Together • issue 1 • August 2013 • B 50110 • ISSN 1612-9873 Information from DAHW Deutsche Lepra- und Tuberkulose Hilfe (DAHW German leprosy and tuberculosis relief organisation) Annual Report for 2012 This is what we have achieved! www.dahw.de
Transcript
Together • issue 1 • August 2013 • B 50110 • ISSN 1612-9873
Information from DAHW Deutsche Lepra- und Tuberkulose Hilfe
(DAHW German leprosy and tuberculosis relief organisation)
Harald Meyer-Porzky. Collaboration: Rolf BauerdickFinancial report: Peter Hofmann, Nicole Hohmann, Bernd KörberTitle photo: Jochen HövekenmeierLayout: Hubertus Wittmers, MünsterPrinting: Bitter & Loose GmbH, GrevenResponsible according to the press law : Burkard KömmCopy deadline: 01. Juli 2013ISSN 1612-9873
Contents
Jackson E.’s hands are m arked by leprosy; his feet had to be am-putated years ago. He has been living in the Gant a Leprosy Hos-pital supported by DAHW for over 20 years. In spite of this he works, serving the hospital, and every evening he feels good be-cause he has earned his meal and is not receiving alms.
When he can't work with the bas-ket weavers because of the pain in his hands, he s its at the en-trance to the outpatient depart-ment and t alks to the new pa-tients who are u ndergoing ex-amination here. He stil ls their fears about the tre atment and
assures them that it is good to be examined for leprosy in g ood time.When Jackson came to Ganta the disease was a lready very ad-vanced and it was impossible to save his feet. “Many new pa-tients profit from his experience” Dr. Pieter de Koning informs us. The Dutch doctor and the It alian sisters who manage the hospital are glad that Jackson enjoys his tasks: “The most important thing for old patients is for them not to feel that they are u seless or a burden.”
Report about Ganta and leprosy in Liberia from page 9.
Title storyThe Ganta Rehab Leprosy Hospital.
Report by the President:A worthwhile mission 3
Management Report 4
Leprosy: Leeroy learns to laugh: DAHW teams are finding lots of new leprosy patients 9
Tuberculosis: The treacherous epidemic and its victims 12
Neglected Diseases: Buruli Ulcer: Leprosy’s little sister 16
Overview of projectsWorldwide relief in 2012 18
People with disabilities: The tragedy of the twins Jaykant and Jaykanti 20
The Ruth-Pfau Foundation: Out of the love for humanity 23
Volunteers support the objectives of DAHW 24
Report by the Financial Director: Donations in good hands 25
Financial report 26
Dedicated to Hermann Kober’s legacy 29
Around DAHW – a review of the year 30
Organisational chart 34
Research: The “outrageous” suffering caused by leprosy 35
Phot
o: Jo
chen
Höv
eken
mei
er
3 DAHW Annual Report 2012
A worthwhile mission“Our vision is a world in which not one sin-gle person suffers from leprosy, tuberculo-sis or other poverty-related diseases and their consequences, such as disability and exclusion.” For over 55 years people in the DAHW Deutsche Lepra- und Tuberkulose-
hilfe e.V. have been c ommitting them-selves to making this vision become reality And it is not “just” the treatment of dis-eases which matters.
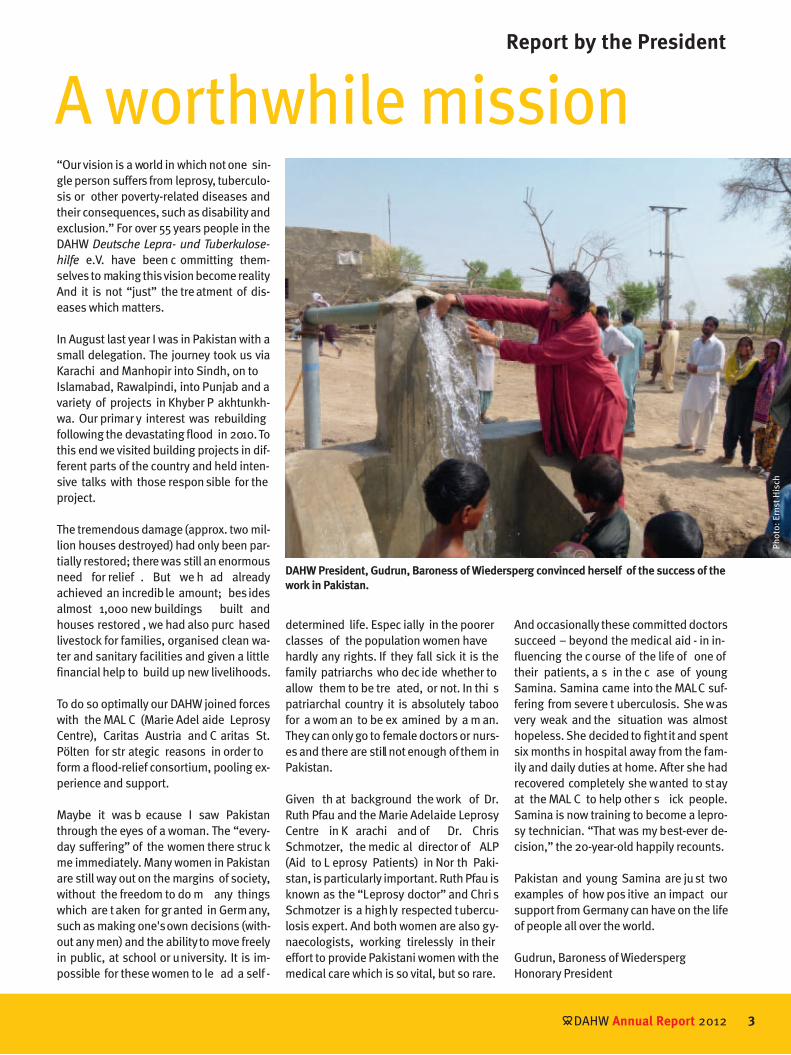
In August last year I was in Pakistan with a small delegation. The journey took us via Karachi and Manhopir into Sindh, on to Islamabad, Rawalpindi, into Punjab and a variety of projects in Khyber P akhtunkh-wa. Our primar y interest was rebuilding following the devastating flood in 2010. To this end we visited building projects in dif-ferent parts of the country and held inten-sive talks with those respon sible for the project.
The tremendous damage (approx. two mil-lion houses destroyed) had only been par-tially restored; there was still an enormous need for relief . But we h ad already achieved an incredible amount; besides almost 1,000 new buildings built and houses restored , we had also purc hased livestock for families, organised clean wa-ter and sanitary facilities and given a little financial help to build up new livelihoods.
To do so optimally our DAHW joined forces with the MAL C (Marie Adel aide Leprosy Centre), Caritas Austria and C aritas St. Pölten for str ategic reasons in order to form a flood-relief consortium, pooling ex-perience and support.
Maybe it was b ecause I saw Pakistan through the eyes of a woman. The “every-day suffering” of the women there struc k me immediately. Many women in Pakistan are still way out on the margins of society, without the freedom to do m any things which are taken for granted in Germany, such as making one's own decisions (with-out any men) and the ability to move freely in public, at school or university. It is im-possible for these women to le ad a self -
DAHW President, Gudrun, Baroness of Wiedersperg convinced herself of the success of the work in Pakistan.
Report by the President
determined life. Espec ially in the poorer classes of the population women have hardly any rights. If they fall sick it is the family patriarchs who dec ide whether to allow them to be tre ated, or not. In thi s patriarchal country it is absolutely taboo for a wom an to be ex amined by a m an. They can only go to female doctors or nurs-es and there are still not enough of them in Pakistan.
Given th at background the work of Dr. Ruth Pfau and the Marie Adelaide Leprosy Centre in K arachi and of Dr. Chris Schmotzer, the medic al director of ALP (Aid to L eprosy Patients) in Nor th Paki-stan, is particularly important. Ruth Pfau is known as the “Leprosy doctor” and Chris Schmotzer is a highly respected tubercu-losis expert. And both women are also gy-naecologists, working tirelessly in their effort to provide Pakistani women with the medical care which is so vital, but so rare.
And occasionally these committed doctors succeed – beyond the medical aid - in in-fluencing the course of the life of one of their patients, a s in the c ase of young Samina. Samina came into the MALC suf-fering from severe t uberculosis. She was very weak and the situation was almost hopeless. She decided to fight it and spent six months in hospital away from the fam-ily and daily duties at home. After she had recovered completely she wanted to stay at the MAL C to help other s ick people. Samina is now training to become a lepro-sy technician. “That was my best-ever de-cision,” the 20-year-old happily recounts.
Pakistan and young Samina are just two examples of how pos itive an impact our support from Germany can have on the life of people all over the world.
Gudrun, Baroness of WiederspergHonorary President
Phot
o: E
rnst
His
ch
Management Report
Reconstruction in Pakistan after the disastrous flooding is by no means complete.
4 DAHW Annual Report 2012
Dear friends and supporters of DAHW
Phot
o: E
rnst
His
ch
DAHW Annual Report 2012
The DAHW Deutsche Lepra- und Tu-
berkulosehilfe e.V. was very successful in carrying out its mission. Again in 2012, the mission which is rooted in the statutes and is financed by many thousands of peo-ple in Germany, Austria, the Czech Repub-lic and elsewhere, has spurred its volun-teers and ful l-time employees on to top performance. Our ability to bring sustain-able aid and support to the needy via our effective, reliable structures – frequently under very difficult conditions – has not gone unremarked by other relief organisa-tions and in stitutions for emerg ency aid and development cooperation. For exam-ple, we received additional funds amount-ing to millions to solve tasks together and to contribute towards a positive change in the fate of needy people affected b y lep-rosy, tuberculosis or other neglected dis-eases and also by disabilities.
We continue to work, concentrating on our vision of a “world in which not one single person suffers from leprosy, tuberculosis and other po verty-related diseases and their consequences, such as disability and exclusion.”
It’s the effect that counts!
From the global point of view neither lep-rosy nor tuberculosis has changed drasti-cally. The burden of disease is still just as high for leprosy. According to information from the World Health Organisation (WHO) in 2011 more th an 230,000 people c on-tracted leprosy. Compared to 2010 num-bers have risen a little. If we want to realise our vision for DAHW, we must insist that the number of new cases must be reduced. Unfortunately, we frequently find that -
and sustainable leprosy work, for example by means of training and suppor t in the form of human resources. This support is a means of creating improvements in the leprosy work which will also affect the fu-ture and whic h raises our politic al influ-ence as a c ivil society organisation with regard to claiming human rights for those people for whom we campaign.
It is our decl ared objective not just to speak for these people, but to enable the people we support to demand their rights themselves. Involving the people who are affected by leprosy and tuberculosis in all the planning work and projects is a funda-mental prerequisite for effective, su stain-
faced with inadequate state funding - the national health authorities in our par tner countries are unable or unwilling to sup-port leprosy work in their own c ountries. Our mere presence and commitment often has the effect that the state provides them with financial means and human resourc-es. In that case sustainable and effective work means a long-term presence and ad-vocacy for the people affected b y leprosy who would not otherwise be he ard and would be unable to demand state aid.
This is how we work: As a relief organisa-tion - an NGO (Non-Government Organisa-tion) - it is our mission to give aid directly to people in need who are affected by lep-rosy and tuberculosis. To this end we de-ploy both our own employees on the spot and partner organisations who take care of the needy with financial support from DAHW. By way of example we c an name some of our partners: the Marie-Adelaide-Leprosy Centre (MALC), of which Dr. Ruth Pfau is the director in K arachi/Pakistan, Aid to Leprosy Patients (ALP), directed b y Dr. Chris Schmotzer in Raw alpindi/Paki-stan, or the Buluba L eprosy Hospital of which Dr. Elizabeth Nionzima in Buluba/Uganda is the director. In the par tner or-ganisations, together and at previously defined intervals, we monitor whether the agreed effect is indeed achieved for the af-flicted persons and whether the don ated money has been used effectively.
