In a 2001 article in this journal,1 we described howconsiderable improvement can be achieved in
patients with missing lateral incisors by combin-ing carefully detailed orthodontic space closure withtechniques from esthetic dentistry. Such methodsmay include:• Individualized extrusion and intrusion duringmesial movement of the canine and first premolar,respectively, to obtain an optimum level for themarginal gingival contours of the anterior teeth.• Careful correction of the crown torque of amesially relocated canine to mirror the optimalcrown torque of a lateral incisor, along with theprovision of optimal torque for the mesially relo-cated maxillary first and second premolars.• Esthetic recontouring of a mesially relocatedcanine to a more ideal lateral incisor shape andsize with a combination of grinding and compos-ite resin build-ups or porcelain veneers.
• Increasing the width and length of mesializedand intruded first premolars with composite resinbuild-ups and/or porcelain veneers to achieveoptimal esthetics and functional occlusion.• Intentional vital bleaching of a yellowishcanine that has been moved mesially into the lat-eral incisor position.• Simple minor surgical procedures for localizedclinical crown lengthening.
Common Esthetic Problems withOrthodontic Space Closure
The most obvious difficulty in substitutingcanines for missing maxillary lateral incisors is theachievement of an excellent esthetic and func-tional outcome that resembles an intact naturaldentition.1-4 Particularly in unilateral agenesiscases, space closure can create problems in match-ing tooth size, shape, and color.4 The canine is nor-mally a longer and larger tooth, mesiodistally andlabiolingually, than the lateral incisor it is to replace,and more saturated with color. The first premolaris generally shorter and narrower than the con-tralateral canine. If these natural size differences arenot compensated for, the esthetic outcome will becompromised,1-3 and, as is commonly seen in ortho-dontic treatment, the premolars substituting forthe canines will be too diminutive.5-9
This article describes the advantages not onlyof increasing first premolar length and width, butalso of evaluating and restoring the maxillary cen-tral incisors to create optimal dental exposure dur-ing function. In addition, it presents importantnew information on indications and contraindica-tions for the space-closure alternative.
Integrating Space Closure andEsthetic Dentistry in Patients withMissing Maxillary Lateral IncisorsFurther ImprovementsMARCO ROSA, MD, DDS, DOBJÖRN U. ZACHRISSON, DDS, MSD, PHD
Dr. Rosa is a Professor of Orthodontics, Insubria University, Varese,Italy, and in the private practice of orthodontics in Trento, Italy. Dr.Zachrisson is an Associate Editor of the Journal of Clinical Ortho-dontics and Professor of Orthodontics at the University of Oslo,Norway. He is in the private practice of orthodontics at Stortingsgt. 10,0161 Oslo, Norway; e-mail: [email protected].
Dr. Rosa Dr. Zachrisson
factory and stable results over many years of sub-stituting canines for missing lateral incisors (Fig. 1),in some patients the outcome was a dentition thatdid not appear entirely natural; in other patients thecomposite resin build-ups needed more mainte-nance than expected. From our recently treatedmaxillary lateral incisor agenesis cases, we haveselected the following two difficult and challeng-ing patients to demonstrate further improvementsin the technique and provide some clinical guide-lines.
Case 1
A 12-year-old female presented in the latemixed dentition with a Class III malocclusion, ahypodivergent growth pattern, a narrow maxilla,and pronounced spacing in the maxillary arch,including spaces from bilaterally missing lateralincisors (Fig. 2). The mandibular arch was normallyshaped with no crowding.
Traditionally, a Class III malocclusion in apatient with missing lateral incisors, a narrow max-illa, and severe spacing has been corrected with
space reopening and replacement of the absent lat-eral incisors with single implants or other restora-tions. Because of the excellent motivation andcooperation shown by this patient, however, it wasdecided to attempt closure of all spaces in the max-illary arch. The treatment plan involved rapid max-illary expansion (RME); improvement of the facialconvexity by molar extrusion, which would increasefacial height and induce clockwise rotation of theocclusal and mandibular planes; extrusion of themaxillary anterior teeth for better exposure duringspeech and smiling; and finishing of the occlusionwith the first molars in a Class II relationship,canines substituting for the missing lateral incisors,and first premolars replacing the canines.
The RME was followed by bonding of fixedappliances in both dental arches, including thelower second molars (Fig. 3), and space closurewith Class III elastics. As recommended in our pre-vious article,1 the marginal gingival contours wereleveled by combining extrusion of the maxillarycanines with lingual root torque and intrusion of thefirst premolars with labial root torque.
