61
Integumentary Integumentary Diseases, Disorders, Diseases, Disorders, and Conditions and Conditions Part I of II Part I of II As presented November 2014 H. Biology II
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | june-sherman |
| View: | 214 times |
| Download: | 1 times |

Integumentary Diseases, Integumentary Diseases, Disorders, and ConditionsDisorders, and Conditions
Part I of IIPart I of IIAs presented November 2014
H. Biology II

Definitions• Disease- an abnormal condition of
the body or the mind that causes dysfunction or discomfort.
• Disorder- a functional abnormality, or disturbance.
• Condition- a state of being, in health, a disease, such as a heart condition.
Top Skin Diseases
• Scaly Red Rashes (5)
• Pigment Changes (2)
• Nodules (2)
• Purpura (1)
• Blisters (4)
• Systemic (3)
• Benign Growths (3)
• Premalignant Growths (2)
• Malignant Growths (3)

Scaly Red Rash 1: Seborrhea
focal parakeratosis, moderate acanthosis, slight
spongiosis and a mild, mixed inflammatory infiltrate. "cradle cap"
Greasy yellow scaly plaques are characteristically distributed in the scalp, Tzone of face, hairy areas of face (eyebrows, eyelashes, beard), behind the ears, on the forehead, trunk, body folds, and genitalia.Unknown etiology.

Scaly Red Rash 2: Psoriasis
Red or pink papule/plaque with silvery or micaceous scaling. The fingernails may show dystrophy, depressions known as "pits" and subungual debis
presence of a thickened epidermis and stratum corneum containing neutrophils and neutophilic debris; no granular layer, elongation of the rete ridges; T cell involvement in etiology

Psoriasis• It can appear anywhere on the body,
but it is most commonly found on the elbows, knees, scalp, and lower back.
• Skin typically becomes red and inflamed and may form white scaly patches.
• It can be quite painful and may itch, crack, and bleed.
• While psoriasis may look like just a skin disease, it is in fact a disease of the immune system.




Scaly Red Rash 3: TineaCentrifugally spreading, reddish or pink plaques or patches with slightly raised advancing edge. Annular. Itchy rash caused by fungus Tricophytum rubrum in most cases.
Tinea corporis Tinea corporis
Tinea capitis
Tinea pedis
Tinea unguium
Tinea capitis KOH prep on hair“spaghetti and meatballs”
Tinea versicolor
Tinea versicolor
Parakeratosis PAS stain showing fungi
thick stratum corneum

Tinea Pedis- Athletes’ Foot
• Athlete's foot is a very common skin infection of the foot caused by fungus.
• . When the feet or other areas of the body stay moist, warm, and irritated, this fungus can thrive and infect the upper layer of the skin..
• Athlete's foot is caused by the ringworm fungus ("tinea" in medical jargon). Athlete's foot is also called tinea pedis. The fungus that causes athlete's foot can be found on many locations, including floors in gyms, locker rooms, swimming pools, nail salons, and in socks and clothing.
• The fungus can also be spread directly from person to person or by contact with these objects.




Scaly Red Rash 4: Eczema
Eczema is very itchy. There are variants of eczema, the so-called "messy" rash, for example, "irritant" eczema, atopic eczema, and contact eczema, all of which are characterized by rashes that are quite itchy and appear "messy" because they are often scratched.TH2 mediated DTH
Flexural distribution
Lichenification from scratching
crusting in the stratum corneum (making one think of a "messy rash") and the "spongiosis" or epidermal edema, as evidenced by the relative pallor around the keratinocytes.

Eczema• Eczema most commonly causes dry,
reddened skin that itches or burns, although the appearance of eczema varies from person to person and varies according to the specific type of eczema.
• Intense itching is generally the first symptom in most people with eczema.
• Sometimes, eczema may lead to blisters and oozing lesions, but eczema can also result in dry and scaly skin.
• Repeated scratching may lead to thickened, crusty skin.




Scaly Red Rash 5: ScabiesScabies (or infestation with the Sarcopetes mite), especially when untreated, can lead to a widespread eczema rash with a few additional distintive features such as heavy involvement in the groin or skin folds and, in particular, involvement of the interdigital web spaces with crusting.
one finds a lot going on in the stratum corneum. Here one can see traces of the mite.

Pigment Changes 1: Vitiligo
With Fontana Masson stain, lesions of long standing vitiligo (right hand panel) show no melanocytes. In normal skin (left panel) darkly stain melanocytes are visible along the dermoepidermal junction.

Vitiligo• Vitiligo (vit-ill-EYE-go) is a pigmentation
disorder in which melanocytes (the cells that make pigment) in the skin are destroyed. As a result, white patches appear on the skin in different parts of the body.
• Similar patches also appear on both the mucous membranes (tissues that line the inside of the mouth and nose), and the retina (inner layer of the eyeball).
• The hair that grows on areas affected by vitiligo sometimes turns white.