Reinforcement of national structures
Besides direct relief, wherever pos sible we try to strengthen those national struc-tures which are respon sible for regul ar
5
It is the top priority of the medical staff to reach the people and inform them about health hazards.
Tuberculosis doctor, Dr. Chris Schmotzer with her medical team at the hospital in
Rawalpindi/Pakistan.
Phot
o: E
nric
Boi
xadó
s
Phot
o: D
AHW
DAHW Lepra-Spezial 20056
Despite her age, leprosy doctor Dr. Ruth Pfau works tirelessly.
Bericht der Geschäftsführung
DAHW Annual Report 20126
able work. Targeted stabilisation of com-munities of interest for independent repre-sentation of the needs of these groups of persons enhances the su stainability of national structures.
Future funding and donation development
DAHW has always been a relief organisa-tion based on the c ommitment of many faithful voluntary supporters. In rec ent years we have discovered that it has not been possible to close the g aps left be-hind by our volunteers of many years standing, who have had to withdraw due to their age, by engaging the same num-ber of young, committed people. This is certainly also due to a change in our soci-ety in which long-term volunteer work has tangibly lost some of its attractiveness.
However, we have also discovered that by making special efforts the rem aining DAHW volunteers have been able to make good a major part of the reduction in sup-port. Personally, I think that DAHW has the best volunteers in the whole of Germany. After all, by contrast with volunteers work-ing in a regional sports club, for example, they can only perceive the success of their efforts indirectly. And never theless, they give all they have year in and year out to help those who have been struck down by leprosy, tuberculosis or some other dis-ease or disability stemming from poverty.
Thanks to the c ommitment of the Public Relations and Fundraising department, in 2012 we rec eived a very respectable
amount of donations. Although don a-tions in Germany dropped almost by five percent in 2012, according to information given by the Deutscher Spendenrat (Ger-man donations council), we suffered a significantly smaller drop in donations of just two per cent. And this was balanced out by higher inc ome from inherit ances and institutional sponsors such as the Austrian Leprosy Relief Organisation, Likvidace Leprosy in the Czech Republic, Miserior or “the Carol Singers” in Aachen, a children’s relief organisation. The virtu-ally u nchanged project expenditure meant we were almost able to achieve a balanced budget.
Risks
Nevertheless, the members of staff agree in their assumption that it is hard to stop the downward trend regarding private donations. This trend applies to almost all relief organisations throughout Ger-many and to the other leprosy relief or-ganisations all over the world. Therefore, we are increasingly looking to institution-al sponsors who wish to make use of the good work done by DAHW, its competent staff and its decades of experience, to in-vest their own funds purposefully and ef-ficiently in our mission. In order to be well equipped for the future in this respect, in
The “Medical Advisory Team” at the DAHW headquarters in Würzburg (from left): Dr. Joseph Chukwu, Dr. Pieter de Koning, Dr. Srinivasan and Dr. Joseph Kawuma.
Phot
o: G
udru
n vo
n W
iede
rspe
rg
Phot
o: Ju
dith
Mat
hias
ch
7 DAHW Lepra-Spezial 2005
Equipping DAHW for the future: Give young donors an understanding of poverty-related diseases.
7 DAHW Annual Report 2012
2012 we re aligned the struct ure of the projects department. In addition, we started to introduc e an intern ationally approved accounting system which will make secure documentation of the funds used and control in the relevant countries and in Würzburg considerably easier. The plan is to have converted all 13 DAHW na-tional offices to the system by December 2013.
In the new departmental structure, quality assurance for our work and knowledg e management - which has been an across-the-board responsibility of all staff in the project department - has now been as-signed to a spec ial competence team. Equally, in future the national offices will receive support from a separ ate compe-tence team in Würzburg when applying to institutional sponsors for funds. The Pro-ject Development and Fund Allocation de-partments will remain and so will the Pro-gramme Development with medical and social experts to co-ordinate the develop-ment of expertise.
Our proven experts in the n ational office who are experiencing the current develop-ments and new c hallenges directly will now be far more involved in the develop-ment of strategies and in impor tant deci-sions at DAHW. The members of the so-called “Medical Advisory Team” estab-lished in October 20 12 are Dr . Joseph Kawuma (medical advisor at DAHW in Uganda), Dr. Joseph Chukwu (DAHW medi-cal advisor in Nigeria), Dr. Pieter de Koning (DAHW medical advisor in Liberia) and Dr. Srinivasan (national DAHW medical coor-
dinator in India). This team advises the management and the Management Board on strategic decisions and important med-ical matters. One of the results after the deliberations in October 2012 was an ur-gent appeal addressed to the Man age-ment Board and the management to invest significantly and effectively in rese arch into how leprosy is transmitted.
Acknowledgement
In December 2012 an article in the fin an-cial journal “Capital” stressed that the work of DAHW, its development and objec-tives are represented very well and trans-parently. The journal had c ommissioned two independent analytical companies to scrutinise the 50 l argest charities in Ger-many. For this purpose the inform ation published by the org anisations was ana-lysed and u ndercover tests were u nder-taken. To our gre at delight DAHW w as among the “Top Ten”.
And it was not only the frankne ss with which information is handled which re-ceived praise from the public. Above all it was the c ommitment of the people who work so hard in the field for people w ith leprosy and t uberculosis. In No vember 2012 Dr. Ruth Pfau was awarded the cov-eted German TV award, BAMBI in the “Si-lent Heroes” c ategory. In her mo ving speech she made it clear to the audience that we are not always aware that here in Europe we live in “paradise” compared to many poor people in c ountries in the southern hemisphere.
Challenges
One of the greatest challenges, besides securing income for the project work, is the search for suitable staff in Germany and the project countries. The vast amount of specialist knowledge required of our exper ts today at headquarters in Germany makes the search for good staff difficult. Just a few of the requirements: finding one's bearings in different cul-tures, mastering several foreign languag-es, coordinating tasks and solution s across several continents and m any countries, expertise in financial manage-
Leprosy involves more than just identifying new cases; it also means taking care of many
old patients. Here at Buluba Hospital in Uganda.
Phot
o: T
hom
as E
inbe
rger
Phot
o: S
abin
e Lu
dwig
Their work is increasingly focusing on per-sons with disabilities. DAHW is working out a global CBR strategy for the project coun-tries.
DAHW Annual Report 20128
ment as well as having one’s own experi-ence from years abroad and proof of com-mitment as a volunteer. The list of expec-tations is just about never-ending and each requirement is in itself completely different and at the same time at a high level. This is because today we no longer aspire to “be doing” all the work of DAHW from Würzburg; instead we want to ena-ble the national experts in the respective countries to support and treat the people independently and at a very high level of quality.
That requires a great deal of patience and empathy as well as being prepared to work together with the c olleagues from the partner countries to find solution s which are acceptable locally, but never-theless satisfy our global quality require-ments.
These problems also apply in a similar way to our staff abroad. Luckily, in past years DAHW has repeatedly succeeded in find-ing excellent staff and experts in the part-ner countries who have fought for a long time to ac hieve the D AHW objectives in their home countries. I would like to men-tion Dr. Joseph Kawuma in Uganda, Dr. Jo-seph Chukwu in Nig eria, Ato Ahmed in Ethiopia and Antoinette F ergusson in Si-
Management Report
Voluntary commitment: Every year in November the group in Würzburg organises a big bazaar to support DAHW. In 2012 they were able to hand over EUR 15,000 to DAHW.
erra Leone by way of example for all our staff in the partner countries. In past years these members of staff have maintained the support for people suffering from lep-rosy and tuberculosis, in some c ases un-der extremely difficult conditions. Howev-er, today the dem and for these high ly qualified, reliable specialists with high ideals is rising and it is becoming increas-ingly difficult to acquire new staff with the same high standards for long-term work at DAHW.
Prospects and key operational aspects in 2013
After 56 years as tenants, DAHW will be building new headquarters in Würzburg in the coming year. This has been made pos-sible by the donation of part of a plot on the condition that we will build on it and use it ourselves. Financially it is also ad-vantageous because in the years to come DAHW will save large sums on rent and heating costs.
DAHW will give more support to research on Buruli in Togo. Furthermore, it will es-tablish a joint research pool together with the ILEP par tner organisation, American Leprosy Missions (ALM) and w ith the Netherlands Leprosy Relief (NLR) and pro-
vide it with a financial basis to f acilitate support for more research into leprosy in the future.
In June several social workers from the project countries prepared the future Com-munity-Based Rehabilitation (CBR) strate-gy of DAHW. This approach enables per-sons with disabilities to take part in social life. DAHW has already been working in a similar way for many years for people who suffer from disabilities caused by leprosy. It wants to open up these projects for CBR in the future.
Following the International Leprosy Con-gress in Bru ssels in September , the DAHW doctors will meet in Würzburg. Dr. Joseph Kawuma, head DAHW doctor in Uganda and Ch airman of the Technical Advisory Group of the WHO, will under-take to co-ordinate this work. Here too the issue is future strategies in the pro-ject countries, so it means that the ex-pertise from the projects is very impor-tant.
Phot
o: Jo
chen
Höv
eken
mei
er
Phot
o: Jo
chen
Höv
eken
mei
er
9 DAHW Lepra-Spezial 2005
Leprosy
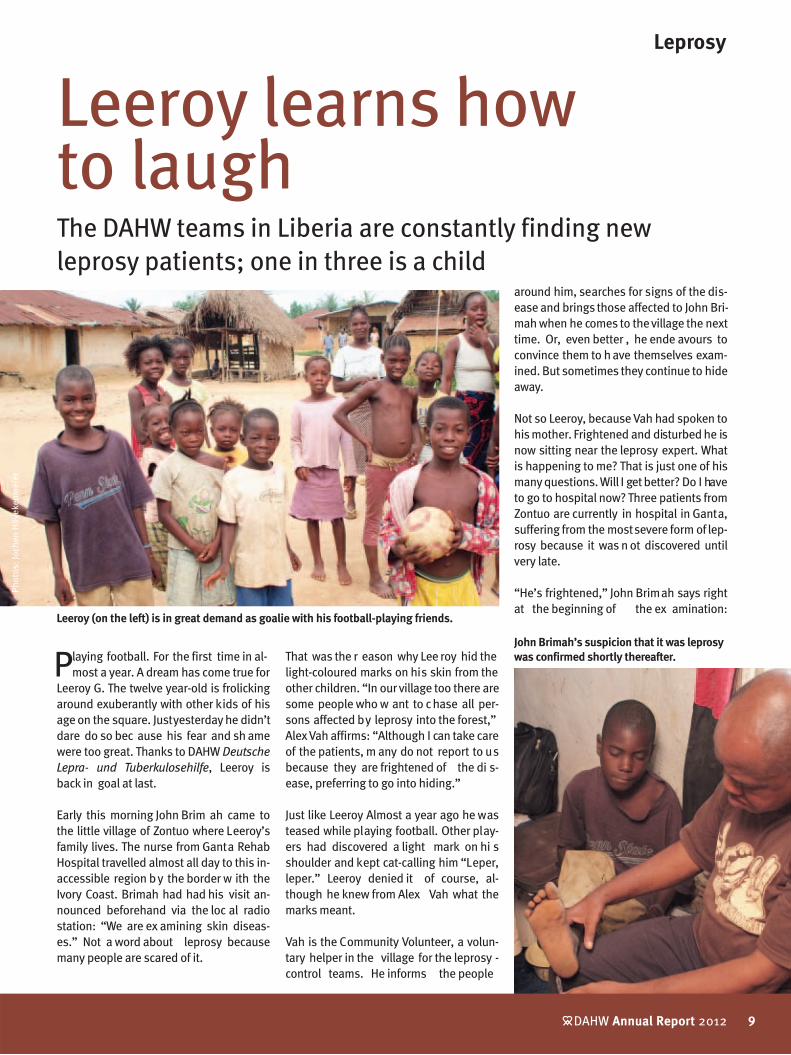
Playing football. For the first time in al-most a year. A dream has come true for
Leeroy G. The twelve year-old is frolicking around exuberantly with other kids of his age on the square. Just yesterday he didn’t dare do so bec ause his fear and sh ame were too great. Thanks to DAHW Deutsche
Lepra- und Tuberkulosehilfe, Leeroy is back in goal at last.
