14
Interim report from Clinical Model Taskforce Anders Nattestad
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 213 times |
| Download: | 0 times |
Interim report from Clinical
Model Taskforce
Anders Nattestad

• Alan Budenz• Richard Fredekind• Marc Geissberger• Alan Gluskin• Foroud Hakim• Peter Hansen• Jeff Kirk• Gene LaBarre• Nader Nadershahi• Anders Nattestad (chair)
Members of the taskforce

• Helix curriculum philosophy of integration
• Clinic model must support evidence based care and critical thinking
• Students are driving the patient’s treatment per their needs
• Our clinic model is thus not patient centered• Chair utilization is 60% at best• Groups are very large – GPA’s role is challenging
in keeping track of students work• Clinic model does not resemble private practice
Why this task force?

• Taskforce established in Summer 2009• Previous taskforce report from last year reviewed• SWOT analysis from that taskforce discussed• SWOT analysis from Fall quarter completed and
discussed• Student’s SWOT analysis from Fall reviewed • Six months of meetings in the current taskforce every
week or every other week including review of experiences from other schools
• Overall features of the model agreed in December 2009
• Implementation groups (7) established in January 2010
Process so far
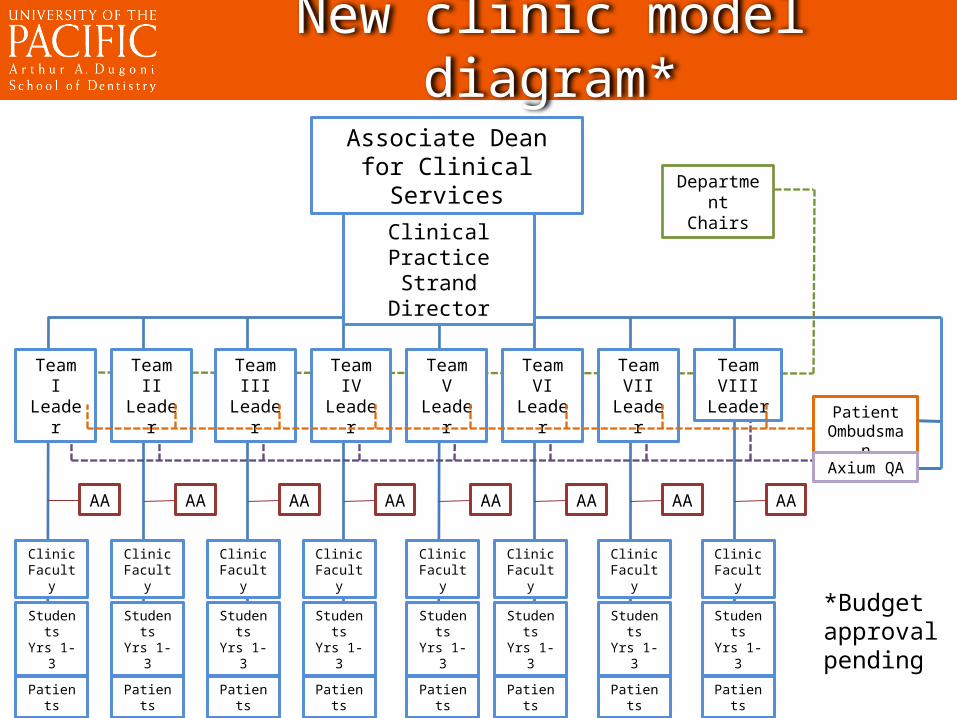
Department Chairs
AA AAAAAAAAAAAA AA
Associate Dean for Clinical Services
Clinical Practice Strand Director
Team I Leader
Team II Leader
Team III Leader
Team IV Leader
Team V Leader
Team VI Leader
Team VII Leader
Team VIII Leader
Patient Ombudsman
ClinicFaculty
Clinic Faculty
Clinic Faculty
Clinic Faculty
Clinic Faculty
ClinicFaculty
ClinicFaculty
Clinic Faculty
StudentsYrs 1-3
StudentsYrs 1-3
StudentsYrs 1-3
StudentsYrs 1-3
StudentsYrs 1-3
StudentsYrs 1-3
StudentsYrs 1-3
StudentsYrs 1-3
PatientsPatientsPatientsPatientsPatientsPatientsPatientsPatients
Axium QA
New clinic model diagram*
*Budget approval pending