Pigment Changes 2: Melasma
large amount of melanin in the basal layer

Papules/Plaques 1: Warts
The hallmarks of warts are hyperkeratosis, papillomatosis (outward expansion of the spinous layer) and acanthosis. The epidermis contains foci of vacuolated cells (koilocytes), clumped keratohyaline granules, and vertical tiers of parakeratotic cells (stratum corneum with retained nuclei).
Flat wart
Genital wart
Aka condyloma acuminatum
Plantar wart
HPV mediated. Here shown is common wart

Warts• Common warts are local growths in the
skin that are caused by human papillomavirus (HPV) infection.
• Although they are considered to be contagious, it is very common for just one family member to have them.
• They often affect just one part of the body (such as the hands or the feet) without spreading over time to other areas.




Papules/Plaques 2: Molluscum
dome-shaped pink-brown papules with secondary umbilication noted in mnay of the well-developed lesions
ballooning-like changes in the keratinocytes as they approach the granular layer. There are intracellular inclusion bodies known as molluscum bodies.

Papules/Plaques 3: Acne Vulgaris

Acne Vulgaris• Acne vulgaris is a common skin disease
that affects 85-100% of people at some time during their lives.
• It is characterized by non-inflammatory pustules or comedones, and by inflammatory pustules, and nodules in its more severe forms.
• Acne vulgaris affects the areas of skin with the densest population of sebaceous follicles; these areas include the face, the upper part of the chest, and the back.
• Treatment is a regimine of topical creams, and oral antibiotics, and or steroids.



Papules/Plaques 4: Urticaria (Hives)
There is little that appears wrong in this histology except for the fact that there is a separation of the collagen bundles, more so than one would usually see in normal skin. There is also a sparse infiltrate in which an occasional lymphocyte may be seen

Urticaria• Hives (medically known as urticaria) are
red, itchy, raised areas of skin that appear in varying shapes and sizes.
• They range in size from a few millimeters to several inches in diameter.
• Hives can be round, or they can form rings or large patches.
• Wheals (welts), red lesions with a red "flare" at the borders, are another manifestation of hives.
• Hives can occur anywhere on the body, such as the trunk, arms, and legs.




Papules/Plaques 5: Erythema Multiforme
The pathologic features of erythema multiforme include a perivascular, lymphocytic infiltrate of variable intensity, vacuolization of the dermal-epidermal junction, extravasation of red blood cells without vasculitis, papillary dermal edema, and variable eosinophilic necrosis of the epidermis.

Nodules 1: Erythema Nodosum
histologic findings associated with erythema nodosum are largely localized to the deep dermis and the subcutaneous tissue. There is an accumulaton of lymphocytes, neutrophils, histiocytes, and giant cells accumulate in the fibrous septae between fat lobules and perivascular infiltration of lymphocytes in the dermis.
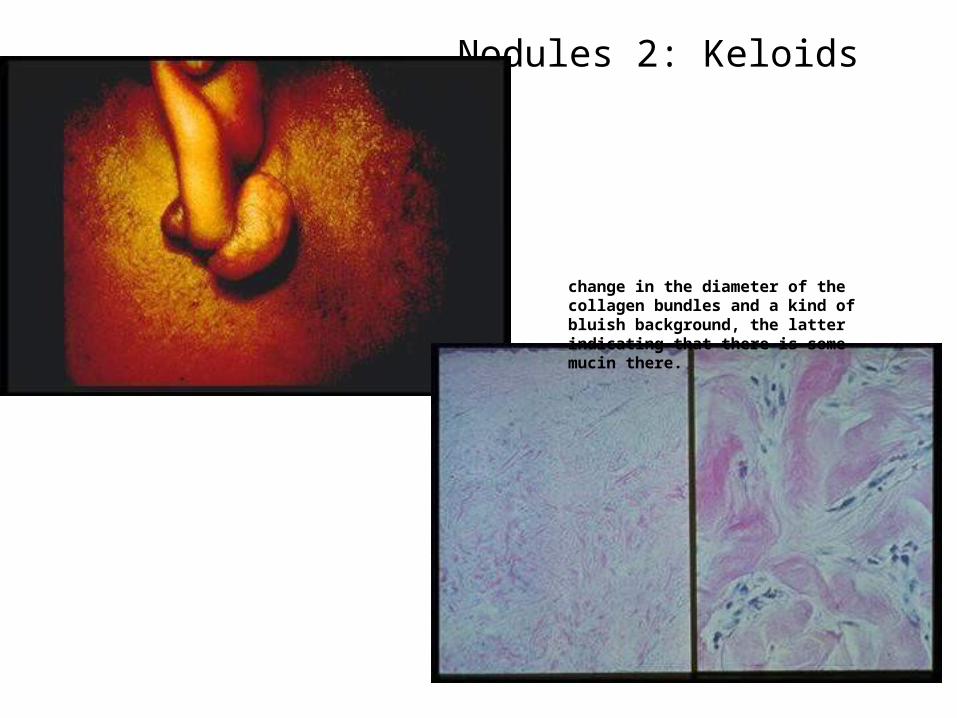
Nodules 2: Keloids
change in the diameter of the collagen bundles and a kind of bluish background, the latter indicating that there is some mucin there.

