European Journal of Obstetrics & Gynecology and Reproductioe Biology, 28 (1988) 213-220 Elsevier EJO 00630 Internal iliac artery ligation in post-partum hemorrhage HervC Femandez ‘, Jean-Claude Pons ‘, Guillemette Chambon ‘, RenC Frydman 1,2and Emile Papiernik I,2 I Department of Gynaecology and Obstetrics and 2 INSERM unit 187, HSpital Antoine B&l&e, 92141 Clamari, France Accepted for publication 10 January 1988 213 Between 1978 and 1986, internal iliac artery ligation was performed on eight patients undergoing treatment for severe post-partum hemorrhage, and dissemi- nated intra-vascular coagulation (DIVC) combined with causal pathology was detected in five patients. This procedure was effective in controlling bleeding in eight patients and no hysterectomy was necessary. Post-operative follow-up was uncomplicated in six patients. One patient suffered from post-operative occlusion. Another patient suffered from renal failure, due to secondary cortical renal necrosis. Surgery is usually simple and does not pose any technical problems. This technique allows for the conservation of the reproductive functions, and two of the women became pregnant at a later stage. Obstetric hysterectomy can be avoided by using this technique. It is recommended in cases where DIVC does not respond to medical treatment and can furthermore be used by all surgeons. Internal iliac artery ligation; Post-partum hemorrhage; DIVC; Conservation of reproductive function Introduction Severe post-partum hemorrhage is one of the most frequent causes of morbidity and obstetric maternal mortality. Emergency obstetric hysterectomy was the sole long-standing therapeutic method for saving the mother’s life. The fact that it causes great damage has led to research into therapeutic procedures in order to preserve the patient’s reproductive functions. Since the first unilateral hypogastric artery Correspondence: Hew? Femandez, Department of Gynaecology and Obstetrics, HBpital Antoine B&&e, 921’41 Clamart, France. 0028-2243/88/$03.50 0 1988 Elsevier Science Publishers B.V. (Biomedical Division)
Transcript
European Journal of Obstetrics & Gynecology and Reproductioe Biology, 28 (1988) 213-220
Elsevier
EJO 00630
Internal iliac artery ligation in post-partum hemorrhage
I Department of Gynaecology and Obstetrics and 2 INSERM unit 187, HSpital Antoine B&l&e, 92141 Clamari, France
Accepted for publication 10 January 1988
213
Between 1978 and 1986, internal iliac artery ligation was performed on eight patients undergoing treatment for severe post-partum hemorrhage, and dissemi- nated intra-vascular coagulation (DIVC) combined with causal pathology was detected in five patients. This procedure was effective in controlling bleeding in
eight patients and no hysterectomy was necessary. Post-operative follow-up was uncomplicated in six patients. One patient suffered from post-operative occlusion. Another patient suffered from renal failure, due to secondary cortical renal necrosis.
Surgery is usually simple and does not pose any technical problems. This technique allows for the conservation of the reproductive functions, and two of the women became pregnant at a later stage. Obstetric hysterectomy can be avoided by using this technique. It is recommended in cases where DIVC does not respond to medical treatment and can furthermore be used by all surgeons.
Internal iliac artery ligation; Post-partum hemorrhage; DIVC; Conservation of reproductive function
Introduction
Severe post-partum hemorrhage is one of the most frequent causes of morbidity and obstetric maternal mortality. Emergency obstetric hysterectomy was the sole
long-standing therapeutic method for saving the mother’s life. The fact that it causes great damage has led to research into therapeutic procedures in order to preserve the patient’s reproductive functions. Since the first unilateral hypogastric artery
Correspondence: Hew? Femandez, Department of Gynaecology and Obstetrics, HBpital Antoine B&&e, 921’41 Clamart, France.
ligation for a gluteal aneurysm in 1812 [l] and since 1960, when the first ligation of internal iliac artery was recommended in obstetrics by Sagarra [2], embolization of arteries and the use of prostaglandins has increased the possibility of preserving the reproductive functions.
The mechanisms of action, the technique and the complications noted in each case were studied in order to determine the role of ligation of the internal iliac artery for control of obstetric hemorrhage.