Early this morning John Brim ah came to the little village of Zontuo where Leeroy’s family lives. The nurse from Ganta Rehab Hospital travelled almost all day to this in-accessible region by the border w ith the Ivory Coast. Brimah had had his visit an-nounced beforehand via the loc al radio station: “We are ex amining skin diseas-es.” Not a word about leprosy because many people are scared of it.
That was the r eason why Lee roy hid the light-coloured marks on his skin from the other children. “In our village too there are some people who w ant to chase all per-sons affected by leprosy into the forest,” Alex Vah affirms: “Although I can take care of the patients, m any do not report to us because they are frightened of the di s-ease, preferring to go into hiding.”
Just like Leeroy Almost a year ago he was teased while playing football. Other play-ers had discovered a light mark on hi s shoulder and kept cat-calling him “Leper, leper.” Leeroy denied it of course, al-though he knew from Alex Vah what the marks meant.
Vah is the Community Volunteer, a volun-tary helper in the village for the leprosy -control teams. He informs the people
Leeroy learns how to laughThe DAHW teams in Liberia are constantly finding new leprosy patients; one in three is a child
around him, searches for signs of the dis-ease and brings those affected to John Bri-mah when he comes to the village the next time. Or, even better , he ende avours to convince them to h ave themselves exam-ined. But sometimes they continue to hide away.
Not so Leeroy, because Vah had spoken to his mother. Frightened and disturbed he is now sitting near the leprosy expert. What is happening to me? That is just one of his many questions. Will I get better? Do I have to go to hospital now? Three patients from Zontuo are currently in hospital in Ganta, suffering from the most severe form of lep-rosy because it was n ot discovered until very late.
“He’s frightened,” John Brimah says right at the beginning of the ex amination:
9 DAHW Annual Report 2012
Leeroy (on the left) is in great demand as goalie with his football-playing friends.
John Brimah’s suspicion that it was leprosy was confirmed shortly thereafter.
Phot
os: J
oche
n Hö
veke
nmei
er
DAHW Annual Report 201210
With an annual health budget of 20 dol-lars per inhabitant the state health sys-tem is overtaxed simply by daily life. Al-most 15 years of civil war have left their traces. In 2010 this poor country official-ly confirmed 482 new leprosy patients. In actual fact there are probab ly far more. There are only two hospitals treat-ing leprosy, one of them close to the capital, Monrovia, with a popul ation of almost two million. Around 300 new lep-rosy patients are treated there per year.
The other i s the Gant a Rehab Leprosy Hospital in the feder al state of Nimba. Last year 180 people were diagnosed as having leprosy although on ly 200,000 people live in the sparsely -populated North West of Liberia. 30 % of the new patients are children below 14 years of age; worldwide the proportion is around 5 %. Leprosy doctors know that this high rate is a sure indic ation that many peo-ple are infected or sick with leprosy who have not yet been discovered.
Therefore DAHW banks on active e arly diagnosis. The leprosy experts swarm out to di stant regions of Nimba to find the people who infect others with lepro-sy. These journeys are complicated and expensive and so f ar it has only been possible to c over a third of the feder al state.
However, to s imply wait until patients come to the hospital of their own accord would be disastrous.
Lepra
162nd in the Human Development Index (out of 169 states), more than 80% of the population obliged to live on less than US$1 per day, one in every seven children dying before reaching his or her fifth birthday. Poverty is part and parcel of everyday life in Liberia, and consequently the diseases of poverty are too – especially leprosy.
Liberia: Poverty and leprosy in a forgotten land.
Six months’ treatment and strictly taking tablets lie before the boy. He gets his first tablets today.
“Frightened of leprosy and its stigma and frightened of being m arked by the di s-ease.” John tests the marks for sensitivity using cotton wool. Leprosy damages the nerves and c auses the ability to feel to dwindle. Each time Leeroy feels the cotton wool touching him he mu st say “Yes.” Close your eyes. The first mark. No feeling, just like the other two.
Now John feels along the nerve paths, searching for nodules. And all the time he speaks soothingly to the boy, saying that he doesn’t need to worry, his health will be restored completely because he has come to be examined early enough. Half an hour later it is clear: Leeroy is suffering from paucibacillary leprosy (PB), the s imple form. Six months of therapy are sufficient. He is given the first tablets immediately. He has u nderstood and a smile slowly comes back to his face.
John explains to Leeroy’s mother that he must take these t ablets every day from now on. Alex Vah is standing next to them, paying attention. He w ill keep his eye on things to m ake sure th at this will work. And he has the pa cks of tablets for the
months thereafter. Then they explain to the Chief and the teacher, informing them that from thi s day on nobody can be in-fected by Leeroy.
Meanwhile, Leeroy sees other c hildren making their way to the foot ball ground. He runs behind them. Without thinking about it he j oins one of the te ams and plays as if he h ad never done anything else. Almost a whole year of suffering and hiding away eradicated by a short exami-nation.
After the game Leeroy returns to his family exhausted, but happy. Everybody is glad that they now know more about the dis-ease which is so easy to heal, if it is exam-ined and treated in good time.
John Brimah packs his things and drives to the next village in this poor region. In all he will find ten new patients on this weekend, four of them children. “If we had more ve-hicles and trained teams we would discov-er far more patients,” he s ays very hope-fully. “And b y the time we h ave treated most of the patients, c hildren like Leeroy will no longer be able to become infected.”
11 DAHW Annual Report 2012
Many hide out of the fear of being stig-matised by leprosy or have already been chased out of their villages and forced to live in the bu sh. But these people c on-tinue to pass on the disease; the victims are especially children who have contact with the outcasts during play or on the way to school.
Until 1989 DAHW was represented in the country and actively supported the lep-rosy control programme. Although lep-rosy was present, it was under control. Thanks to suc cessful educational work only a few people sick with leprosy were outcast and ther e was ac cess to diag-nostics and tre atment almost every-where.
However, when c ivil war broke out the risks for its staff was too great and DAHW had to pull out of the country. Owing to the lack of national structures, the entire leprosy-control system broke down.
Now that peace is back and the c ountry has a functional government, DAHW has returned to Liberia. Dr. Pieter de Koning, formerly working as a doctor at the Würz-burg DAHW headquarters is currently es-tablishing a small, but already functional, leprosy programme at the Ganta location and in the federal state of Nimba.
Talks with the Ministry of Health are un-derway for further developing this work and soon a national leprosy control pro-gramme is to be in stalled. DAHW will continue to invest in thi s programme, but it will share the responsibility for it with the Liberian state.
Patients worldwide in 2011*New cases of leprosy worldwide: 229,328*
Cared for in DAHW projects: 41,467Proportion covered by DAHW worldwide 18.08 %
People with disabilities caused by leprosy: approx. 4 Mio.Cared for in DAHW projects: 225,000Proportion covered by DAHW worldwide 5.63 %
Leprosy figures
Spread of new leprosy cases in 2011
less than 500501 - 1,0001,001 - 4,0004,001 - 10,000more than 10,000
no data available
Prevalence*
* Sources: World Health Organisation (WHO) and national leprosy control programmes; the figures for 2012 will not be available until the end of 2013
Development* the statistically recorded incidences
0
200,000
400,000
600,000
800,000
2006 2007 2008 2009 2010 20112004 2005
Zontou, District Twan River
Ganta Rehab LeprosyHospital (Ganta)
Worldwide India Worldwide without India
DAHW Annual Report 201212
Tuberculosis
The treacherous epidemic and its victimsLots of work for DAHW in India
Jayan and his wife Shylaha can go back to a normal family life.
Phot
os: D
AHW
Indi
en
13 DAHW Annual Report 2012
family often, encouraging them and giv ing them security.” Japamala Bhavan, an on-site DAHW staff member, says. “One time we were visiting we di scovered conspicu-ous symptoms in the c hildren. They were coughing badly. The two little ones were examined; they had caught tuberculosis.
Their mother, Shylaha was di straught: “First my husband and now the c hildren,” she stammered. Tears were running down her face. Bhavan and hi s colleagues took care of the fr antic wife and soothed her . They assured her that they could and would help her children by means of an effective
treatment. From this time on they visited the family three time s a week bringing medicine and hope with them.
At last the first big day comes: Father Jayan has a negative result in the TB test; he is well again. Neighbours and friends share the family’s joy. And later, at the end of their treatment, the children are cured of the dis-ease. “The four of them st ill visit us occa-sionally,” Japamala Bhavan tells us, “and they thank us every time for helping so that today they are all well.”
Change of location: Hyderabad in the federal state of Andhra Pradesh
Almost 900 kilometres away from Kottay-am. DAHW teams are at work here too. One of them di scovered 13 year-old orphan, Sherly, in the K ukatpally slum are a. The only information was that the mother had spit blood shortly before she died. Conse-quently the helpers suspected that she had TB.
The girl was poorly. She was struggling be-cause of the loss of her parents; her we ak body was racked by daily fits of coughing. In the Siv ananda hospital multi-resistant TB bacteria were fin ally found. “The little one was in great danger,” says Nuthan, the director of the orphanage on the hospit al grounds.The fact that Sherly now lives here ultimate-ly saved her life because DAHW also works in the hospital which it has been support-ing for many years. It meant that the staff soon saw that the tre atment was working: “After twelve days her condition had per-
Kottayam, a town in south-west India Jayan and Shylaha live here w ith their
two children Vrundha and Ambady . Their quarter, Vellore, is a huge slum area, over-populated with many families living at very close quarters and almost all of them work as day labourers.
The meagre wages which father Jayan brings home in the evenings have to suffice for the next day. The principle here is from hand to mouth. But one day Jayan couldn’t go to work. He was weak, couldn’t get up and was coughing and a fever tortured his body. “We were terribly worried,” his wife, Shylaha, says.
The staff at DAHW were able to dispel her worries: “They took Jayan to the infirmary to be examined. After the examinations it was definite that he had tuberculosis.” But this worry did not last long because the teams are quick to inform the f amily and neigh-bours about the disease and its treatment. Jayaraman Ravichandran, DAHW represent-atives in India says: “We don’t just heal the disease we also take away the anxiety of the people surrounding our patients.”
The Indian D AHW teams always test rela-tives and neighbours of new patients. This is the only way they can prevent the lethal disease from spre ading even f aster. And they make checks that the medicine is be-ing taken regularly: if it is not taken until the disease has been completely cured, the surviving bacteria f orm resistances. This multi-resistant TB (MDR-TB) is extremely dif-ficult to tre at and gives rise to enormou s costs: up to 50 times more expensive than normal therapy. “This is why we visit the
“First my husband, and now the children” mother Shylaha lamented. But the two little ones bravely took their medicine regularly.
At last normal family life came back to them.