At the end of the orthodontic phase, the
564 JCO/SEPTEMBER 2007
Integrating Space Closure and Esthetic Dentistry
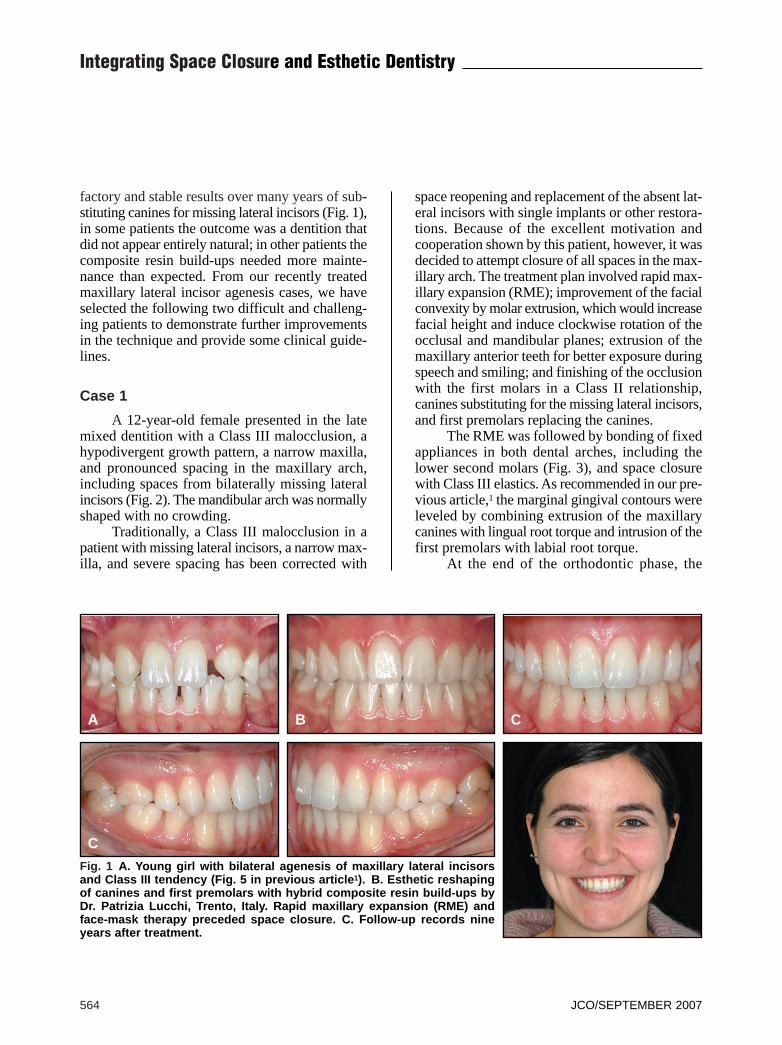
Fig. 1 A. Young girl with bilateral agenesis of maxillary lateral incisorsand Class III tendency (Fig. 5 in previous article1). B. Esthetic reshapingof canines and first premolars with hybrid composite resin build-ups byDr. Patrizia Lucchi, Trento, Italy. Rapid maxillary expansion (RME) andface-mask therapy preceded space closure. C. Follow-up records nineyears after treatment.
A B C
C
VOLUME XLI NUMBER 9 565
Rosa and Zachrisson
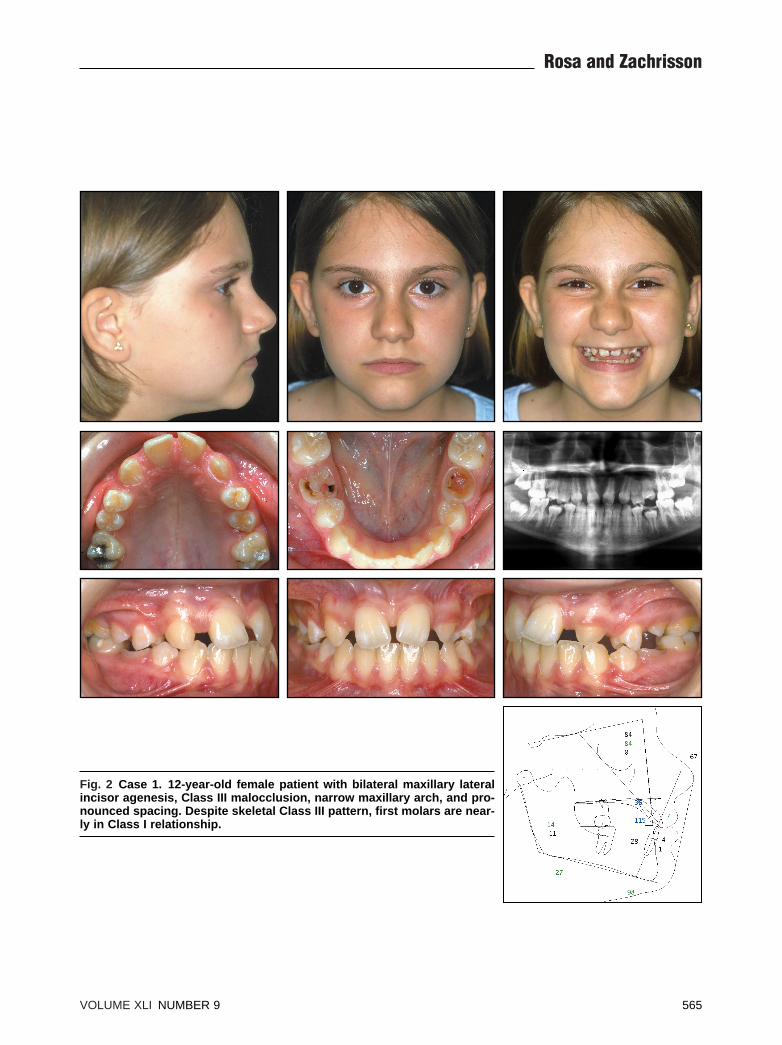
Fig. 2 Case 1. 12-year-old female patient with bilateral maxillary lateralincisor agenesis, Class III malocclusion, narrow maxillary arch, and pro-nounced spacing. Despite skeletal Class III pattern, first molars are near-ly in Class I relationship.
