Leeds Institute of Molecular Medicine Leeds Institute of Molecular Medicine Michael McDermott ([email protected]) Section of Musculoskeletal Disease, Leeds Institute of Molecular Medicine, University of Leeds, UK Inflammasomes and autoimmune diseases
Transcript
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
NALPs in vitiligo and hypertension
Jin Y et al. NALP1 in vitiligo-associated multipleautoimmune disease. N Engl J Med 2007 356:1216-22
• NALP1 SNPs associated with several autoimmune and autoinflammatorydiseases, implicating innate immunity in the pathogenesis of these disorders• these diseases include autoimmune thyroid disease (Graves' disease andautoimmune hypothyroidism), Addison's disease, rheumatoid arthritis,psoriasis, pernicious anaemia, and SLE among patients with generalised vitiligo• NALP1 expressed in T-lymphocytes, granulocytes and monocytes
T. Omi et al. An intronic VNTRs of the cold-inducedautoinflammatory syndrome 1 (CIAS1) gene modifies geneexpression and is associated with essential hypertension.Eur J Hum Genet. 2006 14:1295–1305
• inflammation oxidative stress-related genes in development of hypertension
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
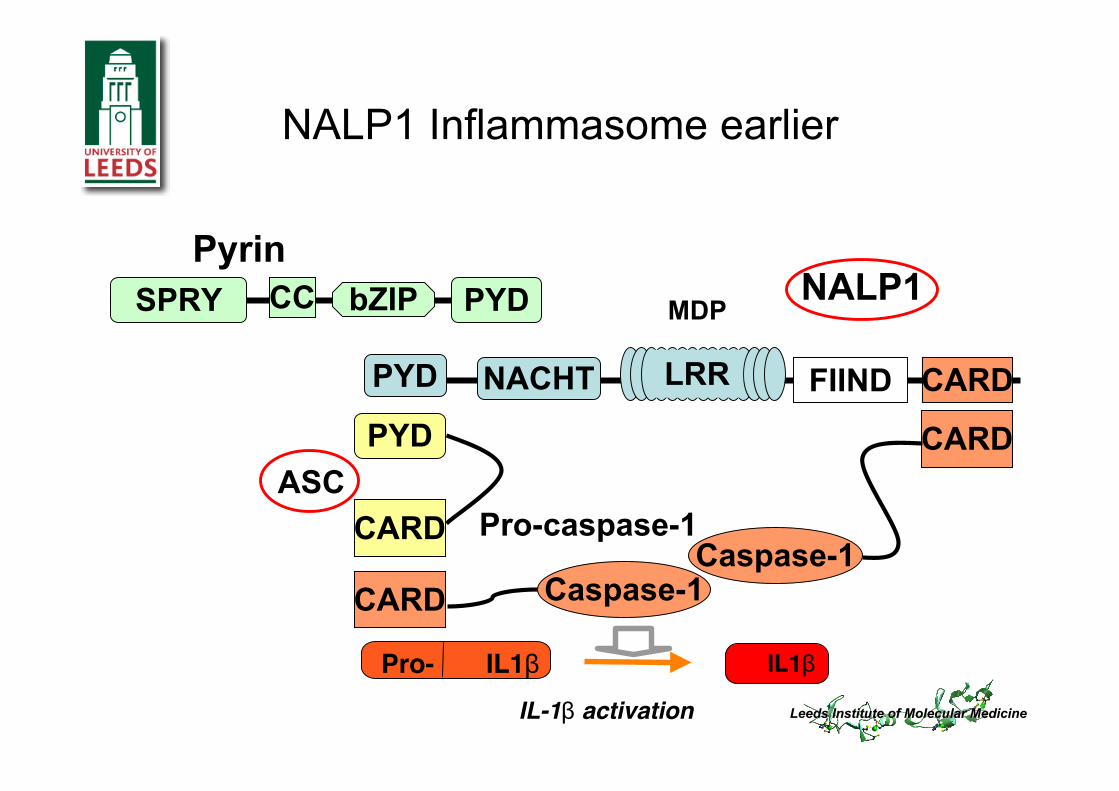
PYDCCSPRY bZIPPyrin
PYD NACHT LRR
NALP1
CARD Caspase-1
CARD
Caspase-1
FIIND CARD
MDP
PYD
CARDASC
Pro-caspase-1
NALP1 Inflammasome earlier
IL1βPro- IL1βIL-1β activation
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
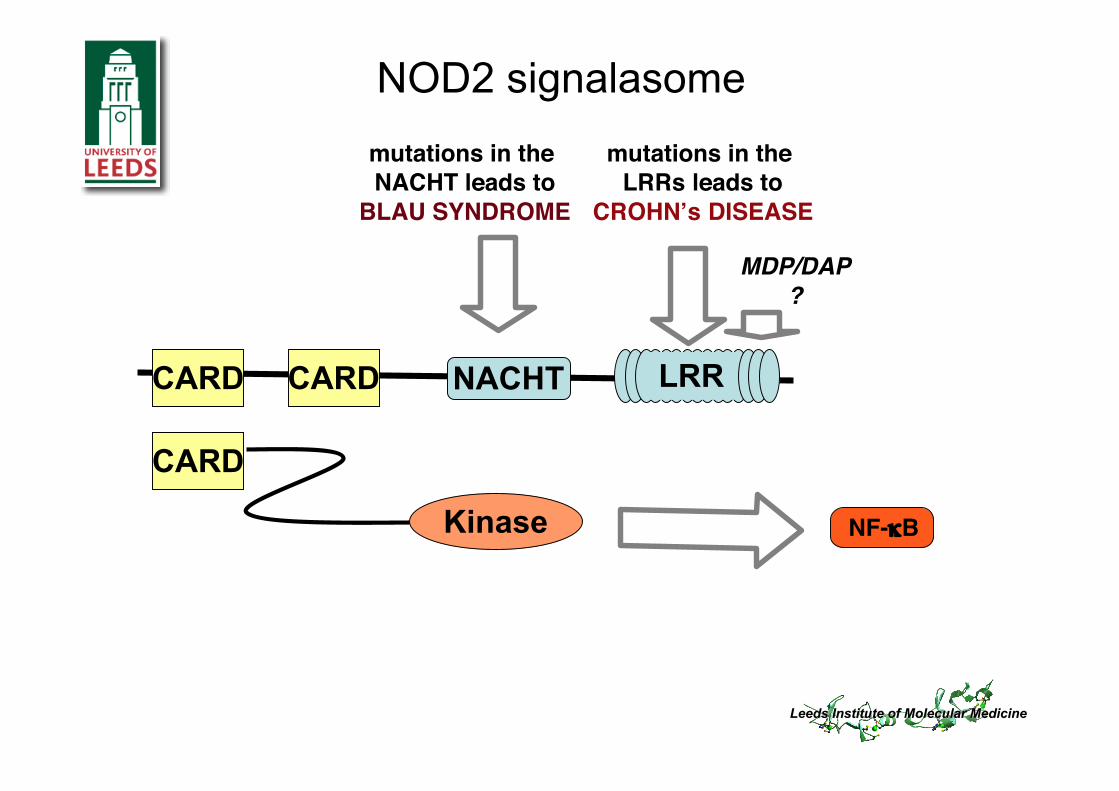
NACHT LRR
Kinase
CARD
NOD2 signalasome
CARD
CARD
NF-κB
MDP/DAP?
