups are reviewed. Heart Block As summarized in Table 1, there is a 19% inci- dence of high-degree (second- or third-degree) heart block complicating acute inferior infarction.5-20 Approximately one half of the patients who develop heart block do so through a gradual progression of their conduction delay, whereas the remainder abruptly develop the highest degree of heart block they will attain.89,12,15,2' The timing of the onset of the heart block in acute inferior infarction is pre- sented in Table 2.9,15,16,22,23 Roughly 8% of all patients who have an inferior infarction have high- degree heart block on arrival at the emergency From the Evans Memorial Department of Clinical Research and the Department of Medicine, the University Hospital, Boston, Massachusetts. Supported in part by NHLBI grant NO1-HV-38031. Address for correspondence: Thomas J. Ryan, MD, 88 E. Newton Street, Boston, MA 02118. Received August 1, 1989; revision accepted October 10, 1989. department, and approximately two thirds of the patients who are eventually going to develop high- degree heart block have done so within 24 hours of admission. Virtually all the remaining patients who develop heart block do so within 3 days of admission. The overall experience with heart block occurring in association with acute inferior infarction indicates that the heart block is responsive to atropine or isoproterenol in the majority of cases, usually does not require placement of a temporary pacemaker, and almost never requires implantation of a perma- nent pacemaker.22 Given the relative ease of treat- ment and rather short duration of the conduction abnormality, it is surprising that the development of heart block during inferior infarction is associated with an in-hospital mortality rate of more than 20%. Virtually every study on the subject has shown a markedly increased in-hospital mortality in patients whose inferior infarctions are complicated by the development of second- or third-degree (high- degree) heart block. As shown in Table 3, the mean in-hospital mortality for patients with high-degree heart block is 23%.5,9,14,17,18,21,22,24-26 When third- degree heart block is present, the average mortality is 29% (Table 4).12,13,23,27-33 All of the studies cited were conducted in the, era of coronary care units, and pacemakers were used when appropriate. It is of interest that almost none of the patients was believed to have died as a result of their heart block (although many died with persistent heart block) or from the treatment of the heart block. It now appears that this increased mortality relates to the observation that heart block developing during inferior infarction is a marker for increased infarc- tion size. Many studies have shown that patients with inferior infarctions associated with heart block have larger infarctions than those without heart block based on estimation of infarct size by enzyme levels,91334 left and right ventricular ejection frac- tions determined by gated blood pool scan,'1425 and wall motion analyses of the left and right ventricles determined by echocardiography.25 While these stud- ies serve to confirm an association between larger infarcts and atrioventricular (AV) block, they do not explain the nature of the relation or the mechanism of the heart block itself. The two most common explanations that have been offered to explain the etiology of the heart block by guest on May 19, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript
401
U Clinical Progress Series
Inferior Myocardial InfarctionHigh-Risk Subgroups
Peter B. Berger, MD, and Thomas J. Ryan, MD
I nferior myocardial infarctions account for 40-50% of all acute myocardial infarctions1l2 andare generally viewed as having a more favorable
prognosis than anterior wall infarctions. Data from anumber of recent trials of thrombolytic therapy inacute infarction appear to support this view, withmortality rates of 2-9% reported among patientswith inferior infarctions assigned to the "standardcare" or control groups within these studies.1-3 It is,thus, not surprising that many of these trials havefailed to demonstrate reduced mortality after throm-bolytic therapy in the subset of patients with inferiorinfarction.1"3'4 It is important to note, however, thatnearly 50% of patients suffering inferior infarctionwill have complications or distinguishing featuresassociated with an increased mortality that will sub-stantially alter an otherwise favorable prognosis. It isthe purpose of this review to identify the complica-tions most likely to occur during acute inferior infarc-tion as defined electrocardiographically by ST-segment elevation in leads II, III, and aVF.Specifically, heart block, concomitant precordial ST-segment depression, and right ventricular infarctionare discussed, their pathogenesis is reviewed, andtheir impact on prognosis is considered. Also, thedata that exist on the impact of thrombolytic therapyon these high-risk subgroups are reviewed.
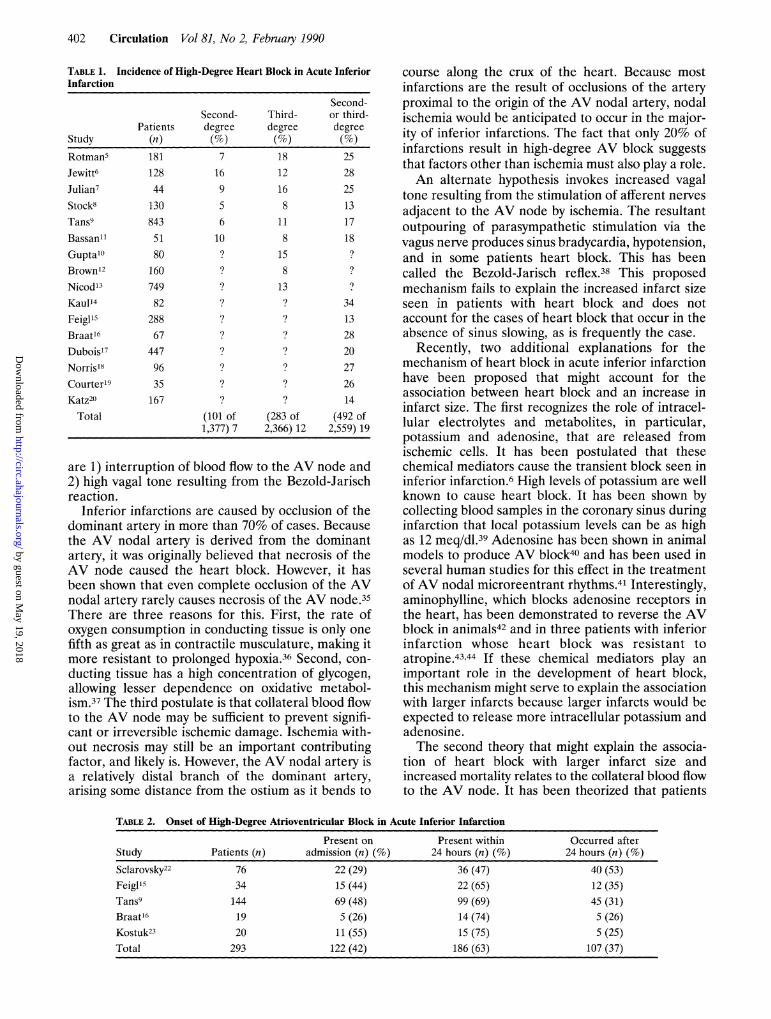
Heart BlockAs summarized in Table 1, there is a 19% inci-
dence of high-degree (second- or third-degree) heartblock complicating acute inferior infarction.5-20Approximately one half of the patients who developheart block do so through a gradual progression oftheir conduction delay, whereas the remainderabruptly develop the highest degree of heart blockthey will attain.89,12,15,2' The timing of the onset ofthe heart block in acute inferior infarction is pre-sented in Table 2.9,15,16,22,23 Roughly 8% of allpatients who have an inferior infarction have high-degree heart block on arrival at the emergency
From the Evans Memorial Department of Clinical Research andthe Department of Medicine, the University Hospital, Boston,Massachusetts.
Supported in part by NHLBI grant NO1-HV-38031.Address for correspondence: Thomas J. Ryan, MD, 88 E.
