Clinician Research Summary Functional Limitations and Physic al Disabilities Surgical Options for Inguinal Hernia Surgical Management of Inguinal Hernia Background Surgical repair oinguinal hernias is the most commonly perormed general surgical procedure in the United States. Such a large volume oprocedures suggests that even modest improvem ents in patient outcomes would substantially improve population health. Te primary goals osurgery include preventing strangulation, repairing the hernia, minimizing the chance orecurrence, returning the patient to normal activities quickly , improving quality olie, and minimizing postsurgical discomort and the adverse effects osurgery. Recurrence occurs in approximately 1 to 5 percent ocases oinguinal hernia. Surgical procedures or inguinal hernia repair generally all into three categories: open repair without a mesh implant (i.e., sutured), open repair with a mesh, and laparoscopic repair with a mesh. Te near-universal adoption omesh means that the most relevant questions about hernia repair involve various mesh procedures. How ever , mesh is not recommended or repair opediatric inguinal hernia or several reasons including concerns about inflammatory reactions, damage to the vas deerens and/or testes, inertility, and growth-related complications. Te findings rom the research review presented here may inorm clinical decisions by patients and surgeons, treatmen t recommendation s by proessional societies, purchasing decisions by hospitals, and coverage decisions by third-party payers. Conclusions Te typical adult in the studies included in this review was a man in his mid 50s, who is of average weight (median body mass index 25.3 kg/m 2 ; interquartile range 25.0–26.7), and who had an elective repair of a primary unilateral inguinal hernia. About a quarter of the men worked in physically strenuous jobs; for these men, a durable repair is important to prevent a recurrence. Te results of the review may inform decisions these men face. It is unclear how these results apply to women. However, it is also unclear how these results apply to men of other age groups. Results indicate that laparoscopic repair oan inguinal hernia is associated with aster recovery times and less risk olong- term (≥6 months) pain; or recurrent hernia, such repair may also lower the risk oanother hernia recurrence. Open hernia repair, however, is amiliar to more surgeons. Such repair may be associated with ewer internal injuries and may have lower recurrence rates in the context oa primary inguinal hernia. Limited evidence suggests that choosing to repair a pain-ree or minimally symptoma tic inguinal hernia with a Lichtenstein or tension-ree mesh repair over watchul waiting may improve quality olie; however, this may not be applicable to other types orepair procedures, and the evidence on adverse effects is inconclusive. Research ound most othe meshes or fixation methods to be equivalent in their effectiveness and risk oadverse effects with only a ew exceptions. Tere are numerous reports that the risk orecurrence decreases when a more experienced surgeon perorms a repair, but there are not enough congruent studies to perorm a meta-analysis. Research Focus for Clinicians A systematic review o151 clini cal studies published be tween January 1990 and November 2011 sought to determine the comparative effectiveness and adverse effects odifferent surgical options or inguinal hernia in a dults and children. Tere were 123 randomized controlled trials (RCs), 2 registries, and 26 studies wit h other designs. Tis summary, based on the ull report oresearch evidence, is provided to inorm discussions ooptions with patients and to assist in decisionmaking along with consideration oa patient’ s values and preerences. How ever, reviews oevide nce should not be construed to represent clinical recommendations or guidelines. Te HML version othis clinician research summary provides links to the ull report or a more detailed discussion othe studies included in each analysis. Te ull report and the HML version othis clinician research summary are available at www.effectivehealthcare.ahrq.gov/in guinal-hernia.cm. Clinical Bottom Line Comparative Effectiveness of Interventions for Primary, Bilateral, or Recurrent Hernias Pain-Free Primary Hernia Ia patient has a pain-ree or minimally symptomatic primary hernia that is not interering with normal activities, a mesh repair may improve their overall health status at 12 months versus those on watchul waiting (difference in mean SF-36 scores = 7.3; 95% CI, 0.4 to 14.3). (Continued on next page) Strength of Evidence Scale High: High confidence that the evidence reflects the true effect. Further research is very unlikely to change our confidence in the estimate oeffect. Moderate: Moderate confidence that the evidence reflects the true effect. Further research may change our confidence in the estimate oeffect and may change the estimate. Low: Low confidence that the evidence reflects the true effect. Further research is likely to change our confidence in the estimate oeffect and is likely to change the estimate. Insufficient: Evidence is ei ther unavailable or does not permit a conclusion.
