29
Insulin Pump What to tell your patient!! Prakash Abraham Isla Fairley
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| Upload: | sharon-gray |
| View: | 218 times |
| Download: | 0 times |

Insulin Pump What to tell your patient!!
Prakash Abraham
Isla Fairley


•

Present generation pumps
•Paradigm (Medtronic £2750)
•Animas (Johnson & Johnson, £2600)
•Spirit (Roche, £2375)
•Deltec Cozmo (Smiths Medical, £2750)

Insulin Pump Usage: Grampian ~2% vs UK 4%

What does the pump do?

2008 NICE recommendations
• Disabling hypoglycaemia (repeated and unpredictable occurrence of hypos that result in persistent anxiety about recurrence and adverse quality of life)
• HBA1c > 8.5% despite high level of care
• Children <12 (where MDI impractical) and should have a trial of MDI between 12-18years.

Who can consider the pump 1
Patient characteristics
• Type 1 DM
• Basal bolus regime
• Well motivated
• Cope with CHO counting (DAFNE)
• Monitoring at least 4 times
• No evidence of Psychological illness

Who can consider the pump 2
Disease characteristics
• Frequent hypoglycaemia
• Hypoglycaemia unawareness
• Gastroparesis
• Poor control
• Marked dawn phenomenon

New Aspects to consider for pump
• Carbohydrate Ratios – DAFNE (Dose adjustment for normal eating)
• Insulin Sensitivity / Correction doses– DAFNE
• Basal Rates (Additional to DAFNE)– 1 basal injection to potentially 48 choices– Fasting at different times to titrate

Carbohydrate/ Insulin Ratio
• number of grams CHO covered by 1 unit insulin
• The 500 Rule: 500 divided by total daily dose equals CHO ratio.
• Usually 10-15
• May vary at different times of the day.


4
8
12
16

Insulin sensitivity
• how much 1 unit of insulin lowers bg over 2-4 hours
• Correction dose
• The 100 rule: 100 / total daily insulin dose
• May vary at different times of the day


8
4
12
16

An overnight drop of upto 2mmol/l is OK
5
10
15

What does the pump involve?
• Insulin set changes every 2-3 days
• Correction doses– Insulin sensitivity to be checked at different
times
• Carbohydrate ratios– Monitor Meal Bolus rates for each of the
meals

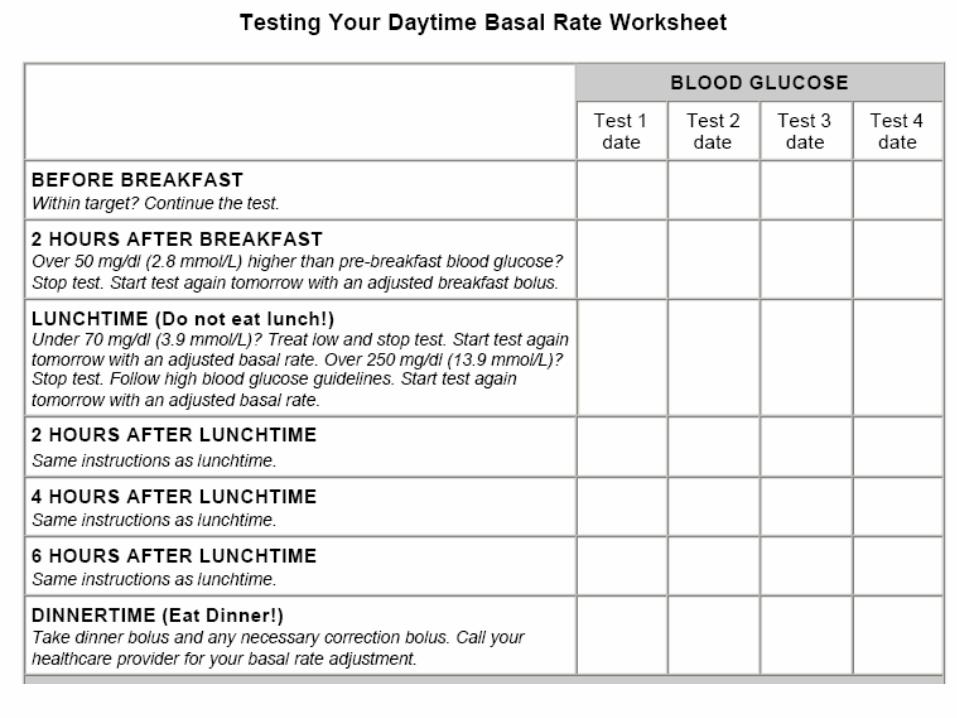
What does the pump involve?
• Basal rates to be checked– Skip breakfast for overnight rate– Skip lunch for daytime rate– Skip dinner for evening rate
• Takes 3-6 months of work to get the various rates and ratios sorted.
• Then work out weekends, more active days etc

Assessment
• Interview with DSN/Doctor/Dietitian
• Confirm eligibility and motivation
• CHO counting (DAFNE course)
• Pump demonstration
• Dummy pump (CGMS) to carry for 2 days
• Pump panel for funding decision
Pump Start
• First week: Intensive (Days off Work)
• Patient Contract
• QOL (PAID) / Hypo questionnaires
• First 3 months: 3 to 6 visits to Diabetes Resource Room, then at 6 & 12 months
• Pump clinic: 4.5 /9 /15 months then ~4 monthly
• (CGMS)

Patient contract
Initial Pump Support Variations
• Two of the new starts in 2007• MT
– 4 months: Phone calls 2 weekly– emails 2 weekly– 9 appointments (3 with Doctor)
• GN– 6 month: 3 phone calls– 3 emails– 3 appointments (2 with doctor)

Disadvantages• Wearing a device
• Essential to check BMs minimum 4 times a day. Risk of DKA as only short acting insulin
• Work involved in assessing rates and ratios.

Advantages
• Minimise Hypoglycaemia
• Less variability in blood sugars
• More precise insulin dosing
• Flexibility to change basal rates depending on activity
• Quality of Life

Summary of profiles over 3 days

CSII NOT for everyone

Effort vs Reward

















