Inflammation and atherosclerosis Dr Khamis Al hashmi MD PhD. Assistant professor Department of Physiology and Clinical Physiology COM&HS, SQU IAS-OSLA Course “Lipid Metabolism and Cardiovascular Risk” Muscat, Oman, 8-10 February 2015
Transcript
Inflammation and atherosclerosis
Dr Khamis Al hashmi MD PhD.
Assistant professor
Department of Physiology and Clinical Physiology
COM&HS, SQU
IAS-OSLA Course “Lipid Metabolism and Cardiovascular Risk” Muscat, Oman, 8-10 February 2015
Outlines
• Process of Atherosclerosis
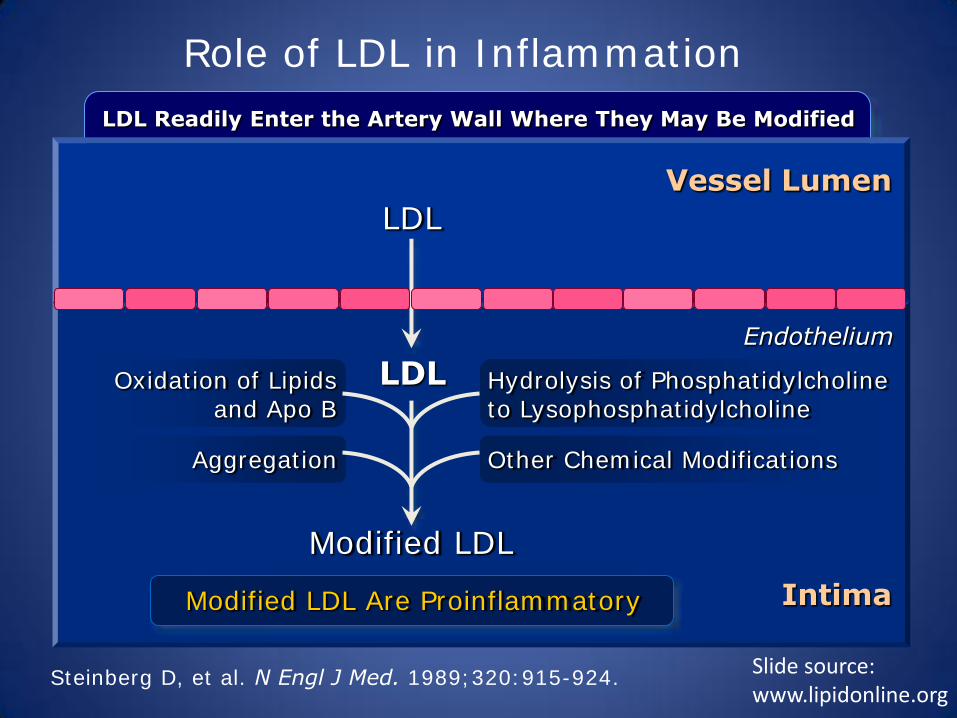
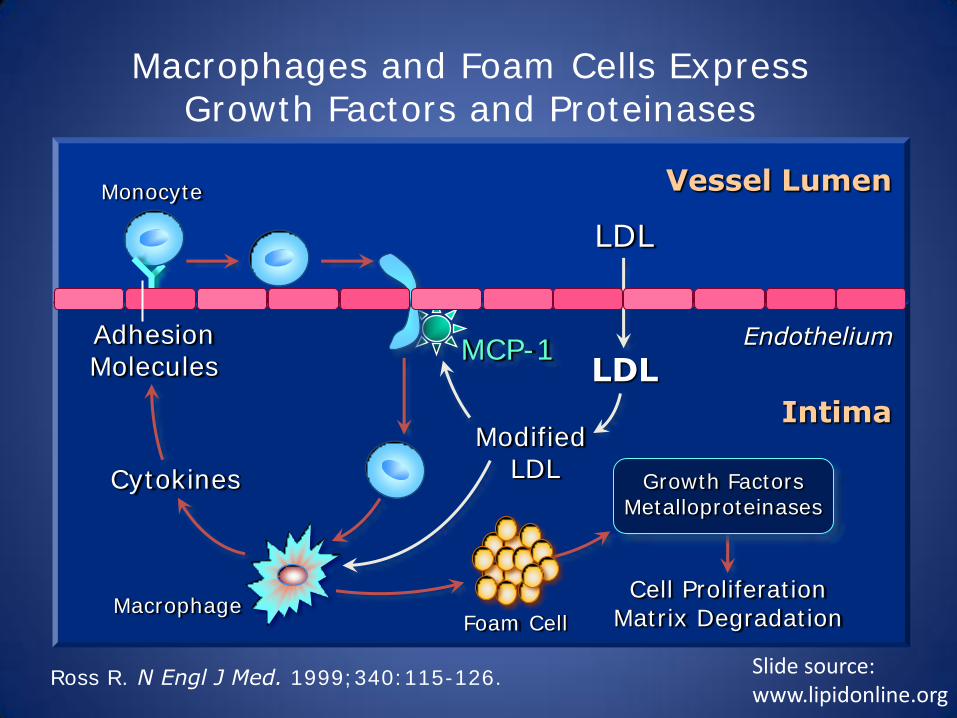
• Role of lipoproteins (LDL & VLDL) in inflammation
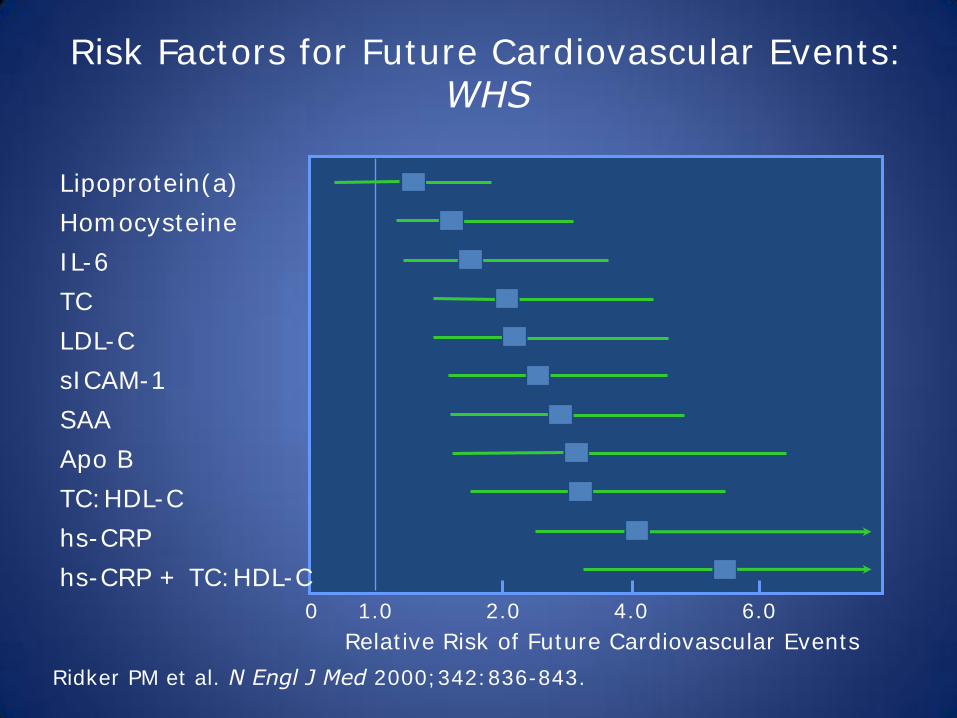
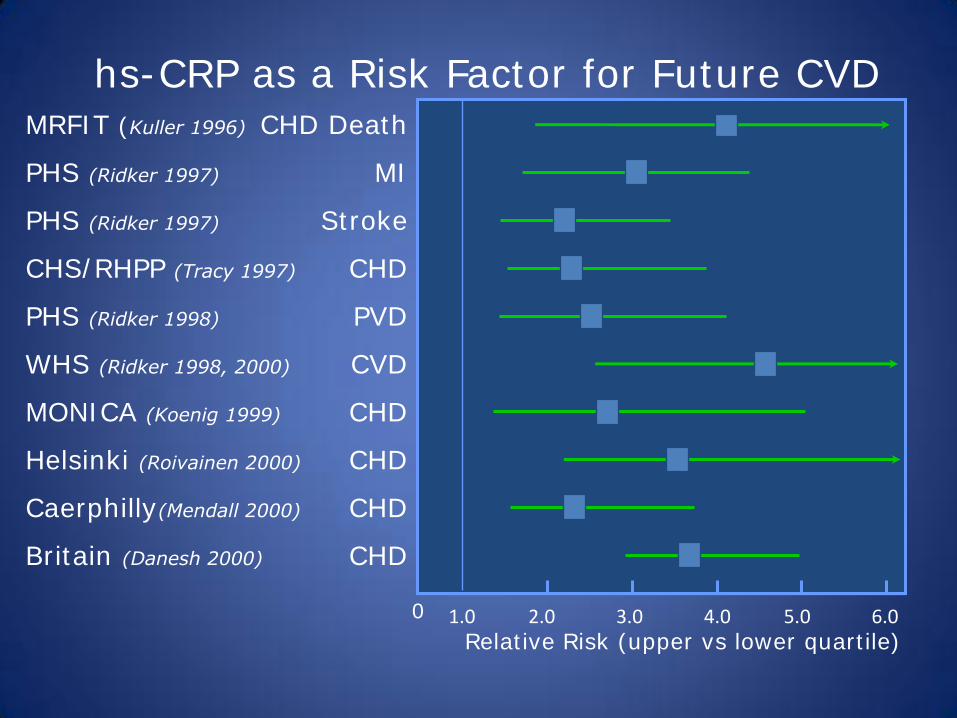
• Inflammatory marker as risk factors for CVD
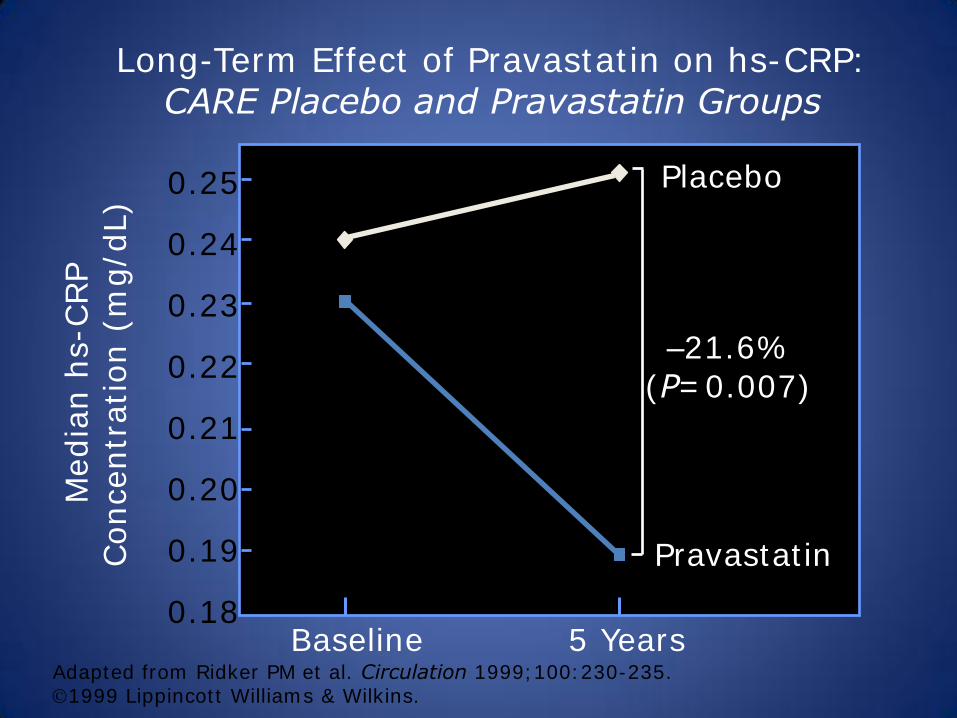
• Inflammatory markers as target for therapy
Atherosclerosis
• Disease of cardiovascular system affecting vessel wall.
• It leads to the narrowing of arteries or complete blockage.
• Its main components are endothelial disfunction, lipid deposition, inflammatory reaction in the vascular wall.
• Remodeling of vessel wall.
Atherosclerosis
• Intense cross-talk between EC, VSMC, plasma-derived inflammatory cells, lymphocytes (involves array of chemokines, cytokines, growth factors).
• Attraction of cells to the sites of atherosclerotic lesion.
• Migration, proliferation, apoptosis, excess production of extracellular matrix.
Arterial wall: structure and function
The development of atherosclerosis
• The key event – damage to the endothelium caused by excess of lipoproteins, hypertension, diabetes, components of cigarette smoke.
• Endothelium becomes more permeable to lipoproteins.
• Lipoproteins move below the endothelial layer (to intima).
• Endothelium loses its cell-repelent quality.
• Inflammatory cells move itno the vascular wall.
The development of atherosclerosis • Disfunctional endothelium express adhesion molecules –
selectins, mediated the „rolling“ interaction of cells. • The key molecule - vascular cell addhesion molecule-1
(VCAM-1) promotes monocytes adhesion (precursors of macrophages).
• Addhering cells are stimulated by monocyte chemoattractant protein-1 (MCP-1).
• Monocytes cross the endothelium, settle down in the intima.
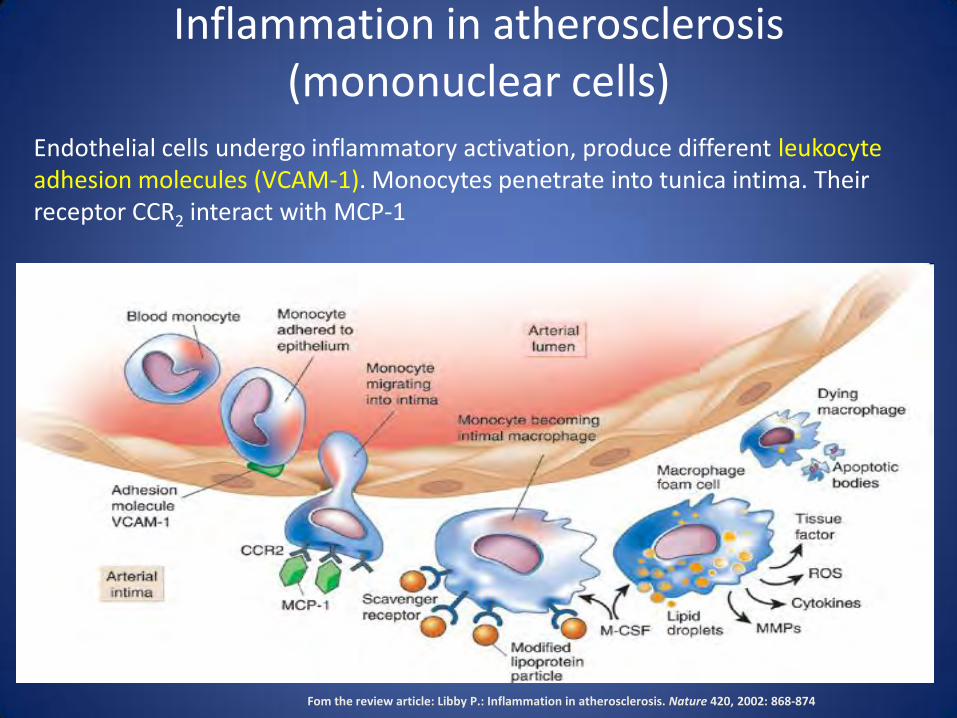
Inflammation in atherosclerosis (mononuclear cells)
Fom the review article: Libby P.: Inflammation in atherosclerosis. Nature 420, 2002: 868-874
Endothelial cells undergo inflammatory activation, produce different leukocyte adhesion molecules (VCAM-1). Monocytes penetrate into tunica intima. Their receptor CCR2 interact with MCP-1
Inflammation in atherosclerosis (T-lymhocytes)
Fom the review article: Libby P.: Inflammation in atherosclerosis. Nature 420, 2002: 868-874
T-lymphocytes enter the intima facilitated by VCAM-1 and trio chemokines- IP-10 (inducible protein-1), Mig (monokine induced by interferon-g) and I-TAC (interferon-inducible T-cells a-chemoattractant). Trio chemokines bind to CXCR3 chemokine receptor expressed by T-cells in the atherogenic lesion.
Inflammation in atherosclerosis (mast cells)
Fom the review article: Libby P.: Inflammation in atherosclerosis. Nature 420, 2002: 868-874
Mast cells infiltrate to the intima. Chemoattractant eotaxin mediate migration of mast cells and interacts with the chemokine receptor CCR3. Resident mast cells in the intima degranulate, release TNF-a, heparin, and enzymes activating proMMPs.
The process of atherogenesis – an overview
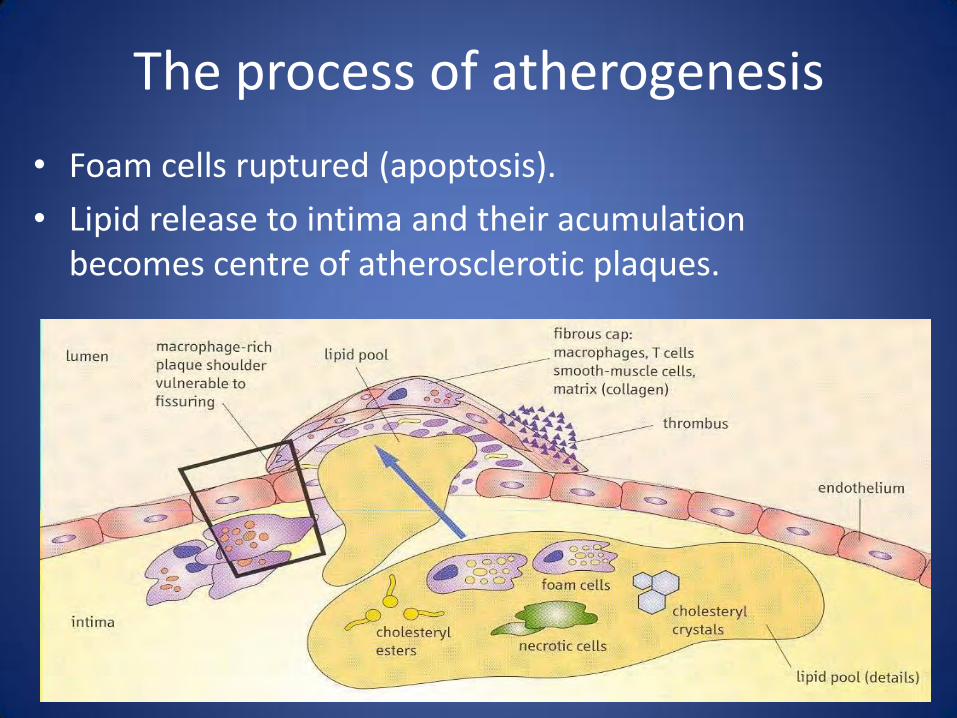
The process of atherogenesis
• Lipid entry into the arterial wall is a key process in atherogenesis.
• Hypercholesterolemia – factor for VCAM-1 and MCP-1 induction.
• LDL and VLDL are most atherogenic, enter vascular wall more easily.
• LDL – in plasma are protected against oxidation by vit. E, ubiquinon, plasma antioxidants (b-carotene, vit. C).
• Out of plasma, LDL phospholipides and fatty acids oxidize.