BackgroundSurgical repair o inguinal hernias is the most commonlyperormed general surgical procedure in the United States.Such a large volume o procedures suggests that even modestimprovements in patient outcomes would substantially improvepopulation health. Te primary goals o surgery include
preventing strangulation, repairing the hernia, minimizing thechance o recurrence, returning the patient to normal activitiesquickly, improving quality o lie, and minimizing postsurgicaldiscomort and the adverse effects o surgery. Recurrence occursin approximately 1 to 5 percent o cases o inguinal hernia.
Surgical procedures or inguinal hernia repair generally allinto three categories: open repair without a mesh implant (i.e.,sutured), open repair with a mesh, and laparoscopic repair with amesh. Te near-universal adoption o mesh means that the mostrelevant questions about hernia repair involve various meshprocedures. However, mesh is not recommended or repair opediatric inguinal hernia or several reasons including concernsabout inflammatory reactions, damage to the vas deerensand/or testes, inertility, and growth-related complications.Te findings rom the research review presented here mayinorm clinical decisions by patients and surgeons, treatmentrecommendations by proessional societies, purchasing decisionsby hospitals, and coverage decisions by third-party payers.
ConclusionsTe typical adult in the studies included in this review was a manin his mid 50s, who is of average weight (median body massindex 25.3 kg/m2; interquartile range 25.0–26.7), and who hadan elective repair of a primary unilateral inguinal hernia. Abouta quarter of the men worked in physically strenuous jobs; forthese men, a durable repair is important to prevent a recurrence.
Te results of the review may inform decisions these men face. Itis unclear how these results apply to women. However, it is alsounclear how these results apply to men of other age groups.
Results indicate that laparoscopic repair o an inguinal herniais associated with aster recovery times and less risk o long-term (≥6 months) pain; or recurrent hernia, such repair
may also lower the risk o another hernia recurrence. Openhernia repair, however, is amiliar to more surgeons. Suchrepair may be associated with ewer internal injuries andmay have lower recurrence rates in the context o a primaryinguinal hernia. Limited evidence suggests that choosing to
repair a pain-ree or minimally symptomatic inguinal herniawith a Lichtenstein or tension-ree mesh repair over watchulwaiting may improve quality o lie; however, this may notbe applicable to other types o repair procedures, and theevidence on adverse effects is inconclusive.
Research ound most o the meshes or fixation methods tobe equivalent in their effectiveness and risk o adverse effectswith only a ew exceptions. Tere are numerous reports thatthe risk o recurrence decreases when a more experiencedsurgeon perorms a repair, but there are not enoughcongruent studies to perorm a meta-analysis.
Research Focus for CliniciansA systematic review o 151 clinical studies published between January 1990 and November 2011 sought to determine the
comparative effectiveness and adverse effects o different surgical options or inguinal hernia in adults and children. Terewere 123 randomized controlled trials (RCs), 2 registries, and 26 studies with other designs. Tis summary, based on theull report o research evidence, is provided to inorm discussions o options with patients and to assist in decisionmakingalong with consideration o a patient’s values and preerences. However, reviews o evidence should not be construed torepresent clinical recommendations or guidelines. Te HML version o this clinician research summary provides links tothe ull report or a more detailed discussion o the studies included in each analysis. Te ull report and the HML versiono this clinician research summary are available at www.effectivehealthcare.ahrq.gov/inguinal-hernia.cm.
Clinical Bottom LineComparative Effectiveness of Interventions forPrimary, Bilateral, or Recurrent Hernias
Pain-Free Primary Hernia
I a patient has a pain-ree or minimally symptomaticprimary hernia that is not interering with normal activities,a mesh repair may improve their overall health status at12 months versus those on watchul waiting (difference inmean SF-36 scores = 7.3; 95% CI, 0.4 to 14.3).
(Continued on next page)
Strength of Evidence Scale High: High confidence that the evidence reflects the trueeffect. Further research is very unlikely to changeour confidence in the estimate o effect.
Moderate: Moderate confidence that the evidence reflectsthe true effect. Further research may change ourconfidence in the estimate o effect and may changethe estimate.
Low: Low confidence that the evidence reflects the trueeffect. Further research is likely to change ourconfidence in the estimate o effect and is likely tochange the estimate.