spaces were fully closed, and a functional occlu-sion with a Class II molar relationship had beenachieved (Fig. 4). After the canine and first pre-molar substitutions, the gingival contours showeda natural high-low-high pattern. Exposure of the sixmaxillary anterior teeth with relaxed lips and insmiling had improved due to the incisor extrusionand clockwise rotation of the occlusal plane andmandible, but their exposure with the lips at restwas still inadequate.10-12
Cosmetic finishing was begun on the day ofdebonding by Dr. Patrizia Lucchi of Trento, Italy(Fig. 5). This involved grinding of the caninesand hybrid composite resin build-ups of both thecanines and the first premolars. The canine cusp tipswere ground only slightly because of their insuf-ficient exposure with the lips at rest. To establishharmony in the anterior segment, it was necessaryto elongate these teeth, which were too square.What made the smile appear natural in the end was
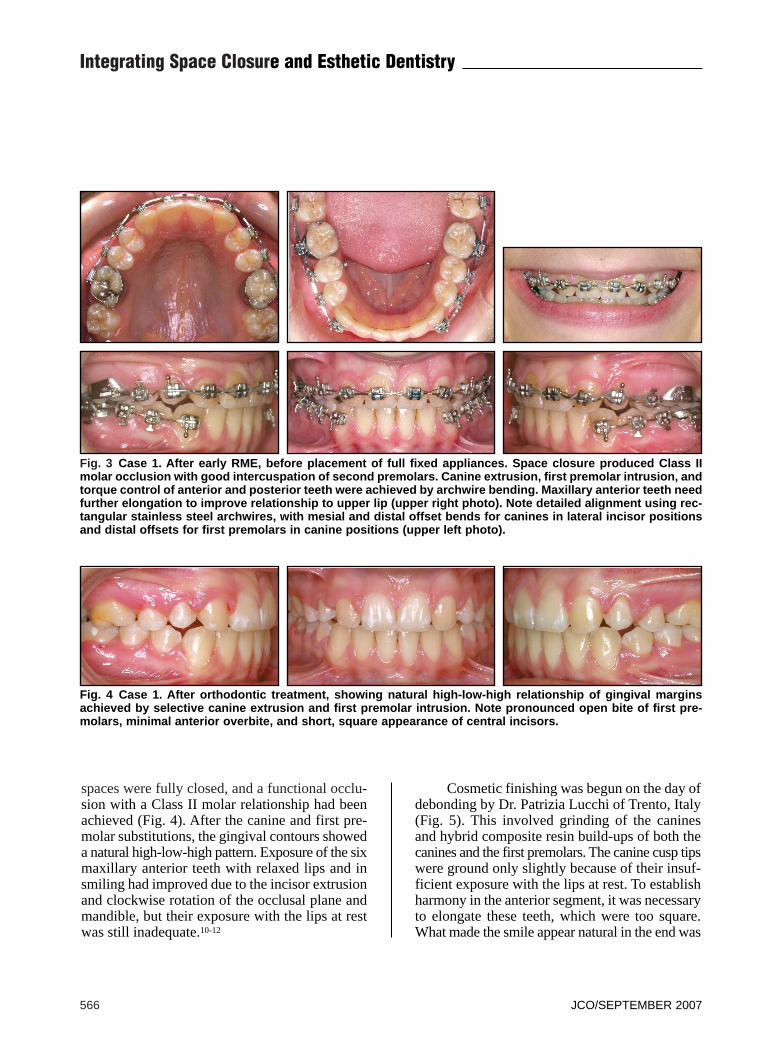
Fig. 3 Case 1. After early RME, before placement of full fixed appliances. Space closure produced Class IImolar occlusion with good intercuspation of second premolars. Canine extrusion, first premolar intrusion, andtorque control of anterior and posterior teeth were achieved by archwire bending. Maxillary anterior teeth needfurther elongation to improve relationship to upper lip (upper right photo). Note detailed alignment using rec-tangular stainless steel archwires, with mesial and distal offset bends for canines in lateral incisor positionsand distal offsets for first premolars in canine positions (upper left photo).
Fig. 4 Case 1. After orthodontic treatment, showing natural high-low-high relationship of gingival marginsachieved by selective canine extrusion and first premolar intrusion. Note pronounced open bite of first pre-molars, minimal anterior overbite, and short, square appearance of central incisors.
