Inter-Rater Reliability amongst Clinical Team-Members for Scoring the Acute Asthma Intensity Research Score (AAIRS) Donald H Arnold, MD, MPH Pediatric Emergency Medicine Center for Asthma Research Vanderbilt University School of Medicine Nashville, Tennessee, USA
Transcript
Inter-Rater Reliability amongst Clinical Team-Members for Scoring
the Acute Asthma Intensity Research Score (AAIRS)
Donald H Arnold, MD, MPH
Pediatric Emergency Medicine
Center for Asthma Research
Vanderbilt University School of Medicine
Nashville, Tennessee, USA
Conflict of Interest Statement Speaker: Donald H Arnold
Supported by UL1 RR024975 (Vanderbilt CTSA), T32 GM07569 (O’Connor).
The speaker has no other competing interests or disclosures.
Background: Acute Asthma Exacerbations
• Most common reason for childhood hospitalization in North America
• Frequent reason for Emergency Department (ED) visits
• Variability of assessment that drives management and hospitalization decision
0
1
2
3
4
5
0 1 2 3 4 5
Treatment Tier Received
by Patient
Acute Asthma Exacerbation Severity
Treatment tier administered to 933 patients according to exacerbation severity. Bubbles correspond to number of patients. Blue line bisects bubbles that represent appropriate treatment tier for exacerbation severity.
Need for Valid and Reliable Exacerbation Severity Assessment
• Emergency Department exacerbation care
– Pulmonary function testing not available
– Multiple clinical team members and hand-offs
– Need for bedside assessment tools to guide treatment and hospitalization decision-making
Objectives
• To examine the inter-rater reliability between nurses, respiratory therapists, and attending clinicians for
– The 7 individual components of the Acute Asthma Intensity Research Score (AAIRS)
– The total AAIR Score
• Drives treatment and hospitalization decision-making
The Acute Asthma Intensity Research Score (AAIRS)
• Patient characteristics chosen a priori that
– Are easily measured and available at the bedside
– Encompass multiple domains of exacerbation severity
• Validated against FEV1 and airway resistance
1. Criterion validity
2. Responsiveness
Arnold DH, Saville BR, Wang W, Hartert TV. Ann Allergy Asthma Immunol. 2012;109(1):78. Arnold DH, O’Connor MG, Hartert TV. Ann Allergy Asthma Immunol. 2015;115(1):69.
The Acute Asthma Intensity Research Score (AAIRS)
Component Exacerbation severity Domain
Component point range Accessory Muscle Use
Sternocleidomastoid
Work of breathing
0 or 2
Intercostal 0 or 2
Subcostal 0 or 2
Air entry Airway obstruction, atelectasis 0 – 3
Wheezing Airway obstruction 0 – 3
SpO2 on room air V/Q mismatch, mucosal edema 0 – 2
Expiratory phase Airway obstruction 0 – 2
Possible total score range 0 - 16
Severity levels: mild 1-6; moderate 7-11; severe 12-16.
Methods • Team member comparisons
1. Attending clinicians vs. Respiratory therapists
2. Attending clinicians vs. Nurses
3. Nurses vs. Respiratory therapists
• Verbal instruction in AAIRS use
• Score patients 3-17 years with acute asthma exacerbations before treatment and 1-hr after albuterol + systemic corticosteroid
O’Connor MG, Berg K, Stack LB, Arnold DH. Ann Allergy Asthma Immunol. In press.
Characteristics of clinical team members scoring AAIRS components and of children with acute asthma exacerbations Number of participating clinical team members
Respiratory therapist 22
Nurse 50
Physician / Nurse practitioner 48
Patients with acute asthma exacerbations
Unique patients, number 144
Median age, years [IQR] 5 [3.3, 8]
Male gender 67%
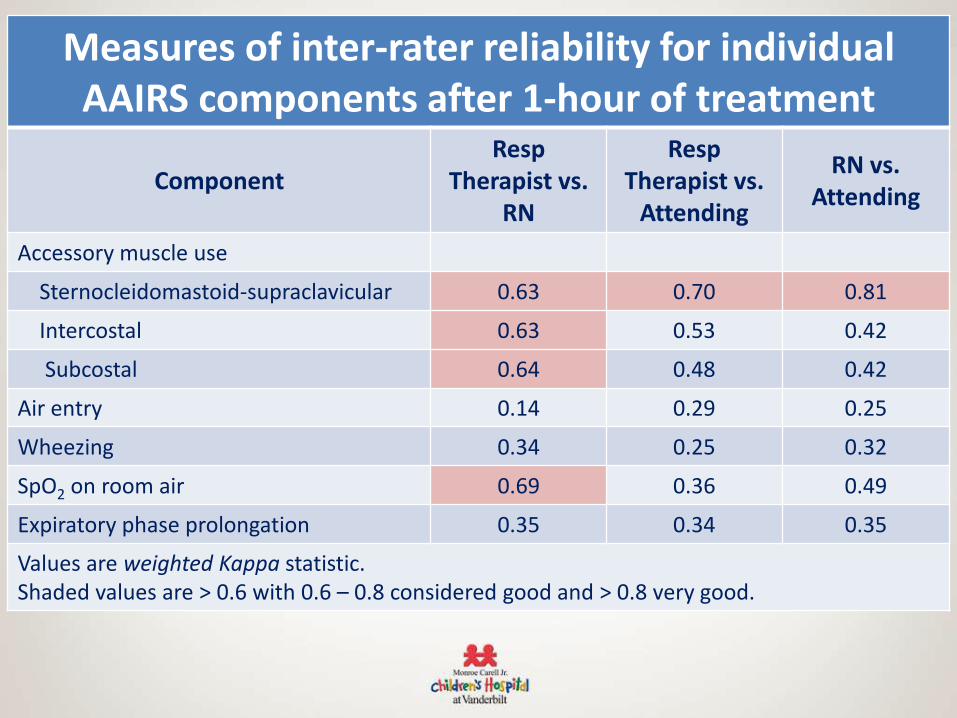
Measures of inter-rater reliability for individual AAIRS components before treatment
Co-investigators Michael G. O’Connor, MD; Pediatric Pulmonary Medicine Kathleen Berg, MD; Emergency Medicine; Lawrence B. Stack, MD; Emergency Medicine Biostatistician Li Wang, MS

















![[PPT]Inter-Rater Reliability - Home - Ivy Tech Community … · Web viewInter-Rater Reliability Respiratory Ivy Tech Community College-Indianapolis What Is Inter-Rater Reliability](https://static.documents.pub/doc/80x56/5aefd30e7f8b9a572b8ea7b7/pptinter-rater-reliability-home-ivy-tech-community-viewinter-rater-reliability.jpg)










