Interactions between health systems and Global Health Initiatives: a WHO/Italy collaborative effort Carissa Etienne Assistant Director-General Health Systems and Services World Health Organization
Transcript
Interactions between health systems and Global Health Initiatives: a WHO/Italy collaborative effort
Carissa EtienneAssistant Director-General
Health Systems and ServicesWorld Health Organization
The context: Global progress on MDG 4
The context: Global progress on MDG 5
The context: Global progress on ART
The diagnostic: the challenges to scale up services for HIV, TB, malaria, and immunization
upper middle income lower middle income low income
Upper Middle Income
What fuels the debate: Government Health spending per capita
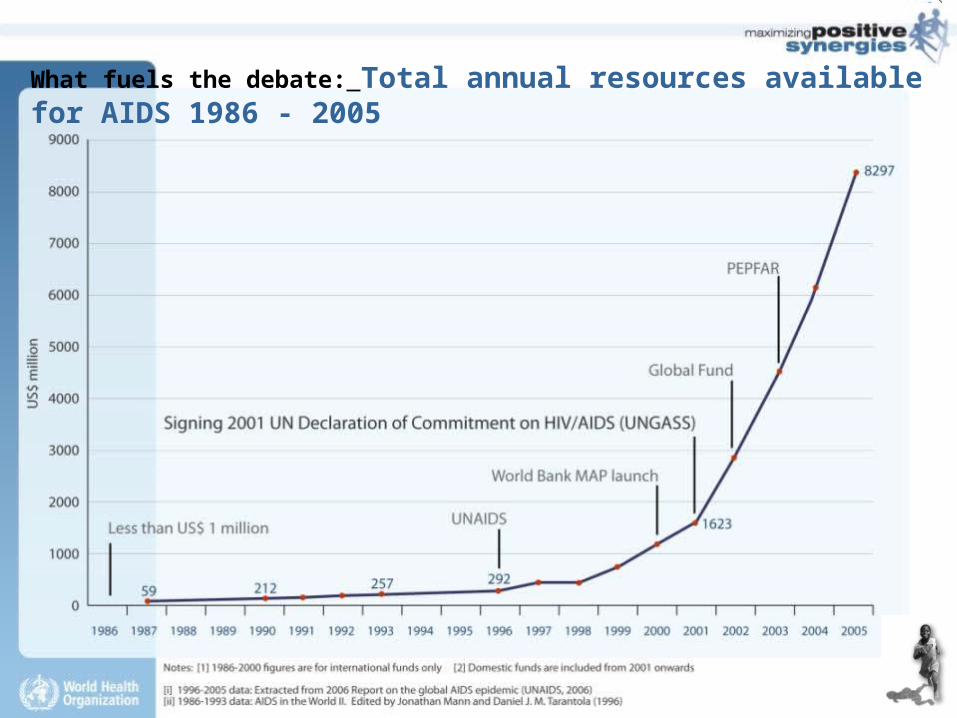
What fuels the debate: Total annual resources available for AIDS 1986 - 2005
The reality check: Life Expectancy vs. Spending
The reality check: Health outcomes and health spending
deprived suburbdeprived suburb
YE
AR
S
But money is not all: Life expectancy in Glasgow, UK
WHR, 2006
100
5454
8282
affluent suburbaffluent suburb
The right question
How can global health initiatives and country health systems optimize their interactions to achieve their common goal of improving health outcomes?
In other words: we need to look at the big picture
The good signals: GAVI and Health Systems Strengthening
The good signals: Global Fund and Health Systems Strengthening
The good signals: PEPFAR and Health Systems Strengthening
• Normative work and wide implementation of Task Shifting• Commitment to produce 140,000 health care workers in PEPFAR2• Importance of broad health systens strenthening in PEPFAR 2
Make the slide nicer -- Add here a PEPFAR photo or logo (Francesca)
1. Time2. Time3. Time
The big challenge 1: not to miss the opportunity
The big challenge 2: do it right
The process: a broad multi-stakeholder collaboration
• Academia
• Civil Society
• Implementers and GHIs
Make the slide nice and add a photo (Francesca)
The products: a broad multi-stakeholder collaboration
• An academic in a peer-review journal
• A case library
• A set of recommendations
• A declaration
Findings
Known sources
- 14 new studies
- Over 250 studies and reports
- 22 country case studies
Two emerging points
- GHIs and country health systems are not independent - GHIs and country health systems are dynamic,
complex entities
studying their interactions defies over-simplistic, single variable, linear analysis and
raises caution with respect to generalizations.
Findings: service delivery
– Expanded access and uptake of targeted services (caution: attribution)
– Expanded access and uptake of non targeted services
– Evidence on role of GHIs or health systems on equity and quality of health services is weak and mixed
Polio vaccination, Haiti
Prenatal visits, Rwanda
Findings: finance
– Association of GHIs with overall increases in global resources for health
– No clear correlation between GHI resources and domestic health budgets or reallocation of resources
– GHIs have contributed to some improvements in health aid-effectiveness, particularly in the area of predictability of financing
– Indication that disease-specific funding may not be well enough aligned
Government spending on HIV
Findings: governance
– Evidence of early lack of alignment
– More recent progress
– Enhanced community participation
Findings: health workforce
– Some potentially negative impacts on already overstretched human resources for health
– Measures to strengthen the health workforce ongoing
– Measures more on in-service training for disease-specific services, and task shifting
Findings: health information
– Focus on coverage, and surveillance for specific diseases
– Innovations in generation and use of new information and communication technologies
– Failure to invest in more rational, robust, efficient and independent common data architecture.
Findings: supply management
– Improvements in availability and affordability of a number of commodities
– Growth in the volume of commodities not matched by improvements in the management of supplies
The recommendations
– Be Bold – Set targets– Enhance leadership – Engage communities – Improve evidence




































![[Etienne Gilson] Christian Philosophy (Etienne Gil(Bookos.org)](https://static.documents.pub/doc/80x56/553f92924a7959960d8b47ef/etienne-gilson-christian-philosophy-etienne-gilbookosorg.jpg)