566 JCO/SEPTEMBER 2007
Integrating Space Closure and Esthetic Dentistry
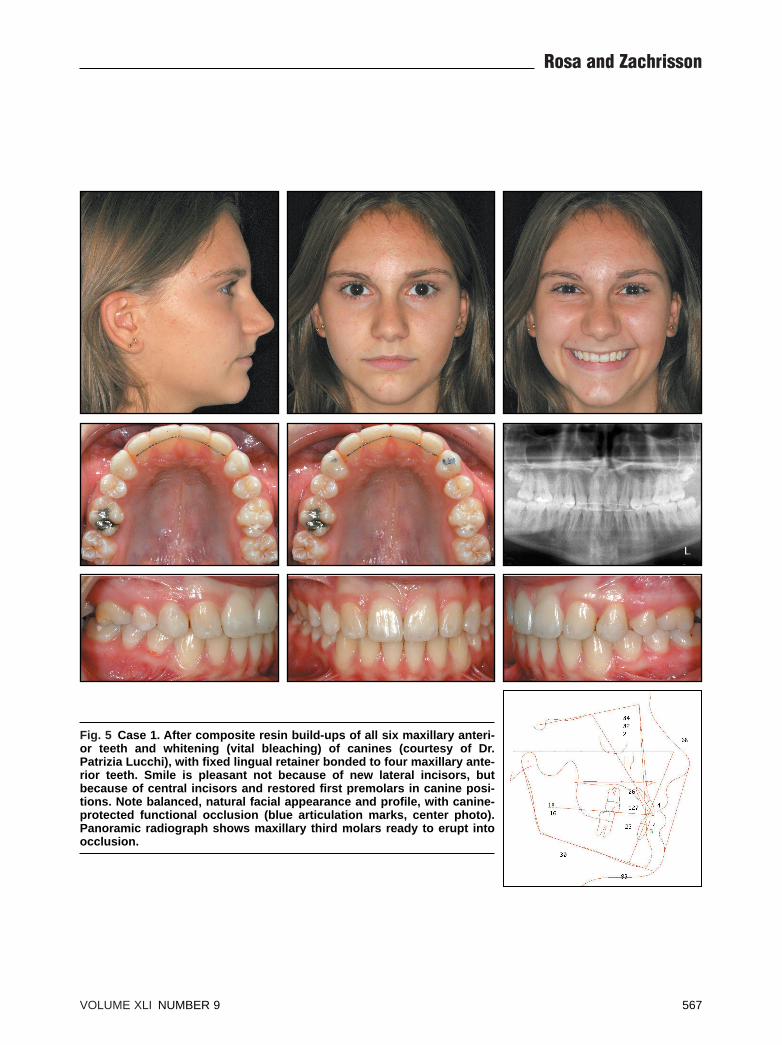
Fig. 5 Case 1. After composite resin build-ups of all six maxillary anteri-or teeth and whitening (vital bleaching) of canines (courtesy of Dr.Patrizia Lucchi), with fixed lingual retainer bonded to four maxillary ante-rior teeth. Smile is pleasant not because of new lateral incisors, butbecause of central incisors and restored first premolars in canine posi-tions. Note balanced, natural facial appearance and profile, with canine-protected functional occlusion (blue articulation marks, center photo).Panoramic radiograph shows maxillary third molars ready to erupt intoocclusion.
VOLUME XLI NUMBER 9 567
Rosa and Zachrisson
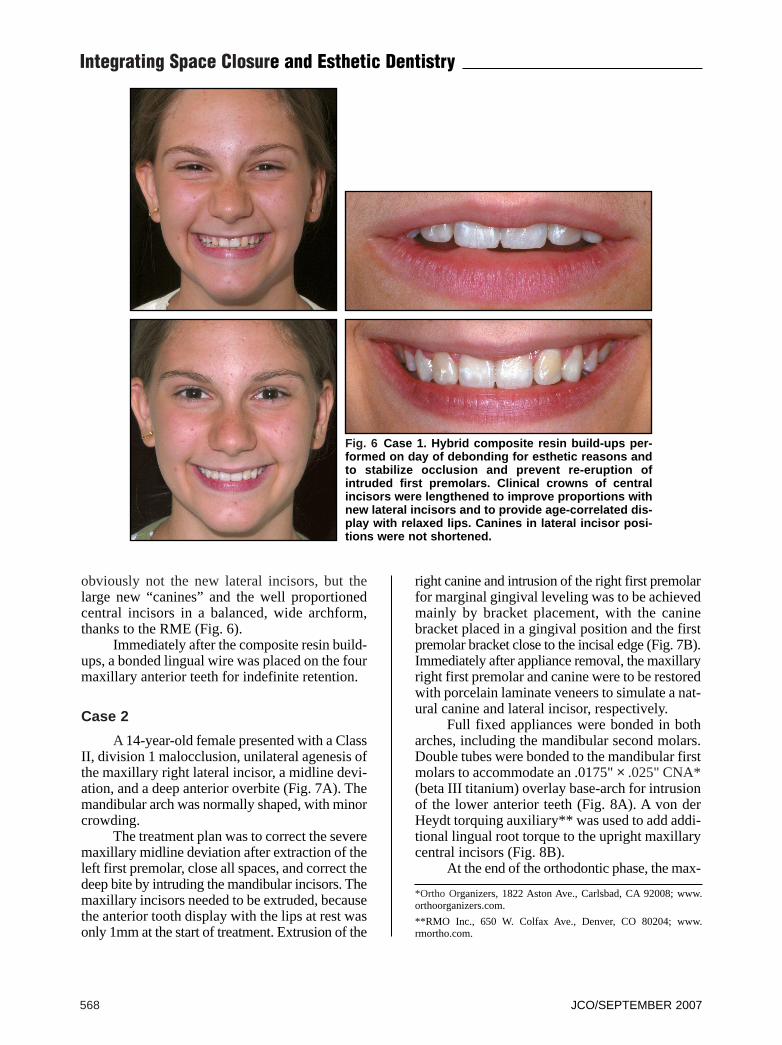
obviously not the new lateral incisors, but thelarge new “canines” and the well proportionedcentral incisors in a balanced, wide archform,thanks to the RME (Fig. 6).
Immediately after the composite resin build-ups, a bonded lingual wire was placed on the fourmaxillary anterior teeth for indefinite retention.
Case 2
A 14-year-old female presented with a ClassII, division 1 malocclusion, unilateral agenesis ofthe maxillary right lateral incisor, a midline devi-ation, and a deep anterior overbite (Fig. 7A). Themandibular arch was normally shaped, with minorcrowding.