DAHW Annual Report 201214
Tuberculosis
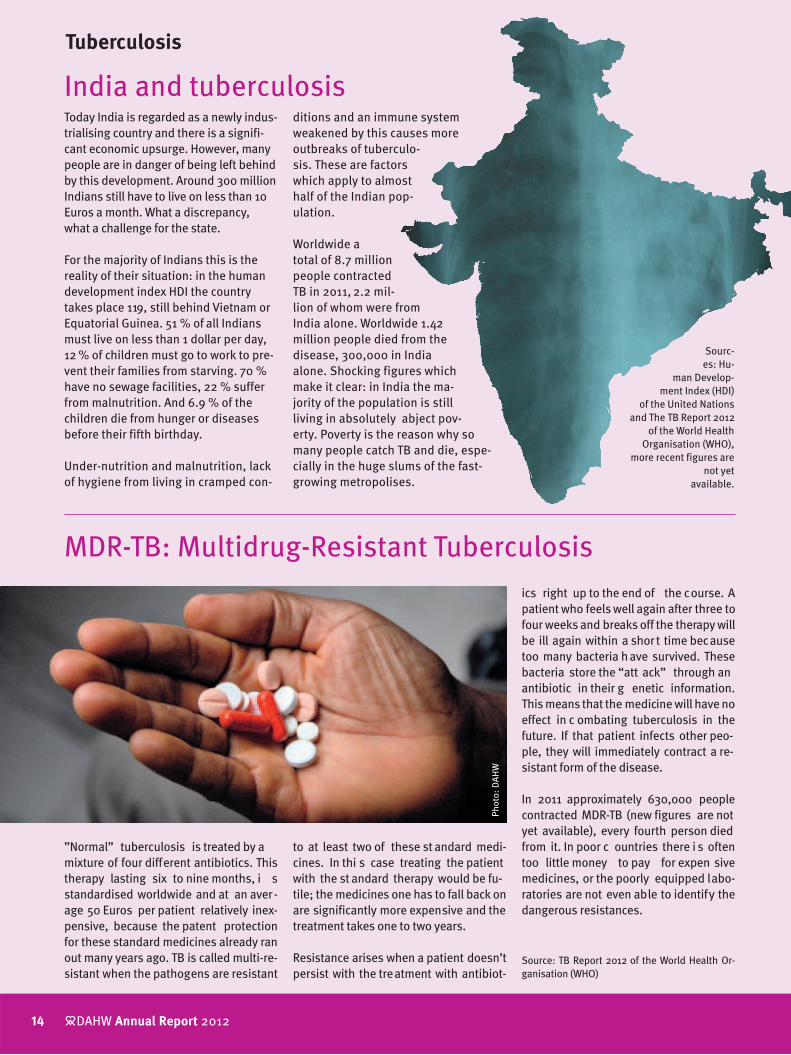
”Normal” tuberculosis is treated by a mixture of four different antibiotics. This therapy lasting six to nine months, i s standardised worldwide and at an aver-age 50 Euros per patient relatively inex-pensive, because the patent protection for these standard medicines already ran out many years ago. TB is called multi-re-sistant when the pathogens are resistant
Today India is regarded as a newly indus-trialising country and there is a signifi-cant economic upsurge. However, many people are in danger of being left behind by this development. Around 300 million Indians still have to live on less than 10 Euros a month. What a discrepancy, what a challenge for the state.
For the majority of Indians this is the reality of their situation: in the human development index HDI the country takes place 119, still behind Vietnam or Equatorial Guinea. 51 % of all Indians must live on less than 1 dollar per day, 12 % of children must go to work to pre-vent their families from starving. 70 % have no sewage facilities, 22 % suffer from malnutrition. And 6.9 % of the children die from hunger or diseases before their fifth birthday.
Under-nutrition and malnutrition, lack of hygiene from living in cramped con-
MDR-TB: Multidrug-Resistant Tuberculosis
India and tuberculosisditions and an immune system weakened by this causes more outbreaks of tuberculo-sis. These are factors which apply to almost half of the Indian pop-ulation.
Worldwide a total of 8.7 million people contracted TB in 2011, 2.2 mil-lion of whom were from India alone. Worldwide 1.42 million people died from the disease, 300,000 in India alone. Shocking figures which make it clear: in India the ma-jority of the population is still living in absolutely abject pov-erty. Poverty is the reason why so many people catch TB and die, espe-cially in the huge slums of the fast-growing metropolises.
Sourc-es: Hu-
man Develop-ment Index (HDI)
of the United Nations and The TB Report 2012
of the World Health Organisation (WHO),
more recent figures are not yet
available.
to at least two of these st andard medi-cines. In thi s case treating the patient with the st andard therapy would be fu-tile; the medicines one has to fall back on are significantly more expensive and the treatment takes one to two years.
Resistance arises when a patient doesn’t persist with the treatment with antibiot-
ics right up to the end of the course. A patient who feels well again after three to four weeks and breaks off the therapy will be ill again within a short time because too many bacteria have survived. These bacteria store the “att ack” through an antibiotic in their g enetic information. This means that the medicine will have no effect in c ombating tuberculosis in the future. If that patient infects other peo-ple, they will immediately contract a re-sistant form of the disease.
In 2011 approximately 630,000 people contracted MDR-TB (new figures are not yet available), every fourth person died from it. In poor c ountries there i s often too little money to pay for expen sive medicines, or the poorly equipped labo-ratories are not even able to identify the dangerous resistances.
Source: TB Report 2012 of the World Health Or-ganisation (WHO)
Phot
o: D
AHW
15 DAHW Annual Report 2012
ceptibly improved,” says Nuthan, “and her appetite had also increased.”
The health assistants explained to the 13 year-old how vital her treatment was, and also how impor tant protection ag ainst in-fection is: “Each time she has a fit of cough-ing she covers her mouth and nose to pro-tect the people around her." The director of the home is clearly proud of the girl under his care. “It’s not easy for her, especially as she has to carry on strictly with the MDR-TB treatment for 24 months.”
Tuberculosis Figures
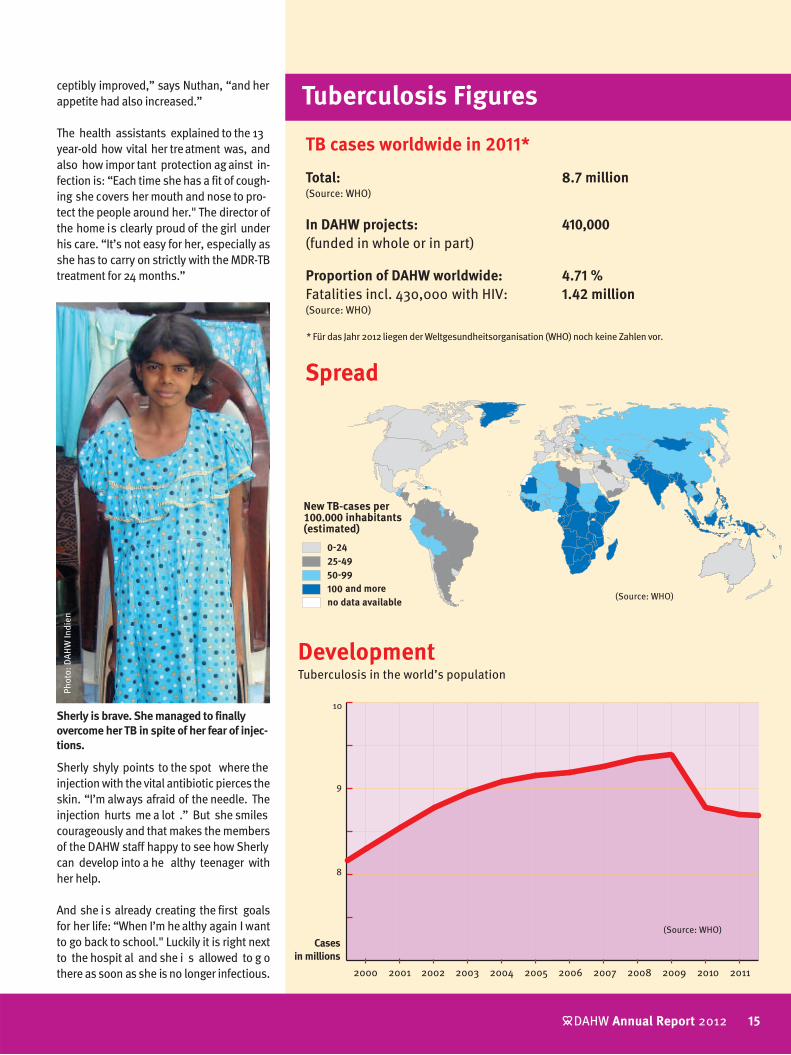
TB cases worldwide in 2011*
Total: 8.7 million(Source: WHO)
In DAHW projects: 410,000 (funded in whole or in part)
Proportion of DAHW worldwide: 4.71 %Fatalities incl. 430,000 with HIV: 1.42 million(Source: WHO)
Spread
DevelopmentTuberculosis in the world’s population
* Für das Jahr 2012 liegen der Weltgesundheitsorganisation (WHO) noch keine Zahlen vor.
Sherly shyly points to the spot where the injection with the vital antibiotic pierces the skin. “I’m always afraid of the needle. The injection hurts me a lot .” But she smiles courageously and that makes the members of the DAHW staff happy to see how Sherly can develop into a he althy teenager with her help.
And she is already creating the first goals for her life: “When I’m he althy again I want to go back to school." Luckily it is right next to the hospit al and she i s allowed to g o there as soon as she is no longer infectious.
Sherly is brave. She managed to finally overcome her TB in spite of her fear of injec-tions.
Phot
o: D
AHW
Indi
en
(Source: WHO)
Compared with earlier times, it only takes a few days to identify the disease. Sample tissue is analysed directly in the local laboratory.
The diagnosis Buruli Ulcer is especially hard for children to bear.
Neglected Diseases
DAHW Annual Report 201216
Buruli Ulcer: the little sister of leprosyDAHW active in Togo, one of the poorest countries
Buruli Ulcer affects children above all: around 70 % of all patients are under
15. Reason enough for Franz Wiedemann, the DAHW representative in Togo, to con-cern himself with this disease in addition to leprosy and t uberculosis. DAHW has been supporting the national Buruli pro-gramme since 2006. Up u ntil then it had virtually only existed on paper.
Just two years later the then Federal Ger-man Minister of Foreign Affairs, Frank-Walter Steinmeier and the Togolese Min-ister of Health, Kondi Charles Agba opened the Buruli Competence Centre in Tsévié where the most severely sick Bu-ruli patients receive medical treatment.
If a patient is discovered too late the only option is operations and sk in trans-plants; often amputations are necessary. However, if the disease is discovered in time, it can be he aled completely and there are no long-term effects. As is the case with leprosy, there are DAHW health assistants travelling around all districts in Togo to provide explanations to peo-ple, to diagnose su spected cases and to initiate treatment as fast as possible. They are the key element both in terms of care and the project work.
Until now, at the Tsévié Buruli C entre samples of tissue were removed from the victims on the spot and sent to Germany for laboratory diagnosis. For a long time there was no laboratory in Togo capable of performing the PCR test, a g enetic analysis enabling Buruli to be diagnosed conclusively. The result was not available for five to s ix weeks. This unnecessarily long wait also delayed the start of treat-ment for many patients.
Together with partners from the Ludwig-Maximilians Uni-versity in Munich (LMU) and from the Bernhard-Nocht In-stitute in Hamburg (BNI) and also with the Europe an Bu-ruliVac research project, Franz Wiedemann has suc-ceeded in setting up an ap-propriate laboratory in Togo. Today the PCR diagnosis only takes seven days.
As in m any other Afric an countries Togo has too few doctors, surgeons and p sy-chologists. They migrate to other countries because they can earn more money there.
This poor country simply hasn’t the funds to pay doctors appropriately.
“Our greatest problem at the moment is mobility,” Wiedemann says. “Without motorbikes and cars we cannot find and treat patients soon enough.” In the course of the next two years DAHW in Togo will require 41 motorbikes and 5 new motor vehicles.
Phot
os: F
ranz
Wie
dem
ann
The DAHW staff will be faced with an-other challenge in 2013: The ancient, almost forgotten disease known a s Yaws. “It reveals itself by a bad r ash on the f ace and h ands” Wiedemann recounts. “Luckily this bacterial infec-tion is relatively easy to he al by means of antibiotics.” It is spread through contact with people who are already infected. In view of the good chances of it healing fast it seems al-most harmless compared to Buruli Ulcer and leprosy.
17 DAHW Annual Report 2012
Buruli Ulcer, the unknown disease
Buruli Ulcer is a disease which is fre-quently referred to a s “Leprosy’s lit-
tle sister”. The pathogen is closely re-lated to the leprosy bacterium and the consequences are also s imilar: For a long time patients don’t notice that they are infected with a destructive disease.
If untreated, both diseases can lead to very severe di sabilities and in soc iety the patients are stigmatised. Buruli Ul-cer and leprosy are to be fou nd in the group of “mysterious” diseases; the WHO classifies them in the category “ne-glected tropical diseases.”
