31
Interesting Case Rounds Rebecca Burton-MacLeod R5 (yikes!), Emerg Med July 5 th , 2007
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | gavin-bradford |
| View: | 221 times |
| Download: | 2 times |
Interesting Case Rounds
Rebecca Burton-MacLeod
R5 (yikes!), Emerg Med
July 5th, 2007
Case
21M presents to ED c/o CPX ~4 hrs
Retrosternal, radiated bilaterally
Not pleuritic
+ SOB +nauseas; not dizzy, no palpitations
Also c/o generalized abdo pain, and pain to bilateral thighs (present x2days)
History cont’d
No previous similar episodes, but sometimes his legs “have pain” Pt moved from India about 2mos prior, ++ language barrier !
PMHx: “healthy”Meds: noneAllergies: none
Further hx
Questions ?
Physical examHR 115, BP 128/72, RR 26, Temp 37.9, sats 92% r/aPt ++ uncomfortable, tearfulCNS—A+OCVS—N heart sounds, PPPResp—lungs clearAbdo—generalized mild tenderness, no guarding, no rebound, + BSMSK—c/o ++ tenderness to palpation bilateral thighs; no erythema or swelling noted
Investigations
??
Investigations
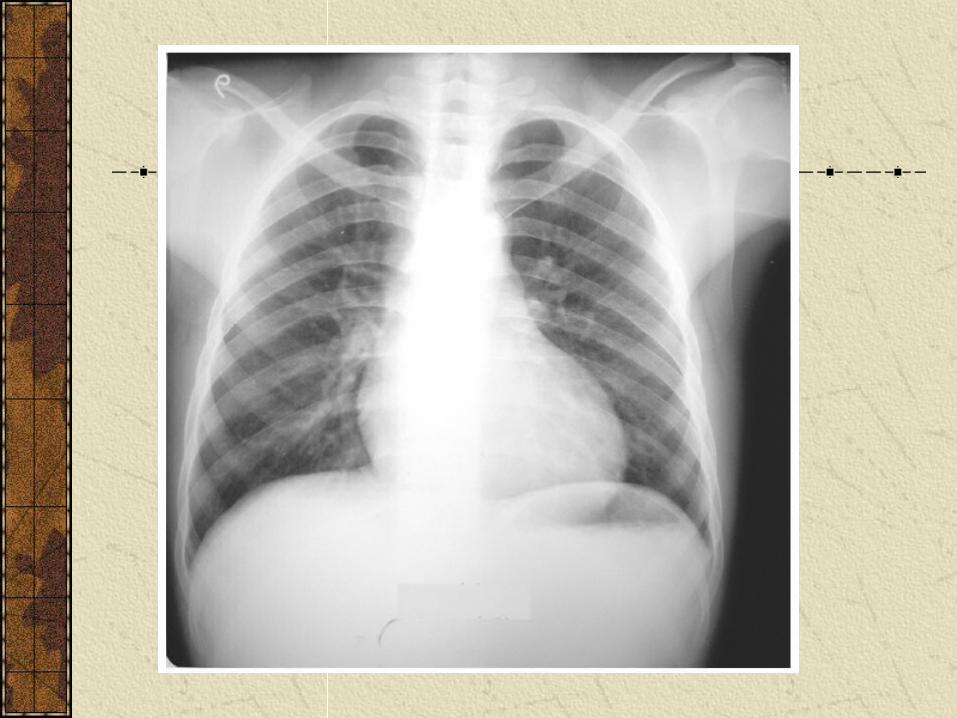
CXR
EKG
CBC, lytes, Cr
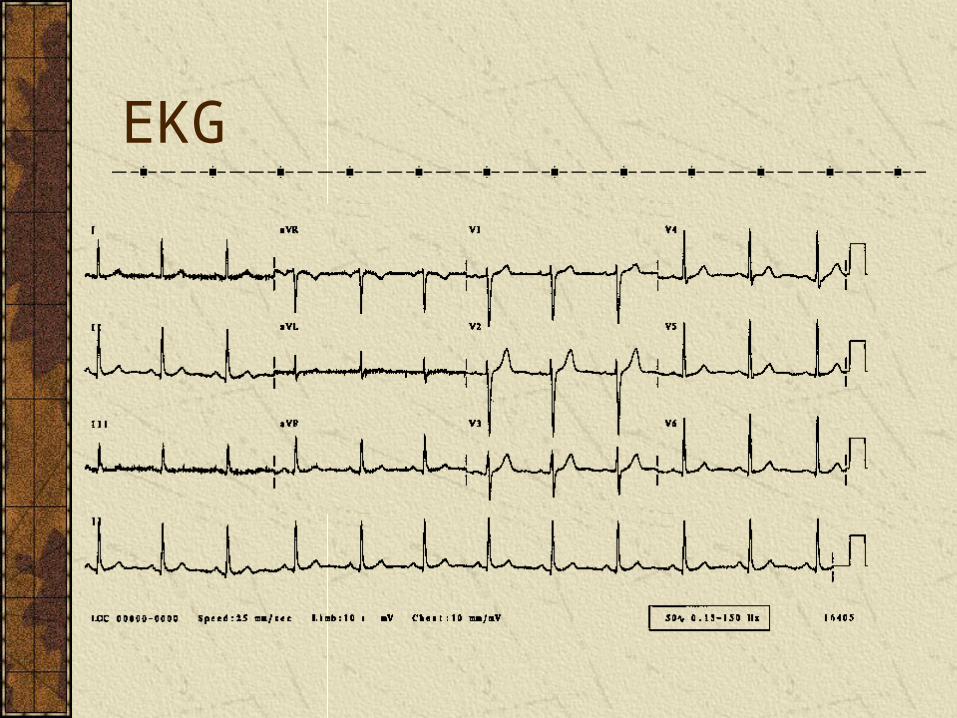
EKG
Bloodwork
Hgb 77
Plt 185
WBC 31
Lytes, Cr N
“Have you ever been told you have anemia before?”…
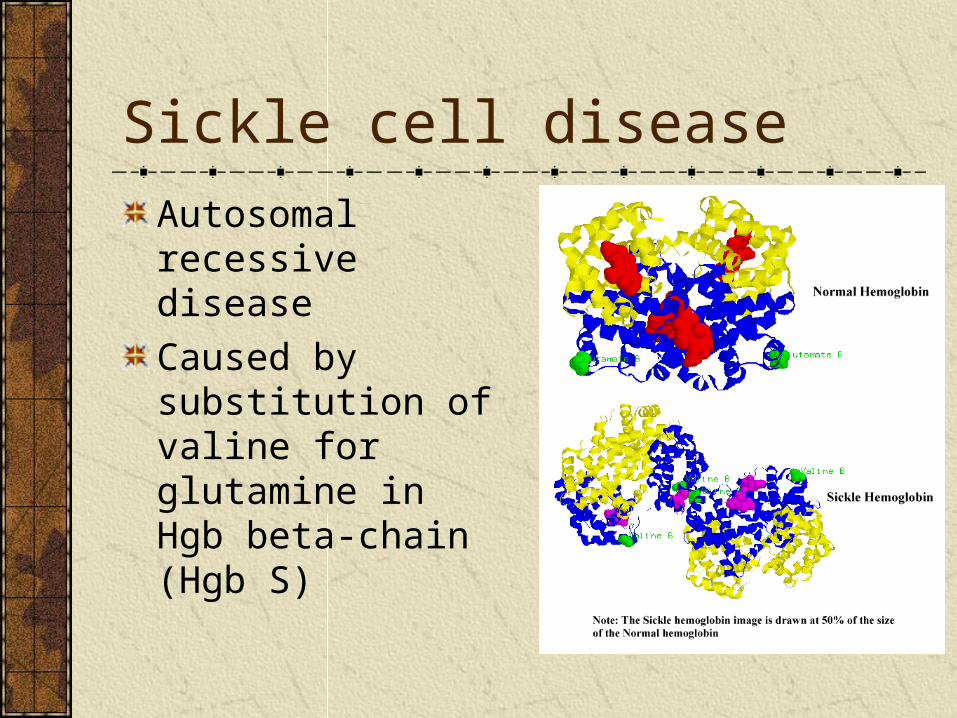
Sickle cell disease
Autosomal recessive disease