The treatment plan was to correct the severemaxillary midline deviation after extraction of theleft first premolar, close all spaces, and correct thedeep bite by intruding the mandibular incisors. Themaxillary incisors needed to be extruded, becausethe anterior tooth display with the lips at rest wasonly 1mm at the start of treatment. Extrusion of the
right canine and intrusion of the right first premolarfor marginal gingival leveling was to be achievedmainly by bracket placement, with the caninebracket placed in a gingival position and the firstpremolar bracket close to the incisal edge (Fig. 7B).Immediately after appliance removal, the maxillaryright first premolar and canine were to be restoredwith porcelain laminate veneers to simulate a nat-ural canine and lateral incisor, respectively.
Full fixed appliances were bonded in botharches, including the mandibular second molars.Double tubes were bonded to the mandibular firstmolars to accommodate an .0175" × .025" CNA*(beta III titanium) overlay base-arch for intrusionof the lower anterior teeth (Fig. 8A). A von derHeydt torquing auxiliary** was used to add addi-tional lingual root torque to the upright maxillarycentral incisors (Fig. 8B).
At the end of the orthodontic phase, the max-
Fig. 6 Case 1. Hybrid composite resin build-ups per-formed on day of debonding for esthetic reasons andto stabilize occlusion and prevent re-eruption ofintruded first premolars. Clinical crowns of centralincisors were lengthened to improve proportions withnew lateral incisors and to provide age-correlated dis-play with relaxed lips. Canines in lateral incisor posi-tions were not shortened.
*Ortho Organizers, 1822 Aston Ave., Carlsbad, CA 92008; www.orthoorganizers.com.
**RMO Inc., 650 W. Colfax Ave., Denver, CO 80204; www.rmortho.com.
568 JCO/SEPTEMBER 2007
Integrating Space Closure and Esthetic Dentistry
illary right first premolar had been intruded and theright canine had been extruded and ground incisal-ly, producing a normal high-low-high marginal gin-gival contour (Fig. 8C). The maxillary midlinewas slightly overcorrected.
Cosmetic finishing was begun immediatelyafter appliance removal by Dr. Sverker Toreskogof Göteborg, Sweden. His treatment involved fab-rication of two ultrathin, enamel-bonded porcelainveneers after a minimally invasive preparation ofthe maxillary right first premolar and canine. The“artificial” right side of the maxilla was almostmore natural looking than the patient’s intact leftside (Fig. 8D).
The maxillary incisor display with relaxedlips was improved by at least 1mm due to theextrusion of the anterior teeth (Fig. 9). The post-treatment smile was full and radiant, with a mild
lingual crown tilt of the canines, straight premo-lars13 (Fig. 8D), and a smile arc consonant with theinner contour of the lower lip (Fig. 9).
Retention involved a six-unit maxillary lingualretainer bonded to the mesial occlusal surface of thefirst premolar, a maxillary removable plate, and amandibular 3-3 lingual retainer. The maxillary re-tainer was cut between the first premolar and canineduring fabrication to minimize the bulk of theentirely passive retainer, as described elsewhere.4
Discussion
These case reports demonstrate that a com-bination of carefully performed orthodontic spaceclosure and a cosmetic finishing stage, includingbuild-ups of anterior teeth with either compositeresin or porcelain laminate veneers, can achieve the
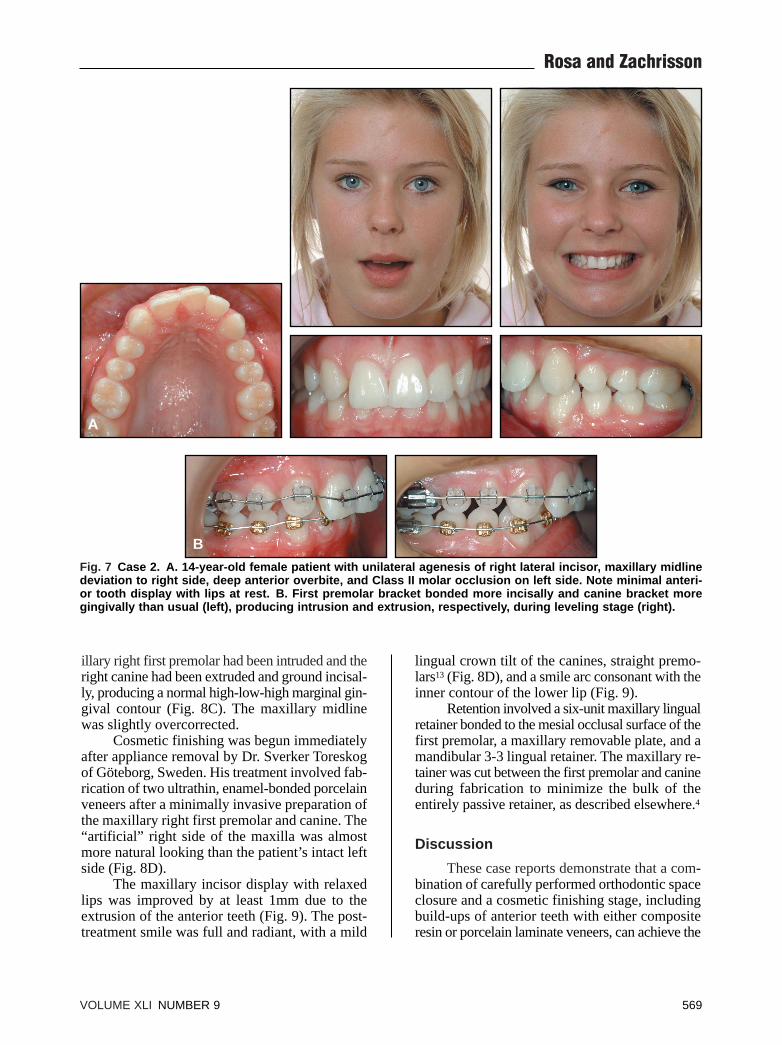
Fig. 7 Case 2. A. 14-year-old female patient with unilateral agenesis of right lateral incisor, maxillary midlinedeviation to right side, deep anterior overbite, and Class II molar occlusion on left side. Note minimal anteri-or tooth display with lips at rest. B. First premolar bracket bonded more incisally and canine bracket moregingivally than usual (left), producing intrusion and extrusion, respectively, during leveling stage (right).