Subjects and methods
All cases of internal iliac artery ligation in patients with severe post-partum hemorrhage between 01.01.1978 and 30.09.1986 at hapital Antoine B&cl&e at Clamart (92141 France) have been reviewed. Post-abortum hemorrhages have been excluded.
The patient’s age, parity, term, birth method, time before ligation of arteries was performed, the infant’s health, medical, pre- and post-operative treatment and duration of hospitalization were recorded. The etiology of post-partum hemorrhage was determined from the patient’s clinical background and biological condition. Follow-up of patients made it possible to study complications, scars and the conservation of their reproductive functions.
All patients underwent bilateral ligation of the arteries through the transperi- toneum with direct access to the internal iliac artery. Using this method, we were also able to assess the accompanying uterine lesions. Simple ligature was performed on seven patients. In two cases linum was used. Polyglycolic acid (Ercedex) was used in two cases and polyglactin in three. A ligature lined with polyglactin was performed on one patient. All procedures were performed by a senior obstetrician.
Results
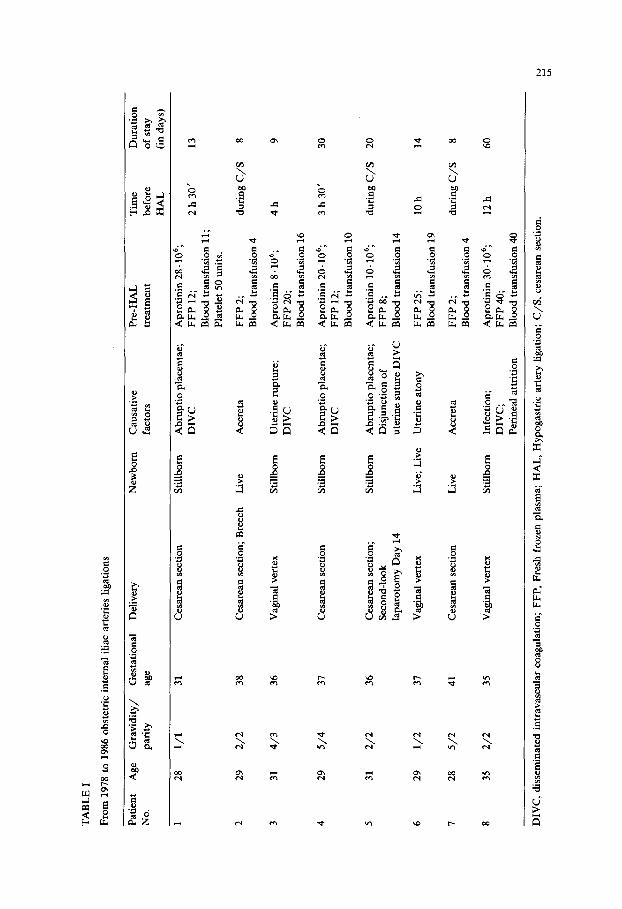
During the study period, eight patients underwent bilateral hypogastric artery ligation for the control of intractable obstetric hemorrhage. The patients and their clinical and biological characteristics are detailed in Table I. In the period ex- amined, 18 492 births occurred.
The frequency of hypogastric artery ligation was 4 per 10000 births. Cesarians were performed in five of eight cases. The other three births were vaginal. Since 1978, five obstetric hysterectomies have been performed. Indications included uterine rupture (three) and placenta accreta (two).
Arterial ligation was indicated during cesarean section in four cases. In one case, ligation was indicated after second-look laparotomy, fourteen days after cesarean section. In the cases of vaginal delivery, this procedure was undertaken after conservative measures for control of the hemorrhage had proved unsuccessful. Such procedures included manual exploration of the uterus, manual uterine massage and pharmacological control with intravenous oxytocin, intramuscular methyl ergono- vine and, in some cases, prostaglandins.