Keloid• A keloid is a scar that doesn't know
when to stop. When the cells keep on reproducing, the result is an overgrown (hypertrophic) scar or a keloid.
• A keloid looks shiny and is often dome-shaped, ranging in color from slightly pink to red.
• It feels hard and thick and is always raised above the surrounding skin.





Purpura 1: Vasculitis
larger vessel is involved in an inflammatory porcess
vasculitis of the superficial vascular plexus. One sees extravation of red blood cells, indicating that the vessels must have been damaged. There is a lot of neutrophilic debris.

Blisters 1: Herpes
cells in the epidermis are undergoing degenerative changes. There is acantholysis (epidermal cells falling apart) and enlarging of the nuclei. In some specimens, one might be lucky enough to see the diagnostic mlti-nucleated giant cells
Note: these images are kind of weak, also, not sure if they are only referring to HSV 1 or HSV 1 and HSV 2.
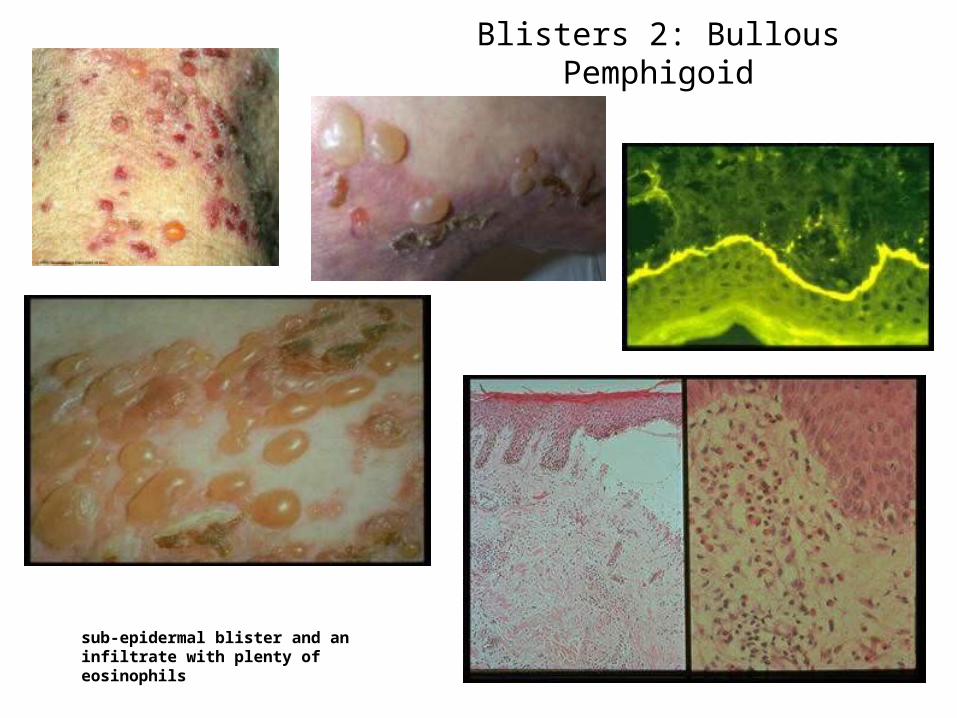
Blisters 2: Bullous Pemphigoid
sub-epidermal blister and an infiltrate with plenty of eosinophils

Blisters 3: Pemphigus Vulgaris
INTRAEPIDERMAL split! (above basal layer)
Mucosal involvement

Blisters 4: Acute Contact Dermatitis

Contact Dermatitis• The word "dermatitis" means
inflammation of the skin. • In contact dermatitis, the skin becomes
extremely itchy and inflamed, causing redness, swelling, cracking, weeping, crusting, and scaling.
• Dry skin is a very common complaint and an underlying cause of some of the typical rash symptoms.
• This is usually occupationally related: hair stylists, medical personnel, photographers, etc.



Systemic 1: Lupus
discoid lupus. There is a perivascular and periappendageal lymphocytic infiltrate that also tends to hug the dermo-epidermal junction, the latter type of infiltrate being referred to as "lichenoid

Systemic 2: Scleroderma
The collagen bundles are thickened and homogenized.

Systemic 3: Drug Eruption

Benign Growths 1: Lentigo
LentiginesThese brown macules are sometimes inappropriately referred to as "liver spots" by lay people.
two features here: the excess pigment in the basal layer and the peculiar elongation of the epidermis itself, sometimes likened to a "hockey stick".

Benign Growths 2: Seborrheic Keratosis
epidermal growth whose borders can almost be distinguished by a pencil line drawing. The cells are banal and basophilic. There are often "pseudo-horn cysts" or keratinaceous intra-epidermal inclusions.

