Caused by substitution of valine for glutamine in Hgb beta-chain (Hgb S)
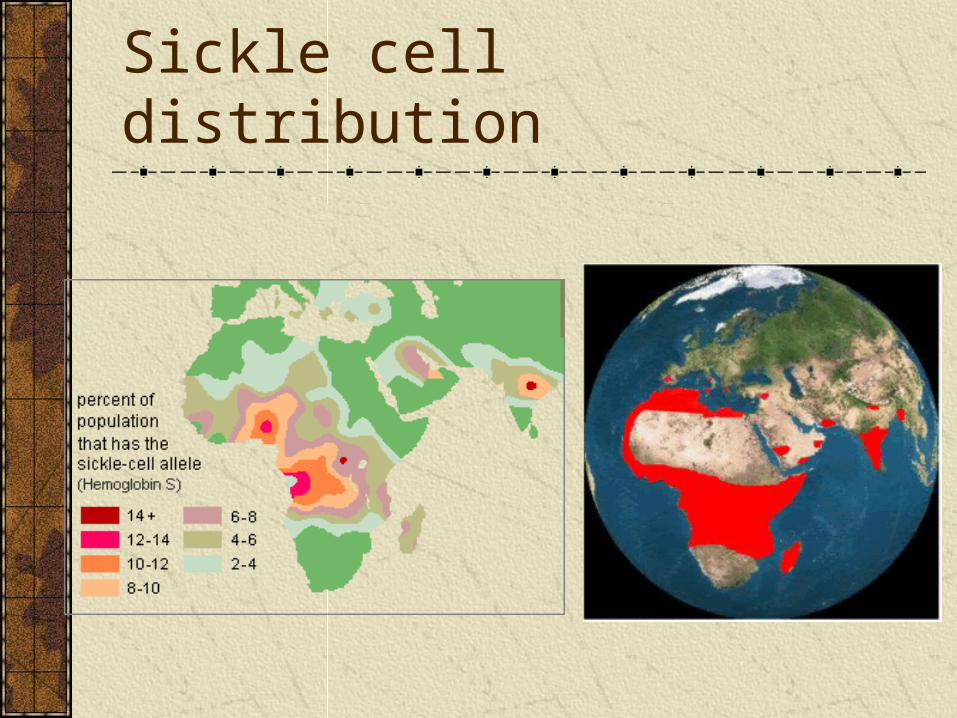
Sickle cell distribution
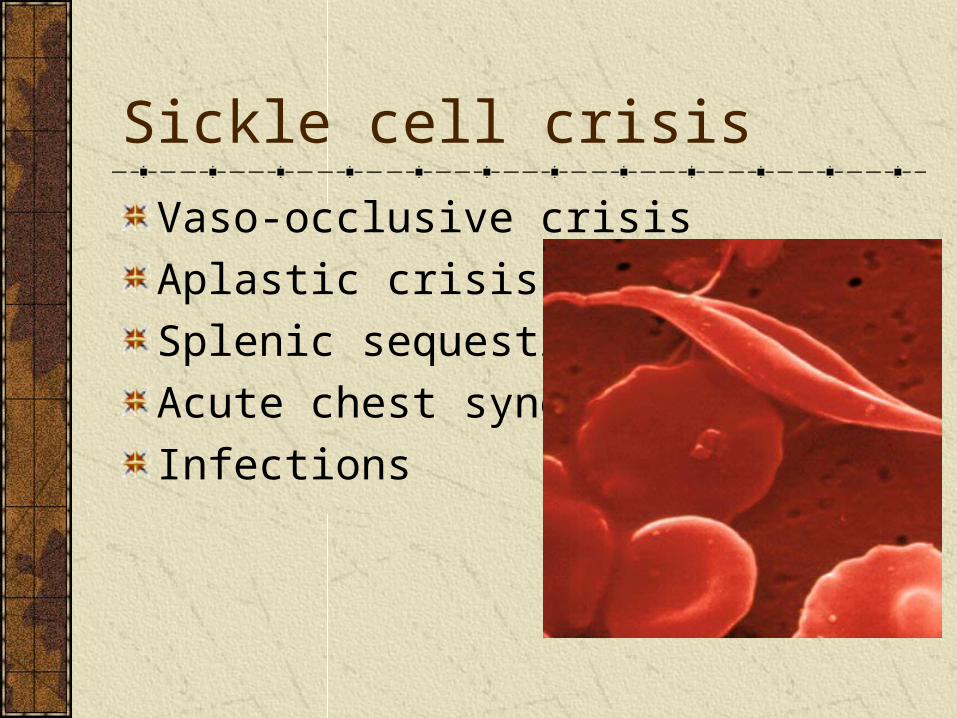
Sickle cell crisis
Vaso-occlusive crisis
Aplastic crisis
Splenic sequestration
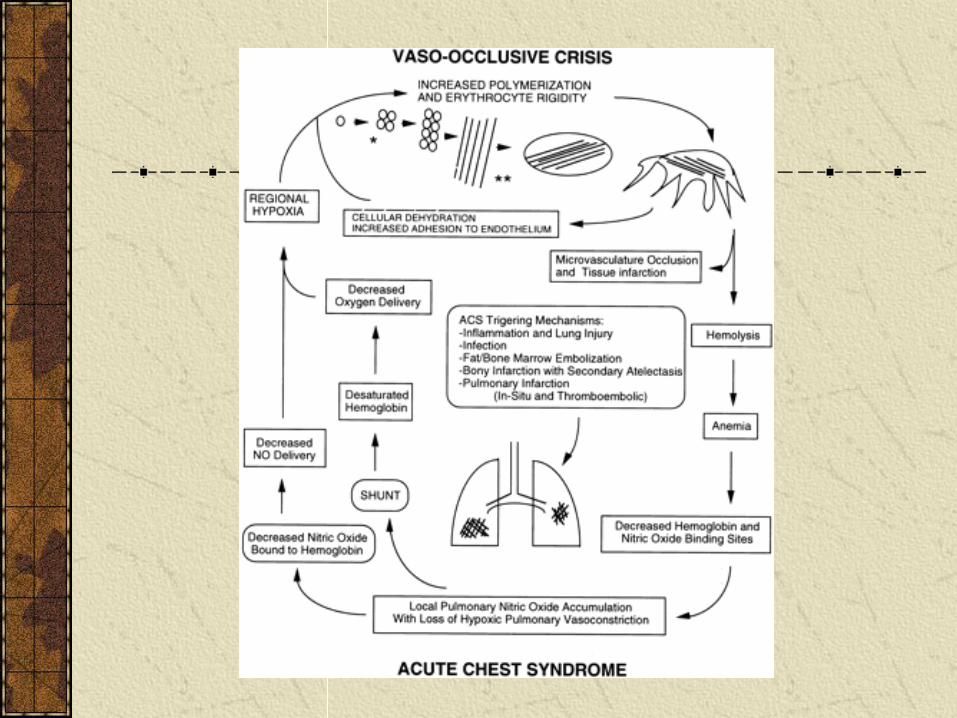
Acute chest syndrome
Infections
Case cont’d
Pt received:IV N/S 1L bolus; 2x maintenance fluids
IV morphine 5mg boluses to total of 20mg
Oxygen by n.p.