mutations in the LRRs leads to
CROHNʼs DISEASE
mutations in the NACHT leads to
BLAU SYNDROME
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
NALP3 Inflammasome
PYDCCSPRY bZIPPyrin
PYD NACHT LRRNALP3
CARDCaspase-1
CARD
Caspase-1
FIIND
CARDCardinal
MDPUric AcidATPCytosolic DNA
PYD
CARDASC
Pro-caspase-1
IL1βPro- IL1β
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
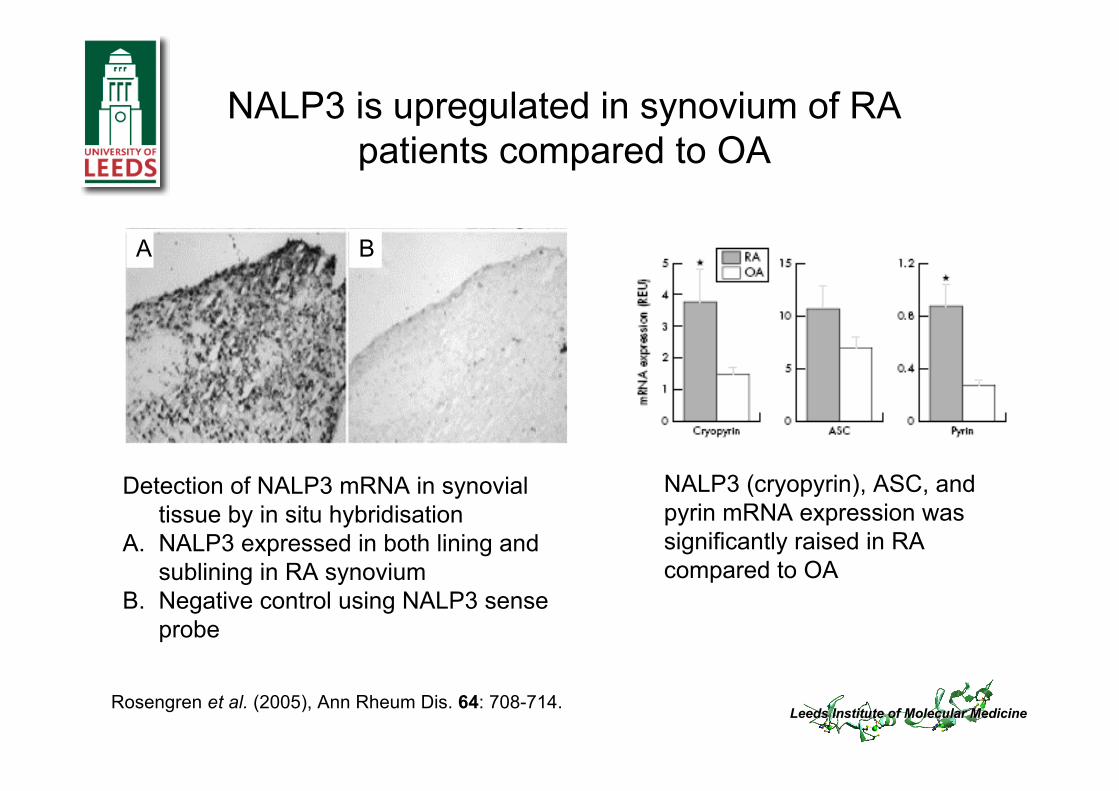
NALP3 is upregulated in synovium of RApatients compared to OA
Rosengren et al. (2005), Ann Rheum Dis. 64: 708-714.