A
B
VOLUME XLI NUMBER 9 569
Rosa and Zachrisson
look of a natural, healthy dentition in a patient withone or both missing maxillary lateral incisors anda coexisting malocclusion (Figs. 5,8D,9).
A major advantage of this approach is the per-manence of the finished result.1-4 Alveolar boneheight is maintained by early mesial movement ofthe canine, avoiding the need to use removable or
resin-bonded retainers until implants can be placed.The two most common reasons for postponingpermanent prosthetic treatment of young and ado-lescent patients—the risk of pulp perforation andthe exposure of gingival crown margins duringtooth eruption—are not contraindications for theminimally invasive ultrathin, enamel-bonded porce-
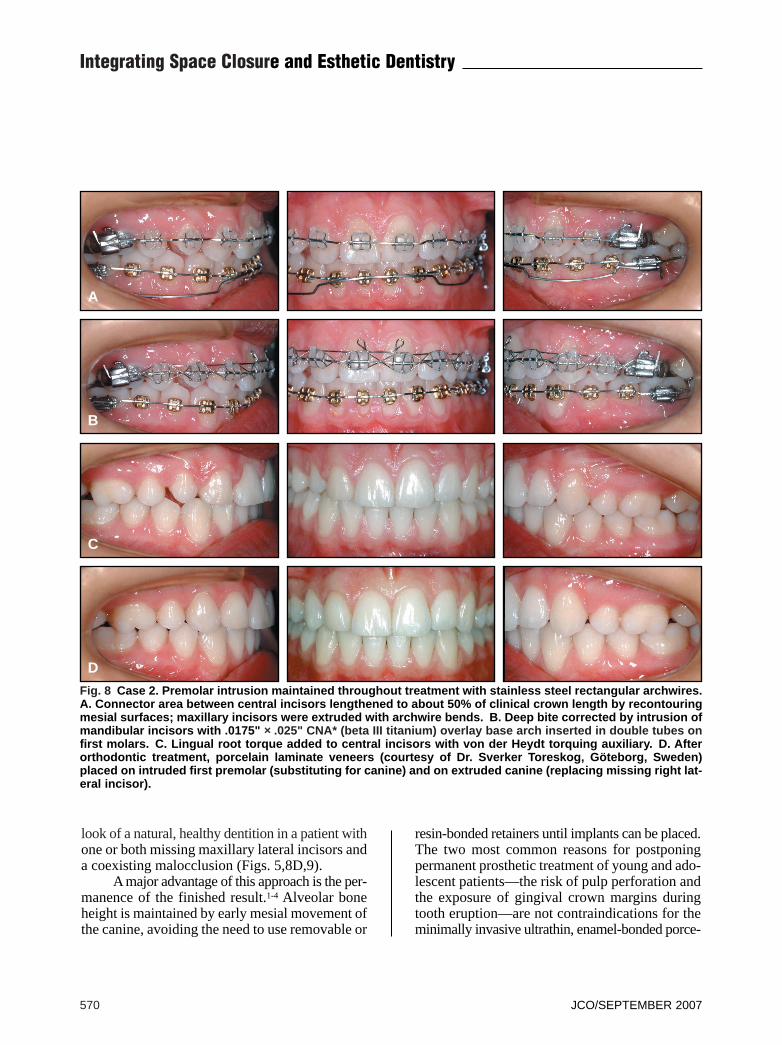
Fig. 8 Case 2. Premolar intrusion maintained throughout treatment with stainless steel rectangular archwires.A. Connector area between central incisors lengthened to about 50% of clinical crown length by recontouringmesial surfaces; maxillary incisors were extruded with archwire bends. B. Deep bite corrected by intrusion ofmandibular incisors with .0175" ×× .025" CNA* (beta III titanium) overlay base arch inserted in double tubes onfirst molars. C. Lingual root torque added to central incisors with von der Heydt torquing auxiliary. D. Afterorthodontic treatment, porcelain laminate veneers (courtesy of Dr. Sverker Toreskog, Göteborg, Sweden)placed on intruded first premolar (substituting for canine) and on extruded canine (replacing missing right lat-eral incisor).
A
B
C
D
570 JCO/SEPTEMBER 2007
Integrating Space Closure and Esthetic Dentistry
lain veneers, which can be placed directly on anyof the anterior teeth14-16 (Fig. 9). The only possibledisadvantage of the space-closure approach—thatspaces may reopen after treatment—can be over-come with long-term fixed retention, using a lin-gually bonded flexible spiral wire retainer from firstpremolar to first premolar1 (Fig. 5). The bondedretainer should be supplemented with a removableplate to be worn continuously for six months andthen only at night. A 10-year follow-up studyfound no apparent side effects with this regimen.17
Another important advantage of the space-closure alternative is that the healthy gingival tis-sues and intact interdental gingival papillae willchange in synchrony with the patient’s own teethover a lifetime. This is in contrast to current long-term experiences with single-implant porcelaincrowns in the esthetic zone.18-24 After only a five-year observation period,25 artificial crowns onosseointegrated implants have shown side effectssuch as progressive resorption of the labial boneplate and bluing of the overlying gingivae; pro-gressive infraocclusion, even in mature adults21,23;and gingival retraction and abutment exposure. Inan award-winning article describing 10-year fol-low-ups of oral implants, Thilander and colleaguesfound increasing degrees of infraocclusion even
after completion of growth, and significant mar-ginal bone loss at tooth surfaces adjacent to theimplants.21 It is our opinion, therefore, that max-illary lateral incisor agenesis patients with gummysmiles should be treated with space closure. If thetreatment plan includes space reopening, it ispreferable to open the spaces for prosthetic replace-ments in the premolar areas.24
We have emphasized that in lateral incisoragenesis cases, where the teeth tend to be relativelysmall, it is frequently desirable to build up the max-illary central incisors to improve the balance of thesix maxillary anterior teeth. If the patient has abroad face, the increased mesiodistal width of thecentral incisors will then be more harmoniouswith the width of the facial structures,4 and theoverall smile will be more esthetic than can beachieved with space reopening and placement ofsmall artificial lateral incisors. This approach willalso minimize the amount of grinding required onthe canines and improve the central incisor display(with relaxed lips and in speaking) in cases of in-sufficient incisor exposure.10-12
Although the materials currently used forcomposite resin build-ups can easily be adapted tocreate optimally esthetic tooth morphology, theyneed frequent repair. We therefore prefer to use the
Fig. 9 Case 2. After cosmetic finishing, maxillary midline is parallel to facial midline, and extrusion of maxil-lary incisors has improved anterior tooth display with lips at rest (compare with Figure 7A). Note natural toothsizes, shapes, colors, and gingival margins on agenesis side.
VOLUME XLI NUMBER 9 571
Rosa and Zachrisson
more durable porcelain veneers,14-16 except forcomposite “corners” on canines in lateral incisorpositions. Porcelain veneers can even be added aftera retention period or after occlusal adjustments ofthe functional occlusion by selective grinding.Porcelain veneers on the canines and first premo-lars (Fig. 9), or on the central incisors if these teethneed to be widened or elongated, are more expen-sive for the patient than grinding or compositebuild-ups, but they compare favorably with the costof restorations on single-tooth implants.22
Furthermore, lifetime maintenance of compositeresin build-ups may be more expensive than onewould expect. The porcelain veneers have shownlong-term durability and excellent esthetics, evenif the gingival margin retracts with time.15,16 Lightreflected on porcelain veneers appears normal, incontrast to ceramic crowns and porcelain crownsfused to gold, where the shadows of incominglight tend to produce dark backgrounds.15,16
Given our recent successful experience, thecustomary contraindications for space closureshould be reconsidered.1 Agenesis of lateral incisorsin Class III malocclusions, especially in caseswith narrow maxillae and pronounced spacing(such as Case 1), has traditionally been regardedas an inarguable indication for space reopening andprosthetic rehabilitation. The reopening of spacessupposedly facilitates maxillary arch expansion andprovides dentoalveolar compensation with signif-icant profile improvement. Nevertheless, bothClass III malocclusion cases shown here (Figs. 1-6), like other cases to be reported in a further arti-cle in this series, demonstrate that space closure canbe a valuable alternative for careful and detailedorthodontic treatment, providing long-term sta-bility after appliance removal (Fig. 1). Recentadvances in miniscrew techniques may improveanchorage control in these cases.
Lateral incisor agenesis patients with exces-sive gingival display in smiling, especially youngones, should not be treated with space reopeningand lateral incisor implant placement. It is incon-ceivable that such a technique can achieve thelong-term occlusal, gingival, and periodontalresults in the esthetic zone that are seen with spaceclosure1,24 (Fig. 1). Even unilateral space closure,
which has long been ruled out in a patient with onlyone missing lateral incisor, can provide a satis-factory outcome from both the esthetic and func-tional25,26 points of view when coupled withcosmetic finishing (Figs. 7-9).
Conclusion
This article has described how to furtherimprove clinical results using space closure andcosmetic finishing in patients with missing max-illary lateral incisors. The following factors havebeen considered:1. Natural marginal gingival contours (high-low-high) can be achieved by selective extrusionand intrusion of the canines and first premolars,respectively.2. Restoration of intruded first premolars withcomposite resin build-ups or porcelain veneers isnecessary to reshape such teeth to resemble nat-ural canines and to produce a balanced smile.3. Composite build-ups may also be required onthe central incisors for two reasons: the caninescannot be ground beyond the diameter of theroots and may be too wide for the existing cen-tral incisors, and the patient’s incisor displaywith relaxed lips is often inadequate.4. Attention to achieving correct maxillary arch-form and torque of the posterior teeth will ensurea full and radiant smile.5. Enamel-bonded porcelain veneers provideimproved esthetics with less need for mainte-nance than composite resin build-ups.6. The major advantages of space closure arethat treatment is finished at an early age, that theresult is permanent, and that optimum gingivaland periodontal health can be preserved, withlater modifications occurring in synchrony withthe patient’s own teeth.7. For these reasons, space closure is particularlyindicated in agenesis patients with gummysmiles.8. A Class III malocclusion (even with a narrowmaxilla) is not a contraindication for space closure.Treatment may be more difficult, but a natural-looking result is possible with good cooperation.