Insufficient: Evidence is either unavailable or does not permita conclusion.
Comparative Effectiveness of Surgical Interventionsfor Primary, Bilateral, or Recurrent Hernias (Continued)
Recurrent Hernia
Several outcomes avor laparoscopic (APP or EP)repair over open (Lichtenstein or Stoppa) repair: Return to normal daily activities about 7 days earlier Less likelihood o experiencing long-term pain (odds
ratio = 0.24; 95% CI, 0.08 to 0.74) In repair o recurrent hernias, lower re-recurrence
rates (7.5% or laparoscopic repair vs. 12.3% oropen repair)
Evidence is inconclusive or all other outcomes andcomparative adverse effects o laparoscopic versus openrepair o recurrent hernias including epigastric vessel injury,hematoma, urinary retention, and wound inection.
Pediatric Hernia (Ages 3 Months to 15 Years)
Laparoscopic and open high ligation repair o pediatrichernias both have similar outcomes or return to dailyactivities.
For laparoscopic versus open high ligation repair opediatric hernias, laparoscopic repair is avored or: Length o hospital stay Long-term patient/parent satisaction Long-term cosmesis
Data on adverse effects are not reported.
95% CI = 95-percent confidence interval; SF-36 = 36-Item ShortForm Health Survey; APP = transabdominal preperitoneal;EP = totally extraperitoneal
Comparative Effectiveness of Open Mesh-BasedRepair Procedures
Different open repair procedures yielded similar results,except that Lichtenstein repair may allow a 4-day earlierreturn to work when compared with a mesh plug. Lichtenstein repair is associated with lower rates oseroma than repair with a mesh plug.
Comparative Effectiveness of Laparoscopic Mesh-Based Repair Procedures
Rates o short-term pain (), intermediate-term pain
(), and long-term pain () are equivalent orboth the APP and EP repairs. APP repair may offer a 1.4-day earlier return to work;however, this difference may not be clinically significant. Research on comparative adverse effects between APPand EP repairs is inconclusive or hematoma, urinaryretention, and wound inection.
Comparative Effectiveness of Surgical Materialsand Fixation Methods
Mesh Material
Hernia recurrence occurs at similar rates with polypropylenemesh versus combination materials.* Long-term pain afer surgery is similar or standardpolypropylene mesh when compared with biologic meshor light-weight polypropylene mesh. Evidence on comparative adverse effects or the differenttypes o mesh materials is inconclusive.
Fixation Methods
Afer laparoscopic surgery, recurrence rates are similaror tacks or staples versus no fixation. Mesh fixations with sutures or with glue during openor laparoscopic surgery are associated with similarrecurrence rates () and long-term pain outcomes() or both procedures. Mesh fixation with fibrin glue during APP repairresults in less long-term pain than when the mesh isfixed with staples. Data on adverse effects are either missing or inconclusive.
* Descriptions o the combination material mesh analyzed or thisoutcome can be ound in the ull report.
Clinical Bottom Line (Continued)
Surgical Bottom Line
Comparative Effectiveness of Surgical Interventionsfor Primary, Bilateral, or Recurrent Hernias (Continued)
Pain-Free Primary Hernia (Continued)
Tere is not enough inormation to know i there aredifferences in long-term pain at rest or during movement,long-term pain that intereres with activities, or acutehernia/strangulation or patients with a pain-ree or
minimally symptomatic hernia who have a mesh repair versus those on watchul waiting.
Painful Primary Hernia
Laparoscopic repair results in a aster return to normalactivities and work when compared with open repair. Laparoscopic repair results in less long-term pain thanopen repair. Open repair may have a lower rate o recurrence thanlaparoscopic repair. Te length o hospital stay is similar or both types osurgery. Laparoscopic repairs have lower rates o hematoma() and wound inection () than open repairs. Open repairs have lower rates o epigastric vessel injuriesthan laparoscopic repairs.
Bilateral Hernia
Patients with bilateral hernias return to work about 2 weekssooner afer laparoscopic (APP or EP) repair versus open(Lichtenstein or Stoppa) repair. Evidence is inconclusive on the comparative adverse effectsor laparoscopic versus open repair o bilateral hernias.