NALP3 (cryopyrin), ASC, andpyrin mRNA expression wassignificantly raised in RAcompared to OA
Detection of NALP3 mRNA in synovialtissue by in situ hybridisation
A. NALP3 expressed in both lining andsublining in RA synovium
B. Negative control using NALP3 senseprobe
A B
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
DAS28 response criteria and methods
Bingham et al (2004), Rheumatology 43: 364-368
Wk 0 Wk 2 Wk 6 Wk 14
PBMC
mRNA
cDNA
qRT- PCR
ASC NALP3
Infliximab regime / sample collection
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
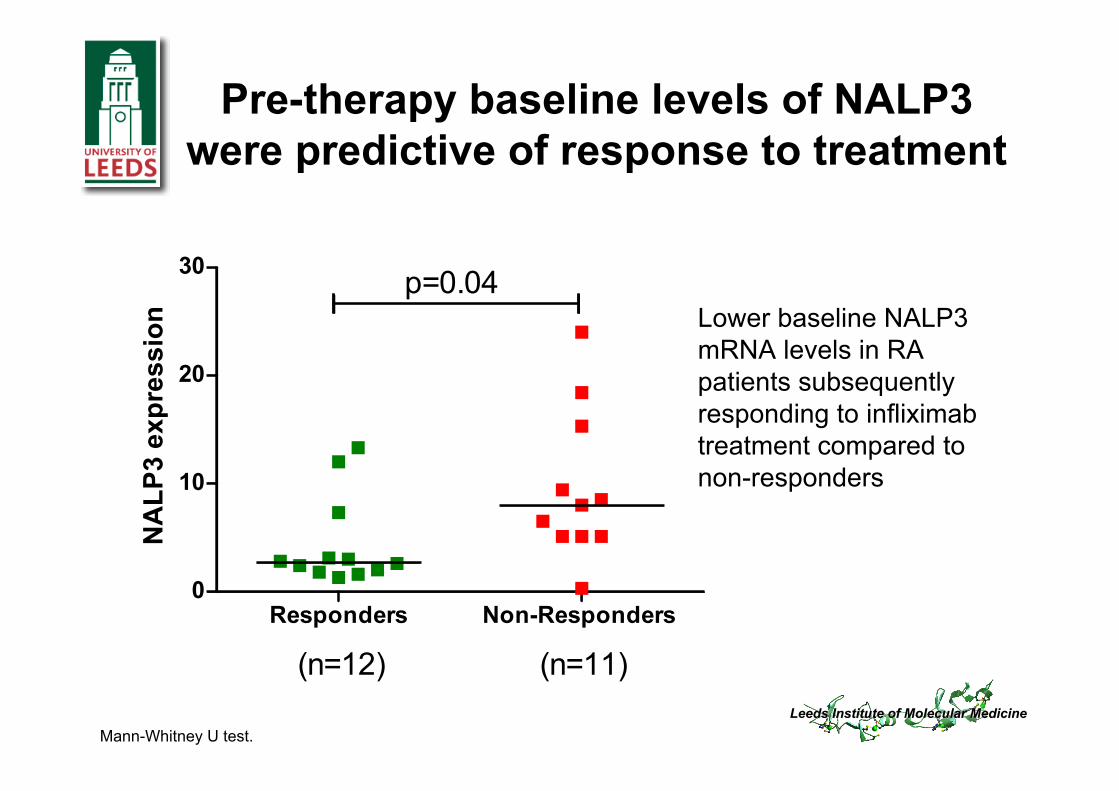
Pre-therapy baseline levels of NALP3were predictive of response to treatment