The etiology of the hemorrhages is detailed in Table II. In 5 cases DIVC was detected. Placenta accreta was detected in two patients. This was later confirmed by
TA
BL
E
I
From
19
78
to 1
986
obst
etri
c in
tern
al i
liac
art
erie
s Ii
gati
ons
Pat
ien
t A
ge
Gra
vid
ity/
G
esta
tion
al
Del
iver
y N
o.
Pam
Y
age
New
bor
n
Cau
sati
ve
Pre
-HA
L
Tim
e D
ura
tion
fact
ors
trea
tmen
t b
efor
e of
sta
y
HA
L
(in
day
s)
1 28
l/l
4 29
5/
4 37
C
esar
ean
sec
tion
S
till
bor
n
5 31
2/
2 36
29
31
29
28
35
31
Ces
area
n s
ecti
on
Sti
llb
orn
2/2
4/3
l/2
5/2
2/2
38
Ces
area
n s
ecti
on;
Bre
ech
L
ive
Acc
reta
36
Vag
inal
ver
tex
Sti
llb
orn
U
teri
ne
rup
ture
; D
IVC
37
41
35
Ces
area
n s
ecti
on;
Sec
ond
-loo
k
lap
arot
omy
Day
14
Vag
inal
ver
tex
Ces
area
n s
ecti
on
Vag
inal
ver
tex
Sti
llb
orn
Liv
e; L
ive
Liv
e
Sti
llb
orn
Ab
rup
tio
pla
cen
tae;
D
IVC
Ab
mp
tio
pla
cen
tae;
D
IVC
Ab
mp
tio
pla
cen
tae;
D
isju
nct
ion
of
ute
rin
e su
ture
DIV
C
Ute
rin
e at
ony
Acc
reta
Infe
ctio
n;
Ap
roti
nin
30
. 10
6;
DIV
C;
FFP
40
;
Per
inea
l at
trit
ion
B
lood
tra
nsf
usi
on 4
0
Ap
roti
nin
28
.106
; FF
P
12;
Blo
od t
ran
sfu
sion
11
;
Pla
tele
t 50
un
its.
FFP
2;
Blo
od t
ran
sfu
sion
4
Ap
roti
nin
8.
106;
FF
P
20;
Blo
od t
ran
sfu
sion
16
Ap
roti
nin
20
.106
; FF
P
12;
Blo
od t
ran
sfu
sion
10
Ap
roti
nin
10
.106
; FF
P
8;
Blo
od t
ran
sfu
sion
14
FFP
25
; B
lood
tra
nsf
usi
on 1
9
FFP
2;
Blo
od
tran
sfu
sion
4
2h30
’
du
rin
g C
/S
4h
3h30
’
du
rin
g C
/S
10 h
du
rin
g C
/S
12 h
13 8 9
30
20
14 8
60
DIV
C,
dis
sem
inat
ed i
ntr
avas
cula
r co
agu
lati
on;
FFP
, Fr
esh
fr
ozen
pla
sma;
H
AL
, H
ypog
astr
ic
arte
ry
liga
tion
; C
/S,
cesa
rean
se
ctio
n.
216
TABLE II
Indication for internal iliac artery ligation
Indication Number DIVC
of associated
patients
Placenta accreta 2 0
Abruptio placentae 2 2
Uterine rupture 1 1
Uterine atony 1 0
Disjunction of uterine suture 1 1
Perineal attrition 1 1
Total 8 5
DIVC, disseminated intravascular coagulation.
pathological examination. Four of 9 children were alive at birth and are today in good health. The five others died in utero. The average duration of hospitalization was 20 days (extremes: 8 and 60 days). In all cases hypogastric artery ligation was effective in controlling bleeding and secondary hysterectomy was not required. Follow-up was uncomplicated in 6 of 8 cases. Coagulation was checked on a daily basis until the return to normal. Two patients suffered from post-operative compli- cations. Embolectomy, using a vena cava clip, was necessary in case 4, due to acute intestinal occlusion on the eighth day after surgery, complicated four days later by ilio-femoral thrombosis. Thrombo-embolic alteration occurred while the patient was undergoing intravenous heparin treatment, using doses normally allowing coagula- tion. Secondary anti-thrombin III insufficiency was not detected. One patient (case 8) suffered from renal failure, due to secondary cortical necrosis as a result of shock brought on by the initial hemorrhage. She is currently following a kidney transplant programme and undergoes dialysis three times a week. However, this complication was not due to arterial ligation but to causal pathology. Eighteen months after undergoing arterial ligation, two patients have become pregnant. One (case 1) gave birth at full term to a baby weighing 3000 g. An abortion was performed on the other in the tenth week of amenorrhea.