However there are diff erences: Buruli patients often suffer from open wounds covering a large area, contrary to leprosy Buruli does not cause any nerves to be-come infected, but it destroys the entire skin and muscle structure right down to the bone. Lik e leprosy, Buruli c an be healed, but one c an be re-infected re-peatedly which extremely rarely occurs with leprosy after a suc cessful treat-ment.
The disease is not passed on due to con-tact with victims, but probably by insects which live in wetl ands. However, this is only conjecture because this disease has been so little researc hed that even experts are often faced with mysteries.
There is no fast and accurate test for the disease; a definite diagnosis can only be obtained by means of a so-c alled PCR test (Polymerase Chain Reaction), a ge-netic examination of skin tissue samples taken from the wounds.
Mensanh, a 15 year-old girl from Togo contracted Buruli when she was a
child, before DAHW could take care of the disease.
Because treatment came so late, Mens-anh has defective positions in both legs and stiffened knee j oints. Without her wheelchair, a tricycle with hand pedals, she would be u nable to do even the simplest everyday things.
Her old wheelchair could hardly be mo-ved any more, but the DAHW staff were able to pro vide her w ith a new one. Tears of emotion and happiness flowed when she sat in the vehicle for the first time and now she can at last go back to school with it.
But eleven-year-old Eli i s receiving in-patient treatment in Tsévié. A Buruli-Ulcus, the ulcer which is typical for this disease, and by which it is named, has formed dangerously close to hi s left eye.
Eli had an ulcer on his eye and could no longer shut his eyelid. He was in danger of losing the eye completely. Thanks to a donation it was possible perform the necessary operations. Further opera-tions are necessary. A specialist surge-on is due to per form the oper ation in the autumn of 2013. Donations for this are needed urgently. The costs will add
Changing fates: DAHW helps Buruli victims
up to around EUR 7,500 even if the Ger-man doctors work for nothing.
Eli and Mensanh are not the only cases which DAHW treats in Togo. Each year children and young people who h ave incurred extremely severe injuries from Buruli Ulcer undergo surgery. And also children who, after the l aboratory ana-lysis, turn out not to have Buruli are tre-ated by DAHW if possible. DAHW and one of its partners sponsor a wou nd project to the t une of EUR 50,000. In 2012 over 1,000 people with all sorts of wounds were c ared for in southern Togo. Here, too, new fu nds must be found to be ab le to continue the work after 2013.
Mensanh still moves around on her old tricycle. The DAHW is helping and the 15 year-old is now looking forward to a modern wheelchair.
Little Elie had an abscess on his eye. Thanks to a donation he was able to be operated. His sight was preserved.
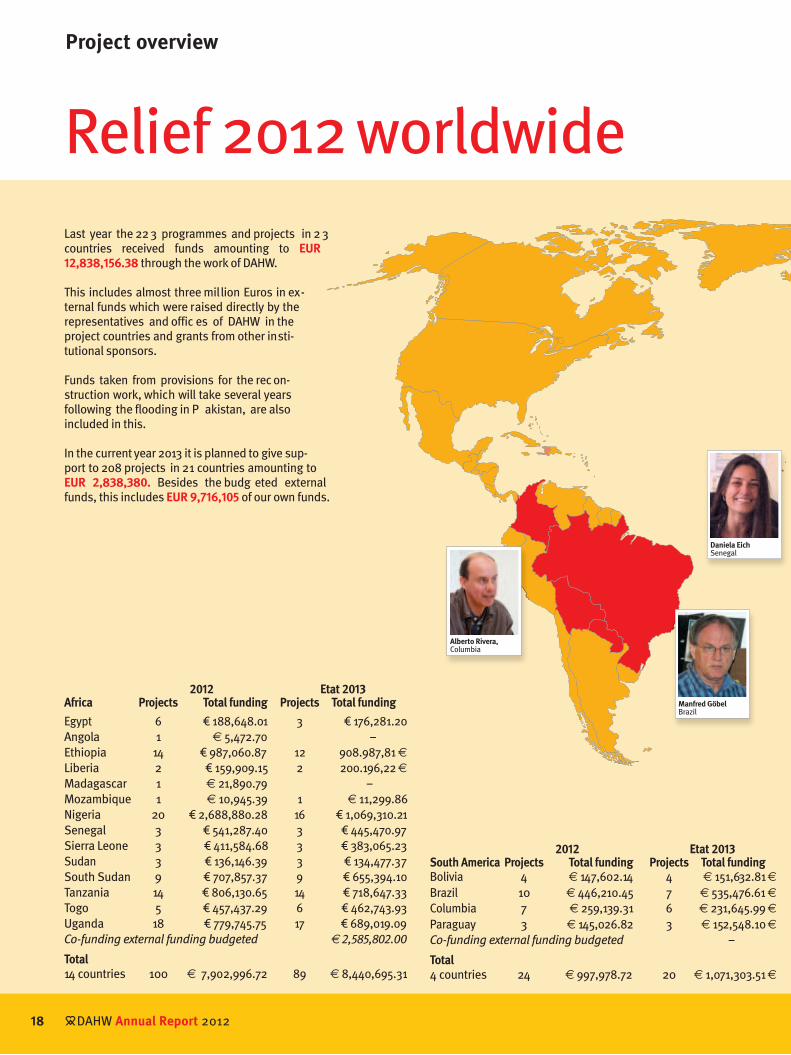
Project overview
Last year the 223 programmes and projects in 2 3 countries received funds amounting to EUR 12,838,156.38 through the work of DAHW.
This includes almost three million Euros in ex-ternal funds which were raised directly by the representatives and offic es of DAHW in the project countries and grants from other insti-tutional sponsors.
Funds taken from provisions for the rec on-struction work, which will take several years following the flooding in P akistan, are also included in this.
In the current year 2013 it is planned to give sup-port to 208 projects in 21 countries amounting to EUR 2,838,380. Besides the budg eted external funds, this includes EUR 9,716,105 of our own funds.
Total5 countries 83 € 3,645,182.87 83 € 2,738,073.19
Research, training and further education2012 2013
Projects Total funding Projects Total fundingApplied Research 5 € 84,615.02 4 € 98,414.00Basic Research 1 € 15,000.00 – –Misc Leprosy Research 1 € 40,941.10 1 € 65,000.00Non-Leprosy Research 1 € 40,000.00 1 € 40,000.00Scientific Support 2 € 12,768.36 2 € 118,000.00Training 3 € 2,926.18 5 € 130,894.00General Field Supply 3 € 95,747.41 3 € 136,000.00
Total 16 € 291,998.07 16 € 588,308.00
Phot
os: J
udith
Mat
hias
ch
below € 100,000
€ 100,000 to € 500,000
above € 500,000
Sponsorship by country
Dr. Jasin Al QubatiJemen
Mohammed AhmedEthiopia
Dr. Yvonne HardingSierra Leone
Olaf HirschmannUganda
Burchard RwamtogaTanzania
Gerhard ÖhlerNigeria
J. RavichandranIndia
Dr. Emile TanyousNorth Sudan
Leonore KüsterSouth Sudan
Franz WiedemannTogo
Disability
DAHW Annual Report 201220
The tragedy of the twins, Jaykant and JaykantiDAHW supports people with disabilities on their way out of dependency.
Phot
os: R
olf B
auer
dick
21 DAHW Annual Report 2012
Over ten years have passed since Ramp-yari brought healthy twins into the world, a girl and a boy called Jaykant and Jaykanti. The brother and s ister devel-oped well and bec ame lively, cheerful children. To make sure they remained healthy the young mother regularly vis-ited the medical check-ups provided by the state of Nepal for babies during the first twelve months of their lives.
Rampyari had the tw ins vaccinated against such diseases and infections as tetanus, measles and diphtheria whic h she knew to be a seriou s threat to the lives of children living in poor c ondi-tions.
Rampyari had no idea that vaccines only give protection if they are used accord-ing to the in structions. However, in Ne-pal negligence and defic ient medical standards brought a tr agedy upon Jay -kant and Jaykanti.
“After one of the vaccinations the chil-dren vomited,” their mother rel ates. “First Jaykanti had a very high fever, and then her brother . Both of them went completely limp and c ouldn’t even crawl.” They also lagged behind in their mental development. Cerebral palsy was the diagnosis, most probably triggered by contaminated serum.
This is a mi sfortune which occurs fre-quently in Nepal, as Prakash Pahari from
the International Nepal Fellowship (INF) organisation knows only too well. “It is not uncommon for vaccines to be stored for far too long, or destroyed b y exces-sive heat.” This is because in towns like Nepalgunj there can be numerous power failures per day.
The major city on the border between Nepal and India is dusty, hot and filthy. It is disastrous for people w ith disabili-ties in Nepalgunj. DAHW and its project partner of long st anding, INF, bank on targeted rehabilitation programmes. For example Kalem, a par aplegic who fel l down a steep slope while gathering ani-mal fodder, today travels around in a new wheelchair as a mobile small trader for his family.
And there is warm-hearted Saradha who was outcast as a little girl and as a wom-an cannot find a hu sband because she has difficulty walking as a consequence of polio; she was given the opportunity to run a kiosk. And the desperate mother of the tw ins, Rampyari has also found her way back to contentment.
After being trained by staff at the INF she does physiotherapeutic exercises with Jaykant and Jayk anti. “Jaykanti is al-ready able to e at without help and i s now learning to stand on his own feet.”
The DAHW and its partner, INF, support people with disabilities in self-help groups.
Vaccines are often unusable in Nepal owing to negligence. It is why Rampyaris' twins are disabled. They were not disabled before the vaccination.
According to st udies by the World Health Organisation (WHO), 10% of
all people world-w ide live w ith disabili-ties. It is their greatest objective to live in a self-determined manner.
Day-to-day problems are not easy to over-come, even in a rich country such as Ger-many. In poor countries, where most peo-ple fear for their daily existence, a disabil-ity presents a huge obstacle.
Poor countries face enormous problems with their health systems as it is: medical staff, medication, technology and logi s-tics are frequently very scarce. Since the system cannot help them, m any people with disabilities have established self-help groups in these countries.
The DAHW Deutsche Lepra- und Tuberku-
losehilfe has been supporting such groups of people for many years now. For those affected, it is a means participating in society, of leading a dignified life, irre-spective of whether the di sability is the result of having had leprosy in e arlier years or not.
DAHW supports people with disabilities
In their self-help groups, they are perfect-ly normal members who are accepted like any other member . In these self -help groups at least, they do not experience any discrimination due to their illness.
Roads are scarce: people have to carry almost everything themselves.
DAHW Annual Report 201222
Die CBR-Arbeit (CBR: „community based rehabilitation“, Rehabilitation
im gewohnten Umfeld) hat sich zum Ziel gesetzt, betroffenen Menschen eine Teil-habe am gesellschaftlichen Leben zu er-möglichen. Dazu gehört der Kampf gegen Diskriminierung ebenso wie eine men-schenwürdige Arbeit, mit der diese Men-schen für ihren L ebensunterhalt sorgen können.
Die Gruppen organisieren sich selbst und die einzelnen Mitglieder helfen s ich ge-genseitig.
Die Sozialarbeiter der DAHW unterstützen sie bei al len auftretenden Prob lemen, beispielsweise gegenüber Behörden oder bei fehlenden finanziellen Möglichkeiten. Nicht nur bei der klassischen Lepra-Arbeit geht es neben der rein medizinischen Hilfe auch um soziale Unterstützung.
CBR setzt auf Eigenverantwortlichkeit. Die Devise lautet, die Zukunft in die ei-gene Hand zu nehmen. Ein w ichtiger Punkt um Ideen verwirklichen zu können, ist Geld: Durch Mikrokredite können sich die Mitglieder der Gruppen das Werkzeug für ihre Arbeit oder eine erste Aus stat-tung ihres kleinen Geschäfts besorgen. Manche benötigen auc h etwas Geld für ein menschenwürdiges Dach über dem Kopf. Mit ihren Einkünften zahlen sie die kleinen Kredite zurück.