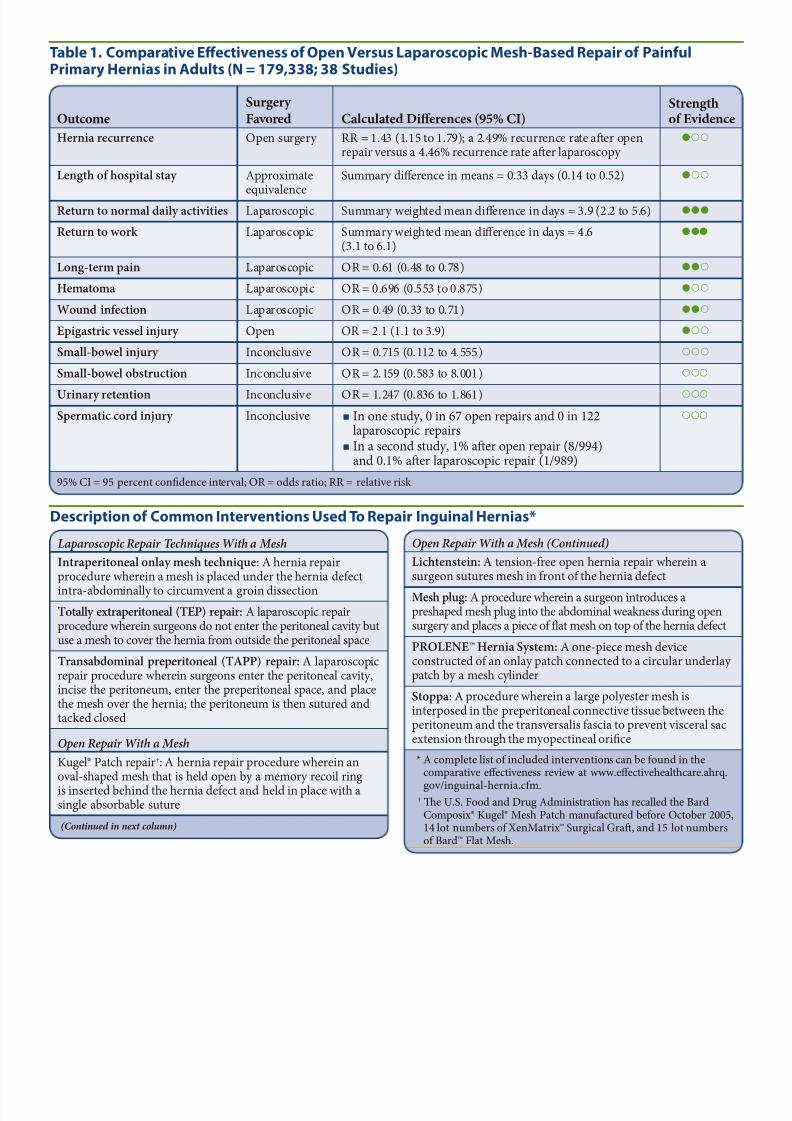
Hernia recurrence Open surgery RR = 1.43 (1.15 to 1.79); a 2.49% recurrence rate afer openrepair versus a 4.46% recurrence rate afer laparoscopy
Length of hospital stay Approximate
equivalence
Summary difference in means = 0.33 days (0.14 to 0.52)
Return to normal daily activities Laparoscopic Summary weighted mean difference in days = 3.9 (2.2 to 5.6)
Return to work Laparoscopic Summary weighted mean difference in days = 4.6(3.1 to 6.1)
Long-term pain Laparoscopic OR = 0.61 (0.48 to 0.78)
Hematoma Laparoscopic OR = 0.696 (0.553 to 0.875)
Wound infection Laparoscopic OR = 0.49 (0.33 to 0.71)
Epigastric vessel injury Open OR = 2.1 (1.1 to 3.9)
Small-bowel injury Inconclusive OR = 0.715 (0.112 to 4.555)
Small-bowel obstruction Inconclusive OR = 2.159 (0.583 to 8.001)
Urinary retention Inconclusive OR = 1.247 (0.836 to 1.861)
Spermatic cord injury Inconclusive In one study, 0 in 67 open repairs and 0 in 122laparoscopic repairs
In a second study, 1% afer open repair (8/994)and 0.1% afer laparoscopic repair (1/989)
95% CI = 95 percent confidence interval; OR = odds ratio; RR = relative risk
Table 1. Comparative Effectiveness of Open Versus Laparoscopic Mesh-Based Repair of PainfulPrimary Hernias in Adults (N = 179,338; 38 Studies)
Open Repair With a Mesh (Continued)
Lichtenstein: A tension-ree open hernia repair wherein asurgeon sutures mesh in ront o the hernia deect
Mesh plug: A procedure wherein a surgeon introduces apreshaped mesh plug into the abdominal weakness during opensurgery and places a piece o flat mesh on top o the hernia deect
PROLENE™ Hernia System: A one-piece mesh deviceconstructed o an onlay patch connected to a circular underlaypatch by a mesh cylinder
Stoppa: A procedure wherein a large polyester mesh isinterposed in the preperitoneal connective tissue between theperitoneum and the transversalis ascia to prevent visceral sacextension through the myopectineal orifice
* A complete list o included interventions can be ound in thecomparative effectiveness review at www.effectivehealthcare.ahrq.