Four patients (cases 5 to 8) received treatment less than a year ago and it has not yet been determined whether their reproductive functions have been preserved.
Discussion
The physiological characteristics and hemodynamics of hypogastric artery liga- tion have been described in Burchell’s seminal publications [3,4]. In 1964, he measured the systolic and diasystolic pressure of the uterine artery and of the distal segment of the hypogastric artery before and after ipsilateral, controlateral and bilateral ligation in the proximal segment of the hypogastric artery. When homo- lateral ligation is applied, the pressure of the systolic surge is reduced by 7791, average pressure by 22% and flow by 22%.
217
In cases of controlateral ligation, systolic surge is reduced by 14% and average pressure by 10%. When bilateral ligation is applied, the drop in pressure of the systolic surge is 85%, with a drop in average pressure of 24% and flow is reduced by 48%. These first studies describe the existence of a retrograde revascularization, where the pelvic arterial system becomes venous, due to the fact that systolic surge disappears when average pressure drops. Bilateral ligation is slightly more effective than homolateral ligation. These phenomena allow for the development, by com- pression, of plate thrombus, which is durable without intervening locally.
In 1966, Burchell and Olson [4] published the results of a study, where aortogra- phy was performed after ligation of the hypogastric arteries. The existence of an immediately functional replacement system and sufficient pressure through three specific collateral arteries, lumbar-iliolumbar, middle sacral-lateral sacral, and superior hemorrhoidal-middle hemorrhoidal arteries, explains the absence of ischemia and tissue necrosis. Arterial repermeabilization was not observed in this study, but non-resorbable thread was used.
Since the mechanism of action of arterial ligation was first described, several medical teams have reported using the technique as an alternative to obstetric
hysterectomy, in treating severe post-partumhemorrhage [5-lo]. Thus, the impor- tance of reconsidering the use of obstetric hysterectomy and its application as some authors [9,11,12] recommend for corporal uterine ruptures and for accreta and percreta placenta is apparent. We have discouraged the use of this technique for uterine rupture and accreta placenta and only five obstetric hysterectomies have been performed since 1978 for these reasons with older patients with parity above
three. In our series, the main causative factors of obstetric hemorrhage were detected,
and disseminated intra-vascular coagulation (DIVC) is one such cause of post-partum hemorrhage [13]. We detected it in five of the eight cases. In medical treatment of
DIVC, fresh frozen plasma, blood and aprotinin (Iniprol) transfusions are used to treat the fibrinolytic constituents of DIVC. This treatment is combined with bilateral ligation of the hypogastric arteries in the case of failure of other treatments or resuscitation complications.
Therefore even if the technique involving arterial ligation put forward by Burchell [3] requires normal coagulation, bilateral ligation of the hypogastric arteries must be possible for use in therapy in the case of major hemostatic problems or if medical treatment fails. Despite the theoretical risks; no technical difficulties arose and no post-operative morbidity occurred in connection with surgery in patients with DIVC. In patients with severe post-partum bleeding without DIVC, ligation of the hypogastric arteries is the optimal method for conserving reproductive functions.
In 1961, Reich and Nechten [14] described a case of pregnancy after ligation of the hypogastric arteries. Since then other authors have described similar cases [5,6,15]. Cesareans have since shown the continued presence of the ligation when non-dissolvable suture was used and repermeability of the hypogastric artery was restored, with the use of dissolvable material.