Viele Jahre lang hat sich die DAHW um die Menschen gekümmert, die als Spätfolge ihrer früheren Lepra-Erkrankung mit Be-hinderungen leben müs sen. Aus diesen SER-Programmen (SER: social and ec o-nomic rehabilitation) wurden in den ver-gangenen vier Jahren CBR-Programme.
Die DAHW unterstützt CBR-Projekte in vielen Ländern:
In Äthiopien, Indien, K olumbien, Nepal, Nigeria, Senegal, Sierra Leone, Uganda und Tansania wurden D AHW-Mitarbeiter zu CBR-Beratern ausgebildet oder bereits ausgebildete Berater eingestellt. Darüber hinaus unterstützt die DAHW ihren Partner in Ägypten bei der Einführung von CBR.
Disability
It is not only to climb Mount Everest that mountain climbers from al l over the
world come to Nepal: Nepal is home to eight of the 10 highest mountains in the world, and ever y year around 300,000 tourists visit the country which has around 30 million inhabitants.
The drawback to this paradise for moun-tain climbers: over half of the country is made up of high mountains, making the already harsh life even more difficult. Many places are h ardly accessible, and not at all during the long w inters. This has a detrimental effect on f arming as well as on health care.
The average income is around €25 a month, considerably less in the mou n-tains. 80% of all Nepalese work in agri-culture. Almost 7 0% have to sur vive on less than $1 a day; 55% on les s than $0.50 (€0.36). 3 1% of all children be-tween the ages of 5 and 14 work to enable their families to survive: as a result, 42% of the Nepalese are illiterate.
4.1% of children die during birth or short-ly afterwards. A further 5.1% don’t make it to their fifth birthday. There is one doctor for 5,000 people here (in Germ any it is one to 300). The poor infrastructure fre-quently prevents patients from getting to a doctor in time.
The lack of roads means that almost all goods must be tr ansported laboriously on foot. People also take advantages of any chance they have to harvest plants or to graze their anim als. This results in a very high number of accidents and sub-sequent disabilities.
Organisations such as the Intern ational Nepal Fellowship (INF) have been estab-lished as self-help groups of people with disabilities. DAHW has been supporting these groups for many years since many leprosy patients also h ave to live their lives with disabilities. The self-help groups ensure that people lead as normal a life as possible despite their di sability and that they can earn their own living.
Source: Human Development Index HDI
Nepal – the land with no roads
DAHW und CBR
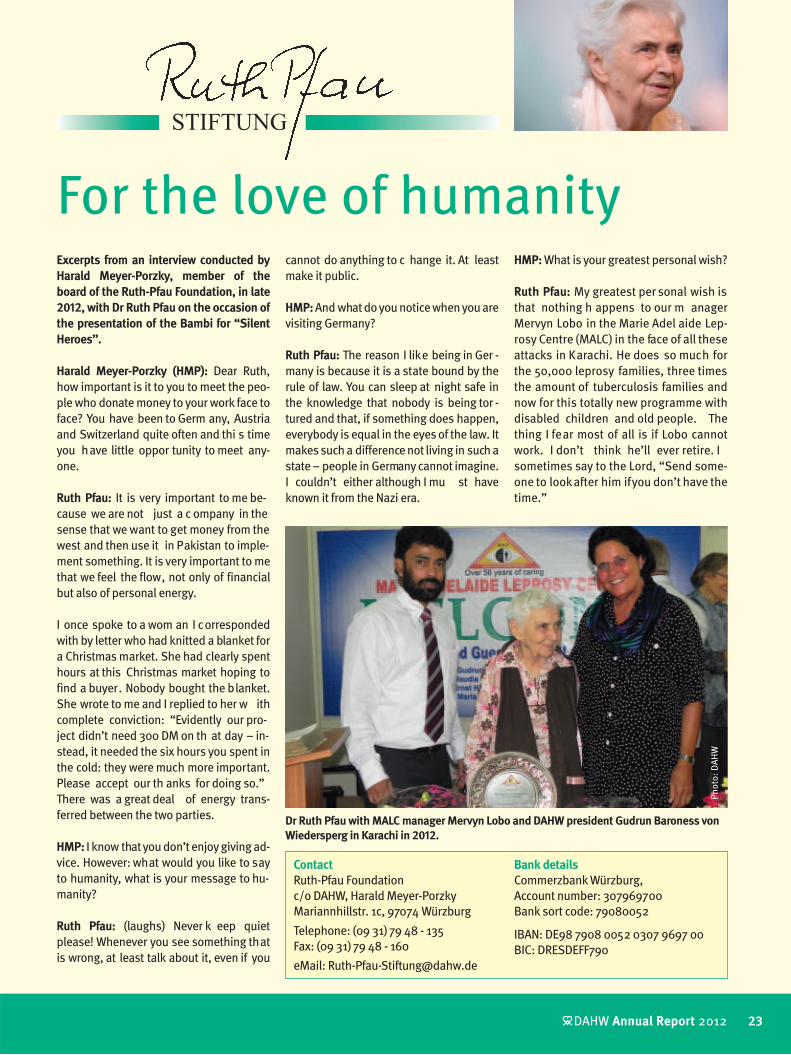
Excerpts from an interview conducted by Harald Meyer-Porzky, member of the board of the Ruth-Pfau Foundation, in late 2012, with Dr Ruth Pfau on the occasion of the presentation of the Bambi for “Silent Heroes”.
Harald Meyer-Porzky (HMP): Dear Ruth, how important is it to you to meet the peo-ple who donate money to your work face to face? You have been to Germ any, Austria and Switzerland quite often and thi s time you have little oppor tunity to meet any-one.
Ruth Pfau: It is very important to me be-cause we are not just a c ompany in the sense that we want to get money from the west and then use it in Pakistan to imple-ment something. It is very important to me that we feel the flow, not only of financial but also of personal energy.
I once spoke to a wom an I corresponded with by letter who had knitted a blanket for a Christmas market. She had clearly spent hours at this Christmas market hoping to find a buyer. Nobody bought the blanket. She wrote to me and I replied to her w ith complete conviction: “Evidently our pro-ject didn’t need 300 DM on th at day – in-stead, it needed the six hours you spent in the cold: they were much more important. Please accept our th anks for doing so.” There was a great deal of energy trans-ferred between the two parties.
HMP: I know that you don’t enjoy giving ad-vice. However: what would you like to say to humanity, what is your message to hu-manity?
Ruth Pfau: (laughs) Never k eep quiet please! Whenever you see something that is wrong, at least talk about it, even if you
For the love of humanitycannot do anything to c hange it. At least make it public.
HMP: And what do you notice when you are visiting Germany?
Ruth Pfau: The reason I like being in Ger -many is because it is a state bound by the rule of law. You can sleep at night safe in the knowledge that nobody is being tor -tured and that, if something does happen, everybody is equal in the eyes of the law. It makes such a difference not living in such a state – people in Germany cannot imagine. I couldn’t either although I mu st have known it from the Nazi era.
HMP: What is your greatest personal wish?
Ruth Pfau: My greatest per sonal wish is that nothing h appens to our m anager Mervyn Lobo in the Marie Adel aide Lep-rosy Centre (MALC) in the face of all these attacks in Karachi. He does so much for the 50,000 leprosy families, three times the amount of tuberculosis families and now for this totally new programme with disabled children and old people. The thing I fear most of all is if Lobo cannot work. I don’t think he’ll ever retire. I sometimes say to the Lord, “Send some-one to look after him if you don’t have the time.”
Dr Ruth Pfau with MALC manager Mervyn Lobo and DAHW president Gudrun Baroness von Wiedersperg in Karachi in 2012.
Bank detailsCommerzbank Würzburg, Account number: 307969700Bank sort code: 79080052
IBAN: DE98 7908 0052 0307 9697 00BIC: DRESDEFF790
23 DAHW Annual Report 2012
Phot
o: D
AHW
DAHW Annual Report 201224
The initiatives for the promotion of DAHW organise and plan their activ i-
ties throughout the whole year in order to achieve the best possible advantages for DAHW at their events. The on-site “per-suasion work” is at least as important as the income and the l ater revenue from the campaigns which go to DAHW. With their good names, the active participants
The support of volunteers for the objectives of DAHWThey are organised in groups or act as “lone warriors” in their region: around 2,000 people worked in a voluntary capacity for the DAHW Deutsche Lepra- und Tuberkulosehilfe in 2012. In addition to tried-and-tested, successful campaigns, they continually develop new campaign models.
vouch for D AHW in their pl aces of resi-dence, and this convinces people.
At the international children’s festival in Würzburg, for in stance, Bavaria’s big-gest children’s festival, at the duck race in Balingen, eating ravioli in Metzingen, at the baked apple campaign in Bad Sal-zuflen (this is only a selection from hun-
The Balingen campaign group has already amassed more than € 100,000 with its duck races, transferring it to DAHW as a donation.
Minister-President Hannelore Kraft talking to DAHW volunteers and pupils from North Rhine-Westphalia, who presented the work of DAHW to the federal state parliament in Düsseldorf on the occasion of World Leprosy Day.
Carmen Dietrich is in charge of the Seve-rin campaign group in Uchtelfangen in Saarland. This group has been collecting money by means of a large bazaar for over 40 years now.
The Leprosy campaign group at the parish of Namen Jesu in Munich was given an award for its 35 years of voluntary aid. Manager Paul Frosch proudly presents the certificate.
Ehrenamt
dreds of campaigns) or at one of the nu-merous bazaars organised by many groups, especially in the ru n-up to Christmas. The volunteers ensure the success of these campaigns and the suc-cess of DAHW in their region. D AHW would like to take this opportunity to ex-press a “heartfelt thank-you for this in-credible commitment”.
Phot
os: D
AHW
Report by the Financial Director
DAHW Deutsche Lepra- und Tuberku-
losehilfe e.V. doesn’t mind showing its books to any one. When all is said and done, it is money from donors who want to help people suffering from di s-eases caused by poverty. For that rea-son, DAHW undergoes two voluntary audits and also f aces a critical evalua-tion of its reporting on the applic ation of funds in the Transparency Award.
The attestation of an ac countant, in compliance with strict specifications and standards, was carried out by the Hemberger Prinz Siebenlist auditing company for the year 2012. The audit-ing was carried out based on the regulations pertaining to Commercial Law, in c ompli-ance with the Institute of Au-ditor standards for auditing associations.
The auditors provided DAHW with a good report: “Accord-ing to our ev aluation based on the inform ation gleaned during the audit, the annual accounts comply with the le-gal regulations and the sup-plementary stipulations of the memorandum and st at-utes, taking into account the principles of adequate and orderly accounting. They convey a pict ure of the a s-set, financial and profit situ-ation of the a ssociation which corresponds to the actual circumstances.“
Donations in good hands
Göttingen, their exper ts in-spect the reporting of aid or-ganisations with regard to the way they use the don a-tions. DAHW has been partic-ipating in this since 2007 and has always come out above average, including in 2012. In some areas, DAHW was even assessed as being “exempla-ry”.
DAHW attaches great impor-tance to these independent audits so that all donors can see for themselves that their money is in good hands and that it reaches the people suffering from po verty-relat-ed diseases.
As the honorary financial ex-ecutive of DAHW, I guarantee
that your donations are in good hands. We work on using this money to provide the best possible aid to the people in the projects. We see the pos itive re-ports by the independent auditors as confirmation that we have been doing a good job to date..
Peter HofmannGraduate in Business ManagementHonorary Financial Director of DAHW
Peter HofmannGraduate in Business Management
Honorary Treasurer
25 DAHW Annual Report 2012
The audit by the Deutsche Zentralinsti-tut für soz iale Fragen (German Central Institute for Social Issues - DZI) is also voluntary. This organisation, also known as the “don ation MOT” awards its DZI seal to exceptionally trustworthy relief organisations. Relief organisa-tions wishing to be awarded this much sought-after seal must undergo a com-plete auditing of their finances. DAHW has been doing this for years, and pro-vides the auditors with full insight into all of the org anisation’s documenta-tion. In this manner, the DZI can see for itself that the aid reaches those people for whom the appeal was set up.