Case cont’d
Called back to see pt as noted to be ++SOB
Sats now 85% on r/a
Clinically—wheezes and crackles heard bilaterally on auscultation of lungs
Temp now 38.7C
ABG—on 8L O2: pH 7.24 /CO2 51 /O2 50; lactate 12

Any thoughts ?
Acute chest s/oDefined as:
New infiltrate on CXRAssociated with new symptoms (fever, cough, sputum production, dyspnea, hypoxia)
Occurs in 50% of SCD pts; recurrent in 80%Preceded by vaso-occlusive crisis in half of patientsLeading cause of death for pts with SCD
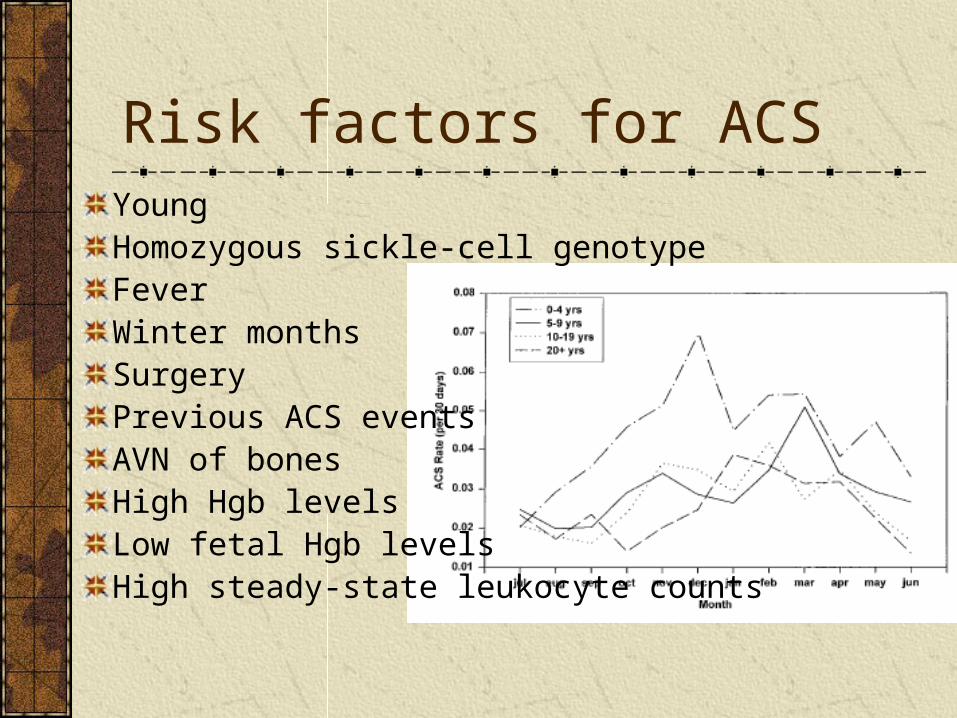
Risk factors for ACSYoungHomozygous sickle-cell genotype FeverWinter monthsSurgeryPrevious ACS eventsAVN of bonesHigh Hgb levelsLow fetal Hgb levelsHigh steady-state leukocyte counts
Pathophysiology
Infection
Fat embolism
Thromboembolism
Vaso-occlusive sickling erythrocytes
Hypoventilation due to rib/sternal infarction and pain
Hypoventilation due to narcotic administration
Pulmonary edema due to fluid overload
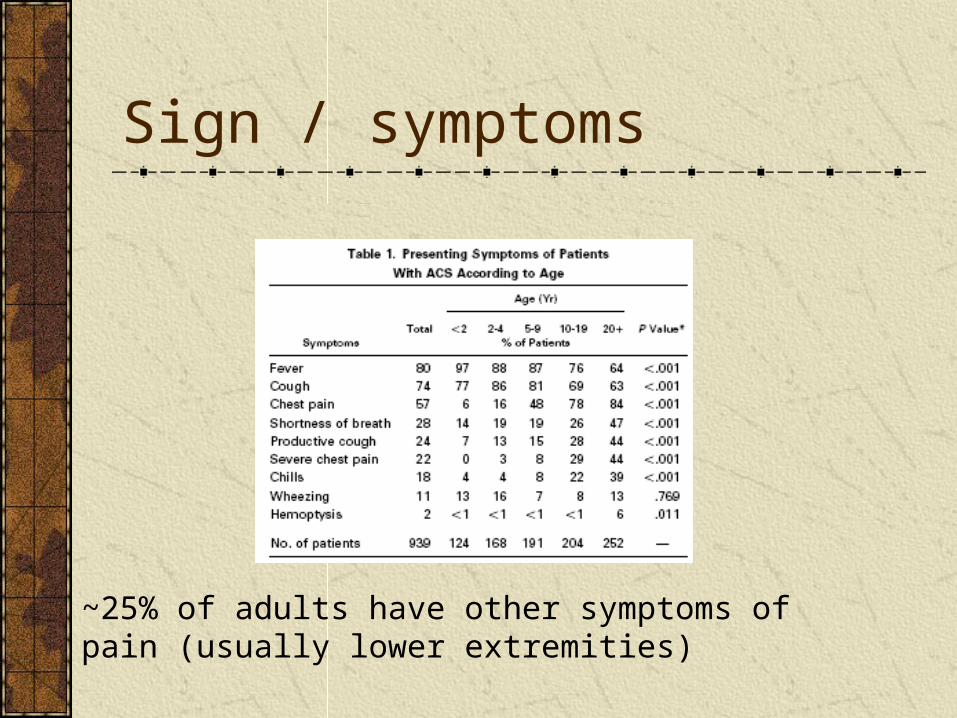
Sign / symptoms
~25% of adults have other symptoms of pain (usually lower extremities)
Mgmt
Identify and treat precipitating factors
Maintain/improve oxygenation
Prevent further alveolar collapse
Maintain adequate fluid volume
Control pain
Treat underlying infection
Oxygenation
Administer O2 to keep PaO2 ~70-100
Pts may require simple, or exchange transfusions (allow removal of Hgb S) if severe anemia
Incentive spirometry, CPAP, or intubation/ mechanical ventilation with PEEP
Indications for exchange tx
Evidence of rapid clinical deterioration