In our series, two pregnancies in two women were possible. Neither fetal hypotrophy nor toxemia occurred in the patients in our program or in other cases of pregnancies after ligation already published, although these two types of complica-
218
tion can potentially arise during pregnancy following ligation of the arteries. This technique’s major advantage is therefore that it allows the conservation of the patient’s reproductive function. Other forms of ‘conservative’ therapy have been suggested as alternatives to obstetric hysterectomy and ligation of the hypogastric arteries in patients with severe post-partum hemorrhage. However, these kinds of procedure are often used for different reasons.
Ligation of the uterine arteries, often combined with ligation of the round ligament and/or the ovarian arteries, has also been recommended with a view to a greater reduction of the uterine flow [16]. The indication for this is, however, more limited, since it cannot be applied in the case of hemorrhages from the lower segment, which are dependent on the cervico-vaginal or vaginal arteries, branches of the hypogastric arteries.
In the case of an enlarged hematoma of the broad ligament accompanied by perineal laceration, hypogastric ligation is recommended since it permits a less selective examination of vascular abrasion, particularly of the internal pudendal artery, which is often affected. Furthermore, a surgical approach to the area vascularized by the internal pudendal when distended by a hematoma can be the cause of ureteral lesions which, together with ischemias, create complications involved in the ligation of arteries.
Nevertheless, alternatives to surgery in the treatment of obstetric hemorrhages do exist. Selective [17] or hyperselective [18] embolization of the hypogastric arteries has been recommended as an alternative to surgical ligature. It can be selected either immediately before any other treatment or as a last resort. In all cases, embolization has the advantage of being better tolerated, since local anesthesia is used. It is also more precise because it is applied locally at the site of the hemorrhage.
The duration of hospitalization can be reduced and post-operative complications avoided by successful embolization, which seals off the hemorrhage area. However, embolization does give rise to complications peculiar to this type of infection or to extensive hematoma at the site of the puncture, particularly in the case of DIVC combined with arterial thrombosis, arteriovenous fistula or ischemia in the case of massive embolization. A vascular radiologist is therefore necessary, since stable hemodynamic conditions are needed to perform, without undue haste, embolization or transfer towards the reference center.
Furthermore, in the case of an associated lesion and/or uterine rupture, emboli- zation allows a precise assessment of the vascular lesions but an associated uterine lesion may go undetected in the diagnosis. Lastly, embolization is indicated only in the case of a hemorrhage not occurring during necessary surgery. Thus, this precludes embolization in 6 of 8 cases in our series, due to four indications arising during cesareans and two cases of uterine rupture and disjunction in the uterine suture. In two cases, embolization could have been performed, but in one case the hemodynamic conditions made any transfer or vascular manoeuvres impossible. In the other case, no radiological reference service was available. Thus, embolization is indicated after delivery with hemorrhage in patients free of organic lesions, after having exhausted alternative resuscitation techniques and thus, essentially in cases of uterine atony and perineal alterations [19], after elimination of associated uterine rupture.
219
Compared to embolism, ligation of the internal iliac arteries, though less attrac- tive technically, has the advantage of emergency use, regardless of hemodynamic conditions or coagulation, and can be performed by all gynecological surgeons.
Lastly, in the particular case of uterine atony, certain authors [20-231 recommend the use of the ocytocic action of prostaglandins Fza or synthetic equivalents, intramurally or intramuscularly [24]. This treatment is an alternative to surgery even in the case of DIVC [25] and does not complicate secondary surgical treatment if it
proves ineffective.
Conclusion
Our study involves eight cases of ligation of the internal iliac arteries and discusses indications for other therapeutic methods in the case of severe post-partum hemorrhage. The indications for obstetric hysterectomy are uterine rupture, placenta accreta and the age of the mother. Prostaglandins are indicated in uterine atony, embolization in hemorrhage after natural delivery with no associated organic lesion and no diagnostic uncertainty, in stable hemodynamic conditions. Internal iliac
artery ligation in severe post-partum hemorrhage should be performed during surgery, regardless of hemodynamic conditions, if doubt exists as to the presence of associated lesions and when DIVC does not respond to medical treatment. Ligation can thus be performed in all surgical facilities. In our department, it obviated reproductive alterations, since two pregnancies were able to be begun thanks to this
choice of therapy.