Newton Street, Boston, MA 02118.Received August 1, 1989; revision accepted October 10, 1989.
department, and approximately two thirds of thepatients who are eventually going to develop high-degree heart block have done so within 24 hours ofadmission. Virtually all the remaining patients whodevelop heart block do so within 3 days of admission.The overall experience with heart block occurring
in association with acute inferior infarction indicatesthat the heart block is responsive to atropine orisoproterenol in the majority of cases, usually doesnot require placement of a temporary pacemaker,and almost never requires implantation of a perma-nent pacemaker.22 Given the relative ease of treat-ment and rather short duration of the conductionabnormality, it is surprising that the development ofheart block during inferior infarction is associatedwith an in-hospital mortality rate of more than 20%.
Virtually every study on the subject has shown amarkedly increased in-hospital mortality in patientswhose inferior infarctions are complicated by thedevelopment of second- or third-degree (high-degree) heart block. As shown in Table 3, the meanin-hospital mortality for patients with high-degreeheart block is 23%.5,9,14,17,18,21,22,24-26 When third-degree heart block is present, the average mortality is29% (Table 4).12,13,23,27-33 All of the studies citedwere conducted in the, era of coronary care units, andpacemakers were used when appropriate. It is ofinterest that almost none of the patients was believedto have died as a result of their heart block (althoughmany died with persistent heart block) or from thetreatment of the heart block.
It now appears that this increased mortality relatesto the observation that heart block developing duringinferior infarction is a marker for increased infarc-tion size. Many studies have shown that patients withinferior infarctions associated with heart block havelarger infarctions than those without heart blockbased on estimation of infarct size by enzymelevels,91334 left and right ventricular ejection frac-tions determined by gated blood pool scan,'1425 andwall motion analyses of the left and right ventriclesdetermined by echocardiography.25 While these stud-ies serve to confirm an association between largerinfarcts and atrioventricular (AV) block, they do notexplain the nature of the relation or the mechanismof the heart block itself.The two most common explanations that have
been offered to explain the etiology of the heart block
TABLE 1. Incidence of High-Degree Heart Block in Acute InferiorInfarction
Study
Rotman5
Jewitt6
Julian7Stock8
Tans9Bassan1'
Gupta10
Brown12
Nicod13
Kaul14
Feigll9
Braat16
Dubois17
Norris18
Courter19
Katz20
Total
Patients(n)181
128
44
130
843
5180
160749
82
288
67
447
96
35
167
Second-degree(%)
7
16
956
10?
?
?
?
1?
1?
1?
1?
(101 of1,377) 7
Third-degree(%)
18
12
16
8
11
8
15
8
13?
1?
1?
1?
1?
1?
(283 Of2,366) 12
Second-or third-degree(%)
2528
25
13
17
18?
34
1328
20
27
26
14
(492 of2,559) 19
are 1) interruption of blood flow to the AV node and2) high vagal tone resulting from the Bezold-Jarischreaction.
Inferior infarctions are caused by occlusion of thedominant artery in more than 70% of cases. Becausethe AV nodal artery is derived from the dominantartery, it was originally believed that necrosis of theAV node caused the heart block. However, it hasbeen shown that even complete occlusion of the AVnodal artery rarely causes necrosis of the AV node.35There are three reasons for this. First, the rate ofoxygen consumption in conducting tissue is only onefifth as great as in contractile musculature, making itmore resistant to prolonged hypoxia.36 Second, con-
ducting tissue has a high concentration of glycogen,allowing lesser dependence on oxidative metabol-ism.37 The third postulate is that collateral blood flowto the AV node may be sufficient to prevent signifi-cant or irreversible ischemic damage. Ischemia with-out necrosis may still be an important contributingfactor, and likely is. However, the AV nodal artery isa relatively distal branch of the dominant artery,arising some distance from the ostium as it bends to
course along the crux of the heart. Because mostinfarctions are the result of occlusions of the arteryproximal to the origin of the AV nodal artery, nodalischemia would be anticipated to occur in the major-ity of inferior infarctions. The fact that only 20% ofinfarctions result in high-degree AV block suggeststhat factors other than ischemia must also play a role.An alternate hypothesis invokes increased vagal
tone resulting from the stimulation of afferent nerves
adjacent to the AV node by ischemia. The resultantoutpouring of parasympathetic stimulation via thevagus nerve produces sinus bradycardia, hypotension,and in some patients heart block. This has beencalled the Bezold-Jarisch reflex.38 This proposedmechanism fails to explain the increased infarct sizeseen in patients with heart block and does notaccount for the cases of heart block that occur in theabsence of sinus slowing, as is frequently the case.
Recently, two additional explanations for themechanism of heart block in acute inferior infarctionhave been proposed that might account for theassociation between heart block and an increase ininfarct size. The first recognizes the role of intracel-lular electrolytes and metabolites, in particular,potassium and adenosine, that are released fromischemic cells. It has been postulated that thesechemical mediators cause the transient block seen ininferior infarction.6 High levels of potassium are wellknown to cause heart block. It has been shown bycollecting blood samples in the coronary sinus duringinfarction that local potassium levels can be as highas 12 meq/dl.39 Adenosine has been shown in animalmodels to produce AV block40 and has been used inseveral human studies for this effect in the treatmentofAV nodal microreentrant rhythms.41 Interestingly,aminophylline, which blocks adenosine receptors inthe heart, has been demonstrated to reverse the AVblock in animals42 and in three patients with inferiorinfarction whose heart block was resistant toatropine.4344 If these chemical mediators play animportant role in the development of heart block,this mechanism might serve to explain the associationwith larger infarcts because larger infarcts would beexpected to release more intracellular potassium andadenosine.The second theory that might explain the associa-
tion of heart block with larger infarct size andincreased mortality relates to the collateral blood flowto the AV node. It has been theorized that patients
TABLE 2. Onset of High-Degree Atrioventricular Block in Acute Inferior Infarction
with inferior infarctions who develop heart block maybe more likely to have concomitant stenosis of the leftanterior descending artery (LAD) proximal to theorigin of the septal perforators, which provide a richnetwork of collateral vessels between the LAD andthe AV nodal arteries. This would predispose the AVnode to greater degrees of ischemia. To test thishypothesis, Bassan et all' studied a consecutive seriesof 51 survivors of inferior infarction who underwentcoronary angiography. Eleven of the 51 developedheart block. Comparing patients with and without heartblock revealed a sixfold greater incidence of heart blockif the LAD had a 75% or greater stenosis before thesecond septal perforator. The presence of heart blockhad a sensitivity of 31%, a specificity of 95%, and apredictive value of 91% for the presence of concomi-tant LAD obstruction. However, two subsequent stud-ies produced opposite findings. An increased incidenceof LAD disease was not found in the Thombolysis inAcute Myocardial Infarction (TAMI)45 or Thromboly-sis In Myocardial Infarction (TIMI)46 populations.Heart block during inferior infarction was not pre-dictive of multivessel disease in either of thesestudies.No placebo-controlled thrombolytic trial has
reported specifically on the outcome of patients withinferior infarction who have high-degree heart block
on presentation to the hospital. Data from the TIMIII trial, in which all patients enrolled in the studywere treated with intravenous recombinant tissue-typeplasminogen activator (rt-PA), reveal an in-hospitalmortality of9% (20 of 231) for patients who developedsecond- or third-degree heart block.46 The TAMIinvestigators report a mortality of 14% among patientswith third-degree heart block after thrombolytictherapy.45 The mortality rate among patients withheart block in these trials in which thrombolytictherapy was used is less than the 23% mortality amongpatients with high-degree heart block from pooleddata from before the thrombolytic era. However, therelative risk of mortality associated with heart blockafter thrombolytic therapy (3.8 in the TIMI II trialcompared with 2.6 in the prethrombolytic era)remains high. Therefore, we have no direct evidenceat the present time that thrombolytic therapy is ofparticular benefit in this group of patients.