The auditors at DZI had a good look at the finances of DAHW and appro ved them. Hence, DAHW was once again awarded the DZI seal of approval for be-ing a trustworthy relief organisation.
The third audit, which is also voluntary, is participation in the tr ansparency prize of the Pric eWaterhouseCoopers auditing company. Along with experts from the Georg-Augu st University in
DAHW Annual Report 201226
Financial report from 01.01.2012 to 31.12.2012
Income 2012 20111. Donations and subsidies– Donations € 9,319,674.95 € 9,107,456.33
– Fines € 110,605.46 € 186,390.00
– Inheritances and legacies € 3,144,742.27 € 2,803,886.52
Total donations € 12,575,022.68 € 12,097,732.85
Donations used not yet in accordance with the memorandum and statutes € 506,480.00 € € 1,146,379.00
– Income from ILEP members € 417,530.32 € 607,568.84
– Subsidiaries from the Federal German government (BMZ), the federal states, the Kreditanstalt für Wiederaufbau (KfW) and the European Union (EU) € 97,190.93 € 239.04
– Direct subsidies from third party funds € 1,532,462.87 € 1,685,701.09
5. Miscellaneous and other expenses € 26,148.04 € 19,411.06
Total expenses € 16,698,603.62 € 16,499,437.34
27 DAHW Annual Report 2012
Balance sheet
DAHW Deutsche Lepra- und Tuberkulose-
hilfe e.V. had its year-end accounts done taking into c onsideration §§ 2 42 of the Commercial Code (HGB) and drew up its balance sheet based on the c ommercial law classification scheme of § 266 of the Commercial Code.
The balance sheet was drawn up and as-sessed in accordance with the principles of adequate and orderly accounting, tak-ing into account the minimum value prin-ciple and in accordance with due commer-cial caution.
The fixed assets are evaluated at the ac-quisition / production costs minus the de-ductions accumulated to date and contin-ued according to sc hedule in the 20 12 business year. Depreciation relating to the fixed assets is carried out in accordance with the linear deduction method.
DAHW used the tax simplification right of election: receivables and other intangible assets are fixed at the nominal value. De-fault risks are taken into consideration by appropriate valuation adjustment. Cash balance and credit balance at banks are put at their nominal amounts.
The reserves correspond to a re asonable business appraisal. The liabilities are classified at the pertinent amounts repay-able.
Income and expenses
In turn, income generated from donations as well as inheritances and legacies have increased slightly, whereas the subsidies from ILEP Members and third-party do-nors have fallen slightly in the year 2012. Overall, however, these c hanges are slight, which contributes towards very good planning reliability.
This is expressed in the expenses, where the total increased slightly over the previ-ous year. Whereas, in 20 11, a surplu s of
€391,032.67 was recorded, which was al-located to reserves, there was a shortfall of €192,873.88 in the year 2012 which is under review and which is balanced out by a withdrawal from the reserves.
In proportion to all income and expenses, however, there is both a surplu s (2.37%) and a shortfall (1.16%) on a scale which is something to be proud of and which bear witness to the respon sible budgeting of the expenses.
Explanations on the balance sheet, income and expenses
Expenditure in 2012
Income 2012
Fines 0,66 %
Inheritances and legacies 18,83 %
Public grants 0,58 %
Grants from members of ILEP 2,50 %
Third party funds, direct grants 9,18 %
Interest and similar income 7,84 %Other income 4,6 %
Donations 55,81 %
Information and PR work*15,94 %
Administration 5,95 %Asset management 1,07 %
Other and extraordinary expenses 0,16 %
Project work 76,88 %
* The item “Information and PR work” encompasses development-related education work for schools, advocacy and lobbying work as well as press and media work, support of voluntary work, communication with donors and advertising in accordance with the statutes.
The expenses for information and PR work are characterised by the tasks established in the D AHW statutes such as develop-ment-related education work, adv ocacy and lobbying, as well as press and media work.
Furthermore, in addition to adver tising, the PR work includes communication with the donors and s upervision and suppor t of the many people who work in a volun-tary capacity for DAHW.
DAHW Annual Report 201228
Liabilities side 2012 2011A, Capital resourcesI, Donations (until 31,12,1976) € 28,318,905.32 € € 28,318,905.32II, Estate and inheritance funds
Status on 01,01, € 9,234,019.01 € 8,842,986.34Withdrawal from reserves € - 192,873.88 0.00 Transfer to reserves € 0.00 € 391,032.67
B, Not yet used donations Pakistan food relief status € 1,500,000.00Withdrawals € -800,000.00Transfers € 443,520.00Donations not yet used country offices
co-founder Hermann Kober has been dead for many years. In many countries, our staff sees to it that leprosy is no longer an inev itable fate. The lives of those suffering from tuberculosis are
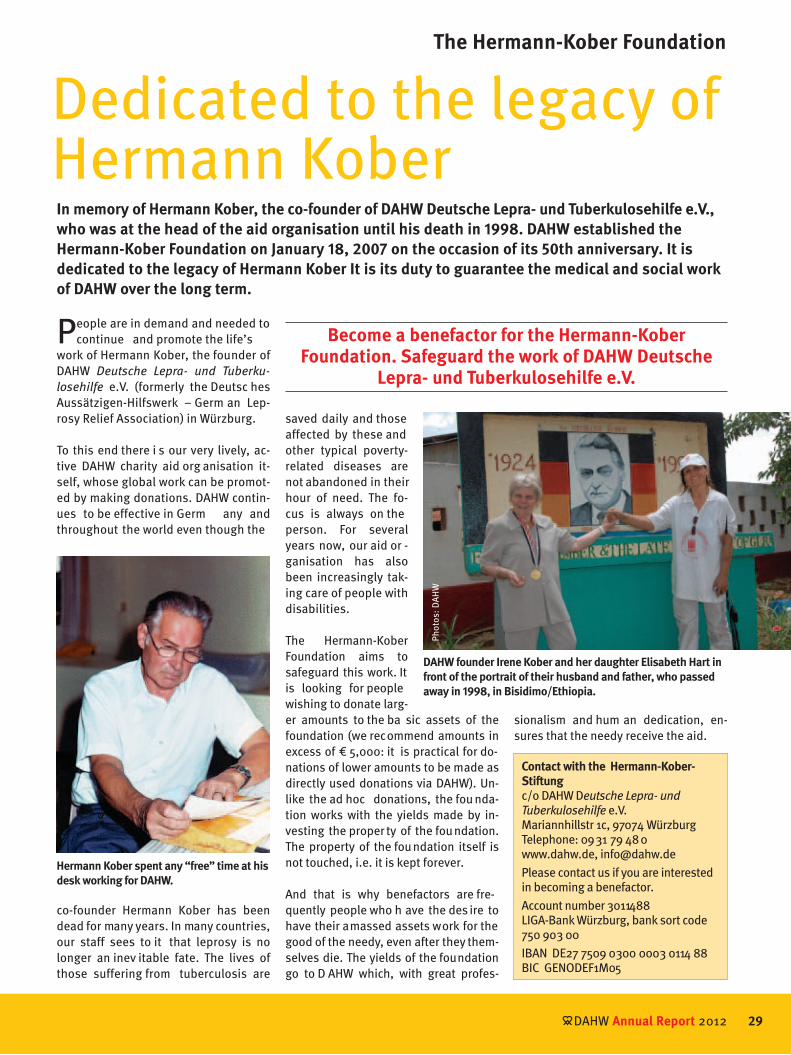
Dedicated to the legacy of Hermann KoberIn memory of Hermann Kober, the co-founder of DAHW Deutsche Lepra- und Tuberkulosehilfe e.V., who was at the head of the aid organisation until his death in 1998. DAHW established the Hermann-Kober Foundation on January 18, 2007 on the occasion of its 50th anniversary. It is dedicated to the legacy of Hermann Kober It is its duty to guarantee the medical and social work of DAHW over the long term.
Contact with the Hermann-Kober-Stiftungc/o DAHW Deutsche Lepra- und Tuberkulosehilfe e.V.Mariannhillstr 1c, 97074 WürzburgTelephone: 09 31 79 48 0www.dahw.de, [email protected] contact us if you are interested in becoming a benefactor.Account number 3011488LIGA-Bank Würzburg, bank sort code 750 903 00IBAN DE27 7509 0300 0003 0114 88BIC GENODEF1M05
saved daily and those affected by these and other typical poverty-related diseases are not abandoned in their hour of need. The fo-cus is always on the person. For several years now, our aid or -ganisation has also been increasingly tak-ing care of people with disabilities.
The Hermann-Kober Foundation aims to safeguard this work. It is looking for people wishing to donate larg-er amounts to the ba sic assets of the foundation (we recommend amounts in excess of € 5,000: it is practical for do-nations of lower amounts to be made as directly used donations via DAHW). Un-like the ad hoc donations, the fou nda-tion works with the yields made by in-vesting the proper ty of the foundation. The property of the foundation itself is not touched, i.e. it is kept forever.
And that is why benefactors are fre-quently people who h ave the des ire to have their amassed assets work for the good of the needy, even after they them-selves die. The yields of the foundation go to D AHW which, with great profes-
Become a benefactor for the Hermann-Kober Foundation. Safeguard the work of DAHW Deutsche
Lepra- und Tuberkulosehilfe e.V.
Hermann Kober spent any “free” time at his desk working for DAHW.
DAHW founder Irene Kober and her daughter Elisabeth Hart in front of the portrait of their husband and father, who passed away in 1998, in Bisidimo/Ethiopia.
sionalism and hum an dedication, en-sures that the needy receive the aid.
People are in demand and needed to continue and promote the life’s
work of Hermann Kober, the founder of DAHW Deutsche Lepra- und Tuberku-
losehilfe e.V. (formerly the Deutsc hes Aussätzigen-Hilfswerk – Germ an Lep-rosy Relief Association) in Würzburg.
To this end there i s our very lively, ac-tive DAHW charity aid org anisation it-self, whose global work can be promot-ed by making donations. DAHW contin-ues to be effective in Germ any and throughout the world even though the
Phot
os: D
AHW
DAHW Lepra-Spezial 200530
DAHW CALENDAR OF EVENTS 2012
January 2012DAHW celebrates its 55th anniversary with a small, internal birthday party in Würz-burg. The co-founder of the aid org anisa-tion, Irene Kober, also attended, celebrat-ing her birthday at the same time.
March 2012Dr Chris Schmotzer visits the DAHW head-quarters in Würzburg, and reports on her work in Pakistan. She has been working in the Rawalpindi hospital in the mountains of the northern Pakistani province of Pun-jab since 1988.
A tour of DAHW – a review of the year
February 2012DAHW presents its work in a prominent po-sition: in the Bavarian state parliament in Munich, following an invitation from Bar-bara Stamm, the president of the Bavarian state parliament. D AHW contributes the story of a woman who is infected with tu-berculosis in Brazil to the “Entwicklungs-land Bayern” travelling exhibition.
30 DAHW Annual Report 2012
Along with her husband Hermann Kober Irene Kober (centre) was co-founder of DAHW. Photo: DAHWBarbara Stamm, president of the
Bavarian federal state parliament,
visits the DAHW stand with DAHW
employee Renate Reichelt and Dami-
an-Versand manager Christina Sedl-
meier. Photo: Sabine Ludwig
Dr Chris Schmotzer visits the DAHW headquarters, bearing plenty of sto-ries. Photo: Sabine Ludwig
DAHW is present at the Düsseldorf
federal state parliament on the occasi-
on of the presentation of the cheque
for €28,000 from the Leprastiftung
NRW (leprosy foundation of North
Rhine-Westphalia).
Photo: Jochen Hövekenmeier
DAHW introduces itself to the Bava-rian federal state parliament in Mu-nich. Photo: Renate Reichelt
Dr Chris Schmotzer with her team in Rawalpindi. Photo: DAHW
Woman with her child in South Sudan. The state only gained independence in July 2011. Photo: DAHW
A patient is examined for tuberculo-
sis. Photo: DAHW
31 DAHW Lepra-Spezial 2005
April 2012As of April, Mervyn F. Lobo is the new man-ager of the Marie Adelaide Leprosy Centre (MALC), the organisation of Dr Ruth Pfau. Lobo has been working for the partner of DAHW for over 20 years: he recently man-aged emergency relief and reconstruction following the flood disaster.