Lower baseline NALP3mRNA levels in RApatients subsequentlyresponding to infliximabtreatment compared tonon-responders
Mann-Whitney U test.
Responders Non-Responders 0
10
20
30
(n=12) (n=11)
p=0.04
NA
LP
3 e
xp
res
sio
n
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
NALP3 mRNA levels were furtherdecreased from baseline in response to
infliximab treatment
Week 0 Week 2 Week 140
5
10
15 p=0.007n=12
Time
NA
LP
3 e
xp
ressio
n
Wilcoxon signed-rank test
Week 0 Week 2 Week 140
10
20
30 n= 11
TimeN
AL
P3
ex
pre
ss
ion
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
Preliminary data suggest that infliximab alsoreduces NALP3 expression in the synovium
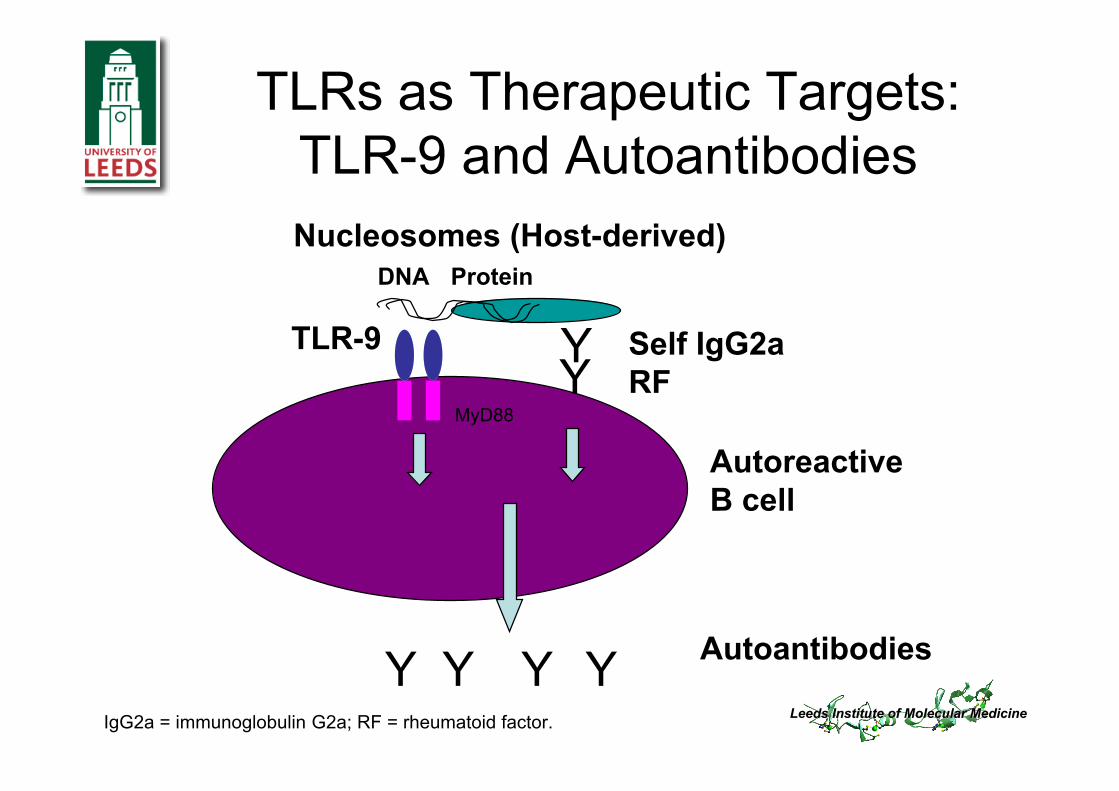
TLRs as Therapeutic Targets:TLR-9 and Autoantibodies
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
INDUCTION OF CO-STIMULATORY MOLECULES CD80/86INDUCTION OF TNF
Courtesy of Steffen Gay and colleagues
sense control probeanti-sense probe
Expression of TLR2 mRNA in RA synovialtissue
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
Toll-like Receptors
10 TLRs
MyD88 Mal Trif Tram
Products ofinflamed tissues
Modulation of immune and inflammatory genes
Immune and inflammatory effector mechanisms
Microbialproducts
NLRs
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
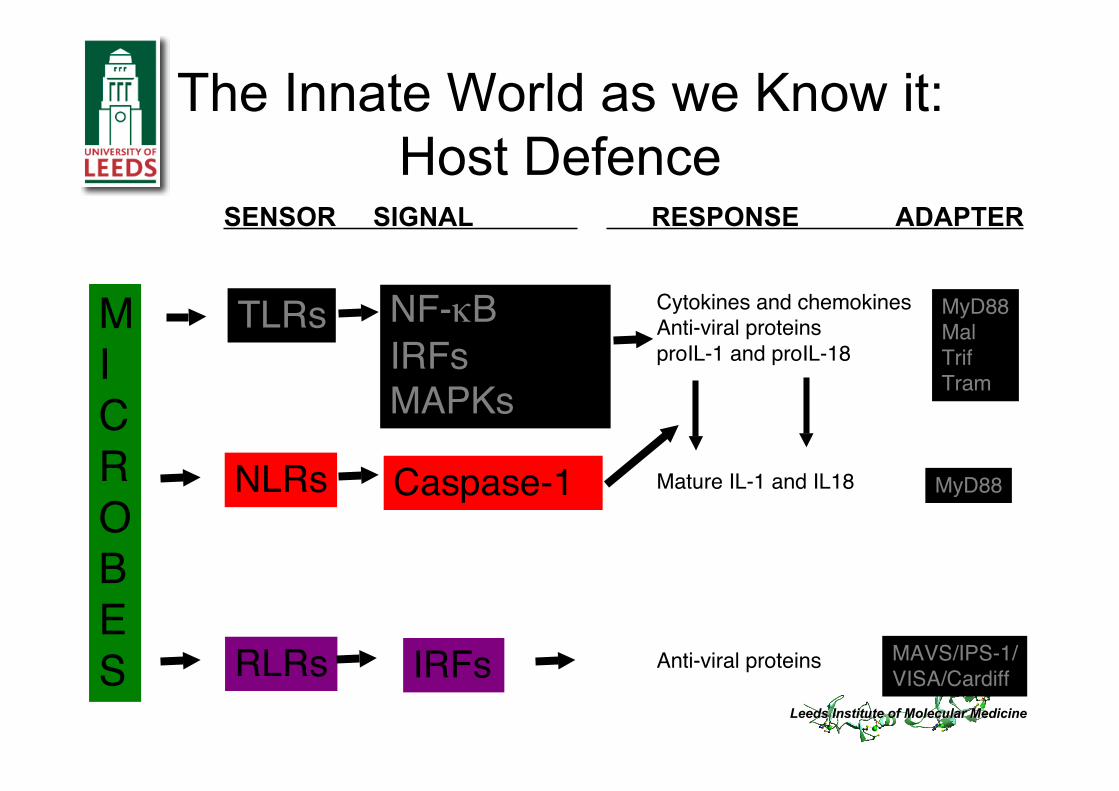
Cytokines and chemokinesAnti-viral proteinsproIL-1 and proIL-18
Mature IL-1 and IL18
Anti-viral proteins
MyD88MalTrifTram
MICROBES
TLRs
NLRs
RLRs
NF-κBIRFsMAPKs
Caspase-1
IRFs
MyD88
MAVS/IPS-1/VISA/Cardiff
SENSOR SIGNAL RESPONSE ADAPTER
The Innate World as we Know it:Host Defence
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
Why is Autoimmunity paradigmso strong?
• Approx 1,000,000, 000 T cell receptors in man• T cell clones expand x 64,000 in 4 days• Each activated Th1 cell attracts up to 1,000
macrophages• T cells stimulate macrophages to make IFN etc
• Repertoire- an almost unlimited number of epitopes
• Memory with secondary responses: occur sooner,steeper, faster, higher and with a lower lowerthreshold
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
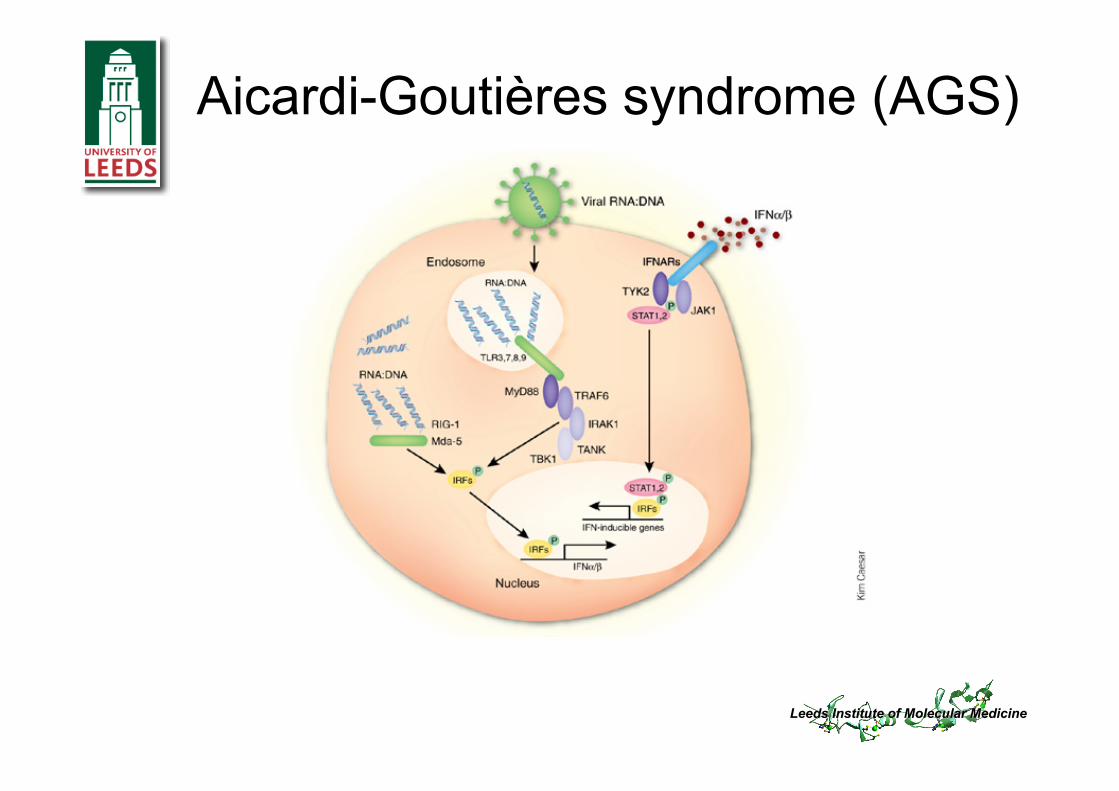
Aicardi-Goutières syndrome (AGS)
Leeds Institute of Molecular MedicineLeeds Institute of Molecular Medicine
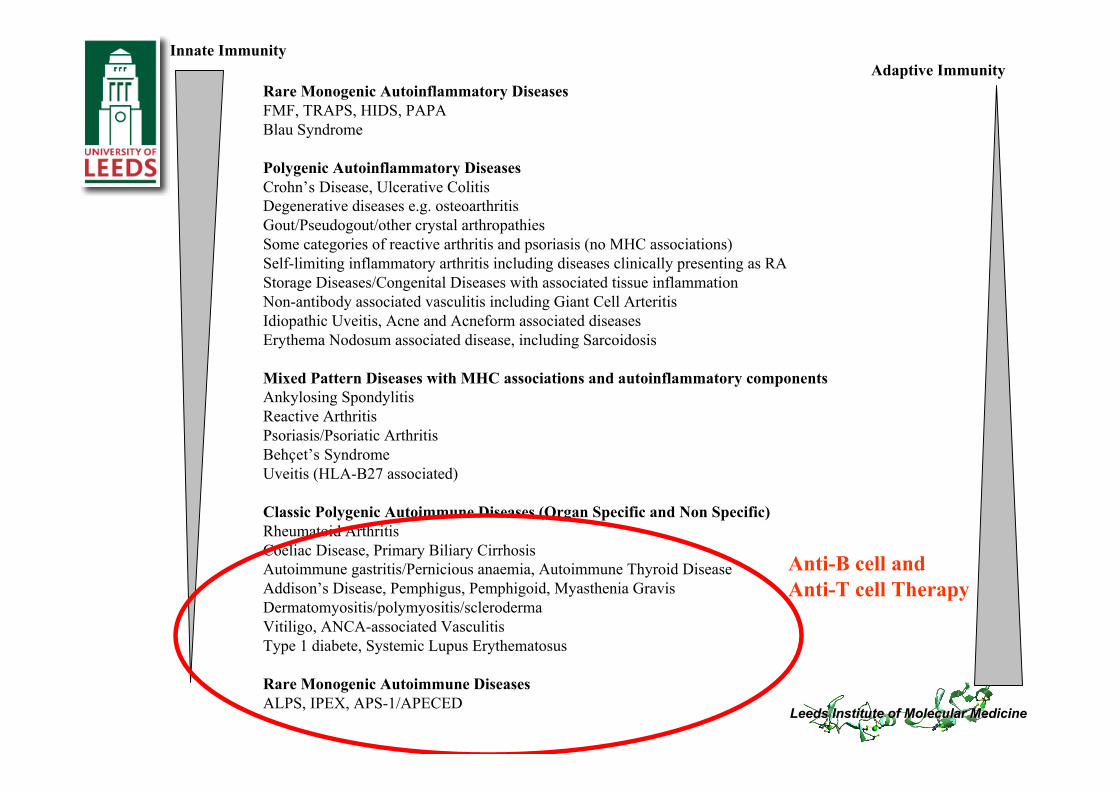
Adaptive vs innate immunity in rheumatoidarthritis
• Rheumatoid arthritis (RA) has traditionally been describedas an adaptive immune response, but, more recently, therehas been a gradual appreciation of the role of the innateimmune system
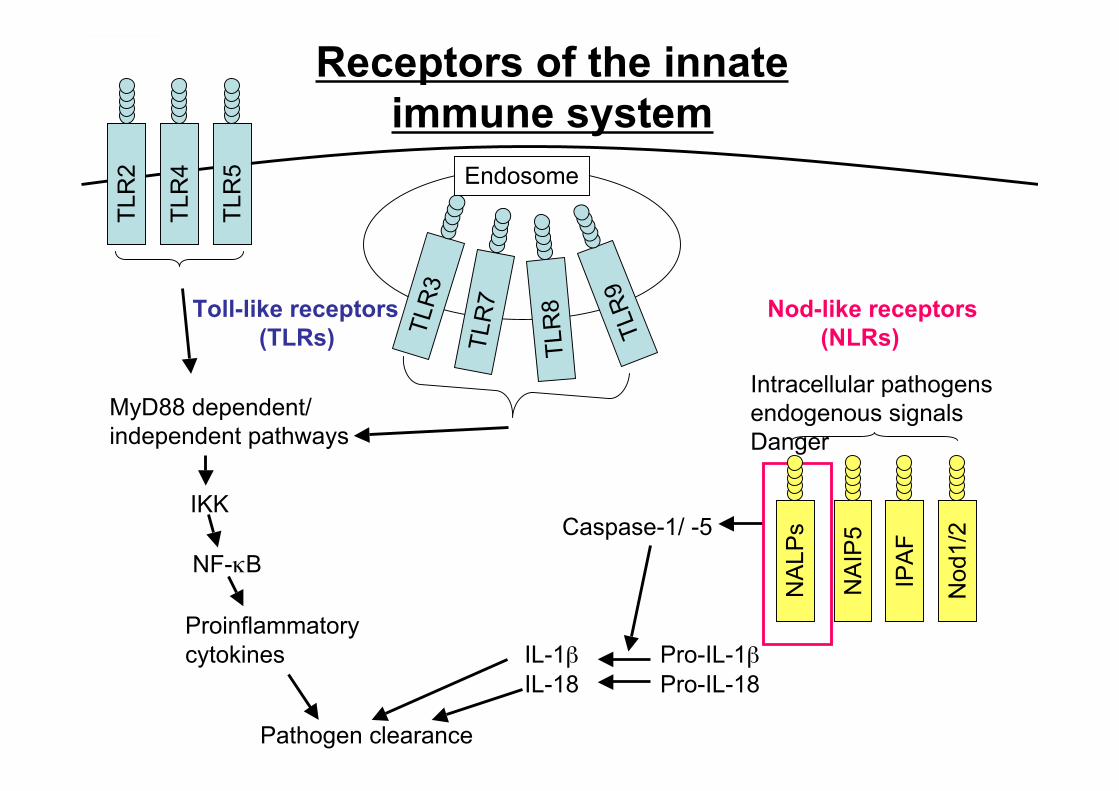
• The innate immune system recognises-microbial pathogen associated molecular patterns (PAMPs)-endogenous signals; danger associated molecular patterns (DAMPs)
• The detection of DAMPs and PAMPs is through Toll-likereceptors (TLRs) and Nod-like receptors (NLRs)