References
1 Tajes RV. Ligation of the hypogastric arteries and its complications in resection of cancer of the
rectum. Am J Gastroenterol 1956;26:612-615.
2 Sagarra M, Glasser ST, Stone ML. Ligation of the internal iliac vessels in the control of post partum
4 Burchell RC, Olson G. Internal iliac artery ligation: aortograms. Am J Obstet Gynecol
1966;94:117-124.
5 Shinagawa S. Extra peritoneal ligation of the internal iliac arteries as a life-saving procedure for
incontrollable post partum hemorrhage. Am J Obstet Gynecol 1964;88:130-131.
6 Lecocq F. Internal iliac artery ligation. Am J Obstet Gynecol 1966;95:320-326.
7 Sack RA Bilateral internal iliac artery ligation to control obstetric and gynecologic hemorrhage. Am
J Obstet Gynecol 1973;16:493-497.
8 Dubay ML, Holshauser CA, Burchell, RC. Internal iliac artery ligation for post partum hemorrhage:
recanalization of vessels. Am J. Obstet Gynecol 1980;135:689-691.
9 Clark SL, Phelan JP, Yeh SY, Bruce SR, Paul RH. Hypogastric artery ligation for obstetric
hemorrhage. Obstet Gynecol 1985;66; 353-356.
10 Evans S, MacShane P. The efficacy of internal iliac artery ligation in obstetric hemorrhage. Surg
Gynecol Obstet 1985;160:250-253.
11 Thonet RGN. Obstetric hysterectomy an 11 years experience. Br J Obstet Gynaecol 1986;93:794-798.
12 Sturdee DW, Rushton DI. Caesarean and post partum hysterectomy 1968-1983. Br J Obstet
Gynaecol 1986;93:270-274.
13 D.H.S.S. Report on confidential enquiries into maternal deaths in England and Wales 1976-1978. Report on health and social subjects 26. Her Majesty’s Stationery Office, London: 1982.
220
14 Reich WJ, Nechton MJ. Ligation of the internal iliac arteries: a life-saving procedure for uncontrolla-
ble gynecologic and obstetric hemorrhage. J Intern Corr Surg 1961;36:157-158.
15 Mengert WF, Burchell RC, Blumstein RW, Daskal JL. Pregnancy after bilateral ligation of the
internal iliac and ovarian arteries. Obstet Gynecol 1969;34:664-666.
16 O’Leary JL. Uterine artery ligation for control of post cesarean section hemorrhage. Obstet Gynecol
1974;43:849-851.
17 Pais SO, Glickman M, Schwarts P, Pingoud E, Berkowitz R. Embolization of pelvic arteries for
control of post partum hemorrhage. Obstet Gynecol 1980;55:754-758.
18 Brown BJ, Heaston DK, Poulson AM, et al. Uncontrollable post partum bleeding: a new approach to
hemostasis through angiographic arterial embolization. Obstet Gynecol 1979;54:361-365.
19 Smith DC, Wyatt JF. Embolization of the hypogastric arteries in the control of massive vaginal
hemorrhage. Obstet Gynecol 1977;49:317-323.
20 Bygdeman M, Kwon SU, Mukherjee T. Effect of intravenous infusion of prostaglandins Et, E, on
motility of the pregnant human uterus. Am J. Obstet Gynecol 1965;102:317-319.
21 Embrey MP. Effect of prostaglandins on human uterus in pregnancy. J Reprod Fertil1970;23:372-376.
22 Corson SL, Bolognese RJ. Post-partum uterine atony treated with prostaglandins. Am J Obstet
Gynecol 1977;129:918-919.
23 Takagi S, Yoshida T, Togo Y, et al. The effects of intramyometrial injection of prostaglandin Faa on
severe post partum hemorrhage. Prostaglandins 1976;12:565-567.
24 Hayashi RH, Castillo MS, Noah ML. Management of severe post partum hemorrhage due to uterine
atony using an analogue of prostaglandin Fz,. Obstet Gynecol 1981;58:426-429.
25 Jacobs MM, Arias F. Intra-myometrial prostaglandin Fzu in the treatment of severe post partum