Precordial ST-Segment DepressionAcute inferior infarction is accompanied by ST-
segment depression in the precordial chest leads inapproximately one half of patients suffering a first,inferior infarction. However, the significance of theprecordial ST-segment depression is less than clear.Initially, it was believed that the anterior ST-segment
TABLE 4. Hospital Mortality in Acute Inferior Infarction Complicated by Complete Heart Block
depression was merely an electrocardiographic phe-nomenon resulting from the "reciprocal" reflection ofthe interior current of injury, with no anatomic orphysiologic significance. It now appears that this is thecase in only a minority of patients. Most studies haveshown that, taken as a group, patients with precordialST-segment depression have larger infarcts as deter-mined by creatine phosphokinase (CPK) levels,47-51more severe regional wall motion abnormalities,48-52and lower left ventricular ejection fractions.48-53 Inaddition, they may be prone to more short- andlong-term complications than patients without ST-segment depression.47,50,5153-55 The two leading expla-nations for anterior ST-segment depression in acuteinferior infarction that are believed to explain thelarger infarcts and more complicated courses observedin these patients are anterior ischemia due to concom-itant LAD disease or more extensive and severeinferoposterior infarction, which produces "posteriorST elevation" manifest as anterior ST-segmentdepression on the surface electrocardiogram.
Antertior IschemiaIt is well established that the incidence of multi-
vessel disease among patients surviving even uncom-plicated inferior infarction is high. Miller et a156catheterized 84 consecutive patients with a mean ageof 52.8±2.8 years surviving uncomplicated inferiorinfarction and found multivessel disease in 80% ofpatients. This was initially believed to support theconcept that anterior ST-segment depression mightbe due to anterior ischemia from concomitant LADdisease. Although two subsequent studies revealedstatistically significant associations between precordialST-segment depression and the presence of LADdisease, both of these studies included only thosepatients who underwent catheterization for clinicalcomplications following inferior infarction and, thus,are considerably biased.5758 There have been sevenstudies of consecutive series of patients undergoingcatheterization after inferior infarction,51-53,59-62 andonly one reported a statistically significant differencein the prevalence of LAD disease between patientswith and without anterior ST-segment depression.53Roubin et a153 studied 84 consecutive survivors of a
first inferior infarction with angiography and ventric-ulography. The prevalence of significant stenosis(more than 70%) in the LAD was significantly higherin the group with precordial ST-segment disease(36% vs. 3%, p<0.05), as was the prevalence ofmultivessel disease (53% vs. 6%,p<0.01). The peakCPK level was significantly higher in the group withST-segment depression (1,879±935 vs. 1,122+800,p<0.01). These patients had a higher incidence ofcomplications in the early postinfarction course,including congestive heart failure, malignant ventric-ular arrhythmia, and high-degree heart block, thanpatients without precordial ST-segment depression.The mean left ventricular ejection fraction was sig-nificantly lower in patients with ST-segment depres-
to note that a comparison of the group of patientswith precordial ST-segment depression and one-vessel disease (25 of 53) with those patients withoutprecordial ST-segment depression (only two of whomhad multivessel disease) reveals a significantly lowerejection fraction (51±12% vs. 56+11%,p<0.05) anda significantly higher CPK release (1,595±833 vs.1J122+800, p<0.01.) in the group with precordialST-segment depression and one-vessel disease. Inthese patients, a branch of the right coronary arterysupplied the lateral wall more commonly (48% vs.19%, p<0.05), and the distal right coronary arterymore often supplied the apex (57% vs. 22%,p<0.05)than it did in patients without anterior ST-segmentdepression. These data provide strong evidence thatprecordial ST-segment depression during acute infe-rior infarction is a marker for larger infarction as aresult of either ischemia at a distance due to thepresence of multivessel disease or a greater amountof myocardium supplied by the infarct-related artery.Shah et a148 studied 44 patients after acute inferior
infarction without a history of a previous infarction.These authors found that the 24 patients with ante-rior ST-segment depression were far more likely tohave abnormal wall motion in the anteroseptal andapical segments on gated blood pool scanning thanthe 20 patients without anterior ST-segment depres-sion (50% vs. 15%, p<0.05). These patients hadlarger infarcts as determined by CPK release, agreater degree of wall motion abnormalities ininfarct-related segments, and lower left ventricularejection fractions.The best modality for studying the significance of
anterior ST-segment depression during inferiorinfarction may be positron emission tomographybecause of its ability to detect myocardial ischemiabased on the depression of metabolic activity. Bill-adello et a163 studied 13 consecutive patients withinferior infarction, nine of whom had anterior ST-segment depression. Positron tomography revealedthree of the nine patients to have anterior ischemia.All three were shown to have significant stenosis ofthe LAD on catheterization associated with anteriorwall motion abnormalities on ventriculography. Twoadditional patients developed "true posterior infarc-tion" (R>S in lead VJ). Despite the small number ofpatients in this study, it does provide compellingevidence that at least some patients with inferiorinfarction and anterior ST-segment depression areundoubtedly experiencing anterior ischemia.
Posterior Transmural InfarctionEvidence supporting the concept that anterior
ST-segment depression represents "reciprocal"expression of a large area of transmural infarctionencompassing the posterior wall is found in the studyby Gibson et al.51 These investigators studied 48consecutive patients after inferior infarction withcoronary angiography, submaximal thallium stresstests, and gated blood pool scans, all within 2 weeksof the acute event. The 27 patients (56%) withsion (48 .-13% vs. 56-+-11%,p<0.05). It is interesting
Berger and Ryan Inferior Myocardial Infarction 405
precordial ST-segment depression had significantlyhigher peak CPK levels, significantly more severeregional wall motion abnormalities, and lower overallleft ventricular ejection fractions. More patients withanterior ST-segment depression evolved electrocar-diographic evidence of true posterior infarction thandid patients without precordial ST depression (26%vs. 5%, p<0.05). Thallium scanning revealed morefrequent and severe inferior and inferoapical perfu-sion abnormalities in the group with anterior ST-segment depression.
Goldberg et a149 studied 25 consecutive patientsafter a first inferior infarction with gated blood poolscans. Thirteen of the 14 patients (93%) with ante-rior ST-segment depression had posterolateral aki-nesis on ventriculography in contrast to the 11patients without anterior ST-segment depression,none of whom had posterior akinesis (p<0.001).Ong et a150 analyzed 70 patients with gated blood
pool scans and thallium scans. The 47 patients withprecordial ST-segment depression had more severelyreduced inferoposterior regional ejection fractions(40% vs. 52%, p<0.005), lower left ventricular ejec-tion fractions (45% vs. 52%,p<0.05), and more than50% greater peak CPK levels (1,856±+1,133 vs.1,135 +705 units, p<0.05). Although the mortality ofthe patients with precordial ST-segment depressionwas greater than the mortality of patients withoutthis finding (28% vs. 4%), precordial ST-segmentdepression was not an independent predictor ofmortality when infarct size and ventricular functionwere included in multivariate analysis.