SaO2 <80% despite aggressive ventilatory support
Serial decline in SaO2
Worsening/unstable vital signs
Persistent RR >30/min
Maintain fluid volume Replenish dehydration with N/S
For further fluid volume, use D5W/0.25N/SHypotonic fluids preferred as allows water to enter RBC
Causes osmotic swelling and reduced tendency for sickling
Treat underlying infection
2nd-3rd gen cephalosporin +/- macrolideBacteremia in ~3.5% of cases of ACS
Strep pneumoniaeH. fluStaph aureusSalmonellaEnterobacterClostridia
Other therapies
DBRCT of IV dex in peds (n=43) showed SS shorter hosp stays, dec blood transfusions, dec clinical deterioration
Multiple case reports and animal studies of nitric oxide improving pt symptoms (lack of NO bioavailability in SCD)
Poloxamer-188 (non-ionic surfactant) may shorten duration of ACS and length of hospitalization (n=43)
Questions ?
References RosensBallas SK, et al. Safety of purified poloxamer 188 in SCD. Hemoglobin. 2004.Bernini JC, et al. Beneficial effects of IV dexamethasone in children with mild to mod severe ACS complicating SCD. Blood. 1998. Gladwin MT, et al. The ACS in SCD. Am J Resp Crit Care Med. 1999.Kararmaz, A et al. ACS in a patient with SC anemia successfully treated with erythrocytopheresis. Int J Emerg Inten Care Med. 2006.Machado RF. Nitric oxide based therapies in SCD: the evidence continues to mount. Crit Care Med. 2007.Vichinsky EP, et al. ACS in SCD: clinical presentation and course. Blood. 1997. Yale SH, et al. ACS in SCD. Postgrad Med. 2000.