gov/inguinal-hernia.cm. † Te U.S. Food and Drug Administration has recalled the Bard
Composix® Kugel® Mesh Patch manuactured beore October 2005,14 lot numbers o XenMatrix™ Surgical Graf, and 15 lot numberso Bard™ Flat Mesh.
Laparoscopic Repair Techniques With a Mesh
Intraperitoneal onlay mesh technique: A hernia repairprocedure wherein a mesh is placed under the hernia deect
intra-abdominally to circumvent a groin dissection
Totally extraperitoneal (TEP) repair: A laparoscopic repairprocedure wherein surgeons do not enter the peritoneal cavity butuse a mesh to cover the hernia rom outside the peritoneal space
Transabdominal preperitoneal (TAPP) repair: A laparoscopicrepair procedure wherein surgeons enter the peritoneal cavity,incise the peritoneum, enter the preperitoneal space, and placethe mesh over the hernia; the peritoneum is then sutured andtacked closed
Open Repair With a Mesh
Kugel® Patch repair†: A hernia repair procedure wherein anoval-shaped mesh that is held open by a memory recoil ringis inserted behind the hernia deect and held in place with asingle absorbable suture
Surgery for an Inguinal Hernia, A Review of the Research for Adults is a ree companion to this clinician researchsummary. It can help patients talk with their health care
proessionals about the decisionsinvolved with the care and maintenanceo an inguinal hernia. It providesinormation about:
ypes o operative treatments Current evidence o effectivenessand harms
Questions or patients to asktheir health care proessionals
Ordering Information
For electronic copies o Surgery for an Inguinal Hernia, AReview of the Research for Adults, this clinician researchsummary, and the ull systematic review, visit www.effectivehealthcare.ahrq.gov/inguinal-hernia.cm. o orderree print copies, call the AHRQ Publications Clearinghouseat 800-358-9295.
Source
Te inormation in this summary is based on SurgicalOptions for Inguinal Hernia: Comparative EffectivenessReview, Comparative Effectiveness Review No. 70, preparedby the ECRI Institute Evidence-based Practice Center underContract No. HHSA 290-2007-10063 or the Agency orHealthcare Research and Quality, August 2012. Availableat www.effectivehealthcare.ahrq.gov/inguinal-hernia.cm.Tis summary was prepared by the John M. EisenbergCenter or Clinical Decisions and Communications
Science at Baylor College o Medicine, Houston, X.
Gaps in Knowledge
How the surgeon’s experience influences surgicaloutcomes such as recurrence and pain
Te comparative effectiveness and adverse effects olaparoscopic repair versus watchul waiting or minimallysymptomatic hernias in adults
Te comparative effectiveness and adverse effects ocontralateral exploration/repair versus watchul waitingin the pediatric population
More evidence on several outcomes related to thecomparisons o mesh products and fixation methodsincluding recurrence rates, perception o a oreign body,long-term pain, and inection rates
Clarification in uture studies o whether the populationincludes emergent as well as elective surgeries and whetheror not the findings apply equally to both populations
What To Discuss With Your Patients
I repair or watchul waiting is the right decision or theirpain-ree or minimally symptomatic inguinal hernia
How to choose between open or laparoscopic surgery ithe option is available
What to expect rom open or laparoscopic repair as aras outcomes and adverse effects, including the risk olong-term chronic pain