In one of the largest studies examining this issue,Hlatky et a154 used the Duke University Data Bank toretrospectively examine 162 consecutive patients suf-fering a first inferior infarction. These authorsrequired only 0.5-mm ST-segment depression inleads V1 through V3 for inclusion into the precordialST-segment depression group, a less-stringent inclu-sion criterion than other studies. The group withprecordial ST-segment depression had significantlylarger infarctions and a greater percentage of poste-rior infarctions as judged by a QRS scoring system.They also had a higher in-hospital mortality (13% vs.4%,p <0.001) and significantly increased incidence of"urgent, nonfatal complications" (defined as reinfarc-tion, persistent hypotension, Killip class III or IVcongestive heart failure, and ventricular tachycardiaor fibrillation) than those patients without precordialST-segment depression (46% vs. 29%, p=0.026).This was one of few studies to reveal a statisticallysignificant increase in mortality in patients with infe-rior infarction associated with precordial ST-segmentdepression. The size of the study and the method ofanalyzing precordial ST depression as a continuousvariable rather than a dichotomous one were likely tohave increased the statistical power of the study.Not all studies investigating the significance of
precordial ST-segment depression have reported it tobe of clinical significance. Several studies failed to
ment of ventricular function,59,62,64 or radionuclideevidence of posterior infarction65 in patients present-ing with precordial ST-segment depression. How-ever, many of these studies used less-stringent crite-ria for precordial ST-segment depression,62,64included patients presenting with inferior ST-segment depression,6265 or were limited by smallsample size.59
Nonetheless, the majority of studies have shownthat patients presenting with inferior infarction asso-ciated with precordial ST-segment depression havelarger myocardial infarctions than patients withoutprecordial ST-segment depression. Despite thisfinding, few studies have examined the impact ofthrombolysis on this high-risk group.The Netherlands Interuniversity Cardiology Insti-
tute reported the results of 533 patients randomlyassigned to either standard care (n=264) or throm-bolytic therapy (n=269).66 These investigators founda strong relation between the amount of summedST-segment deviation, defined for inferior infarctionas the amount of ST-segment elevation in leads I, II,
III, aVL, aVF, V5, and V6 combined with the amountof ST-segment depression in leads V, through V4, andenzymatic infarct size, ejection fraction and mortal-ity. Multivariate regression analysis revealed that thelargest limitation of infarct size after thrombolytictherapy was present in patients with the greatestsummed ST-segment deviation. A preliminary reportby the same group on the results of a recent trial inwhich 721 patients were randomized to receive eitherrt-PA or placebo supports the finding that amongthose patients with inferior infarction, those withprecordial ST-segment depression benefit the mostfrom thrombolytic therapy.67
Berland et a152 reported on 38 consecutive patientswho underwent left ventriculography, coronary angi-ography, and treatment with intracoronary streptoki-nase within 6 hours of a first inferior myocardialinfarction.52 A second angiographic study was per-formed on all patients between the 12th and 15thhospital days. Pretreatment ventriculography re-vealed a lower mean ejection fraction in the 23patients (60%) with precordial ST-segment depres-sion than in the 15 patients (40%) without ST-segment depression (51±10% vs. 59+7%,p<0.01).Follow-up ventriculography revealed that patientswho had successful thrombolysis and a patent coro-nary artery on repeat angiography had a better meanejection fraction than those patients with an occludedvessel (56±9% vs. 47±8%, p<0.01). However, thebenefit in ventricular function was confined to thosepatients with precordial ST-segment depression onadmission electrocardiogram. There was improve-ment in segmental contraction in those patients whopresented with anterior ST-segment depression, inwhom successful recanalization resulted in adecrease in the hypokinetic surface (from 11.3±6 to8.5±4.5 cm2,p<0.05) and in the hypokinetic percent-age of the ventricular perimeter (from 48±14% to
show evidence of larger infarction,59 greater impair- 40-t9%, p<0-05). In contrast, there was no signifi-
cant change in the hypokinetic zone after successfulthrombolysis in the patients without precordial ST-segment depression (hypokinetic surface area from4.7+2.4 to 6.5+3.1 cm2, p=NS; and hypokineticpercentage of the ventricular perimeter from25±13% to 34+12%,p=NS).
Bates et a168 reported on the impact of throm-bolytic therapy in the 159 patients with inferiorinfarctions treated with rt-PA and randomized toearly angioplasty or deferred angioplasty in theTAMI-I trial. These investigators found that the 74patients (47%) with precordial ST-segment depres-sion had lower left ventricular ejection fractionsbefore treatment with thrombolytic therapy than the85 patients (53%) without precordial ST-segmentdepression (54% vs. 58%,p<0.02). Repeat ventricu-lography at 7 days revealed that the group withprecordial ST-segment depression had a persistentlylower mean left ventricular ejection fraction (53% vs.57%, p<0.02). However, the difference in ejectionfraction between the patients with and without pre-cordial ST-segment depression in this study is lessthan has been reported in prior studies, leading theauthors to suggest that the patients with precordialST-segment depression benefited from thrombolytictherapy.
Little et a169 administered intracoronary streptoki-nase to 17 patients in the acute phase of inferiorinfarction. Fourteen of these patients had precordialST-segment depression. Recanalization of the rightcoronary artery was successful in 12 of these patientsand resulted in the prompt resolution of the precor-dial ST-segment depression, including those patientswith LAD disease.
Right Ventricular InfarctionOnly recently has the occurrence and significance of
right ventricular (RV) infarction been appreciated.Previously, RV infarction was not believed to be aclinically significant entity. Starr et al, in 1943,70 dem-onstrated no adverse hemodynamic effects after cau-terizing the RV free wall in open-chest dogs. Sawataniet al71 replaced the RV free wall in dogs with aprosthetic patch and frequently found no hemody-namic impairment. It was not until 1973 that Cohn eta172 first described the now classic clinical syndromeproduced by acute ischemic RV dysfunction.RV myocardial infarction is predominantly a com-
plication of inferior infarction. Whether it is diag-nosed by echocardiography,73,74 first pass,75,76 orequilibrium radionuclide ventriculography,76-82 orautopsy,83,84 RV infarction has been shown to occurin approximately one third of patients suffering anacute inferior infarction. In about one half of thesepatients, it is of hemodynamic significance.74,77,82,85 Incontrast, RV infarction occurs in association withanterior myocardial infarction in less than 10% ofcases.86,87 Isolated RV infarction is rare.83
It is generally believed that patients suffering infe-rior infarctions complicated by RV involvement have
artery resulting in infarction of the anterolateral wallof the RV, which is primarily perfused by acutemarginal branches.77,79,81 However, several pathologicanalyses have shown that it is the posterior RV wallthat is most frequently involved in RV infarction andnearly always in association with left ventricular pos-terior and posteroseptal infarction.8487,88 The occa-sional development ofRV infarction after occlusion ofthe circumflex artery in left dominant patients77'84'88and in patients with occlusions of the distal rightcoronary artery and posterior descending artery87 sup-port the significance of the posterior circulation in RVinfarction. It appears that obstruction of blood flow toboth the posterior circulation and acute marginalvessels increases the likelihood, and size, of RVinfarction.88 Because most inferior infarctions resultfrom occlusion of the right coronary artery at itsproximal or middle portion before the acute marginalvessels and the posterior descending artery, it is notintuitively clear why only a minority of inferior infarc-tions are complicated by RV involvement. Theoriespostulated to explain the relative infrequency of RVinfarction include 1) lower oxygen requirements of theRV due to its smaller muscle mass and work load; 2) agreater total amount of blood flow available due togreater coronary blood flow during systole; 3) moreextensive collateralization of the RV, primarily fromthe left coronary system; and 4) diffusion of oxygenfrom intracavitary blood through the thin wall of theRV.82,89 Several studies have indicated that patientswith RV hypertrophy are more likely to have RVinfarction,90-92 whereas others have not found thisassociation.84'87,89 One study shows that patients withRV involvement are more likely to have concomitantLAD lesions, reducing possible collateralization to theposterior right and left ventricles,89 but others havenot found an increased prevalence of multivesseldisease in patients with RV involvement.77818490Therefore, it remains unclear what the predisposingfactors are for RV involvement in acute inferiormyocardial infarction.The clinical sequelae of RV infarction vary widely,
ranging from no hemodynamic compromise to severehypotension and cardiogenic shock.72'74'77'85 Thehypotension and shock occur when there is enoughRV ischemia to decrease RV compliance, raising thediastolic filling pressure in the RV. Filling of the RVis reduced, and RV stroke volume decreases. As aresult, filling of the left ventricle is impaired, cardiacoutput is reduced, and systemic blood pressuredecreases.72
Therefore, patients with hemodynamic compro-mise due to RV infarction will often have an elevatedjugular venous pressure, usually 10 mm or more, witha positive Kussmaul's venous sign and clear lungfields.85 In severe cases, systemic hypotension ispresent.72 There may also be signs of tricuspidregurgitation.93,94 Characteristic findings on physicalexamination may be absent despite noninvasive evi-
more proximal occlusions of their right coronary dence of RV involvement.74,77,82,85
Berger and Ryan Inferior Myocardial Infarction 407
Hemodynamic findings on catheterization typicallyreveal disproportionate elevation of right heart pres-sures, with a ratio of right atrial to pulmonary capillarywedge pressure of 0.80 or more.73,76,85,95 Because thesefindings may also be present in pericardial constrictionand less frequently in cardiac tamponade, an accuratediagnosis may be difficult.84,96The most reliable electrocardiographic evidence of
RV infarction is ST-segment elevation of 1 mm ormore in the right precordial leads and, in particular,lead V4R, when there is associated ST elevation inleads II, III, and aVF. Several studies have shownthis to have a sensitivity and specificity for RVinfarction of more than 90%, with a positive predic-tive value of more than 80%.16,79,97,98 Right precor-dial ST-segment elevation usually resolves early inthe course of inferior infarction and must be lookedfor promptly.