Key features of new model
• Teams would perform emergency and screening along with general dental and simple endo, perio, removable, implants and oral surgery

Existing clinic model
GP MODEL
Oral Surgery
Endo
Perio
OrthoPros
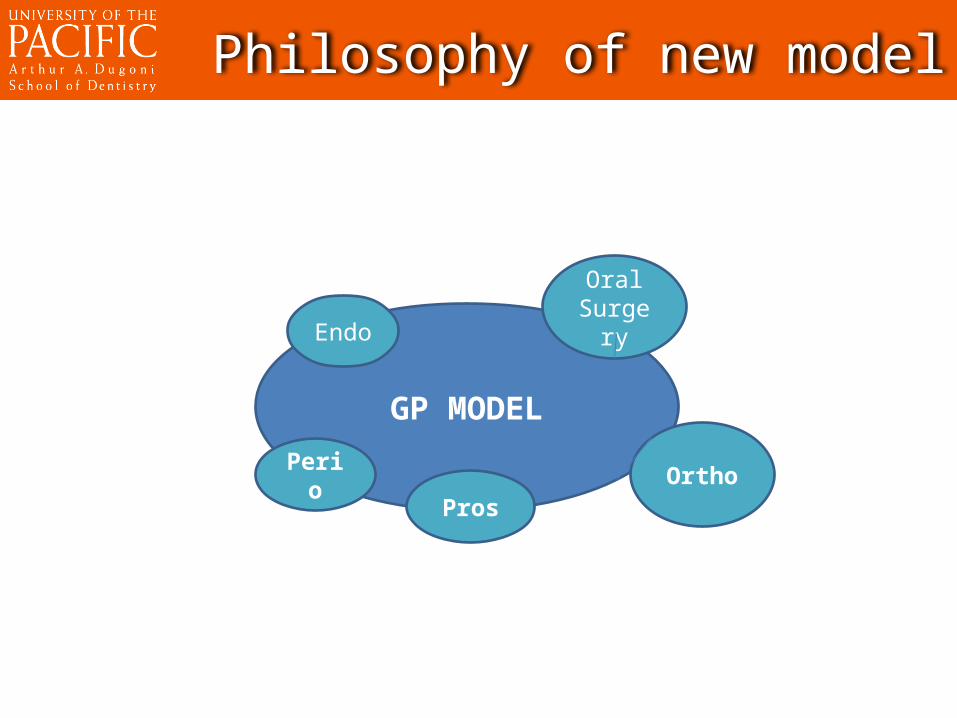
Philosophy of new model
GP MODEL
Oral SurgeryEndo
Perio OrthoPros
• Each chair will decide what can be done within the model and what needs to be referred to specialty clinics
• Each chair will decide what training is required for GP faculty before supervising “simple” specialty procedures
• GP faculty interested in supervising these “simple” specialty procedures will be approved by individual chairs of that specialty
Full general practice model
Key features of new model
• Focus on being truly patient centered comprehensive care and less driven by student’s needs by revisiting requirements and ultimately making appointments for the students

Key features of new model
• 2nd and 3rd year students to work together in teams (share patient pool, 2nd yr do simple + assist, 3rd yr teach)
• Move ICS into the Summer quarter of 2nd year• Create a patient ombudsman position• Create a faculty appointment for AxiUm + QA

• Create a faculty appointment for “Clinical Practice Strand Director” that would work on communication between teams, cross training, scheduling
• Add some faculty members• More “hands on” role of team leaders• Stronger identity of the team (colors etc.)• Faculty are responsible to team leaders during
their clinical assignments, the appropriate portion of their annual evaluation will come from their team leader
Key features of new model
• Final report of these groups due tomorrow• Last meeting of the quarter is tomorrow• Implementing begin with a few features July
2010• Implementation phased in during the year
while hiring and cross training occur• Full implementation pending funding begin
July 2011
Timeline from here

Questions?

