572 JCO/SEPTEMBER 2007
Integrating Space Closure and Esthetic Dentistry
1. Rosa, M. and Zachrisson, B.U.: Integrating esthetic dentistryand space closure in patients with missing maxillary lateral in-cisors, J. Clin. Orthod. 35:221-234, 2001.
2. Tuverson, D.L.: Orthodontic treatment using canines in placeof missing maxillary lateral incisors, Am. J. Orthod. 58:109-127, 1970.
3. Tuverson, D.L.: Close space to treat missing lateral incisors,Am. J. Orthod. 125:17A, 2004.
4. Zachrisson, B.U.: Improving the esthetic outcome of caninesubstitution for missing maxillary lateral incisors, World J.Orthod. 8:72-79, 2007.
5. Dietschi, D. and Schatz, J.P.: Current restorative modalities foryoung patients with missing anterior teeth, Quintess. Int.28:231-240, 1997.
6. Kokich, V.O. Jr. and Kinzer, G.A.: Managing congenitallymissing lateral incisors, Part I: Canine substitution, J. Esth.Restor. Dent. 17:5-10, 2005.
7. Armbruster, P.C.; Gardiner, D.M.; Whitley, J.B.; and Flerra, J.:The congenitally missing maxillary lateral incisor, Part 1:Esthetic judgment of treatment options, World J. Orthod.6:369-375, 2005.
8. Armbruster, P.C.; Gardiner, D.M.; Whitley, J.B.; and Flerra, J.:The congenitally missing maxillary lateral incisor, Part 2:Assessing dentists’ preferences for treatment, World J. Orthod.6:376-381, 2005.
9. Sabri, R.: Management of missing maxillary lateral incisors, J.Am. Dent. Assoc. 130:80-84, 1999.
10. Zachrisson, B.U.: Esthetic factors involved in anterior toothdisplay and the smile: Vertical dimension, J. Clin. Orthod.32:432-445, 1998.
11. Vig, R.G. and Brundo, G.C.: The kinetics of anterior tooth dis-play, J. Prosth. Dent. 39:502-504, 1978.
12. Dong, J.K.; Jin, T.H.; Cho, H.W.; and Oh, S.C.: The estheticsof the smile: A review of some recent studies, Int. J. Prosthod.12:9-19, 1999.
13. Zachrisson, B.U.: Buccal uprighting of canines and premolarsfor improved smile esthetics and stability, World J. Orthod.7:406-412, 2006.
14. Curry, F.T.: Porcelain veneers: Adjunct or alternative to ortho-dontic therapy, J. Esth. Dent. 10:67-74, 1998.
15. Zachrisson, B.U. and Toreskog, S.: Esthetic considerations inrestoring the traumatized dentition: A biological approach, inTextbook and Color Atlas of Traumatic Injuries to the Teeth,
4th ed., ed. J.O. Andreasen, F.M. Andreasen, and L. Andersson,Blackwell Munksgaard Co., England, 2007, pp. 798-813.
16. Zachrisson, B.U. and Toreskog, S.: Missing maxillary centralincisors: Interdisciplinary approach with orthodontic space clo-sure, autotransplantation of premolars, and single-tooth im-plants, in The Art of the Smile, ed. R. Romano, QuintessencePublishing Co., New Malden, England, 2005, pp. 142-166.
17. Thordarson, A.; Zachrisson, B.U.; and Mjör, I.A.: Remodelingof canines to the shape of lateral incisors by grinding: A long-term clinical and radiographic evaluation, Am. J. Orthod.100:123-132, 1991.
18. Weisgold, A.S.; Arnoux, J.P.; and Lu, J.: Single-tooth anteriorimplant: A word of caution, Part I, J. Esth. Dent. 9:225-233,1997.
19. Arnoux, J.P.; Weisgold, A.S.; and Lu, J.: Single-tooth anteriorimplant: A word of caution, Part II, J. Esth. Dent. 9:285-294,1997.
20. Belser, U.C.; Buser, D.; Hess, D.; Schmid, B.; Bernard, J.P.;and Lang N.P.: Aesthetic implant restorations in partially eden-tulous patients: A critical appraisal, Periodontol. 2000 17:132-150, 1998.
21. Thilander, B.; Odman, J.; and Lekholm, U.: Orthodonticaspects of the use of oral implants in adolescents: A 10-yearfollow-up study, Eur. J. Orthod. 23:715-731, 2001.
22. Salama, H.; Garber, D.A.; Salama, M.A.; Adar, P.; and Rosen-berg, E.S.: Fifty years of interdisciplinary site development:Lessons and guidelines from periodontal prosthesis, J. Esth.Dent. 10:149-156, 1998.
23. Bernard, J.P.; Schatz, J.P.; Christou, P.; Belser, U.; and Kiliari-dis, S.: Long-term vertical changes of the anterior maxillaryteeth adjacent to single implants in young and mature adults: Aretrospective study, J. Clin. Periodontol. 31:1024-1028, 2004.
24. Zachrisson, B.U.: Single implant-supported crowns in the ante-rior maxilla: Potential esthetic long-term (> 5 years) problems,World J. Orthod. 7:306-312, 2006.
25. Nordquist, G.G. and McNeill, R.W.: Orthodontic vs. restora-tive treatment of the congenitally absent lateral incisor: Long-term periodontal and occlusal evaluation, J. Periodont. 46:139-143, 1975.
26. Robertsson, S. and Mohlin, B.: The congenitally missing upperlateral incisor: A retrospective study of orthodontic space clo-sure versus restorative treatment, Eur. J. Orthod. 22:697-710,2000.