Early recognition of RV infarction is clinicallyimportant to ensure not only that appropriate treat-ment is instituted but also that treatments that arecontraindicated are avoided. Initial therapy for ahemodynamically significant RV infarction requiresthe administration of volume to increase filling of theischemic, noncomplicant RV. This is essential toraise the cardiac output and increase the preload ofthe underfilled left ventricle.7280'9599 It is criticallyimportant to avoid drugs that result in venodilationand a decrease in RV filling because these maydramatically worsen systemic hypotension. In fact,hypotension after administration of sublingual nitro-glycerin in the setting of inferior infarction shouldimmediately raise the suspicion of RV involvement.In those patients who fail to increase their cardiacoutput despite volume loading, dobutamine'00 anddopamine82 have been shown to be effective. Whentreated correctly, the hypotension and shock arereadily reversed in the majority of patients. In theabsence of hemodynamic compromise, no specifictreatment for a RV infarction is required.
Controversy exists regarding the natural history ofRV wall motion abnormalities that develop in associ-ation with inferior infarction. A number of investiga-tors have shown through the use of serial radionuclideventriculograms that RV dysfunction often improveswith time after acute inferior infarction.77,10' In con-trast, others have shown that the RV wall motionabnormalities generally persist.75 02 This discrepancymay reflect the existence of two different populationsof patients. In some cases, RV wall motion abnormal-ities detected early in the course of inferior infarctionmay represent stunned myocardium resulting fromischemia that does not produce substantial necrosis.Those patients in whom RV dysfunction persists pre-sumably have had ischemia resulting in infarction.The short-term consequences of RV infarction are
not limited to the characteristic hypotension andright heart failure. Barrillon et al in 19741'3 were thefirst to report that patients with right precordialST-segment elevation during inferior myocardialinfarction were at least threefold more likely to
develop second- or third-degree heart block thanpatients without ST elevation. Others have found STelevation in V4R to be predictive of the subsequentdevelopment of high-degree heart block in 48-75%of patients during acute inferior infarction.16'104The long-term clinical consequences of RV infarc-
tion are not well known. The available evidencesuggests that RV infarction is not only predictive ofmajor complications during the hospital course butalso a possible independent risk factor for long-termmortality as well. Polak et al105 have shown inpatients with coronary artery disease and chronicheart failure that RV dysfunction is a risk factor formortality independent of left ventricular dysfunction.Pfisterer et al106 found that RV dysfunction is anindependent risk factor for complex ventricularectopy and sudden death in the year after a myocar-dial infarction. However, Gadsboll et al107 found noindependent association between RV dysfunctionand mortality during the year after acute myocardialinfarction. Unfortunately, each of these studies failedto distinguish between true RV infarction associatedwith inferior infarction and RV dysfunction thatoccurs most commonly after anterior infarction as aresult of left ventricular infarction and the secondaryelevation of pulmonary pressures, increasing the RVafterload. Patients suffering RV infarction may bemore susceptible to the future development of rightheart failure; further studies involving long-termfollow-up are needed.There is little experimental or clinical evidence
about the impact of thrombolysis on patients withRV involvement during inferior infarction. Schuler etal108 retrospectively studied 19 patients with acuteinferior infarction due to proximal right coronaryartery occlusion from a larger series of patients withacute inferior infarction to study the response of theRV to successful thrombolysis. All patients under-went radionuclide ventriculography before adminis-tration of intravenous streptokinase that was fol-lowed by acute catheterization, intracoronarystreptokinase, and percutaneous transluminal coro-nary angioplasty, if needed. Patients were dividedinto two groups based on whether recanalization wassuccessful (12 patients, 63%) or unsuccessful (sevenpatients, 37%). Radionuclide imaging repeated 4weeks after acute infarction revealed markedimprovement in RV function only in the patients inwhom thrombolysis was successful (29.7+8.7% to43.2±5.0%, p<0.01); there was no improvement inRV function in the patients without successfulthrombolysis (33.4+4.8% to 32.2+6.1%, p=NS).These findings are in contrast to those of Verani et
al,77 who found that RV function improved even inthose patients without successful thrombolysis. How-ever, both of these studies suffered from small sam-ple size. Data from the TIMI II trial support the viewthat successful thrombolysis reduces the incidence ofRV involvement during inferior infarction.109 In thetrial, 1,017 patients with acute inferior infarctionunderwent radionuclide ventriculography before dis-
charge. RV wall motion abnormalities were presentin 62 patients (6%). Angiographic analysis of thosepatients undergoing protocol catheterization 18-48hours after treatment with rt-PA reveals that patientswith patency of the infarct-related artery had a muchlower incidence of RV infarction (15 of 387, 4%,compared with 11 of 68, 16% incidence amongpatients with occluded arteries; p<O.OO1). In addi-tion, patients with RV infarction were significantlymore likely to have occlusion of the infarct-relatedartery despite thrombolytic therapy (11 of 26, 42%)than patients without RV involvement (57 of 429,13%, p<O.OO1). The low incidence of RV infarctionamong patients with patency and the greater inci-dence of occlusion in patients with RV infarctionprovide evidence that successful thrombolysisreduces the incidence of RV infarction.
ConclusionPatients with inferior infarction complicated by
heart block, concomitant precordial ST-segmentdepression, and RV involvement have larger infarc-tions and a worse prognosis than patients withoutthese features. The effect of thrombolysis on thesehigh-risk groups is not well known. At the presenttime, there is conflicting evidence regarding theefficacy of thrombolytic therapy in patients withinferior infarction. In view of the increasing evidencethat patients with the largest infarctions benefit themost from acute reperfusion, patients in these high-risk subgroups may be particularly good candidatesfor thrombolytic therapy.