May 201215,000 visitors attend the 3 7th Interna-tional Children’s Festival in Würzburg. Fol-lowing heavy showers, the sun comes out on the afternoon. The proceeds go to the Brazilian DAHW aid project, Educar.
June 2012More than 50 young East Frisians set off on the long road to Würzburg. 620km, over 10 hours on the coach – just to put on a show free of charge for a good cause. Directors Elke Warmuth and Isburga Dietrich wrote the play “SehnSucht” (yearning). It ex-plores the question of what various young people understand by “paradise”, wheth-er parents or teachers are any good as role models or whether the youngsters have to find their way on their own.
31 DAHW Annual Report 2012
Mervyn F. Lobo with Dr Ruth Pfau and DAHW president Gudrun Baroness von Wiedersperg in the MALC, Karachi. Photo: DAHW
Reconstruction following the flood
disaster in 2011 is co-ordinated under
the management of Mervyn F. Lobo.
Photo: DAHW
Women and children trust the doctors in the MALC. Photo: Ernst Hisch
DAHW representative Ahmed Moham-med reports on his work in Ethiopia. Photo: Enric Boixadós
A young patient in Ethiopia longs to
have her health back. Photo: Enric Boixadós
DAHW masters of the barbecue provi-
de a culinary treat. Photo: Sabine Ludwig
Alcohol and drugs are not the answer. Photo: Elke Warmuth
Children’s eyes and the sun vie for the biggest sparkle when the main prize for the competition is awarded. Photo: Michael Röhm
d t e way o t e ow .
SehnSucht nach dem Paradies
(Yearning for Paradise).
Photo: Elke Warmuth
It tastes twice as good made up! Pho-
to: Günther Klebinger
12
Focus on today’s young people. Photo: Michael Röhm
DAHW Lepra-Spezial 200532
DAHW CALENDAR OF EVENTS 2012
July 2012Motorbikes save lives in the DAHW project countries. The relief organisation points this out on the occasion of the motorbike pilgrimage to Kevelaer on the Lower Rhine. A DAHW team is also there.
September 2012Numerous visitors are present when DAHW celebrates its 55th annivers ary in Münster. Volunteers, full-time employees, the president of DAHW and members of the Board of Directors contribute towards a jolly time and stimulating conversations in the “Haus der Begegnung”.
August 2012DAHW brings Fatoumata Diawara to the stage of the Würzburger Hafensommer, the festival held around the Würzburg har-bour. She is a superstar in her home coun-try of Mali, and you can hear her mu sic wherever you go. Today, following a great deal of political turmoil, her songs are banned in large parts of her home country. The young singer is delighted to h ave found so many fans in Germany: however, they cannot replace the loss of her home-land.
Getting around is frequently impos-sible in the project countries during the rainy season. Photo: DAHW
Baroness Gudrun von Wiedersperg
visits DAHW projects in Pakistan.
Photo: Ernst Hisch
TB prevention is frequent amongst children and adolescents in India. Photo: Ursula Meissner
Prayer and reflection in the chapel of Kevelaer. Photo: Jochen Hövekenmeier
DAHW is represented with an infor-mation stand. Photo: Jochen Hövekenmeier
Singers of the Shanty choir of St.
Ambrosius Ostbevern get people in
the right mood. Photo: Franz Tönnes
The rain couldn’t spoil the motorised
pilgrimage. Photo: Jochen Hövekenmeier
Fatoumata Diawara radiates joie de
vivre at the Würzburger Hafensommer.
Photo: Jochen Hövekenmeier
Würzburg meets Münster. DAHW celebrates its 55th anniversary. Photo: Franz Tönnes
33 DAHW Lepra-Spezial 2005
October 2012DAWH representative Manfred Göbel glad-ly reports on how much the work of DAHW is appreciated in distant Amazonia. During the talk in Manaus, Dr Carlos Alberto Chi-rano Rodrigues, director of the local refer-ence centre for leprosy , hands over two commemorative plaques, expressing his thanks for the c o-operation and suppor t which have been g oing on for o ver 33 years.
November 2012The leprosy doctor and nun Dr Ruth Pfau is awarded the “B ambi” as a “s ilent hero-ine”. She is referred to as a “superstar by laudatory Johannes B. Kerner in this major TV gala. Walking to the st age, Ruth Pfau received standing ovations from the al-most exclusively celebrity audience which went on for several minutes.
December 2012Musician Carolina Eyck organises a charity concert in L eipzig to benefit the work of Ruth Pfau. Theremin, guitar and ba ss charm the audienc e in the Liebfr auen-kirche. Vinzenz Wieg on the guitar and Ja-kob Müller on the bass are also present. They present a very special musical even-ing which yielded a donation of €1,151 for DAHW.
33 DAHW Annual Report 2012
St Francis Hospital Nyenga celebrates
its 80th anniversary. Founded in 1932,
it has been a co-operation partner of
DAHW in Uganda since 1961, making it
the DAHW's first and oldest partner in
that country. Photo: Thomas Einberger
The children at the Sonderpädago-
gischen Förderzentrums Würzburg
(Special Needs School Würzburg
– SFZ) set up a bazaar in Würzburg’s
Sparkasse for their partner school in
Bisidimo. Photo: Michael Röhm
DAHW has been active in Brazil for over 33 years. DAHW representative Manfred Göbel is delighted with the two commemorative plaques. Photo: DAHW
The flea and car-boot sale by the Würzburg Campaign Group for the benefit of DAHW took in over €15,000. Photo: DAHW
Always on call: DAHW representative
Manfred Göbel in Brazil. Photo: Rolf Bauerdick
Dr Chris Schmotzer is a guest at the World Health Summit in Berlin. Photo: Jochen Hövekenmeier
A Bambi for Dr Ruth Pfau.
Photo: Hubert Burda Medien
Even the youngest benefit from the DAHW projects in Pakistan. Photo: Ernst Hisch
Charity concert: experiencing great live music and doing a good deed at the same time. Photo: privat
DAHW Annual Report 201234
Organization chart at August 2013
Organisational and staff development
Management Matthias Schröter
Maria Döhlen, Human Resources Management
David Gross, EDPGeorg Weißenberger, Procurement/
Property ManagementMichael Welter, Post Room
Public relations and fundraising
Head of Department Harald Meyer-Porzky
AssistenzSabine Slany
Press Offi ceJochen Hövekenmeier
Sabine Ludwig
Volunteers and School TeamTeam leadership Michael Röhm
Administration of foundations, wills and assetsNicole Hohmann
Peter Hofmann, Financial Director of DAHW (in compliance with the statutes)
Medical and social projects
Management Jürgen Ehrmann
Team Project SupportTeam leadership Birgit Markfelder
(Deputy Head of Department)Sandra Dreher, ControllingAnne Heinrich, East AfricaHeike Himmelsbach, Asia
Susanne Knoch, West Africa /Latin America
Team Project: Financial ResourcesTeam leadership Roland Müller
Laure Almairac
Team Program Development & Research
Team leadership Ernst Hisch, Disability and Rehabilitation
Dr. Joost Butenop, doctorChrista Kasang, research
Standards & Improvement Team Project
Team Management Martin HilgersChristine Porsch
Lea Thiel
Elke Herbst-TilgnerAssistant to the Chairman and Management
Harald Meyer-PorzkyDeputy Managing Director
The three highest annual salaries which are distributed among the Managing Director, the Director for Public Relations & Fundraising, the Deputy Managing Director and one other Head of Department (all of them employed full time) add up to a gross amount of EUR 235,210.38.All the 52 members of staff are paid according to the collective bargaining agreement for the Civil Service: Tariff group 5 (1 employee), TG 6 (11), TG 7 (2) TG 8 (3), TG 9 (9), TG 10 (19), TG 11 (2), TG 12 (1), TG 13 (1), TG 14 (2).12 members of staff work part-time, and 5 are semi-retired.The remuneration of the Managing Director is not subject to any collective bargaining agreement.The members of the Management Board work voluntarily. They do not receive any allowances; they only receive the actual travel expenses incurred if they apply for it.
Meeting of members (67 full members)
Honorary Chairman*Gudrun Freifrau von Wiedersperg (President)
Prof. Dr. med. August Stich (Vice President, medical advisor)Peter Hofmann (Financial Director),
Dr. Christof T. Potschka (Deputy Chairman)Dr. Reinhardt Mayer Monika HuesmannDr. Michael Rückert
Burkard KömmManaging Director
* As decided by vote on June 22, 2013, subject to final entry into the Registry of Associations.
Research
35 DAHW Annual Report 2012
DAHW Deutsche Lepra- und Tuberkulose-
hilfe e.V., is demanding investment in re-search into the transmission routes and vaccines for leprosy On World Leprosy Day Burkard Kömm, Director of the relief or-ganisation domiciled in Würzburg, points out that over 230,000 people contract lep-rosy every year although the di sease is classified as having been “eliminated”.
As the DAHW Director states the “elimina-tion” is merely a statistical variable used by the World Health Organisation, the limit being one patient per 10,000 inhabitants: “If there were 350 patients with leprosy in Berlin, the disease would be said to have been eliminated there, no matter what the citizens of Berlin have to say about it.”
Due to the st atistical definition, leprosy moves further away, escaping the atten-tion of health politics. One consequence of this according to Kömm is that there are now virtually no more funds, even if – for example like after the w ars in Liberia or South Sudan – a c ompletely new leprosy programme must be set up.
More new cases of leprosy again
The number of new cases has risen slight-ly, probably to a little o ver 230,000. In 2011 96 c ountries reported a tot al of 219,075 patients to the WHO (2010: 228,474 patients from 11 7 countries)- Among the countries which have not yet reported any figures for 2011 are Ethiopia, Nigeria and Tanzania; in 20 10 they ac-counted for almost 11,000 new cases.
“Leprosy is considered unprogressive and therefore hardly any governments want to have anything to do with it,” is the conclu-
sion drawn by DAHW director Kömm. But this could be changed if there were incen-tives to do so: “If wealthy countries like Germany begin to invest in leprosy re-search or the implement ation of pro-grammes and projects, this disease would no longer have to be hidden away.”
This is also a c onsequence of the stigma that typically surrounds leprosy. Besides structural disadvantages, Kömm also fo-cuses especially on the respon sibility to not abandon the people affected. “People with leprosy are still being ostracised and have hardly any chance of taking part in society. This is the huge mission facing us at DAHW today.”
The “outrageous” suffe-ring caused by leprosyDAHW demands investment in research and development
DAHW will set a good example and itself invest over EUR 150,000 in leprosy re-search. Together with funds from partner organisations in the USA, the Netherlands and Canada, in future leprosy research will have almost EUR 500,000 at its disposal each year.
In 2011 over 260,000 people affected b y leprosy found help in the D AHW projects. This included m any former patients who have to live with disabilities which are the long-term effects of leprosy, as well as 40,000 who have contracted it at present; that is almost 20 % of all patients regis-tered worldwide.
“Investments in research are becoming increasingly urgent,” DAHW Director Burkard Kömm states.
Phot
o: E
nric
Boi
xadó
s
www.dahw.de
go to 55,000 people in Germany who donated money for our workto the 2,000 people who are committed volunteers working for the sake of our relief organisation and who have collected numerous donations
to the parishes and schools which have supported our work from collections and campaigns
to the companies, foundations and institutions which have supported and sponsored our work
to state authorities and governments which have supported our work by means of financial donations and fast, straightforward help
to public prosecutors and courts of law who have given consideration to our relief organisation by allocating fines to it
as well as
to those people who, during their lifetime included our relief organisation in their wills and have bequeathed us
on behalf of almost 700,000 patients in 223 relief projects in 23 countries and on behalf of over 200,000 people whom we have actively supported following the catastrophic flooding in Pakistan and whom we can now help reconstruct their homelands.