PRACTICAL GASTROENTEROLOGY • MAY 2011 20 A Review of Postoperative Crohn’s Disease INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71 Seymour Katz, M.D., Series Editor Clyde A. Collins Rachana Potru Jesse Green While surgical resection remains a mainstay of the treatment of Crohn’s disease (CD), postoperative recurrence of disease is common. The ideal management of patients after surgery is unclear and varies widely in clinical practice. Both patients and clinicians must weigh the risks and benefits of treatment in reaching a decision. Those at low risk of postoperative recurrence may not need any therapy while those at moderate risk of disease recurrence may be treated with immunomodulator therapy. Patients with the highest risk for recurrence should ideally be treated with biologic therapy. Regardless of risk, all patients should undergo ileocolonoscopic surveillance at 6–12 months after surgery. This review will outline the current evidence for various medical therapies in the prevention of postsurgical recurrence and outline a management algorithm of these patients based on risk stratification. INTRODUCTION C rohn’s disease is characterized by chronic inflam- mation often exacerbated by acute relapses. Surgery still plays a critical role in the manage- ment of this patient population, and postoperative care is challenging. Current therapy in Crohn’s disease is moving beyond the goal of induction and maintenance of remission. In addition to these standard outcome measures, successful management can also be quanti- fied by assessing the incidence of complications and measuring the patient’s quality of life. This paper dis- cusses (i) standard methods to identify recurrent Crohn’s disease, (ii) risk factors for recurrence, (iii) and review of postoperative medical management. BACKGROUND Despite medical treatment advancements with immunomodulators and biologic therapy, the failure of Clyde Collins, M.D., Fellow, of Gastroenterology; Rachana Potru, M.D., Fellow, of Gastroenterology; Jesse Green, M.D., F.A.C.G., Director of Endoscopy Unit, Associate Professor of Medicine, Division of Gastroenterology; all at The Albany Medical College, Albany, NY. (continued on page 22)
Transcript
PRACTICAL GASTROENTEROLOGY • MAY 201120
A Review of Postoperative Crohn’s Disease
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
Seymour Katz, M.D., Series Editor
Clyde A. Collins Rachana Potru Jesse Green
While surgical resection remains a mainstay of the treatment of Crohn’s disease (CD),postoperative recurrence of disease is common. The ideal management of patients aftersurgery is unclear and varies widely in clinical practice. Both patients and cliniciansmust weigh the risks and benefits of treatment in reaching a decision. Those at low riskof postoperative recurrence may not need any therapy while those at moderate risk ofdisease recurrence may be treated with immunomodulator therapy. Patients with thehighest risk for recurrence should ideally be treated with biologic therapy. Regardlessof risk, all patients should undergo ileocolonoscopic surveillance at 6–12 months aftersurgery. This review will outline the current evidence for various medical therapies inthe prevention of postsurgical recurrence and outline a management algorithm of thesepatients based on risk stratification.
INTRODUCTION
Crohn’s disease is characterized by chronic inflam-mation often exacerbated by acute relapses.Surgery still plays a critical role in the manage-
ment of this patient population, and postoperative careis challenging. Current therapy in Crohn’s disease ismoving beyond the goal of induction and maintenance
of remission. In addition to these standard outcomemeasures, successful management can also be quanti-fied by assessing the incidence of complications andmeasuring the patient’s quality of life. This paper dis-cusses (i) standard methods to identify recurrentCrohn’s disease, (ii) risk factors for recurrence, (iii)and review of postoperative medical management.
BACKGROUNDDespite medical treatment advancements withimmunomodulators and biologic therapy, the failure of
Clyde Collins, M.D., Fellow, of Gastroenterology;Rachana Potru, M.D., Fellow, of Gastroenterology;Jesse Green, M.D., F.A.C.G., Director of EndoscopyUnit, Associate Professor of Medicine, Division ofGastroenterology; all at The Albany Medical College,Albany, NY. (continued on page 22)
PRACTICAL GASTROENTEROLOGY • MAY 201122
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
A Review of Postoperative Crohn’s Disease
medical management is an indication for surgery totreat related complications (i.e., stricture and fistulaeformation). Seventy-five percent of patients willrequire surgical intervention at least once during theirlifetime (1). However, unlike ulcerative colitis, surgeryis not typically curative.
Resection of the diseased bowel is not curative andmost recurrences occur at the resection site or proxi-mal to the surgical anastomosis (2). After ileocolonicresection and anastomosis, endoscopic recurrence ofdisease arises in the neoterminal ileum in 30% ofpatients after 3 months (3), and has been reported asearly as 1 week after surgery (4). At one year, 70-90%of patients will have endoscopic evidence of recurrent
(continued from page 20)
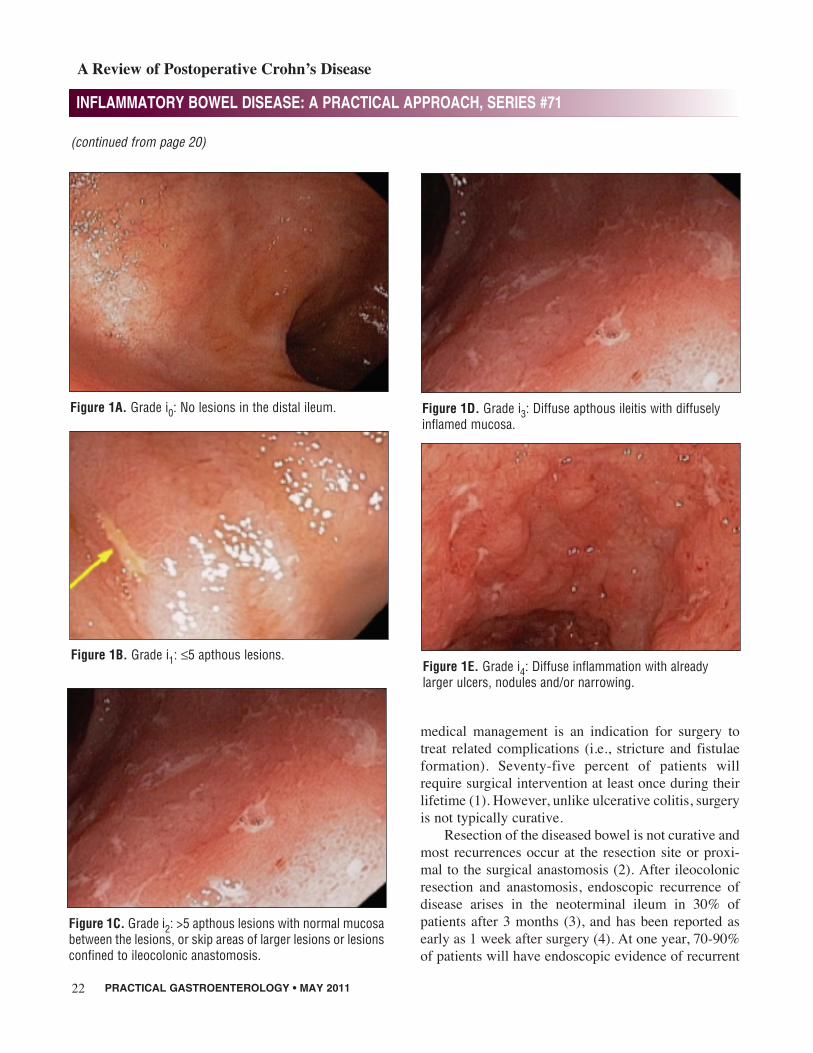
Figure 1A. Grade i0: No lesions in the distal ileum.
Figure 1B. Grade i1: ≤5 apthous lesions.
Figure 1C. Grade i2: >5 apthous lesions with normal mucosabetween the lesions, or skip areas of larger lesions or lesionsconfined to ileocolonic anastomosis.
Figure 1D. Grade i3: Diffuse apthous ileitis with diffuselyinflamed mucosa.
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
A Review of Postoperative Crohn’s Disease
disease (5). Clinical recurrence rates have beenreported to be as high as 20–30% at 1 year with a 10%increase in each of the subsequent years. The need forrepeat surgery occurs in 15–45% of patients at 3 years,26–65% at 10 years and 33–82% at 15 years (6).
DISEASE RECURRENCEAfter surgical resection, the use of ileocolonoscopyhas been the primary surveillance tool used to assessfor recurrence of Crohn’s disease. However, given theinvasive nature of ileocolonoscopy, alternative tech-niques have been evaluated to assess postoperativerecurrence. Transabdominal ultrasonography (TUS)has been proposed for detecting small bowel lesions inpatients with suspected or known CD, showing a sen-sitivity of 67%–84% and 81%–95%, respectively (7).In experienced hands, small intestine contrast ultra-sonography (SICUS) has been shown to detect intesti-nal lesions in patients with suspected small boweldiseases with a high (>95%) sensitivity and speci-ficity, when compared with small bowel follow-through and enema (8). SICUS has shown a significantcorrelation with the findings during endoscopy (7).
The Rutgeerts scoring system is the most widelyapplied, studied, and clinically established scoringsystem to predict endoscopic progression and clinicalrecurrence (Figure 1) (9). One-year endoscopic scoresof i0 or i1 correlate with a low risk of endoscopic pro-gression and with clinical recurrence rates of less than10% over 10 years. Endoscopic scores of i2 correlatewith clinical recurrence rates of 20% over 5 years,whereas scores of i3 and i4 correlate with clinicalrecurrence rates of 50–100% and a high likelihood ofrequiring reoperation (9).
The Crohn’s Disease Activity Index (CDAI) (10)has been used in medical trials with scores of <150being indicative of remission (Table 1). However, therehave been conflicting reports in regards to the utility ofthe CDAI as a measure of clinical recurrence. TheCDAI has also been shown to have poor agreementwith the prediction of endoscopic recurrence 1 yearafter surgery. In a study by Regueiro et al, patients whowere found to have endoscopic remission (i0, i1) andendoscopic recurrence (i2, i3, i4) had an identical meanCDAI score of (134). The sensitivity of CDAI (using athreshold of >200) for predicting 1-year postoperativerecurrence was only 33%, with a corresponding false-
Table 1.The Crohn’s Disease Activity Index (11)
Clinical or laboratory variable Weighting factor
Percentage deviation from standard weight. × 1Number of liquid or soft stools each day for seven days. × 2Abdominal pain (graded from 0–3 on severity) each day for seven days. × 5Absolute deviation of Hematocrit from 47% in men and 42% in women. × 6General well being, subjectively assessed from 0 (well) to 4 (terrible) each day for seven days. × 7Presence of an abdominal mass (0 as none, 2 as questionable, 5 as definite). × 10Presence of complications.* × 20Taking Lomitil or opiates for diarrhea. × 30
Modified table from the URL http://en.wikipedia.org/wiki/Crohn’s_Disease_Activity_Index and used under the following license http://creativecommons.org/licenses/by-sa/3.0/*One point each is added for each set of complications: • The presence of joint pains (arthralgia) or frank arthritis• Inflammation of the iris or uveitis• Presence of erythema nodosum, pyoderma gangrenosum, or aphthous ulcers• Anal fissures, fistulae or abscesses• Other fistulae• Fever (>100°F) during the previous week.
PRACTICAL GASTROENTEROLOGY • MAY 201124
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
A Review of Postoperative Crohn’s Disease
negative rate of 67%. This means approximately two-thirds of patients with objective endoscopic recurrencehad a CDAI <200 (most <150) and thus did not meetcriteria for clinical recurrence (5).
Another study reported a CDAI of ≥148 predictedrecurrence with a sensitivity of 70%, and specificity of81%. This study suggested that the CDAI is likely notsuitable for use as a primary outcome measure and acombination of symptom assessment plus endoscopicevidence of recurrence should remain the gold stan-dard definition for assessing outcomes (11).
RISK FACTORSThere are multiple risks factors that predisposepatients to disease recurrence. Factors such as the pres-ence of granulomas, perforating disease phenotype,ileal or ileocecal resection with ileocolic anastomosisand smoking have all been identified. In a multivariateanalysis, surgery for a perforating indication was anindependent predictor of early recurrence (14). Inaddition, recurrences requiring additional surgeryoccurred twice as fast in the perforating type as in thenonperforating type (12,13). However, the presence ofan ileocolic anastomosis and smoking are the onlywell-replicated predictors of postoperative recurrence,making prevention a challenging problem (6,14,15).
The pathogenesis of CD involves complex interac-tions between microbial, environmental, immunologi-cal, and genetic variables. Understanding theseinteractions provides the basis for understanding fac-tors, which influence disease recurrence. A dysregula-tion of the mucosal immune system leading to anexcessive immunologic response to normal microflorahas been well established. The composition of theintestinal microflora is complex. The evidence whichlinks bacterial flora and intestinal inflammationincludes an observation of a relatively high concentra-tions of bacteria (>10–12 organisms/g) in the normaldistal ileum and colon (4). In part, this may explain thepredominance of CD in these segments of the gas-trointestinal tract (4). An imbalance favoring morepathogenic organisms (Clostridia spp., Bacteroidesvulgatus and Escherichia) has been observed inmucosal biopsies during active inflammation. In animportant study, Rutgeerts et al, demonstrated that five
patients with CD who had undergone resection with adiverting loop ileostomy proximal to an ileocolic anas-tomosis had no endoscopic evidence of recurrence inthe neoterminal ileum 6 months after surgery (16).However, after bowel continuity was restored, essen-tially all patients displayed rapid endoscopic recur-rence in the neoterminal ileum. These findings suggestthat the diversion of bowel contents protects theneoterminal ileum from recurrent inflammation andthat bacterial flora and/or other components of thefecal stream play a key role in disease initiation (17).
The best defined and most important environmen-tal factor in CD is smoking. Smoking is strongly asso-ciated with a higher relapse rate, a more aggressivedisease course, and increased risk of postoperativerecurrence (18). A meta-analysis by Reese et al.demonstrated a twofold increase in clinical relapseafter surgery in smokers compared with non-smokers,as well as a 2.5-fold increase in the risk of furthersurgery by 10 years (19). Several explanations havebeen postulated to delineate the exact mechanism thatsmoking has on disease activity. These explanationsdescribe a direct immunosuppressive effect of smok-ing influencing cellular and humoral immunity (20).Another plausible explanation is that vascular changescaused by components of tobacco smoke (such as oxi-dizing chemicals) may have prothrombotic effectswhich in turn could exacerbate ischemia of the bowelwall (21). Other environmental factors, which mayhave an effect on disease activity, include medications.For example, oral contraceptives and nonsteroidalanti-inflammatory drugs (NSAIDs) have been studiedand found to be associated with disease relapse (22).
There have been several studies examining theassociation between genetic variants and surgical recur-rence in Crohn’s patients. The NOD2/CARD15 genevariants have been the most studied. The gene encodesa protein that functions as an intracellular sensor ofmuramyl-dipeptide, a bacterial cell wall component(23). Three common mutations within this gene lead toa compromised host immune response to enteric bacte-ria. A study by Büning et al reported a higher risk ofpostoperative relapse and reoperation, with 12 of 29patients (41.4%) with NOD2/CARD15 mutationsrequiring a second operation compared with only 2 of
(continued on page 26)
PRACTICAL GASTROENTEROLOGY • MAY 201126
12 patients (16.7%) without NOD2/CARD15 muta-tions (24). A later study by Alvarez-Lobos et al showedthat patients with NOD2/CARD15 variants underwentsurgery more frequently (OR 3.63; 95% CI 1.42 to9.27) and required surgery at an earlier time (25).
TREATMENTNumerous studies have emerged over the last twentyyears attempting to elucidate ideal prophylaxis andtreatment of postoperative recurrent Crohn’s Disease.The major agents that have been studied are the 5-Aminosalicylate agents, probiotics, antibiotics,immunomodulators, and biologic therapies. Thesestudies have yielded mixed results and as such, a uni-versally accepted management algorithm has not yetemerged. Here we will outline the available medicaltherapies, the major conclusions to date about efficacyand safety of each, and present a management algo-rithm based on the reviewed data.
The results of studies using 5-aminosalicylates forpost-operative Crohn’s disease have been varied. Thishas been partly due to studies using different end-points, particularly clinical versus endoscopic recur-rence, the latter being a more robust measurement ofdisease remission. A Cochrane group meta-analysisfound that twelve patients needed to be treated withmesalamine to prevent one clinical recurrence andeight patients be treated to prevent one endoscopicrecurrence (26). A more recent meta-analysis withadditional studies found that, while sulfasalazineoffered no benefit over placebo, mesalamine was moreeffective than placebo or no therapy with a numberneeded to treat (NNT) of ten patients (27). Of the 11randomized controlled trials included, most of themused clinical endpoints rather than endoscopic or radi-ologic endpoints.
A previously published meta-analysis also showedmesalamine decreased clinical but not endoscopicpostoperative Crohn’s disease recurrence (28). A mul-ticenter, double-blind, double-placebo randomizedcontrolled trial comparing efficacy of mesalamine andazathioprine in postoperative Crohn’s patients withmoderate or severe endoscopic recurrence showed nodifference at 1 year in rates of clinical relapse (29).Despite the most recent meta-analysis showing some
possible effect greater than placebo or no therapy, the5-ASA products are of questionable utility as thedemonstrated effect is quite small and was mainlyshown to decrease clinical but not endoscopic recur-rence. Therefore, mesalamine remains an option foruse in patients with a contraindication to immunosup-pression though is not the therapy of choice in postop-erative Crohn’s disease.
Although antibiotics such as metronidazole andornidazole have been shown to be effective in reducingseverity of endoscopic recurrence, these are not usefulfor long term administration due to toxicities (e.g. gas-trointestinal symptoms, neuropathy) (30,31).
Five studies of probiotic use to prevent postopera-tive Crohn’s disease recurrence were evaluated in theaforementioned Cochrane review. In this review, nodifference was found between placebo and probioticsin clinical or endoscopic recurrence (29).
The immunomodulators consist of 6-Mercaptop-urine (6-MP) and azathioprine (AZA). These agentsinhibit DNA synthesis, and are particularly effective atimpeding cells that are rapidly proliferating. Severalstudies have compared these agents to 5-aminosalicy-late products and placebo with evidence thatimmunomodulators are more effective in preventingpostoperative Crohn’s disease recurrence, though thedifference in effect appears limited.
In 2008 D’Haens et al. compared metronidazoleplus AZA versus metronidazole alone in postoperativeCrohn’s disease patients at high risk for recurrence(32). The control group received placebo for 12 monthswhereas the other group received additional AZA for12 months. At 12 months the patients treated with AZAhad significantly less endoscopic recurrence comparedto the placebo group. There was no significant differ-ence in adverse effects between the two groups.
Domenech et al. examined the effect of azathio-prine on a group of 56 postoperative Crohn’s diseasepatients who had undergone curative resection (33). Ofthese, the cumulative probability of endoscopic recur-rence was 44%, 69% and 82% at 1, 3 and 5 yearsrespectively. The paper concluded that AZA was effec-tive in delaying but not preventing endoscopic recur-rence of postoperative Crohn’s disease.
Recently a double blind, double dummy random-ized control trial studied the effects of azathioprine
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
A Review of Postoperative Crohn’s Disease
(continued from page 24)
versus mesalamine in patients less than two years post-operative from curative resection with endoscopicrecurrence. None of the 78 patients in the study hadclinical recurrence at the time of entry. At 12 months,none of the AZA patients had clinical recurrence com-pared to four of the mesalamine patients, a statisticallysignificant finding. Furthermore, while only one thirdof the mesalamine patients had a one-point drop inRutgeert’s score, two thirds exhibited such a drop inthe azathioprine group. Side effects led to cessation in22% of the AZA patients and none of the mesalaminepatients (30).
Knowledge of the efficacy of anti-TNF agents inmucosal healing led to the study of infliximab for bothprophylaxis and treatment of recurrence of Crohn’sdisease after surgical resection. The first study todemonstrate the potential of infliximab was performedby Sorentino et al. (34). Twenty-three patients who hadundergone surgical resection for Crohn’s disease werestudied and 16 received mesalamine and sevenreceived infliximab and methotrexate. At 2 years aftersurgery, patients in the mesalamine group had a 75%endoscopic recurrence rate and the infliximab-methotrexate group experienced a 0% recurrence rate.
The only randomized controlled trial of infliximabtherapy to date for postoperative recurrence comparedinfliximab and placebo. The 24 patients in this studywere permitted to remain on stable preoperative dosesof immunomodulators and 5-aminosalicylate productsbut not steroids or antibiotics. Infliximab was initiatedwithin 4 weeks of surgery in the treatment group.Endoscopic recurrence at 1 year was significantlylower in the infliximab group at 9.1% compared to84.6% in the placebo group (p = .0006) (35). Histo-logic recurrence rate at 1 year was similarly signifi-cantly lower in the infliximab group at 27.3% versus84.6% in the placebo group. Adverse events were sim-ilar in frequency between the two groups.
Infliximab has also been studied in the treatmentof patients with established disease recurrence aftersurgery. Yamamoto et al. divided a group of 26patients who were clinically asymptomatic with endo-scopic recurrence at 6 months after resection. Thegroups were treated with either mesalamine, azathio-prine, or infliximab. At 6 months endoscopic diseasewas improved in 75% of the infliximab group patients,
38% of those on azathioprine and 0% in themesalamine group (p = .006) (36).
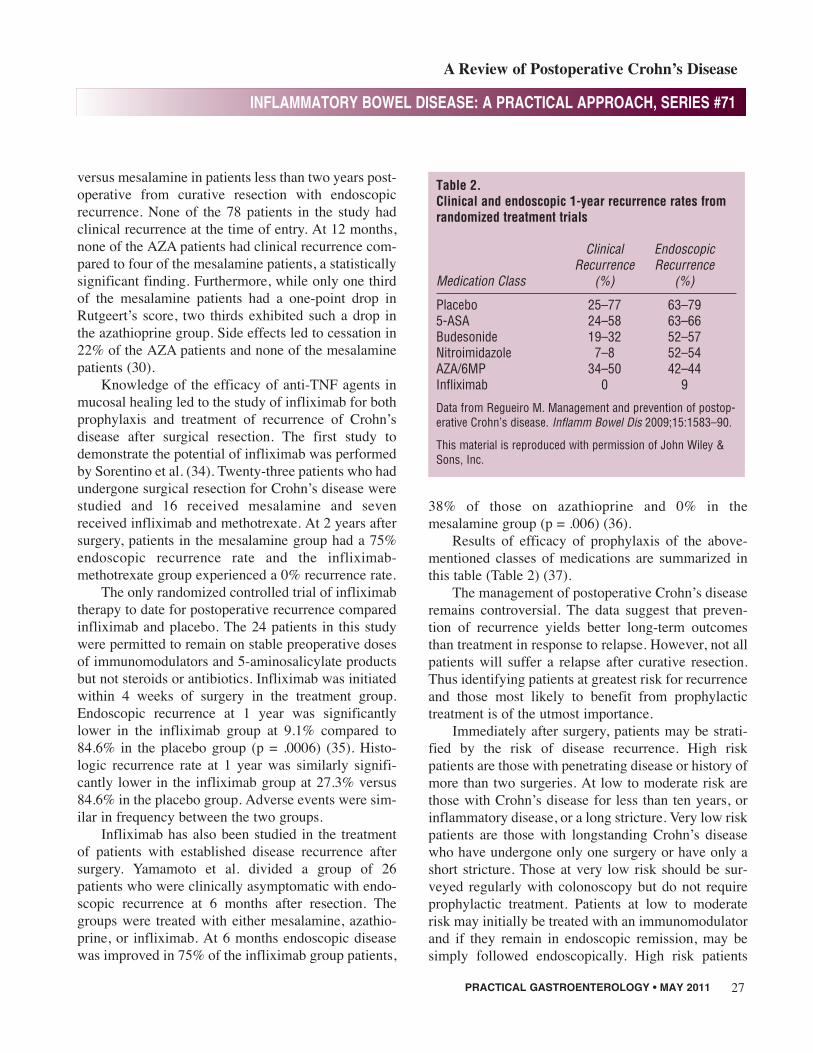
Results of efficacy of prophylaxis of the above-mentioned classes of medications are summarized inthis table (Table 2) (37).
The management of postoperative Crohn’s diseaseremains controversial. The data suggest that preven-tion of recurrence yields better long-term outcomesthan treatment in response to relapse. However, not allpatients will suffer a relapse after curative resection.Thus identifying patients at greatest risk for recurrenceand those most likely to benefit from prophylactictreatment is of the utmost importance.
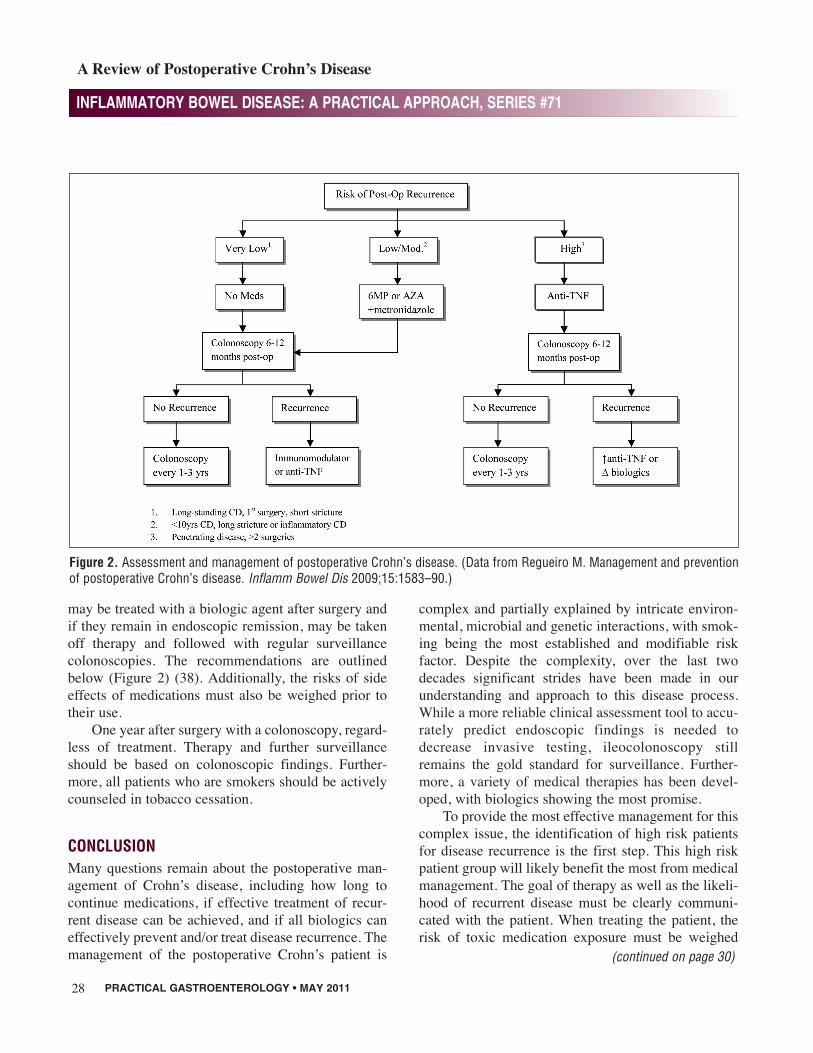
Immediately after surgery, patients may be strati-fied by the risk of disease recurrence. High riskpatients are those with penetrating disease or history ofmore than two surgeries. At low to moderate risk arethose with Crohn’s disease for less than ten years, orinflammatory disease, or a long stricture. Very low riskpatients are those with longstanding Crohn’s diseasewho have undergone only one surgery or have only ashort stricture. Those at very low risk should be sur-veyed regularly with colonoscopy but do not requireprophylactic treatment. Patients at low to moderaterisk may initially be treated with an immunomodulatorand if they remain in endoscopic remission, may besimply followed endoscopically. High risk patients
PRACTICAL GASTROENTEROLOGY • MAY 2011 27
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
A Review of Postoperative Crohn’s Disease
Table 2.Clinical and endoscopic 1-year recurrence rates fromrandomized treatment trials
Data from Regueiro M. Management and prevention of postop-erative Crohn’s disease. Inflamm Bowel Dis 2009;15:1583–90.
This material is reproduced with permission of John Wiley &Sons, Inc.
PRACTICAL GASTROENTEROLOGY • MAY 201128
may be treated with a biologic agent after surgery andif they remain in endoscopic remission, may be takenoff therapy and followed with regular surveillancecolonoscopies. The recommendations are outlinedbelow (Figure 2) (38). Additionally, the risks of sideeffects of medications must also be weighed prior totheir use.
One year after surgery with a colonoscopy, regard-less of treatment. Therapy and further surveillanceshould be based on colonoscopic findings. Further-more, all patients who are smokers should be activelycounseled in tobacco cessation.
CONCLUSIONMany questions remain about the postoperative man-agement of Crohn’s disease, including how long tocontinue medications, if effective treatment of recur-rent disease can be achieved, and if all biologics caneffectively prevent and/or treat disease recurrence. Themanagement of the postoperative Crohn’s patient is
complex and partially explained by intricate environ-mental, microbial and genetic interactions, with smok-ing being the most established and modifiable riskfactor. Despite the complexity, over the last twodecades significant strides have been made in ourunderstanding and approach to this disease process.While a more reliable clinical assessment tool to accu-rately predict endoscopic findings is needed todecrease invasive testing, ileocolonoscopy stillremains the gold standard for surveillance. Further-more, a variety of medical therapies has been devel-oped, with biologics showing the most promise.
To provide the most effective management for thiscomplex issue, the identification of high risk patientsfor disease recurrence is the first step. This high riskpatient group will likely benefit the most from medicalmanagement. The goal of therapy as well as the likeli-hood of recurrent disease must be clearly communi-cated with the patient. When treating the patient, therisk of toxic medication exposure must be weighed
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71
A Review of Postoperative Crohn’s Disease
(continued on page 30)
Figure 2. Assessment and management of postoperative Crohn’s disease. (Data from Regueiro M. Management and preventionof postoperative Crohn’s disease. Inflamm Bowel Dis 2009;15:1583–90.)
PRACTICAL GASTROENTEROLOGY • MAY 201130
against the benefits of significant morbidity reduction.The interpretation of a significant morbidity reductionwill vary between patients, thus a clear understandingof the patient expectations by the Gastroenterologist isneeded to guide appropriate future management. n
References1. Bennell O, Lapidus A, Hellers G. Risk factors for surgery and
postoperative recurrence in Crohn’s disease. Ann Surg2000;231:38–45.
2. Swoger JM, Regueiro M. Postoperative Crohn’s disease: how canwe prevent it? Expert Rev Clin Immunol. 2010 Jul;6(4):501-4.
3. Van Assche G, Rutgeerts P. Medical management of postopera-tive recurrence in Crohn’s disease. Gastroenterol Clin North Am2004;33:347-60.
4. D’Haens G, Geboes K, Peeters M, et al. Early lesions of recurrentCrohn’s disease caused by infusion of intestinal contents inexcluded ileum. Gastroenterology. 1998;114:262–267.
5. Regueiro M, Kip KE, Schraut W, Baidoo L, Sepulveda AR, PesciM, El-Hachem S, Harrison J, Binion D. Crohn’s disease activityindex does not correlate with endoscopic recurrence one yearafter ileocolonic resection. Inflamm Bowel Dis. 2010 May 27.
6. Rutgeerts P. Strategies in the prevention of post-operative recur-rence in Crohn’s disease. Best Pract Res Clin Gastroenterol2003;17:63-73.
7. Calabrese E, Petruzziello C, Onali S, Condino G, Zorzi F, PalloneF, Biancone L. Severity of postoperative recurrence in Crohn’sdisease: correlation between endoscopic and sonographic find-ings. Inflamm Bowel Dis. 2009 Nov;15(11):1635-42.
8. Calabrese E, La Seta F, Buccellato A, et al. Crohn’s disease: acomparative prospective study of transabdominal ultrasonogra-phy, small intestine contrast ultrasonography, and small bowelenema. Inflamm Bowel Dis. 2005;11:139–145.
9. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R,Hiele M. Predictability of the postoperative course of Crohn’sdisease. Gastroenterology.1990;99:956-983.
10. Best WR, Becktel JM, Singleton JW, Kern F Jr. “Development ofa Crohn’s disease activity index. National Cooperative Crohn’sDisease Study”. Gastroenterology 70 (3): 439–44. Mar 1976.
11. Walters TD, Steinhart AH, Bernstein CN, Tremaine W, McKen-zie M, Wolff BG, McLeod RS. Validating Crohn’s disease activ-ity indices for use in assessing postoperative recurrence. InflammBowel Dis. 2010 Nov 15.
12. Greenstein AJ, Lachman P, Sachar DB, et al. Perforating andnon-perforating indications for repeated operations in Crohn’sdisease: evidence for two clinical forms. Gut 1988;29:588–92.
13. Lautenbach E, Berlin JA, Lichtenstein GR. Risk factors for earlypostoperative recurrence of Crohn’s disease. Gastroenterology1998;115:259–67.
14. Cullen G, O’toole A, Keegan D, et al. Long-term clinical resultsof ileocecal resection for Crohn’s disease. Inflamm Bowel Dis2007;13:1369-73.
15. Unkart J, Anderson L, Li E, et al. Risk factors for surgical recur-rence after ileocolic resection of Crohn’s disease. Dis Colon Rec-tum 2008;51:1211-16.
16. Rutgeerts P, Goboes K, Peeters M, et al. Effect of faecal streamdiversion on recurrence of Crohn’s disease in the neoterminalileum. Lancet 1991;338:771-4.
17. Ahmed T, Rieder F, Fiocchi C, et al. Gut (2010). doi:10.1136/Gut 2010.221705.
18. Bernstein C, Rawsthorne P, Cheang M, et al. A population-basedcase control study of potential risk factors for IBD. Am J Gas-troenterol 2006;101:993-1002.
19. Reese G, Nanidis T, Borysiewicz C, et al. The effect of smokingafter surgery for Crohn’s disease: a meta-analysis of observa-tional studies. Int J Colorectal Dis 2008;12:1213-21.
20. Lindberg E, Jarnerot G, Huitfeldt B. Smoking in Crohn’s disease:effect on localization and clinical course. Gut 1992;33:779-82.
21. Cottone M, Rosselli M, Orlando A, et al. Smoking habits andrecurrence in Crohn’s disease. Gastroenterology 1994;106:643-8.
22. Danese S, Sans M, Fiocchi C. Inflammatory bowel disease: therole of environmental factors. Autoimmun Rev 2004;3:394-400.
23. Sehgal, Rishabh M.B., B.Ch et al NOD2/CARD15 MutationsCorrelate With Severe Pouchitis After Ileal Pouch-Anal Anasto-mosis Diseases of the Colon & Rectum: November 2010, Volume53, Issue 11, pp 1487-1494.
24. Büning C, Genschel J, Bu¨hner S, et al. Mutations in theNOD2/CARD15 gene in Crohn’s disease are associated withileocecal resection and are a risk factor for reoperation. AlimentPharmacol Ther 2004;19:1073-8.
25. Alvarez-Lobos M, Arostegui JI, Sans M, et al. Crohn’s diseasepatients carrying NOD2/CARD15 gene variants have anincreased and early need for first surgery due to stricturing dis-ease and higher rate of surgical recurrence. Ann Surg2005;242:693-700.
26. Doherty G, Bennett G, Patil S, et al. Interventions for preventionof postoperative recurrence of Crohn’s Disease. Cochrane Database Syst Rev 2009; Art. No.: CD006873. Doi:10.1002/14651858.CD006873.pub
27. Ford AC, Khan KJ, Talley NJ, Moayyedi P. 5-Aminosalicylatesprevent relapse of Crohn’s disease after surgically induced remis-sion: systematic review and meta-analysis. Am J Gastro 2010Epub.
28. Doherty GA, Bennett G, Patil S, et al. Meta-analysis ofmesalamine in the prevention of postoperative recurrence ofCrohn’s disease. Gastroenterology 2009; 136 (Suppl 1):A-522.
29. Reinisch W, Angelberger S, Petritsch W, et al.: Azathioprine ver-sus mesalazine for prevention of postoperative clinical recurrencein patients with Crohn’s disease with endoscopic recurrence: effi-cacy and safety results of a randomized, double-blind, double-dummy, multicentre trial. Gut 2010, 59:752-759.
30. Rutgeerts P, Hiele M., Geboes K, et al.: Controlled trial ofmetronidazole treatment for prevention of Crohn’s recurrenceafter ileal resection. Gastroenterology 1995, 108:1617-1621.
31. Rutgeerts P, Van Assche G, Vermeire S, et al.: Ornidazole forprophylaxis of postoperative Crohn’s disease recurrence: a ran-domized, double-blind, placebo-controlled trial. Gastroenterol-ogy 2005, 128:856-861.
32. D’Haaens GR, Vermeire S, Van Assche G, et al.: Therapy ofmetronidazole with azathioprine to prevent postoperative clinicalrecurrence in patients with Crohn’s disease: a controlled random-ized trial. Gastroenterology 2008, 135:112-1129.
33. Domenech E, Manosa M, Vernal I, et al. Impact of azathioprinetherapy on the prevention of postoperative Crohn’s disease recur-rence: results of a prospective, observational, long-term follow-up study. Inflamm Bowel Dis 2008;14:508-513.
34. Sorrentino D, Terrosu G, Avellini C, et al. Infliximab with low-dose methotrexate for prevention of postsurgical recurrence ofileocolonic Crohn’s disease. Arch Intern Med 2007; 167:1804-1807.
35. Regueiro M, Schraut W, Baidoo L, et al. Infliximab preventsCrohn’s disease recurrence after ileal resection. Gastroenterology2009; 136:441-450.
36. Yamamoto T, Umegae S, Matsumoto K. Impact of infliximabtherapy after early endoscopic recurrence following ileocolonicresection of Crohn’s disease: a prospective pilot study. InflammBowel Dis 2009; 15:1460-1466.
37. Regueiro M. Management and prevention of postoperativeCrohn’s disease. Inflamm Bowel Dis 2009;1583-1590.
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #71