Inflammatory Stress and Models of Idiosyncratic DILI Robert A. Roth, PhD, DABT Dept. of Pharmacology and Toxicology Center for Integrative Toxicology Michigan State University [email protected]517-353-9841 Why DILI Idiosyncrasy? The Immune System and Beyond ... March 14-15, 2012
Transcript
Inflammatory Stress and Models of Idiosyncratic DILI
Robert A. Roth, PhD, DABTDept. of Pharmacology and ToxicologyCenter for Integrative Toxicology
Why DILI Idiosyncrasy? The Immune System and Beyond ...March 14-15, 2012
Presenter
Sticky Note
Thank you, Mark. And I would like to thank the organizers and Dr. Senior for inviting me here to talk about my work. I was here last year talking about somebody else's work. So, this is a new thing for me in this group. Therefore, I put together kind of a general talk. Some of you have probably heard this before, but I figured I couldn't cover everything in 20 minutes. So, those of you who have heard it before can, I guess, kind of tune out. And I thought I would start with a definition again. I think Dr. Senior talked about this a bit yesterday.
• Idiosyncratic adverse drug response (IADR) = an adverse reaction that occurs in a minority of patients as a result of drug therapy.
• Implication: occurrence is governed by susceptibility factors within individuals.
• Characteristics of IADRs:– Usually affect a small fraction of people;
– Occur at doses that do not cause toxicity in most people;
– Have inconsistent temporal relationship to exposure;
– Are generally not reproducible in typical animal tests.
“Idiosyncratic” Reactions:
Presenter
Sticky Note
But in terms of idiosyncratic reactions, there are a lot of different definitions if you take your pharmacology texts off the wall and look at them. The way we define this is just simply an adverse reaction that occurs in a minority of patients as a result of drug therapy. The implication here is that these reactions are governed by susceptibility factors within individuals, as we have already heard. Having said that, these reactions have a number of characteristics. They usually occur, although not always, in a small fraction of people, they occur at doses that don't cause toxicity in the majority of individuals. They have an inconsistent temporal relationship to exposure. So, for some drugs, people get these reactions very soon after starting on drug therapy and others much later. And they are generally not reproducible in the typical animal tests that are used for preclinical drug testing.
– Drug metabolism polymorphism hypothesis
– Adaptive immunity hypothesis
– Transporter polymorphism hypothesis
– Multiple determinant hypothesis
– Pharmacological interaction hypothesis
– Mitochondrial toxicity hypothesis
– Failure-to-adapt hypothesis
– Inflammatory stress hypothesis
We really don’t know what causes these reactions: Many hypotheses, no thoroughly convincing proof!
Modes of Action of Idiosyncratic Drug-induced Liver Injury (IDILI)?
Presenter
Sticky Note
There have been a number of hypotheses put forward about the mechanisms and the modes of action of idiosyncratic reactions. We heard yesterday a lot about the adaptive immunity hypothesis. I am not going to read through this list for you, but just to say that after each of them is the word "hypothesis". I do think it is true that we really don't know what causes these reactions. There's a lot of hypotheses and no thoroughly-convincing proof. I am going to be talking about the inflammatory stress hypothesis, the last one on this list, but I am open-minded enough to believe that there are a lot of different ways in which the idiosyncratic reactions can occur.
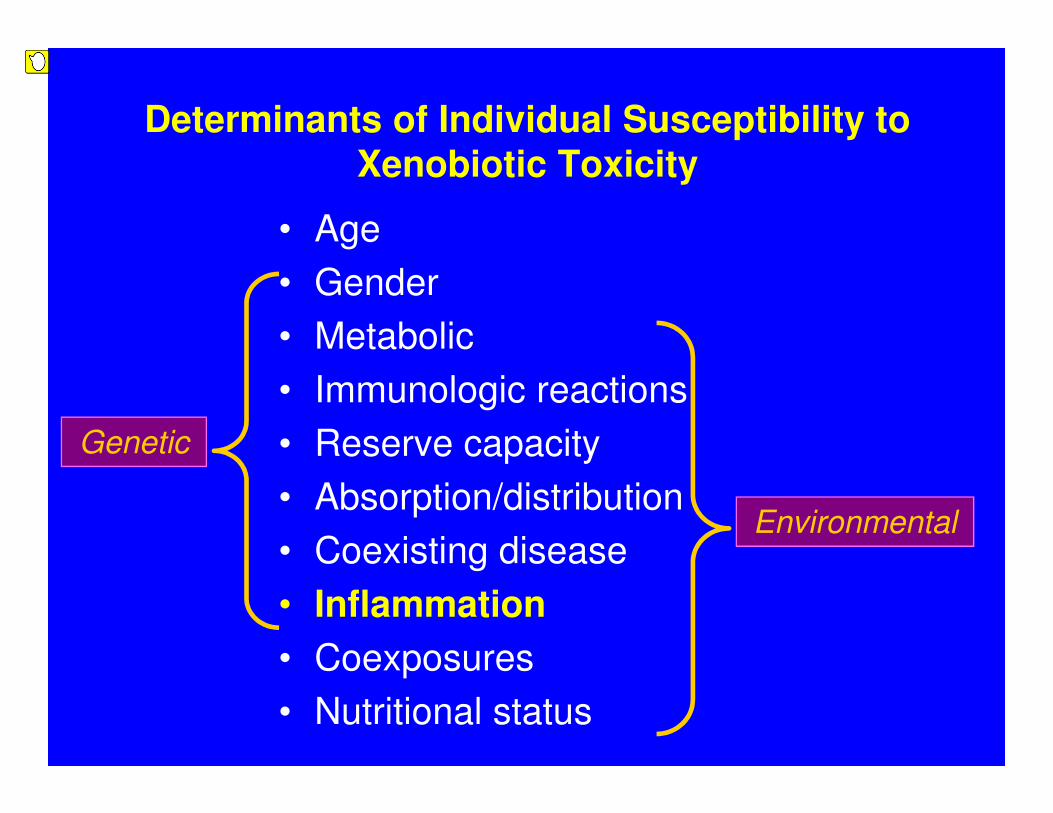
Determinants of Individual Susceptibility to Xenobiotic Toxicity
• Age
• Gender
• Metabolic
• Immunologic reactions
• Reserve capacity
• Absorption/distribution
• Coexisting disease
• Inflammation
• Coexposures
• Nutritional status
Environmental
Genetic
Presenter
Sticky Note
And more than one may even apply to a single drug.
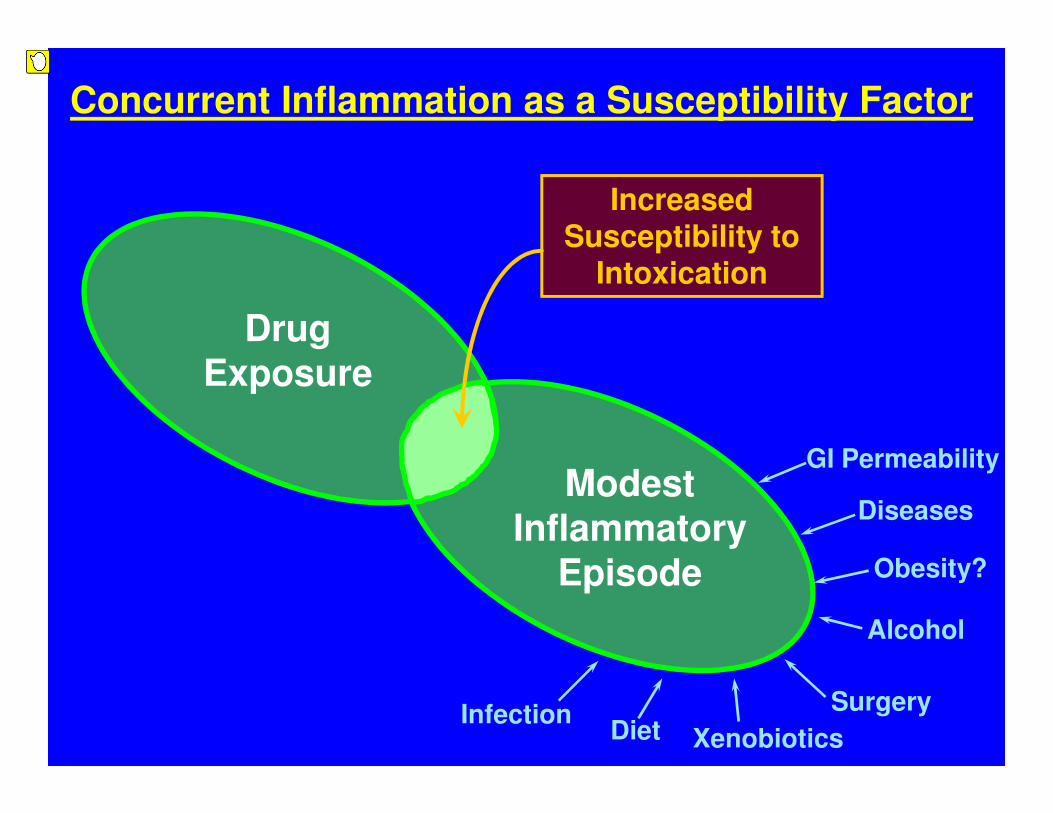
Modest Inflammatory
Episode
Increased Susceptibility to
Intoxication
Drug Exposure
Diseases
Alcohol
Diet Xenobiotics
SurgeryInfection
Concurrent Inflammation as a Susceptibility Factor
Obesity?
GI Permeability
Presenter
Sticky Note
So, this hypothesis really involves the concept that an intersection between a modest inflammatory episode in drug exposure can lead to hepatotoxicity. As we all know, there's a lot of things ‑‑ and I have listed a few of them here on the right, the lower right ‑‑ that can cause modest inflammatory episodes. I won't have time to go through all of those.
Time on Maintenance Drug Therapy
Dru
g C
on
c. in
Pla
sm
aHypothesis: Inflammatory Stress Precipitates
Idiosyncratic Responses
Threshold for Toxicity
Toxic ResponseMinimum Effective Conc.
Presenter
Sticky Note
So, this really presents the hypothesis from a pharmacokinetic perspective. I wish I had a pointer up here, but this is a plot, just a hypothetical plot, of drug concentration in the plasma over time on maintenance therapy with a drug. And the yellow line in the middle is what happens when we give a drug at regular dosing intervals at the same dose, as long as that drug is eliminated by first-order kinetics. We establish a plateau drug concentration, and the objective of therapy, of course, is to keep that plasma level above the minimum effective plasma concentration below which we don't get any pharmacologic effect ‑‑ I'm sorry ‑‑ above that level and the below the level that is a threshold for toxicity. When we teach this to our graduate students and our medical students, we kind of picture this threshold of toxicity as a constant. But, in fact, we know that it is not a constant and it can vary.
• Characteristics of IADRs:– Usually affect a small fraction of people--
– Intersection of drug therapy with a sufficient inflammatory episode is likely infrequent.
– Occur at doses that do not cause toxicity in most people—
– Inflammatory stress lowers the threshold for toxicity.
– Have inconsistent temporal relationship to exposure—
– Inflammatory episodes occur inconsistently within and across individuals.
– Are generally not reproducible in typical animal tests
– Preclinical testing does not typically involve animals subjected to inflammatory stresses.
The inflammatory stress hypothesis can explain the characteristics of many IADRs
Presenter
Sticky Note
And one of the things that can make it vary are inflammatory episodes. So, what is pictured here is someone going through life with these inflammatory episodes. I should point out that it doesn't necessarily have to be inflammation. It could be other things that cause this threshold to change, alterations in drug metabolism, et cetera. So, this patient is going along just fine until such time as that threshold for toxicity dips down into the range of plasma concentrations, at which point we are going to get a toxic response to the drug. And I would argue that a lot of the characteristics, the idiosyncratic reactions, can be explained by this hypothesis. So, these drugs usually affect a small fraction of people, and you would expect that because the intersection of drug therapy with a sufficient inflammatory episode is likely not all that frequent. They occur at doses that don't cause toxicity in most people, and you would expect that if the inflammatory stress is lowering the threshold to toxicity. They have an inconsistent temporal relationship to exposure, and you would expect that since inflammatory episodes occur inconsistently within and across individuals. And they are generally not reproducible in animal tests because preclinical testing doesn't typically involve animals that are subjected to inflammatory or other stresses, for that matter.
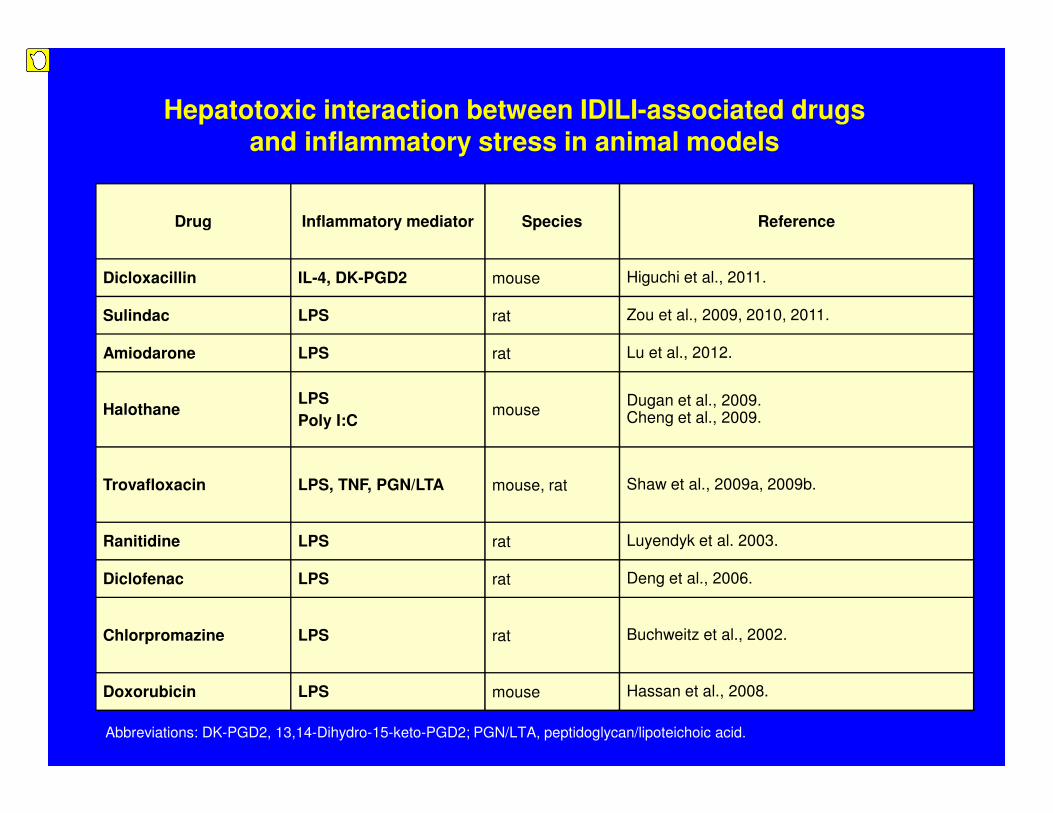
Hepatotoxic interaction between IDILI-associated drugs and inflammatory stress in animal models
Dicloxacillin IL-4, DK-PGD2 mouse Higuchi et al., 2011.
Sulindac LPS rat Zou et al., 2009, 2010, 2011.
Amiodarone LPS rat Lu et al., 2012.
HalothaneLPS
Poly I:C mouse
Dugan et al., 2009. Cheng et al., 2009.
Trovafloxacin LPS, TNF, PGN/LTA mouse, rat Shaw et al., 2009a, 2009b.
Ranitidine LPS rat Luyendyk et al. 2003.
Diclofenac LPS rat Deng et al., 2006.
Chlorpromazine LPS rat Buchweitz et al., 2002.
Doxorubicin LPS mouse Hassan et al., 2008.
Presenter
Sticky Note
Well, what I have here ‑‑ and I don't know how visible this is ‑‑ but this is a list of drugs. Well, let me back up and say that part of our efforts over the last decade have been attempts to try to develop animal models based on this hypothesis. And so, what we have done typically is to give some kind of an inflammatory stimulus, usually LPS, that causes liver inflammation, but no hepatotoxicity, no hepatocellular injury, and then couple that with drug administration. What we, and now others, have found with a number of drugs listed here, that cause idiosyncratic hepatotoxicity in people, is that we can get these animals that don't normally response with hepatotoxicity to these drugs to respond with increases in ALT and hepatocellular necrosis. So, you can read down this list. And you heard a little bit about this in one of the talks yesterday. My clinician friends hate ranitidine. I just might make a comment about that. Ranitidine, there are probably only, I think, two reports of ranitidine liver failure in people in the clinical literature, but there are dozens of reports of at least increased ALTs. So, whether you consider that idiosyncratic hepatotoxicity I guess depends on your definition. I think this is one thing about these models. We really don't know to what extent they can distinguish between severe hepatotoxicity and hepatotoxicity that is more mild.
Trovafloxacin (TVX)
• A broad spectrum fluoroquinolone antibiotic released in 1998;
• Toxicology: Liver injury not apparent in preclinical safety evaluation or clinical trials.
• In 1999, TVX was linked with hepatotoxicity, and its use was curtailed-- 14 cases of acute liver failure were linked to TVX, including 6 deaths;
• The incidence of liver injury caused by TVX was about 1 in 18,000 and about 1 in 178,000 for severe hepatotoxicity;
• Levofloxacin (LVX), in the same pharmacologic class, has far less IDILI liability;
Presenter
Sticky Note
But what I would like to do for the rest of the talk is focus on one of these. That is trovafloxacin. As most of you know, trovafloxacin is a broad-spectrum antibiotic. It sailed through its preclinical and clinical trials fine, but about a year after it was introduced onto the market, liver injury began to appear which was severe in some patients. The incidence of that liver injury was low. So, it is a rare reaction, an idiosyncratic reaction. This will come up in a moment, but levofloxacin, in the same pharmacologic class, has far less IDILI liability than does trovafloxacin.
Inflammatory Stress Hypothesis: Mouse Model of TVX-Inflammation Interaction
-3 hr 2-24 hr
Vehicleor
TVX(nontoxic dose, po)
0 hr
Vehicleor
LPS(nontoxic dose, ip)
Serum ALT
Histopathology
Etc.
Presenter
Sticky Note
So, we have developed animal models both in the mouse and the rat. I am really going to talk just about the mouse model today with trovafloxacin. In this model, the treatment paradigm we settled on was giving trovafloxacin three hours before LPS and, then, looking thereafter at hepatotoxicity. This is a dose response curve resulting from that treatment paradigm. What you see here, in the green on the bottom is what happens when you give trovafloxacin alone. We really don't get any hepatotoxicity. I think the student who did this went out to about 500 milligrams per kilogram, to the point where he was starting to kill animals, and still didn't find any hepatotoxicity.
A modest inflammatory episode renders TVX hepatotoxic
TVX (mg/kg)
0 50 100 150 200
AL
T (
U/L
)
0
2000
4000
6000 LPS
Veh
*
*
*
*
Presenter
Sticky Note
The LPS alone, if you look at the zero point on the bottom, does not cause any liver injury by itself. But when the two are given together, you see a dose-related increase in toxicity.
Liver Histopathology of TVX/LPS-treated Mice
Presenter
Sticky Note
And I don't know how well this is going to show up. But this is the histopathology. So, what we see predominantly is an inflammatory response and hepatocellular necrosis that is predominantly mid-zonal, but also we do see lesions in the centrilobular area that are somewhat less frequent.
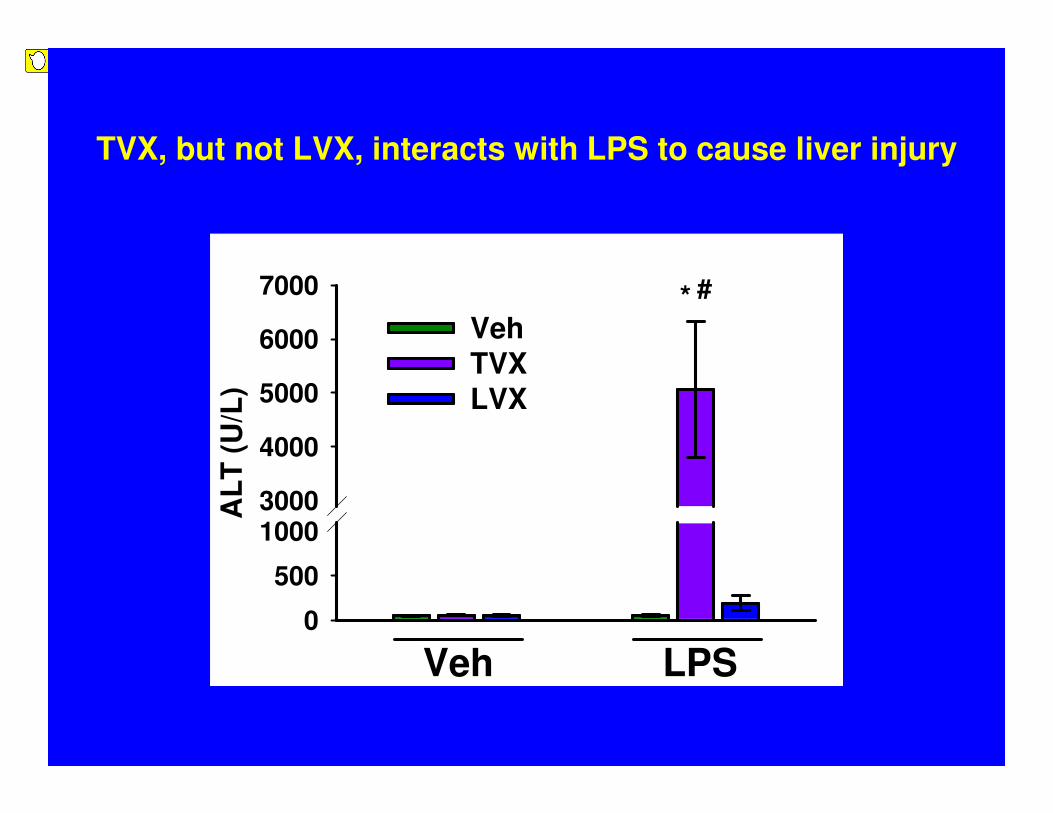
TVX, but not LVX, interacts with LPS to cause liver injury
AL
T (
U/L
)
0
500
10003000
4000
5000
6000
7000
Veh
TVX
LVX
Veh LPS
* #
Presenter
Sticky Note
When we have been able to identify them, we have tried to use negative comparators, that is, drugs in the same pharmacologic class that have less liability for IDILI. And what you see here on the right is, if you can just focus on the three bars, that is LPS alone on the left, LPS plus trovafloxacin. As I have shown you, that leads to pronounced hepatotoxicity in the mice. And then, when we gave levofloxacin along with the LPS, we didn't get that response. The levofloxacin dose we used here, by the way, was about two-and-a-half times the dose that we used for the trovafloxacin because we were trying to keep the ratio of those doses similar to the ratios that is used in people clinically.
Tumor Necrosis Factor-alpha (TNF)
• Inflammatory cytokine (17kD) released by macrophages and other cells;
• Its release is stimulated by several inflammatory mediators, including LPS;
• Acts on two receptors TNFR1 (p55) and TNFR2 (p75) –each of which has been reported to be involved in various models of liver injury.
• Actions:
• Activates the acute phase response
• Stimulates production of secondary inflammatory mediators
• Can cause death of hepatocytes (directly).
Presenter
Sticky Note
We have spent a lot of effort trying to figure out what factors are involved in this interaction between drugs and the inflammatory response. I am not going to have time to share all of that with you. But one of the factors we think that is very important and proximal in a cascade of events that occurs is tumor necrosis factor. I think you are probably all familiar with this. You know that it acts at a couple of different receptors, a p55 and a p75 receptor, and it has many actions that may contribute to interaction with a drug.
Hours after LPS or Veh
0 1 2 3 4 5 6
TN
F (
pg
/mL
)
0
1000
2000
3000
4000 Veh/Veh
TVX/Veh
LVX/Veh
Veh/LPS
TVX/LPS
LVX/LPS *
*
*
*
*
**
#
#
TVX prolongs the LPS-induced increase in plasma TNF
Properties
Sticky Note
So, what happens to TNF when we give our LPS? That is shown here. So, what we have is TNF concentration in the plasma plotted against time after LPS administration. At the bottom, the dotted black line is what happens when we give trovafloxacin alone. That is, we don't see any increase in TNF in the plasma. And that kind of "tealy" line is LPS alone. It is well-known that, when animals are exposed acutely to LPS, TNF rises in the plasma. It takes about an hour and a half and then drops off relatively-rapidly. And then, the purple line is trovafloxacin and LPS co-treatment. What you see here is that the trovafloxacin enhanced the appearance of TNF. We think, more importantly, it prolonged the TNF peak. So, it prolonged the appearance of TNF in the plasma. I don't know if it is apparent, but the kind of olive drab line is what happens with levofloxacin coupled with LPS. So, again, with levofloxacin, we didn't get any hepatotoxicity when we also don't increase that TNF response.
AL
T (
U/L
)
0
10005000
6000
7000
8000
TVX/LPS TVX/LPS/p55 -/- TVX/LPS/p75 -/-
*
* #
WT
p55 -/-
p75 -/-
TNF Receptor Knockout Affords Protection
Presenter
Sticky Note
Animals that were deficient in the TNF receptors, actually, either one of them, were markedly protected against the injury, suggesting that the TNF is causally involved in this response. And also, when we gave the etanercept, which is basically a soluble receptor that inactivates TNF when it is released, that afforded almost complete protection.
Etanercept, a soluble TNF receptor, reduces TVX/LPS-induced liver injury
TVX/Veh/LPS
TVX/Etan/LPS
AL
T (
U/L
)
0
250
500
2000
4000
6000
8000 *
#
Veh/Veh/Veh TVX/Veh/LPS TVX/Etan/LPS
AL
T a
cti
vit
y (
U/L
)
0
1000
2000
3000
4000
5000
-1 h + 1.5 h + 4 hnone
**
Time of etanercept administration
Presenter
Sticky Note
And importantly, when we gave etanercept at the TNF peak, okay, which is, again, an hour and a half after LPS administration, we were also able to markedly blunt the response, almost eliminate it. So, again, this is the reason why we think that this prolongation in the TNF peak is really important.
Can TNF replace LPS in the model?
-3 hr 21 hr
Vehicleor
TVX(150 mg/kg, po)
0 hr
Vehicleor
Murine TNF(50 ug/kg, ip)
Serum ALT
Histopathology
Etc.
Presenter
Sticky Note
Well, if it is important, the next question was: can we actually replace LPS with TNF in the model? So, here, what you see is at zero hours, well, what you see is the same treatment regimen I showed you before, but at zero hours, instead of giving LPS, we gave TNF to the animals. And so, the answer to the question is yes. Again, if you look on the right, TNF alone didn't produce any hepatotoxicity at the dose we used. But when it is coupled with trovafloxacin, it did.
AL
T a
cti
vit
y (
U/L
)
0
1000
2000
3000
4000
5000
Veh
TVX
Veh TNF
* #
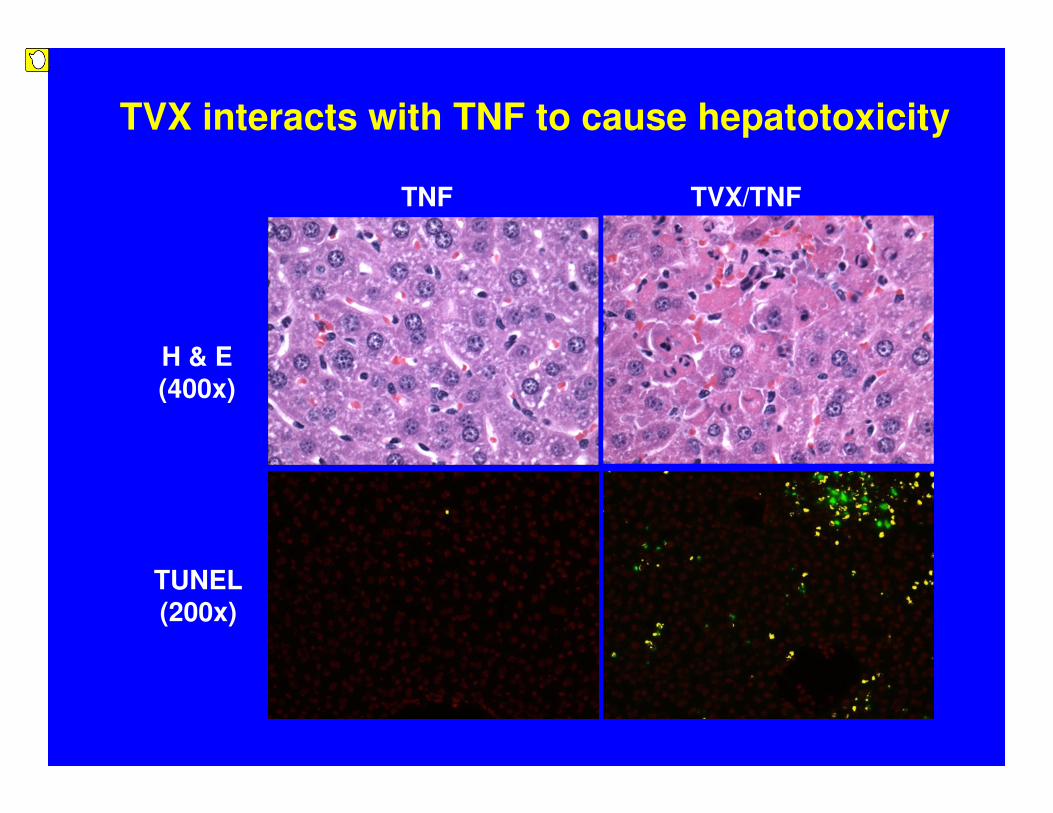
TVX interacts with TNF to cause hepatotoxicity
H & E(400x)
TUNEL(200x)
TNF TVX/TNF
Presenter
Sticky Note
And this just shows the histopathology. Again, I am not sure how well that is showing up over there. But we saw, again, areas of hepatocellular necrosis. It seemed, by the way, to look like kind of a combination of oncotic necrosis and apoptosis. This was associated with an increase in TUNEL staining, suggesting DNA damage.
TNF α
↑Thrombin
PMN accumulation
PMN activation
Fibrin Hypoxia
Proteases
Chemokines
PAI-1
IFN
IL18
Caspases
Drug
Drug
Liver Injury
LPS
Drug-induced enhancement of LPS-mediated TNF appearance is critical for distal events in the pathogenesis
Presenter
Sticky Note
Well, I am not going to have time to go through everything else we have done with this drug model. But this kind of summarizes some of the things we found.
TNFLPS
RAW
TVX
+?
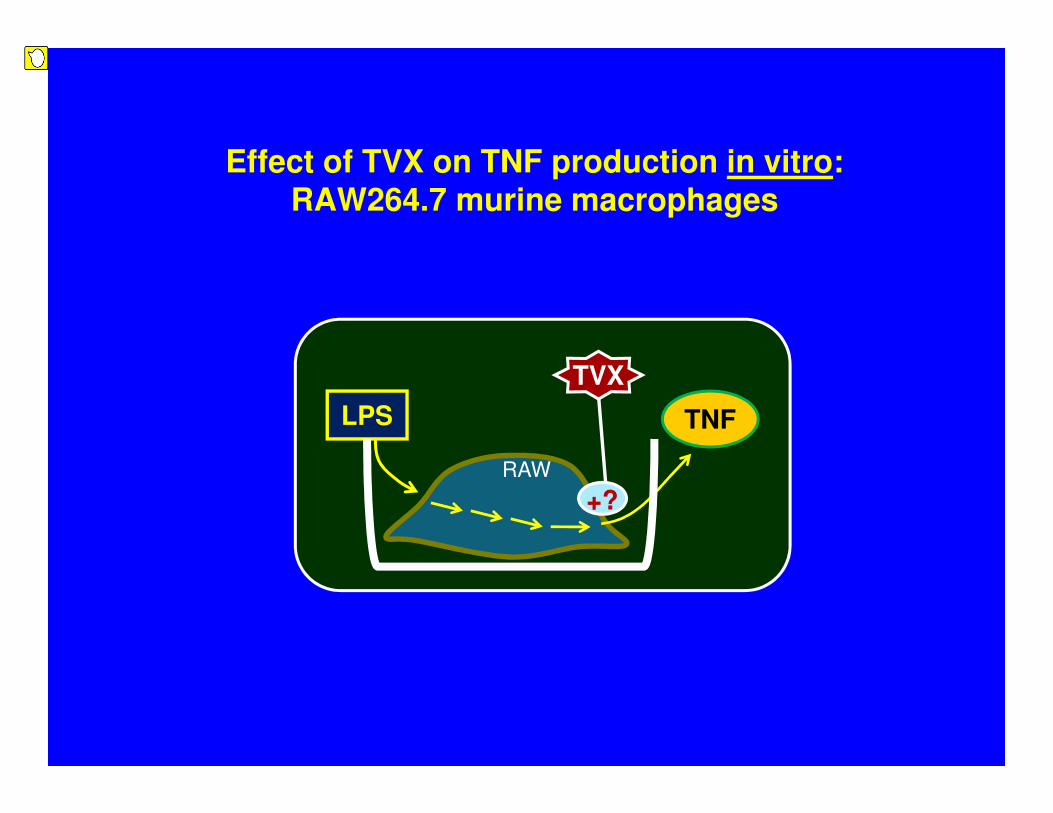
Effect of TVX on TNF production in vitro: RAW264.7 murine macrophages
Presenter
Sticky Note
So, we think LPS is doing at least two important things to initiate this response. One is to cause this increase in TNF, and another is to bring neutrophils into the liver. If you just kind of follow along the TNF line and look a little bit north of that, one thing that happens ‑‑ and, by the way, we have evidence in some way or another for each one of these arrows except for one, which I will try to mention. But we have really a cytokine storm that is set up where we get a disregulated amplification of cytokine release that is, again, initiated by TNF, but the drug seems to potentiate that. The neutrophils that accumulate in the liver, as a response to LPS, really aren't doing anything harmful there. They are just sitting there, and they require activation in order to participate in the response, which they seem to do. So, if we neutrophil-deplete animals, we get a partial protection, and the neutrophil is maybe doing a bunch of things. But the neutrophil proteases like elastase seemed to be involved in this response. And then, down at the bottom, TNF also can cause expression of tissue factor and activation of the coagulation system. And when we give anticoagulants, we also see partial protection. So, we think the coagulation system plays a role in all this, too.
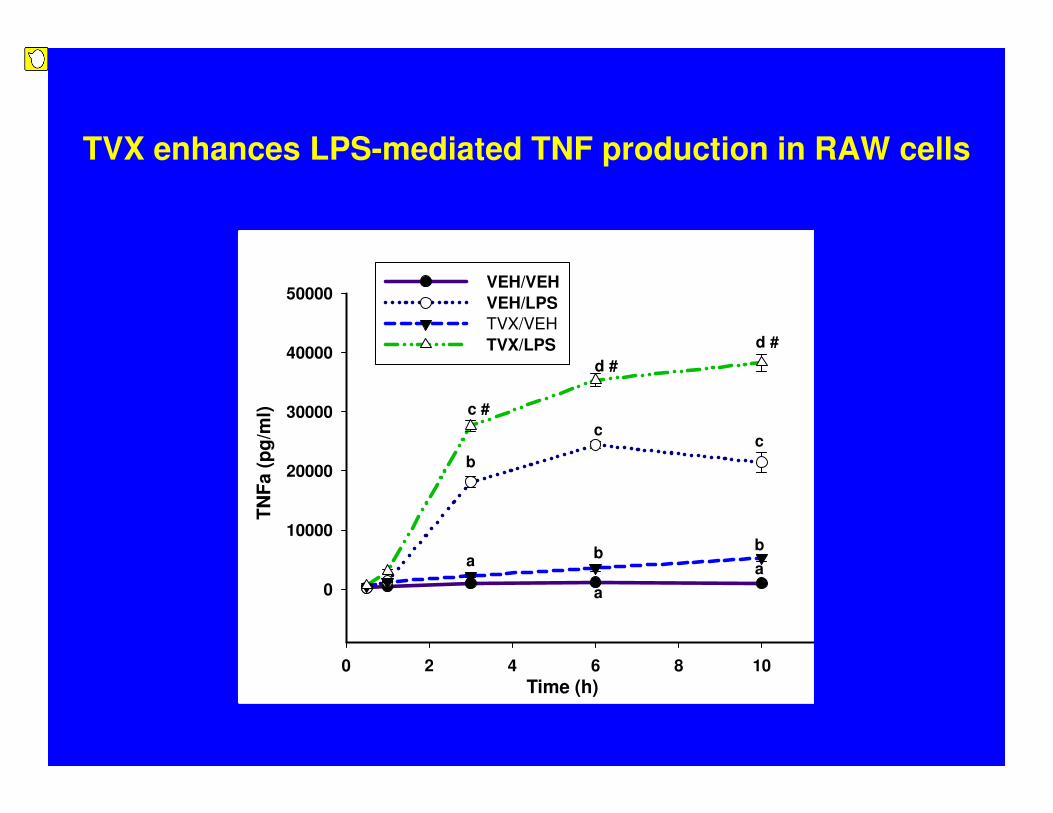
TVX enhances LPS-mediated TNF production in RAW cells
0 2 4 6 8 10 12
0
10000
20000
30000
40000
50000VEH/VEH
VEH/LPS
TVX/VEH
TVX/LPS
c
b
a
d #
c
b
a
d #
b
a
c #
TN
Fa (
pg
/ml)
Time (h)
Presenter
Sticky Note
We may have also have direct effects of TNF in killing hepatocytes which are amplified by certain cytokines like interferon-gamma and, also, perhaps by the drug increasing hepatocellular sensitivity to the TNF. Since the production of TNF, the enhanced production of TNF is important, one of the things we have been doing lately is to try to carry some of these things we have learned in vivo into the culture dish and see if we can reproduce them there. So, what we have done in our preliminary studies is, using raw cells, raw 264.7 cells, which are murine macrophage cell line, in this case a surrogate, if you will, for the Kupffer cell, what we have done, and what other people have shown, is that LPS will activate toll receptors on these cells. And that results in the release of TNF into the medium.
(Treatments with different letters differ significantly within a time point, p< 0.05)
0 2 4 6 8
-2000
0
2000
4000
6000
8000
10000
12000
14000 Veh/Veh
Veh/LPS
TVX/Veh
TVX/LPS
a
bb
c
a
c
a
b
a
b
b
a
b
a
aa
Rate
of
TN
F C
on
c.
Ch
an
ge
(pg
/ml/
hr)
Time (hr) after LPS addition
a
TNF production rate after exposure of RAW cells to LPS and/or TVX
Presenter
Sticky Note
The question is, does trovafloxacin enhance that? And the answer is yes. So, here we are looking again, on the ordinate, the TNFs, and the medium over times. And what you can see in the dotted blue line is that trovafloxacin itself has a very small effect, actually, which is kind of interesting to us. The line in the middle there is what happens with LPS alone. So, when you give LPS, of course, you get enhanced cytokine release. And then, the green line at the top shows that you get a synergistic response with trovafloxacin and LPS onboard together.
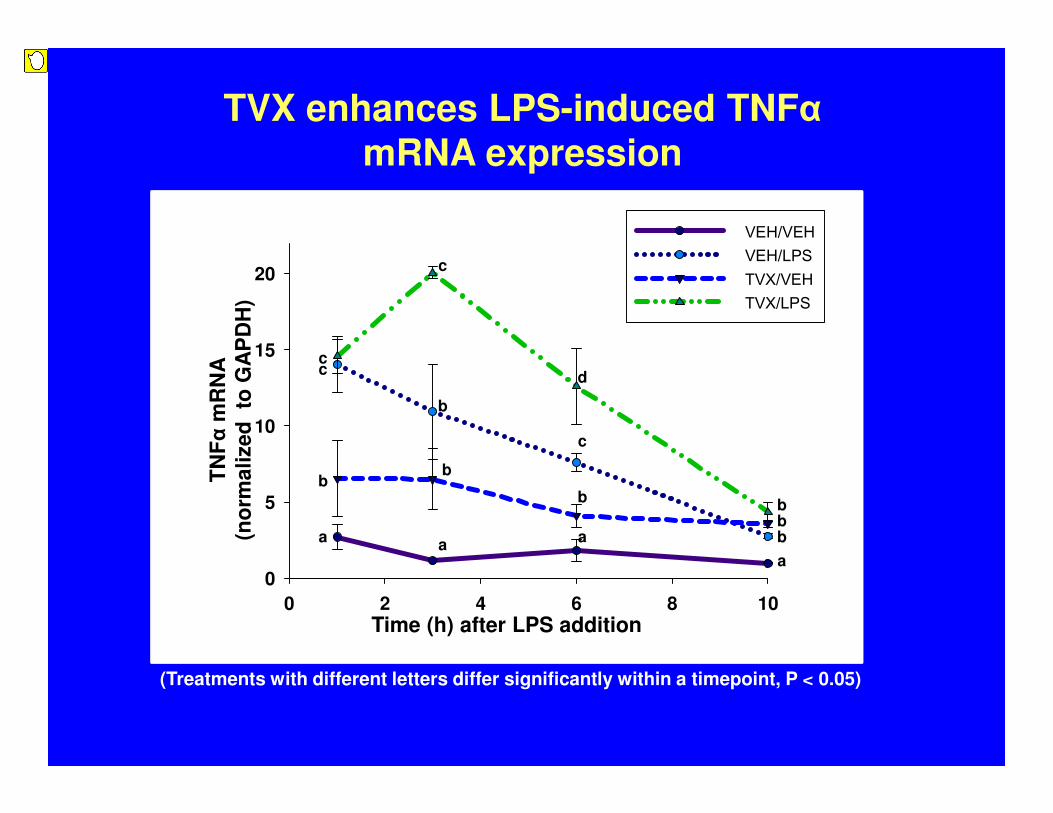
TVX enhances LPS-induced TNFαmRNA expression
(Treatments with different letters differ significantly within a timepoint, P < 0.05)
0 2 4 6 8 10
0
5
10
15
20
VEH/VEHVEH/LPSTVX/VEHTVX/LPS
Time (h) after LPS addition
TN
Fα
mR
NA
(no
rma
lize
d
to G
AP
DH
)
a
b
c
a
b
c
a
b
c
d
a
b
c
bb
b
Presenter
Sticky Note
If we actually plot the slopes of these lines, which really relates to the rate of release, you get curves that look like this, which really look a lot like the curve of LPS in the plasma I showed you in vivo. So, I think the important thing to point out here is that, if you look at the top line, the rate of release continues to be significantly elevated over what happens with LPS alone. So, this seems to be an important facet of what the drug does, at least in vivo, not only in this model, but in other models of LPS drug interaction at which we have looked. This response seems to be, at least in part, due to enhanced expression, a gene expression for mRNA, as shown here.
Hepatotoxic interaction between IDILI-associated drugs and inflammatory stress in animal models
Abbreviations: DK-PGD2, 13,14-Dihydro-15-keto-PGD2; PGN/LTA, peptidoglycan/lipoteichoic acid.*Drugs for which TNF is critically important in the pathogenesis (not examined in most of the other models)
Drug Inflammatory mediator Species Reference
Dicloxacillin IL-4, DK-PGD2 mouse Higuchi et al., 2011.
Sulindac LPS rat Zou et al., 2009, 2010, 2011.
Amiodarone LPS rat Lu et al., 2012.
HalothaneLPS
Poly I:C mouse
Dugan et al., 2009. Cheng et al., 2009.
Trovafloxacin LPS, TNF, PGN/LTA mouse, rat Shaw et al., 2009a, 2009b.
Ranitidine LPS rat Luyendyk et al. 2003.
Diclofenac LPS rat Deng et al., 2006.
Chlorpromazine LPS rat Buchweitz et al., 2002.
Doxorubicin LPS mouse Hassan et al., 2008.
Presenter
Sticky Note
To wrap up, then, we are kind of back to this slide. I guess what I might say here is that we, or others, have looked at a number of different drugs that cause IDILI in people and have been successful in obtaining liver injury, actual liver injury, usually pronounced liver injury, in these models. They really do represent the first models in which liver injury has been obtained over a range of drugs that represent different pharmacologic classes. Well, okay, I am a little ahead of myself.
• Animal studies suggest that some IDILI reactions are likely to result from interaction of drugs with inflammatory episodes (or other stresses);
• The inflammatory stress hypothesis has provided the first animal models of IDILI in which liver injury occurs over a range of drugs;
• TVX and other IDILI-associated drugs interact with LPS to cause liver injury in mice—
– These drugs increase (prolong) the appearance of TNF;
– TNF is a proximal mediator of drug-LPS hepatotoxicity;
– Distal (downstream) mechanisms are complex, involving cytokines,
neutrophils, the hemostatic system, and probably other factors;
– In vitro, TVX
• (1) increases TNF production by macrophages and
• (2) increases hepatocellular sensitivity to TNF-mediated killing.
Conclusions and perspectives:
Presenter
Sticky Note
So, in conclusion, then, animal studies suggest that some of these IDILI reactions are likely to result from interactions with drugs with inflammatory episodes and really other stresses, too. I actually think one of the reasons the inflammatory response works in this is that the inflammatory response is really a collage of responses. And it could be that, for one drug, it might be reactive oxygen species; for another drug, the cytokines might be more important. We really don't know that yet. And as I mentioned, this hypothesis has provided us with the first animal models in which frank liver injury actually occurs over a range of drugs. And then, the third point really relates to TNF. I won't read all that to you, but just to go down to the bottom, in vitro, as I have shown you, we get increases in TNF in macrophage preparations with some of these drugs.
• Do other IDILI-associated drugs increase cytokine
production in cells stimulated by TLR agonists?
• The Hope: Understanding of mechanisms will lead to
high-throughput, cell-based assays that predict IDILI
potential.
Conclusions and perspectives (cont’d):
Presenter
Sticky Note
And in data I haven't had time to show you, if we use hepatocytes, we have also shown that the trovafloxacin, for example, can increase hepatocellular sensitivity to the killing by TNF or the combination of TNF and other cytokines like interferon-gamma, and others have shown this as well. So, these are some of the questions. I think an important one is, do other IDILI-associated drugs increase cytokine production in vitro in cells that are stimulated by LPS or other toll receptor agonists? And our hope, then, is that by understanding the mechanisms and, hopefully, evidence for the modes of action with animal models, that this will lead to more high-throughput, cell-based assays that might actually be useful in preclinical situations to predict which drug candidates might have IDILI potential.
So, I will finish with this. This is really kind of, I guess what I would call, an integrated conceptual framework here. But we have our inflammatory stress, which can be, again, precipitated by a lot of different things, and GI permeability increases, diseases, et cetera. We have the PAMPs and the DAMPs that others have talked about activating toll-like receptors on various inflammatory cells, probably in the liver, especially Kupffer cells, to release cytokines and other factors that we would define as inflammatory stress. And the hypothesis here is that, then, the drugs or the metabolites of these drugs can enhance this inflammatory stress and also cause stress on hepatocytes. And then, these two together, probably through cell-death-signaling pathways, can lead to liver injury, which, again, as you have already heard, that many people can adapt to that. And so, it may not be everybody who responds to this with liver injury. But in some sensitive individuals, that might lead to liver failure. And then, I think inflammation might also relate to the adaptive immunity hypothesis. And I won't go through all of that with you. You are all familiar with it. But the inflammatory stress may provide a danger signal which would take a normally perhaps innocuous adaptive immune response and throw it over into one that actually becomes hepatotoxic. And it may be that the drug is necessary not only to produce the metabolite and, therefore, the hapten, but also to enhance the inflammatory response to lead to that untoward reaction.
Support
NIH-NIEHS
NIH-NIDDK
Abbott Labs
Pfizer, Inc.
Michigan State Univ.
Patti Ganey
Mike Scott
Pat Shaw
Wei Zou
Jim Luyendyk
Rohit Singhal
Erica Sparkenbaugh
Aaron Fullerton
Christine Dugan
Kevin Beggs
Kyle Poulsen
Jingtao Lu
Kaz Miyakawa
Inflammatory Stress
Idiosyncratic Reaction
Drug Exposure
Acknowledgments
Abbott Labs
Jeff Waring
Mike Liquori
Eric Blomme
Presenter
Sticky Note
So, I will stop there. By the way, I am from Michigan State University, the basketball school. I think it says "University of Michigan," and we don't want to make that mistake. (Laughter.)