References1. Gruppo Italiano per lo Studio della Streptochinasi nell'In-
farto Miocardico (GISSI): Effectiveness of intravenousthrombolytic treatment in acute myocardiac infarction. Lan-cet 1986;1:397-402
2. ISIS-2 (Second International Study of Infarct Survival) Col-laborative Group: Randomized trial of intravenous streptoki-nase, oral aspirin, both or neither among 17,187 cases ofsuspected acute myocardial infarction: ISIS-2. Lancet 1988;2:349-360
3. Kennedy JW, Martin GV, Davis KB, Maynard C, Stadius M,Sheehan FH, Ritchie JL: The Western Washington intrave-nous streptokinase in acute myocardial infarction random-ized trial. Circulation 1988;77:345-352
4. Kennedy JW, Ritchie JL, Davis KB, Fritz JK: WesternWashington randomized trial of intracoronary streptokinasein acute myocardial infarction. N Engl J Med 1983;309:1477-1482
5. Rotman M, Wagner GS, Waugh RA: Significance of highdegree atrioventricular block in acute posterior myocardialinfarction. Circulation 1973;47:257-262
6. Jewitt D: The genesis of cardiac arrhythmias in acute myo-cardial infarction. Prog Cardiol 1972;1:61-94
7. Julian DJ, Valentine PA, Miller GG: Disturbances of rate,rhythm and conduction in acute myocardial infarction. Am JMed 1964;37:915-927
8. Stock RJ, Macken RJ: Observations on heart block duringcontinuous electrocardiographic monitoring in myocardialinfarction. Circulation 1968;38:993-1005
9. Tans, Lie KI, Durrer D: Clinical setting and prognosticsignificance of high degree atrioventricular block in acuteinferior myocardial infarction: A study of 144 patients. AmHeart J 1980;99:4-8
11. Bassan R, Maig IG, Bozza A, Amino JGC, Santos M:Atrioventricular block in acute inferior wall myocardialinfarction: Harbinger of associated obstruction of the leftanterior descending coronary artery. J Am Coil Cardiol1986;8:773-778
12. Brown RW, Hunt D, Slomon JG: The natural history ofatrioventricular conduction defects in acute myocardialinfarction. Am Heart J 1969;78:460-466
13. Nicod P, Gilpin E, Dittrich H, Polikar R, Henning H, Ross J:Long-term outcome in patients with inferior myocardialinfarction and complete atrioventricular block. J Am CollCardiol 1988;12:589-594
14. Kaul V, Haron H, Malhotra A, Bhatia ML: Significance ofadvanced atrioventricular block in acute myocardial infarc-tion-A study based on ventricular function and holtermonitoring. Int J Cardiol 1986;11:187-193
15. Feigl D, Ashkenasy J, Kishon Y: Early and late atrioventric-ular block in acute inferior myocardial infarction. JAm CollCardiol 1984;4:35-38
16. Braat SH, deZwaan C, Brugada P, Coenegracht JM, WellensHJJ: Right ventricular involvement with acute inferior wallmyocardial infarction identifies high risk of developing atri-oventricular nodal conduction disturbances. Am Heart J1984;107:1183-1187
20. Katz R, Conroy RM, Robinson K, Mulcahy R: The aetiologyand prognostic implications of reciprocal changes in acutemyocardial infarction. Br Heart J 1986;55:423-427
21. Beregovich J, Fenig S, Lasser J, Allen D: Management ofacute myocardial infarction complicated by advanced atrio-ventricular block. Am J Cardiol 1969;23:54-65
22. Sclarovsky S, Strasberg B, Hirshberg A, Arditi A, Lewin RF,Agmon J: Advanced early and late atrioventricular block inacute inferior wall myocardial infarction. Am Heart J 1984;108:19-24
24. Chatterjee K, Leathem A, Harris A: The risk of pacing afterinfarction and current recommendations. Lancet 1969;2:1061-1063
25. Strasberg B, Pinchas A, Arditti A, Lewin RF, Sclarovsky S,Hellman C, Zafrir N, Agmon J: Left and right ventricularfunction in inferior acute myocardial infarction and signifi-cance of advanced atrioventricular block. Am J Cardiol1984;54:985-987
26. Friedberg CK, Cohen H, Donoso E: Advanced heart block asa complication of acute myocardial infarction: Role of pace-maker therapy. Prog Cardiovasc Dis 1968;10:466-481
27. Rodrigues RD, Vidaillet HJ, Hlatky MA: Long term prog-nosis of complete heart block during acute myocardial infarc-tion (abstract). Circulation 1987;76(suppl IV):IV-283
28. Gould L, Reddy CVR, Kim SG, On KC: Bundle electrogramin patients with acute myocardial infarction. PACE 1979;2:428-434
29. Lassers BW, Julian DG: Artificial pacing in management ofcomplete heart block complicating acute myocardial infarc-tion. Br Med J 1968;20:142-146
30. Paulk EA, Hurst JW: Complete heart block in acute myocar-dial infarction. Am J Cardiol 1966;17:695-706
31. Leth A, Hansen JF, Meibom J: Acute myocardial infarctioncomplicated by third degree atrioventricular block treatedwith temporary pacemaker; hospital and long-term survival in57 patients. Acta Med Scand 1974;195:391-395
Berger and Ryan Inferior Myocardial Infarction 409
32. Christiansen I, Haghelt T, Amtorp 0: Complete heart blockin acute myocardial infarction: Drug therapy. Am Heart J1973;85:162-166
33. Gregory JJ, Grace WJ: The management of sinus bradycar-dia, nodal rhythm and heart block for the prevention ofcardiac arrest in acute myocardial infarction. Prog CardiovascDis 1968;10:505-517
34. Opolski G, Kraska T, Ostrzycki A, Zielinski T, Korewicki J:The effect of the infarct size on atrioventricular and intra-ventricular conduction disturbances in acute myocardialinfarction. Int J Cardiol 1986;10:141-147
35. Bilbao FJ, Zabalza IE, Vilanova JR, Froufe J: Atrioventric-ular block in posterior acute myocardial infarction: A clini-copathologic correlation. Circulation 1987;75:733-736
36. Schiebler TH, Stark M, Caesar R: Die stoffwechselsituationdes reizleitungssystems. Klin Wochenschr 1956;34:181-183
37. Dehaan R: Differentiation of the atrioventricular conductingsystem of the heart. Circulation 1961;24:458-469
38. Von Bezold A, Hirt L: Uber die physiologischen Wirkungendes essigsauren veratrin's. Unter a d Physiol Lab Wurzburg1867;1:73-96
39. Harris AS: Factors which determine prognosis in experimen-tal coronary occlusion, in Surawicz B, Pellagrino ED (eds):Sudden Cardiac Death. New York, Grune & Stratton, 1964,pp 110-121
40. Belardinelli L, Mattos EC, Berne RM: Evidence for adeno-sine mediation of atrioventricular block in the ischemiccanine myocardium. J Clin Invest 1981;68:195-205
41. DiMarco JP, Sellers TD, Berne RM, West GA, BellardinelliL: Adenosine: Electrophysiologic effects and therapeutic use
for terminating paroxysmal supraventricular tachycardia. Cir-culation 1983;68:1254-1263
42. Belardinelli L, Fenton R, West A, Linden J, Althaus J, BerneRM: Extracellular action of adenosine and the antagonism byaminophylline on the atrioventricular conduction in isolatedperfused guinea pig and rat hearts. Circ Res 1982;51:569-579
43. Shah PK, Nalos P, Peter T: Atropine resistant post infarctioncomplete AV block: Possible role of adenosine and improve-ment with aminophylline. Am Heart J 1987;113:194-195
44. Wesley RC, Lerman BB, DiMarco JP, Berne RM, Belar-dinelli L: Mechanism of atropine-resistant atrioventricularblock during inferior myocardial infarction: Possible role ofadenosine. JAm Coll Cardiol 1986;8:1232-1234
45. Clemmensen P, Bates ER, Califf RM, Hlatky M, George BS,Kereiakes DJ, Aronson L, Berrios E, Topol EL: Is completeheart block in inferior infarction a benign phenomenonfollowing reperfusion therapy (abstract)? J Am CoIl Cardiol1989;13(suppl II):26
46. Berger PB, Ruocco NA, Jacobs AK, Ryan TJ: Increasedmortality associated with heart block during inferior infarc-tion: Results from TIMI II. Circulation 1989;80(suppl II):II-347
47. Gelman JS, Saltups A: Precordial ST segment depression inpatients with inferior infarction; Clinical implications. BrHeart J 1982;48:560-565
48. Shah PK, Pichler M, Berman DS, Maddahi J, Peter T, SinghBN, Swan HJC: Noninvasive identification of a high risksubset of patients with acute inferior myocardial infarction.Am J Cardiol 1980;46:915-921
49. Goldberg HL, Borer JS, Jacobstein JG, Kluger J. Scheidt SS,Alonso DR: Anterior S-T segment depression in acuteinferior myocardial infarction: Indicator of posterolateralinfarction. Am J Cardiol 1981;48:1009-1015
50. Ong L, Valdellon B, Coromilas J, Brody R, Reiser P,Morrison J: Precordial S-T segment depression in inferiormyocardial infarction: Evaluation by quantitative thallium-201 scintigraphy and technetium-99m ventriculography.Am JCardiol 1983;51:734-739
52. Berland J, Criber A, Behar P, Letac B: Anterior ST depres-sion in inferior myocardial infarction: Correlation withresults of intracoronary thrombolysis. Am Heart J 1986;3:481-488
53. Roubin GS, Shen WF, Nicholson M, Dunn RF, Kelly DT,Harris PJ: Anterolateral ST segment depression in acuteinferior myocardial infarction: Angiographic and clinicalimplications. Am Heart J 1984;107:1177-1782
54. Hlatky MA, Calif RM, Lee KL, Piyor DB, Wagner GS,Rosati RA: Prognostic significance of precordial ST-segmentdepression during inferior acute myocardial infarction. Am JCardiol 1985;55:325-329
55. Nasmith J, Marpole D, Rahal D, Homan J, Stewart S,Sniderman A: Clinical outcomes after inferior myocardialinfarction. Ann Int Med 1982;96:22-26
56. Miller RR, DeMaria AN, Vismara LA, Salel AF, MaxwellKS, Amsterdam EA, Mason DT: Chronic stable inferiorinfarction: Unsuspected harbinger of high risk proximal leftcoronary arterial obstruction amenable to surgical revascu-larization. Am J Cardiol 1977;39:954-960
57. Salcedo JR, Baird MG, Chambers RJ, Beanlands DS: Signif-icance of reciprocal S-T segment depression in anteriorprecordial leads in acute inferior myocardial infarction:Concomitant left anterior descending coronary artery dis-ease? Am J Cardiol 1981;48:1003-1008
59. Cohen M, Blanke H, Karsh KR, Holt J, Rentrop P: Implica-tions of precordial ST segment depression during acuteinferior myocardial infarction: Arteriographic and ventricu-lographic correlations during the acute phase. Br Heart J1984;52:497-501
60. DeWood MA, Heit J, Spores J, Eugster GS, Coulston D,Reisig AH, Hinnen ML, Shields JP: Significance of precor-dial ST segment depression in acute inferior transmuralmyocardial infarction: Assessment by coronary arteriographyand ventriculography during the early hours (abstract). Cir-culation 1982;66(suppl II):II-182
62. Feit F, Rey M, Sherman W, Cohen M, Stecy P, Cole W,Nachamie M, Thornton, Rentrop P, and the Mt Sinai-NYUReperfusion Study Group: Does anterior ST-depression inacute inferior wall MI (IWMI) have predictive value(abstract)? Circulation 1988;78(suppl II):II-212
63. Billadello JJ, Smith JL, Ludbrooke PA, Tiefenbrunn AJ,Jaffe AS, Sobel BE, Geltman EM: Implications of "reciprq-cal" ST segment depression associated with ac4te myocardialinfarction identified by position tomography. J Am CollCardiol 1983;2:616-624
64. Croft CH, Woodward W, Nicod P, Corbett JR, Vpwis SE,Willerson JT, Rude RE: Clinical implications of anterior S-Tsegment depression in patients with acute myocardial infarc-tion. Am J Cardiol 1982;50:428-436
65. Mukharji J, Murray S, Lewis SE, Croft CH, Corbett JR,Willerson JT, Rude RE: Is anterior ST depression with acutetransmural inferior infarction due to posterior infarction? Avectorcardiographic and scintographic study. JAm Coll Car-diol 1984;4:28-34
66. Vermeer F, Simoons ML, Bar FW, Tijssen JGP, DomburgRT van, Serruys PW, Verheugt FWA, Res JCJ, Zwann C de,Loarse A van der, Krauss XH, Lubsen J, Hugenholtz PG:Which patients benefit most from early thrombolytic therapywith intracoronary streptokinase? Circulation 1986;74:1379-1389
67. Arnold AER, Werf FV, Simoons ML, Lubsen J, VerstraeteM: Intravenous rt-PA for acute myocardial infarction: Whichpatients benefit most (abstract)? Circulation 1988;78(supplII):II-212
68. Bates ER, Clemmensen PM, Gorman LE, Aronson LG:Precordial ST segment depression predicts a worse prognosisin inferior infarction despite reperfusion therapy (abstract).Circuilation 1988;78(suppl II):II-211
69. Little WC, Rogers EW, Sodums MT: Mechanism of anteriorST segment depression during acute inferior myocardialinfarction: Observations during coronary thrombolysis. AnnIntem Med 1984;100:226-229
70. Starr I, Jeffers WA, Meade RH Jr: The absence of conspic-uous increments of venous pressure after severe damage tothe right ventricle of the dog, with a discussion of the relationbetween clinical congestive failure and heart disease. AmHeart J 1943;26:291-301
71. Sawatani S, Mandell G, Kusaba E, Schraut W, Cascade P,Wajszczuk WJ, Kantrowitz A: Ventricular performance fol-lowing ablation and prosthetic replacement of right ventric-ular myocardium. Trans Am Soc Artif Int Organ 1974;20:629-636
72. Cohn JN, Gulha NH, Broder MI, Limas CJ: Right ventricularinfarction: Clinical and hemodynamic features. Am J Cardiol1974;33:209-214
73. Dell'ltalia LJ, Starling MR, Crawford MH, Boros BL,Chaudhuri TK, O'Rourke RA: Right ventricular infarction:Identification by hemodynamic measurements before andafter volume loading and correlation with noninvasive tech-niques. JAm Coll Cardiol 1984;4:931-939
74. Lopez-Sendon J, Garcia-Fernandez MA, Coma-Canella I,Yanguela MM, Banuelos F: Segmental right ventricularfunction after acute myocardial infarction, two-dimensionalechocardiographic study in 63 patients. Am J Cardiol 1983;51:390-396
75. Reduto LA, Berger HJ, Cohen LS, Bottschalk A, Zaret BC:Sequential radionuclide assessment of left and right ventric-ular performance after acute transmural myocardial infarc-tion. Ann Int Med 1978;89:441-447
76. Starling MR, Dell'Italia LJ, Chandhuri TK, Boros BL,O'Rourke RA: First transit and equilibrium radionuclideangiography in patients with inferior transmural myocardialinfarction: Criteria for the diagnosis of associated hemody-namically significant right ventricular infarction. J Am CollCardiol 1984;4:923-930
77. Verani MS, Tortoledo FE, Batty JW, Raizner AE: Effect ofcoronary artery recanalization on right ventricular function inpatients with acute myocardial infarction. JAm Coll Cardiol1985;5:1029-1035
78. Nishumura T, Yasuda T, Gold HK, Leinbach RC, BoucherCA, McKusick KA, Strauss HW: High-risk subgroup ofinferior infarction: Importance of anterior wall motion andright ventricular function. Radiol Med 1986;4:112-118
79. Braat SH, Brugada P, deZwaan C, denDulk K, Wellens HJJ:Right and left ventricular ejection fraction in acute inferiorwall infarction with or without ST segment elevation in leadV4 R. JAm Coll Cardiol 1984;4:940-944
81. Lew AS, Laramee P, Shah PK, Maddahi J, Peter T, Gann W:Ratio of ST segment depression in lead V2 to ST segmentelevation in lead aVF in evolving inferior acute myocardialinfarction: An aid to the early recognition of right ventricularischemia. Am J Cardiol 1986;57:1047-1051
82. Shah PK, Maddahi J, Berman DS, Pichler M, Swan HJC:Scintographically detected predominant right ventricular dys-function in acute myocardial infarction: Clinical and hemo-dynamic correlates and implications for therapy and progno-sis. JAm Coll Cardiol 1985;6:1264-1272
83. Wartman WB, Hellerstein HK: The incidence of heartdisease in 2000 consecutive autopsies. Ann Intem Med 1948;28:41-65
84. Isner JM, Roberts WC: Right ventricular infarction compli-cating left ventricular infarction secondary to coronary heartdisease: Frequency, location, associated findings and signifi-cance from analysis of 236 necropsy patients with acute orhealed myocardial infarction. Am J Cardiol 1978;42:885-894
85. Dell'Italia LJ, Starling MR, O'Rourke RA: Physical exami-nation for exclusion of hemodynamically important rightventricular infarction. Ann Intemn Med 1983;99:608-611
86. Cabin HS, Clubb KS, Wackers FJT, Zaret BL: Right ventric-ular myocardial infarction with anterior wall left ventricularinfarction: An autopsy study. Am Heart J 1987;113:16-22
87. Ratliff NB, Hackel DB: Combined right and left ventricularinfarction: Pathogenesis and clinicopathologic correlations.Am J Cardiol 1980;45:217-221
88. Anderson HR, Falk E, Nielson D: Right ventricular infarc-tion: Frequency, size and topography in coronary arterydisease: A prospective study comprising 107 consecutiveautopsies from a coronary care unit. J Am Coll Cardiol1987;10:1223-1232
89. Haupt HM, Hutchins GM, Moore GW: Right ventricularinfarction: Role of the moderator band artery in determininginfarct size. Circulation 1983;67:1268-1272
90. Forman MB, Wilson BH, Sheller JR, Kopelman HA, VaughnWK, Virmani R, Friesinger GC: Right ventricular hypertro-phy is an important determinant of right ventricular infarc-tion complicating acute inferior left ventricular infarction. JAm Coll Cardiol 1987;10:1180-1187
91. Kopelman HA, Forman MB, Wilson BH, Kolodgie FD,Smith RF, Friesinger GC, Virmani R: Right ventricularmyocardial infarction in patients with chronic lung disease:Possible role of right ventricular hypertrophy. J Am CollCardiol 1985;5:1302-1307
92. Wade WG: The pathogenesis of infarction of the rightventricle. Br Heart J 1959;21:545-554
93. Zone DD, Botti RE: Right ventricular infarction with tricus-pid insufficiency and chronic right heart failure. Am J Cardiol1976;34:445-448
94. D'Arcy B, Nanda NC: Two-dimensional echocardiographicfeatures of right ventricular infarction. Circulation 1982;65:167-173
95. Lloyd EA, Gersh BJ, Kennelly BM: Hemodynamic spectrumof "dominant" right ventricular infarction in 19 patients. AmJ Cardiol 1981;48:1016-1022
96. Lorrell B, Leinbach RC, Pohost GM, Gold HK, DinsmoreRE, Hutter AM, Pastore JO, DeSanctis RW: Right ventric-ular infarction: Clinical diagnosis and differentiation fromcardiac tamponade and pericardial constriction. Am J Cardiol1979;43:465-471
97. Erhardt LR, Sjogren A, Wahlberg I: Simple right-sidedprecordial lead in the diagnosis of right ventricular involve-ment in inferior myocardial infarction. Am Heart J 1976;91:571-576
98. Croft CH, Nicod P, Corbett JR, Lewis SE, Huxley R,Mukharji J, Willerson JT, Rude RE: Detection of acute rightventricular infarction by right precordial electrocardio-graphy. Am J Cardiol 1982;50:421-427
99. Baigrie RS, Haq A, Morgan CD, Rakowski H, Drobac M,McLaughlin P: The spectrum of right ventricular involvementin inferior wall myocardial infarction: A clinical, hemody-namic and noninvasive study. J Am Coll Cardiol 1983;1: 1396-1404
100. Dell'italia LJ, Starling MR, Blumhardt R, Lasher JC,O'Rourke RA: Comparative effects of volume loading, do-butamine, and nitroprusside in patients with predominantright ventricular infarction. Circulation 1985;72:1327-1335
101. Dell'italia LI, Lemro NJ, Starling MR, Crawford MH, Sim-mons RS, Lasher JC, Blumhardt R, Lancaster J, O'RourkeRA: Hemodynamically important right ventricular infarction:Follow-up examination of right ventricular systolic functionat rest and during exercise with radionuclide ventriculogra-phy and respiratory gas exchange. Circulation 1987;75:996-1003
102. Marmor A, Geltman EM, Biello DR, Sobel BE, Siegel BA,Roberts R: Functional response of the right ventricle tomyocardial infarction: Dependence on the site of left ventric-ular infarction. Circulation 1981;64:1005-1011
103. Barrillon A, Chaignon M, Guizel L, Berbaux A: Premonitorysign of heart block in acute posterior infarction. Br Heart J1975;37:2-8
Berger and Ryan Inferior Myocardial Infarction 411
104. Nistor-Hemmert D, Ciplea A: The predictive value of V3R-V4R precordial leads in the occurrence of conduction distur-bances in inferior acute myocardial infarction (AMI). Physi-ologie 1982;19:87-90
105. Polak JF, Holman L, Wynne J, Colucci WS: Right ventricularejection fraction: An indicator of increased mortality inpatients with congestive heart failure associated with coro-nary artery disease. JAm Coll Cardiol 1983;2:217-224
106. Pfisterer M, Emmenegger H, Soler M, Burkhart F: Prognos-tic significance of right ventricular ejection fraction forpersistent complex ventricular arrhythmias and/or suddencardiac death after first myocardial infarction: Relation toinfarct location, size, and left ventricular function. Eur HeartJ 1986;7:289-298
107. Gadsboll N, Hoilund-Carlsen PF, Madsen EB, Marving J,Pedersen A, Lonborg-Jensen H, Dige-Petersen H, JensenBH: Right and left ventricular ejection fractions: Relation toone-year prognosis in acute myocardial infarction. Eur HeartJ 1987;8:1201-1209
108. Schuler G, Hoffman M, Schwarz F, Mehmel H, Manthey J,Tillmanns H, Hartmann S, Kubler W: Effect of successfulthrombolytic therapy on right ventricular function in acuteinferior wall myocardial infarction. Am J Cardiol 1984;54:951-957
109. Berger PB, Ruocco NA, Timm CT, Zaret BL, Wackers FJTh, and the TIMI Investigators: The impact of thrombolytictherapy on right ventricular infarction complicating inferiormyocardial infarction: Results from TIMI II (abstract).Circulation 1989;80(suppl II):II-313
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.81.2.401
1990;81:401-411Circulation.
http://circ.ahajournals.org/content/81/2/401.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions: