Page 1
1
International Council of Ophthalmology
HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS
LEARNING EMERGENCY OPHTHALMOLOGY
Compiled by The Task Force on Undergraduate Teaching in Ophthalmology of the International Council of
Ophthalmology and based on their curriculum 2009
Page 2
2
Inthisbookletwehaveputtogethercommonophthalmicemergency
conditionsthatwethinkyouneedtoknowandkeyophthalmic
disorderswethinkyouneedtohaveseen.Therearedescriptionsand
colourpicturesoftheseconditions.Thispocketsizedbooksummaries
thekeypointsintheophthalmologycurriculumcompliedbytheTask
ForceoftheInternationalCouncilofOphthalmologyandisaformat
thatisveryportable!
SueLightman,DoNhuHonandPeterMcCluskey
OnbehalfoftheInternationalCouncilofOphthalmologyandVietnam
NationalInstituteofOphthalmology,HanoiMedicalUniversity2010
OtherContributingAuthorswiththanks
AnhDinhKim,AnhNguyenQuoc,ChauHoangThiMinh,DongPhamNgoc,HaTran
Minh,HonDoNhu,NgocDoQuang,QuanBuiDao,RichardAndrews,ThangNguyen
Canh,ThanhPhamThiKim,ThuyNguyenThiThu,ThuyVuThiBich,TungMaiQuoc,
VanPhamThiKhanh, VanPhamTrong,YenNguyenThu,SimonTaylor
Page 3
Haveyouseen? Tickifyes
Doyouknowhowitiscausedandtreated?
Tickifyes
Noteforyou:Remembertolookitup
Trauma
Periorbitalhaematoma
Orbitalblowout
Lidlaceration
Subconjunctival
Haemorrhage
Chemicalburns–cornea
andconjunctiva
Foreignbody
Cornealabrasion
Hyphema
Iridodialysis
Cataract
Lenssubluxation/dislocation
Intraocularforeignbody
Scleralrupture
3
Page 4
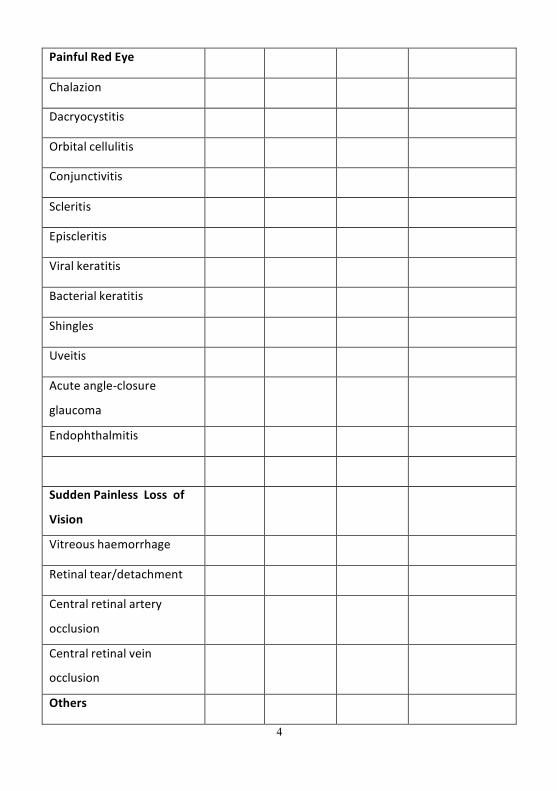
PainfulRedEye
Chalazion
Dacryocystitis
Orbitalcellulitis
Conjunctivitis
Scleritis
Episcleritis
Viralkeratitis
Bacterialkeratitis
Shingles
Uveitis
Acuteangle-closure
glaucoma
Endophthalmitis
SuddenPainless Loss of
Vision
Vitreoushaemorrhage
Retinaltear/detachment
Centralretinalartery
occlusion
Centralretinalvein
occlusion
Others
4
Page 5
5
Proptosis
VIInervepalsy
TRAUMA
Oculartraumaisverycommon,especiallyindevelopingcountries.Itcaninvolveanypartoftheocularsystem,includingtheeyelids,globeandvisualpathways. Allpatientswithahistoryoftraumamusthaveafullophthalmicexamination.
Periorbitalhaematoma
Page 6
6
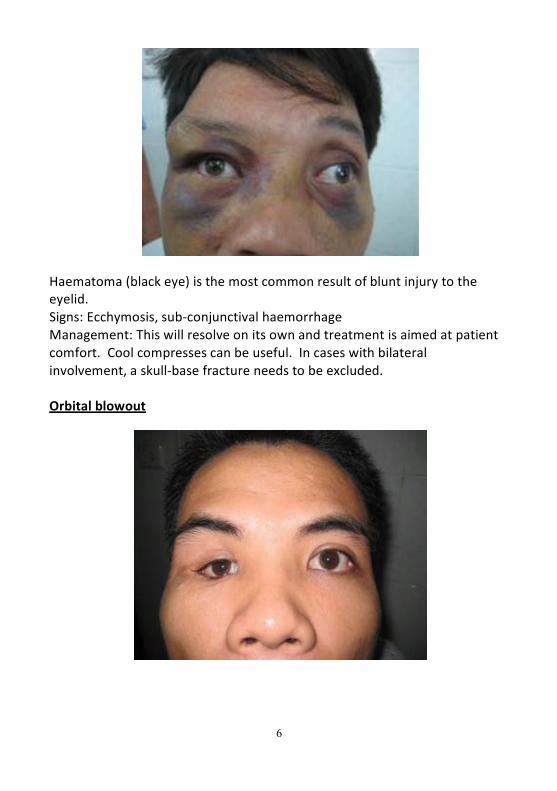
Haematoma(blackeye)isthemostcommonresultofbluntinjurytotheeyelid.Signs:Ecchymosis,sub-conjunctivalhaemorrhageManagement:Thiswillresolveonitsownandtreatmentisaimedatpatientcomfort.Coolcompressescanbeuseful. Incaseswithbilateralinvolvement,askull-basefractureneedstobeexcluded.
Orbitalblowout
Page 7
7
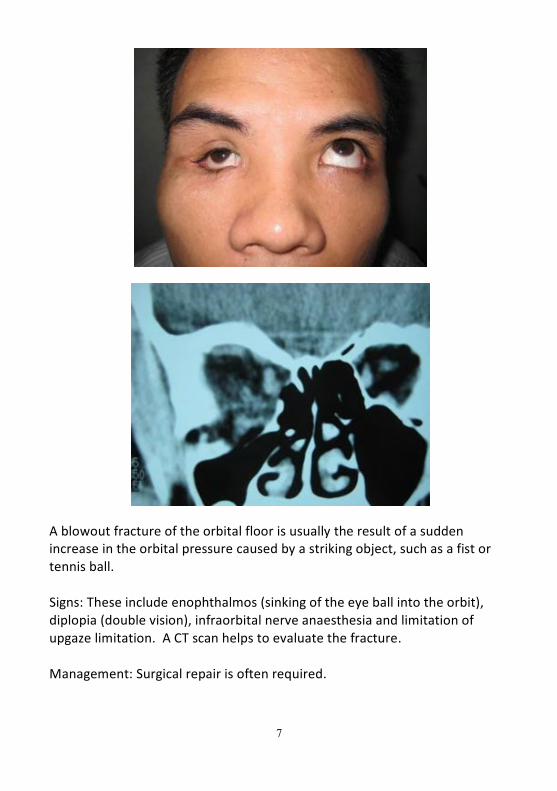
Ablowoutfractureoftheorbitalfloorisusuallytheresultofasuddenincreaseintheorbitalpressurecausedbyastrikingobject,suchasafistortennisball.
Signs:Theseincludeenophthalmos(sinkingoftheeyeballintotheorbit),diplopia(doublevision),infraorbitalnerveanaesthesiaandlimitationofupgazelimitation.ACTscanhelpstoevaluatethefracture.
Management:Surgicalrepairisoftenrequired.
Page 8
8
Lidlaceration
Lidlacerationsmustbeexploredthoroughlytoensurethelacrimalsystemisintact.Impropereyelidclosurecancauseexposurekeratopathy.
Management:minorlidlacerationsshouldberepairedbydirecthorizontalclosurewheneverpossible,inordertoarchivethebestfunctionalandcosmeticresults.Accurateappositionoftheeyelidmarginsiscritical.Majortissuelossneedsoculoplasticsurgery.Laceratedlacrimalductsshouldberepairedtomaintainnormalteardrainage.
Page 9
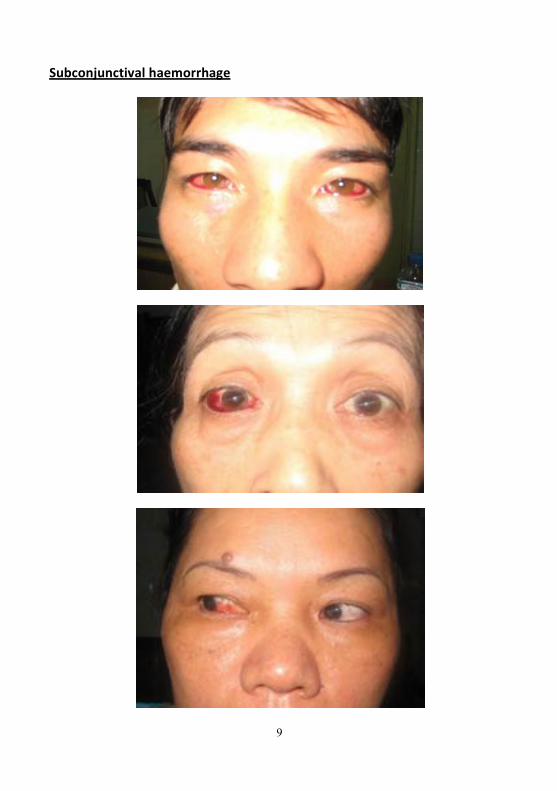
Subconjunctivalhaemorrhage
9
Page 10
ThisisBloodundertheconjunctiva,andisusuallyunilateral,localisedandsharplycircumscribed;theunderlyingscleraisoftennotvisible. Thereisnoinflammation,painordischarge,andthevisualacuityisunchanged.Sometimes,therecanbeanassociationwithminorinjuries,includingeye-rubbing,anditismorecommonwithuseofanti-plateletagentsandanticoagulants.Management:Thisismostlyreassururance,butcheckingbloodpressureandcoagulationmaybeindicated.
Chemicalburnsofcorneaandconjunctiva
Mild
Moderate
10
Page 12
12
Alkalis(bleach,cement)tendtopenetratedeeperintotheocularstructuresthanacids.Thisisanocularemergency,andtheinitialmanagementconsistsofcopiousirrigationoftheeyesundertopicalanaesthetic.Signsincludecornealhaze,limbalischaemiaandlossofepithelium.Management:Anacuteocularemergency.Immediate,prolongedandcopiousirrigationwithnormalsalineuntiltheocularpHremainsnormal.Intensivetopicalsteroids,antibioticsandLubricantsaregiven. Latermanagementmayincludelimbalstem cellgraftingforlimbalstemcellloss,butkeratoplastyorkeratoprothesis(artificalcornea)surgerymayberequiredfordensecornealscarring.
Page 13
13
SuperficialforeignBody Cornea
Page 14
14
Bulbarconjunctiva Signs:foreignbodyoncornealsurfaceorbulbarconjunctiva.Iftheforeignbodyisnotvisible,everttheeyelidstoexposeapossiblesubtarsalforeignbody.Management:topicalantibioticsafterremovaloftheforeignbody.
Cornealabrasion
Cornealepitheliumisscrapedandlostaftereyetrauma.Symptoms:sore,wateryeyewithblurredvision.Signs:redandwateryeye.Fluoresceinstaininginareawherecornealepitheliumislost.Management:topicalantibioticsandeyepadforsymptomaticrelief.
Page 15
15
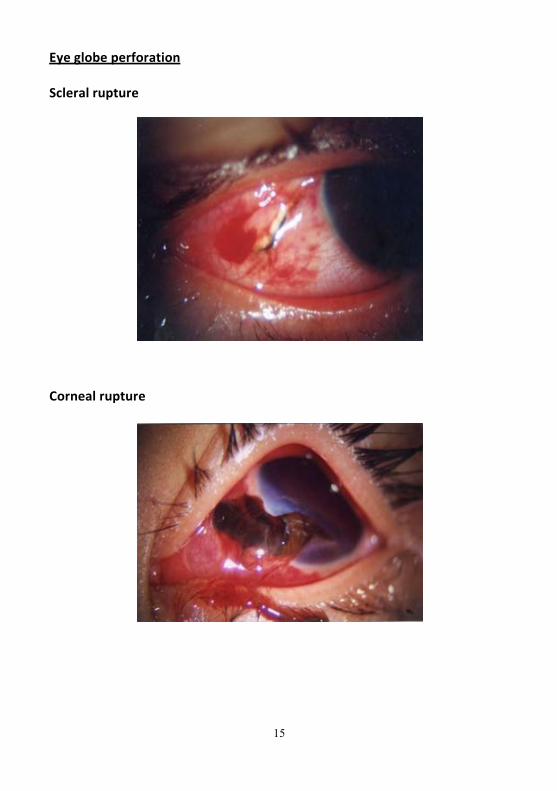
Eyeglobeperforation Scleralrupture
Cornealrupture
Page 16
16
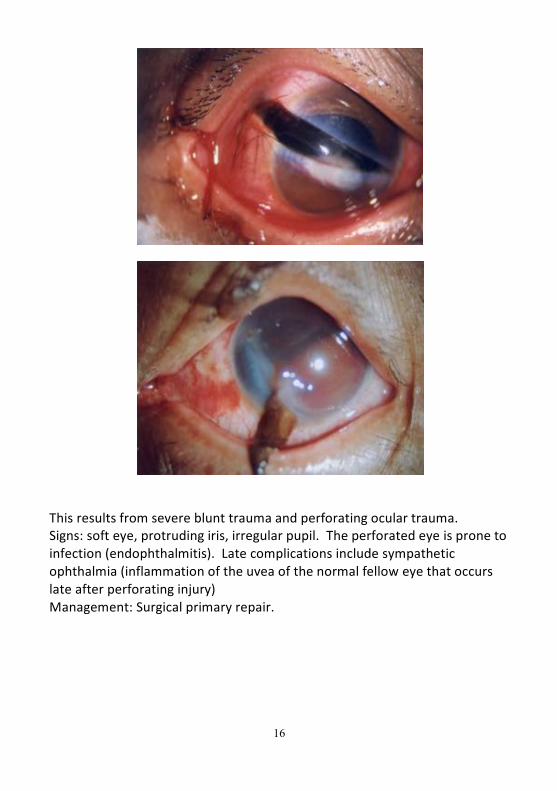
Thisresultsfromsevereblunttraumaandperforatingoculartrauma.Signs:softeye,protrudingiris,irregularpupil.Theperforatedeyeispronetoinfection(endophthalmitis). Latecomplicationsincludesympatheticophthalmia(inflammationoftheuveaofthenormalfelloweyethatoccurslateafterperforatinginjury)Management:Surgicalprimaryrepair.
Page 17
17
Hyphaema Mild
Severe
Bloodintheanteriorchamberfollowingblunttraumatotheeye.Symptoms:redeyeandseverelossofvisionfollowingtrauma.Signs:visiblebloodinanteriorchamberandcorneamayalsobestained.Eyemaybeverysoreifintraocularpressureisraised.Haematocorneacausescloudyvision.Management:BedrestAndtopicalatropinetoreducetheriskofrebleeding.Urgentassessmentbyophthalmologistisrequired,astreatmentofraisedintraocularpressureoranteriorchamberirrigationmayberequired.
Page 18
18
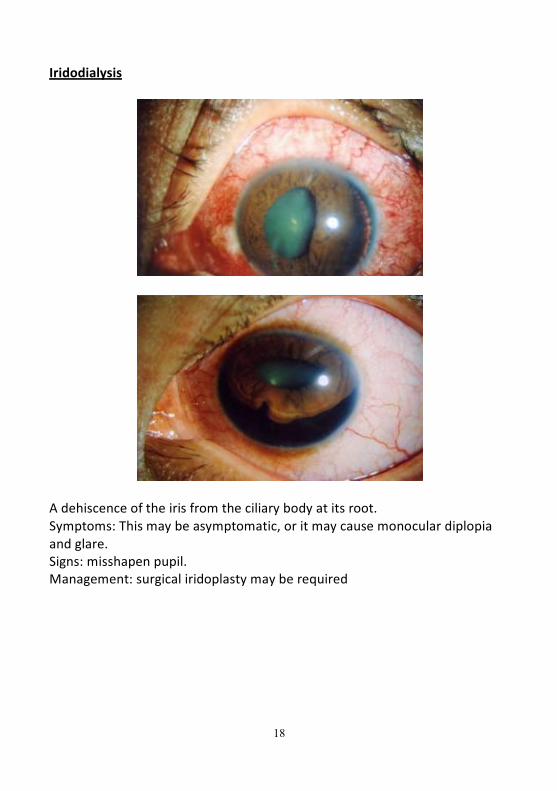
Iridodialysis
Adehiscenceoftheirisfromtheciliarybodyatitsroot.Symptoms:Thismaybeasymptomatic,oritmaycausemonoculardiplopiaandglare.Signs:misshapenpupil.Management:surgicaliridoplastymayberequired
Page 19
19
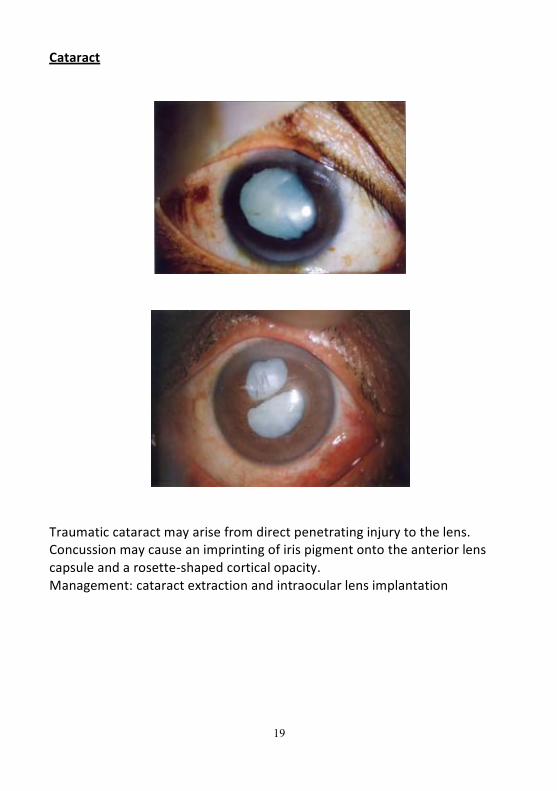
Cataract
Traumaticcataractmayarisefromdirectpenetratinginjurytothelens.Concussionmaycauseanimprintingofirispigmentontotheanteriorlenscapsuleandarosette-shapedcorticalopacity.Management:cataractextractionandintraocularlensimplantation
Page 20
20
Lenssubluxation/dislocation Lenssubluxation
Lensdislocatedintotheanteriorchamber
Lensdislocatedoutfromtheglobe
Page 21
21
Directtraumatotheeyemayresultinlenssubluxationortotaldislocation.Victimsmayexperiencereducedvision,monoculardiplopiaandintraocularhypertension.Management:lensremovalwith(usually)intraocularlensimplantation.
Intraocularforeignbody(IOFB)
Anteriorchamber
Lens
Page 22
22
Vitreous/retina
AnIOFBmaylodgeinanyoftheocularstructuresitpassesthrough,somaybelocatedanywherefromtheanteriorchamber,lenstotheretinaandchoroid.Foreignbodiesarepronetoresultininfection(endophthalmitis).Management:immediatereferraltoophthalmologistforremovalofforeignbody.
Siderosis
RetinaltoxicitycanbecausedbyanironIOFBremainingintheeyeforalongtime. Symptoms:reducedvisionSigns:dilatedpupil,rust-brownoryellowlensopacityandabolisedelectro-retinogram(ERG).Management:lateIOFBremovalmaynothelpvisualrecovery.
Page 23
23
PAINFULREDEYE Chalazion
Page 24
24
Inflammationofthemeibomianglandscauseslumpsintheeyelids.Signs:eyelidswelling,rednessandpain.Management:self-limited,topicalantibioticsandsurgicalremovalifnecessary.
Ophthalmiczoster(shingles)
ApainfulconditioncausedbyHerpeszosterinfection.Signs:whenthe1st
division(ophthalmicnerve)ofthe5th(trigeminal)cranialnerveisaffected,extremelypainful,blister-likelesionsappearontheface.Sometimes,thecornea,uveacangetinflammed.Management:anti-viraldrugsandanalgesics.
Page 25
25
Dacryocystitis
Infectionofthelacrimalsac–usuallysecondarytoobstructionofthelacrimalduct.Signs:atender,red,tenseswellingatthemedialcanthus.Maybeassociatedwithpreseptalcellulitis.Management:initialwarmcompressesandoralantibiotics.Sometimes,drainingandtearsacremovalmaybenecessary.
Page 26
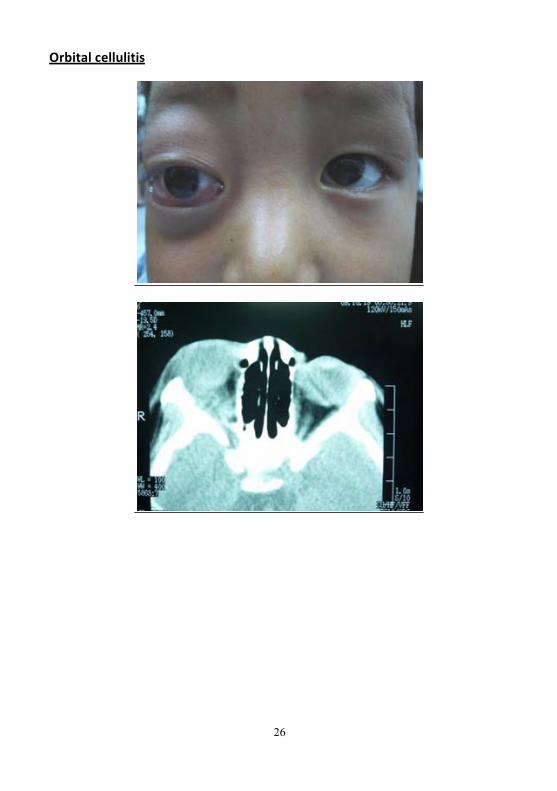
Orbitalcellulitis
26
Page 27
27
Thisisalife-threateninginfectionofthesofttissuesbehindtheorbitalseptum. Itismorecommoninchildren.Symptoms:fever,painandvisualimpairment.Signs:unilateral,tender,warmandredperiorbitallidoedema,proptosis,painfulophthalmoplegiaandopticnervedysfunction.CTscanshowsthickenedperioculartissues.Management:admissionandintravenousantibiotictherapy.
Page 28
28
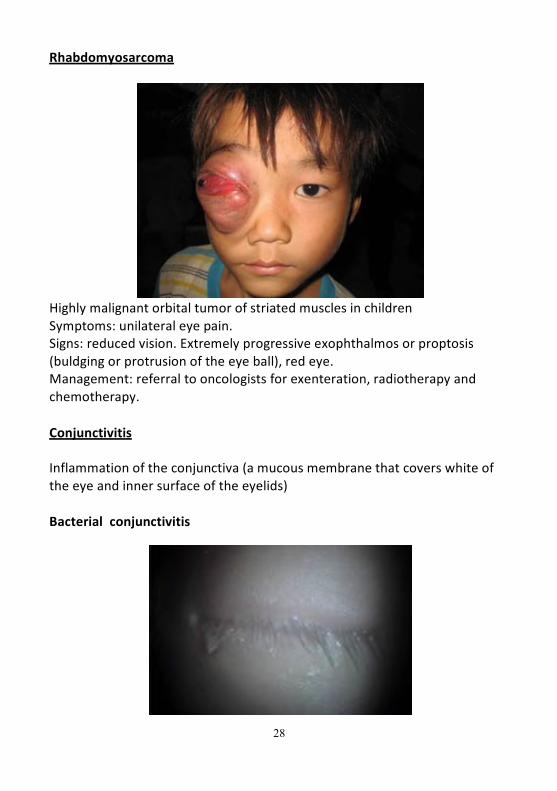
Rhabdomyosarcoma
HighlymalignantorbitaltumorofstriatedmusclesinchildrenSymptoms:unilateraleyepain.Signs:reducedvision.Extremelyprogressiveexophthalmosorproptosis(buldgingorprotrusionoftheeyeball),redeye.Management:referraltooncologistsforexenteration,radiotherapyandchemotherapy.
Conjunctivitis
Inflammationoftheconjunctiva(amucousmembranethatcoverswhiteoftheeyeandinnersurfaceoftheeyelids)
Bacterialconjunctivitis
Page 29
29
Symptoms:Redstickyeyes,usuallybilaterally.Signs:redeyeswithpurulentdischarge.Nocornealoranteriorchamberinvolvement.Systemicallywell.Management:regularhygienetominimisesecretionbuildup,topicalantibioticsfor5days.
Viralconjunctivitis
Page 30
30
Contacthistorywithrecenteyeorupperrespiratorytractinfectionsymptoms(especiallychildren).Highlycontagious.Symptoms:burningsensationandwaterydischarge(differentfrompurulentexudateinbacterialinfections).Classicallybeginsinoneeyewithrapidspreadtotheother,oftenpre-auricularlymphadenopathy.Signs:eyeredandwatery.Swollenconjunctivaparticularlyinlids.Management:willresolveonownandtreatmentaimedatcomfort.Coolcompresses,regularlubricants(withoutpreservative).Antibioticdropsifindicated.Resolutionmaytakeweeks.
Allergicconjunctivitis
Page 31
31
Symptoms:eyesitch(++)andareredandsore.Signs:eyelidswellingand.papillae(tinyelevationonthepalpebralconjunctiva).Historyofatopye.gasthma,eczema.Management:removeallergenswherepossible,topicalanti-histamines,coolcompresses.
Episcleritis
Sectoralepiscleritis
Page 32
32
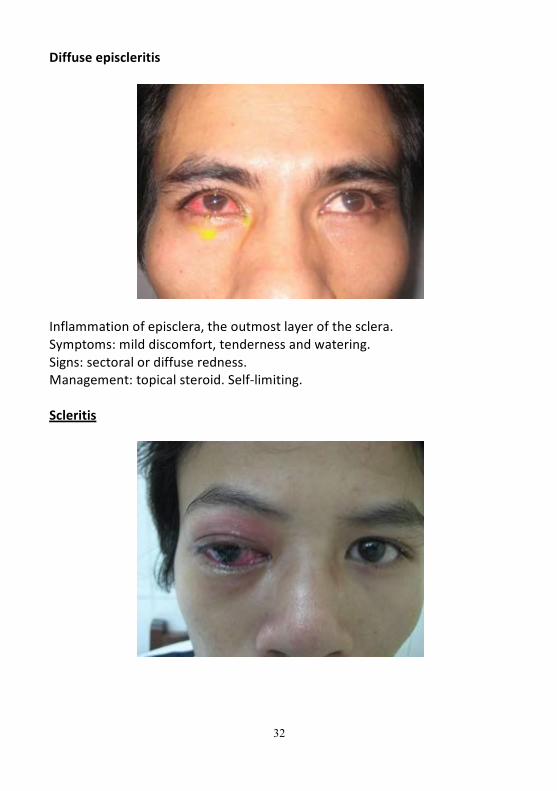
Diffuseepiscleritis
Inflammationofepisclera,theoutmostlayerofthesclera.Symptoms:milddiscomfort,tendernessandwatering.Signs:sectoralordiffuseredness.Management:topicalsteroid.Self-limiting.
Scleritis
Page 33
33
Thisisinflammationofthesclera.Inthemostsevereformscleralnecrosiscanoccur.Symptoms:Eyepainwhichradiatestoheadandwakespatientatnight.Signs:Theeyeisredandmayhavevisiblescleranodulesoranecroticpatch.Thescleramaybediscoloredandistendertopalpation.Thereisoftenanassociatedhistoryofrheumatoidarthritis,vascularorconnectivetissuedisease.Management:Urgent(sameday)referraltoanophthalmologist.Topicaland/orsystemiccorticotherapymayberequired.
Keratitis
Viralkeratitis
Page 34
34
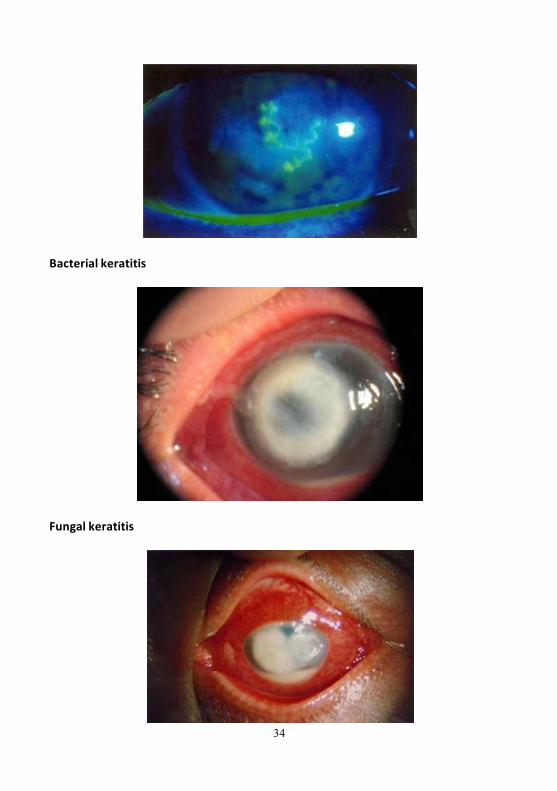
Bacterialkeratitis
Fungalkeratitis
Page 35
35
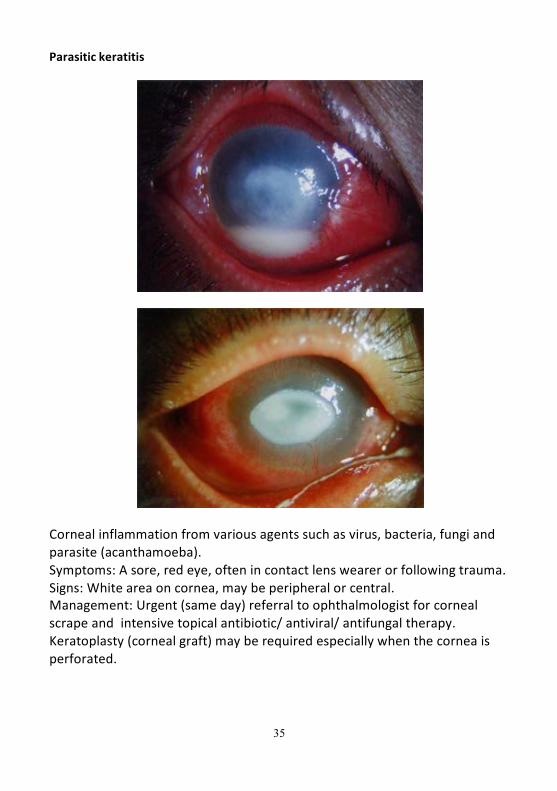
Parasitickeratitis
Cornealinflammationfromvariousagentssuchasvirus,bacteria,fungiandparasite(acanthamoeba).Symptoms:Asore,redeye,oftenincontactlenswearerorfollowingtrauma.Signs:Whiteareaoncornea,maybeperipheralorcentral.Management:Urgent(sameday)referraltoophthalmologistforcornealscrapeandintensivetopicalantibiotic/antiviral/antifungaltherapy.Keratoplasty(cornealgraft)mayberequiredespeciallywhenthecorneaisperforated.
Page 37
37
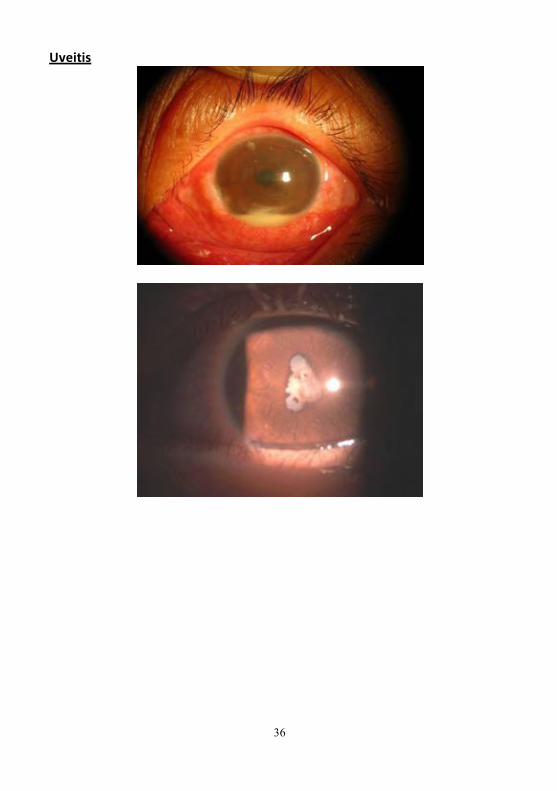
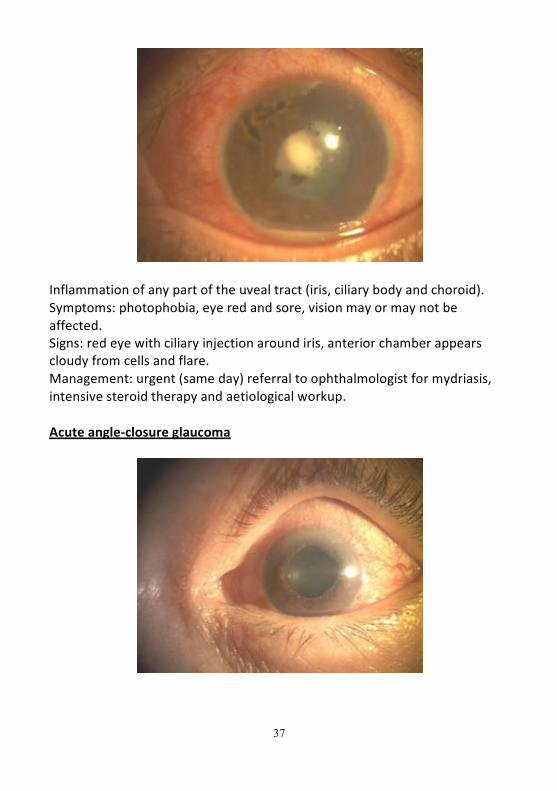
Inflammationofanypartoftheuvealtract(iris,ciliarybodyandchoroid).Symptoms:photophobia,eyeredandsore,visionmayormaynotbeaffected.Signs:redeyewithciliaryinjectionaroundiris,anteriorchamberappearscloudyfromcellsandflare.Management:urgent(sameday)referraltoophthalmologistformydriasis,intensivesteroidtherapyandaetiologicalworkup.
Acuteangle-closureglaucoma
Page 38
38
Asuddenincreaseinintraocularpressureoccursowingtotoaclosedanteriorchamberanglewhichpreventsaqueousdrainage.Symptoms:Painfuleyewithsystemicsymptomsincludingheadache,nauseaandvomiting.Signs:MorecommoninAsianraces.Theeyeisred,verytenderandfeelshardonpalpation;thecorneausuallyhashazyappearance.Theanteriorchamberisshallowwithirregularsemi-dilatedpupil.Management:urgent(sameday)referraltoophthalmologist.Topicalpilocarpine,Aqueousinhibitorsandbetablockersmayhelptolowertheintraocularpressure.Laseriridotomyortrabeculectomyisindicatedaccordingtointraocularpressurelevelandwhethertheangleisopen.Additionalcataractextractionmayhelptoopentheangleandnormalizethepressure.
Endophthalmitis
Page 39
39
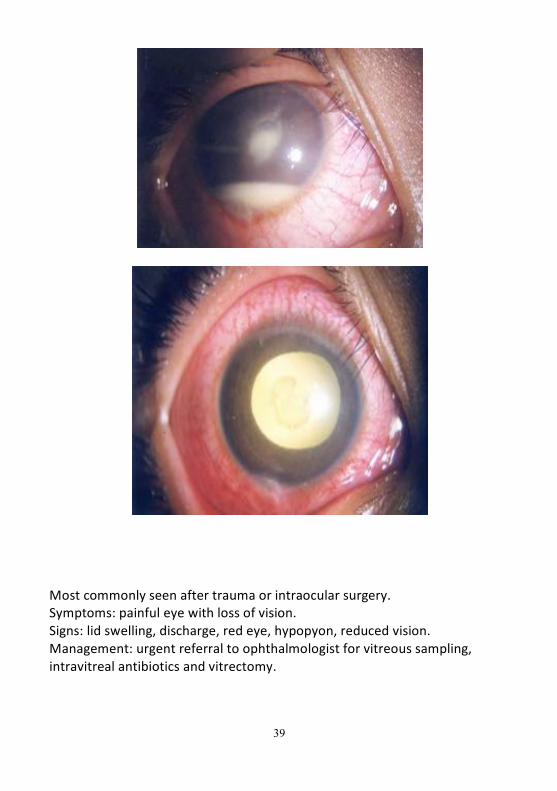
Mostcommonlyseenaftertraumaorintraocularsurgery.Symptoms:painfuleyewithlossofvision.Signs:lidswelling,discharge,redeye,hypopyon,reducedvision.Management:urgentreferraltoophthalmologistforvitreoussampling,intravitrealantibioticsandvitrectomy.
Page 40
40
SUDDENPAINLESSLOSSOFVISION
Vitreoushaemorrhage
Bleedinginthevitreouscavityseeninindividualswithdiabetesmellitus,cardio-vasculardiseasesandretinaldetachment.Symptoms:Suddenlossofvisionoftenwithfloaters.Signs:Reducedorabsentredreflex.Limitedornofundalview.Management:Refertoophthalmologistforultrasoundscantoensurethatthereisnounderlyingretinaldetachment. Avitrectomymayberequiredfornon-clearinghaemorrhage.
Page 41
41
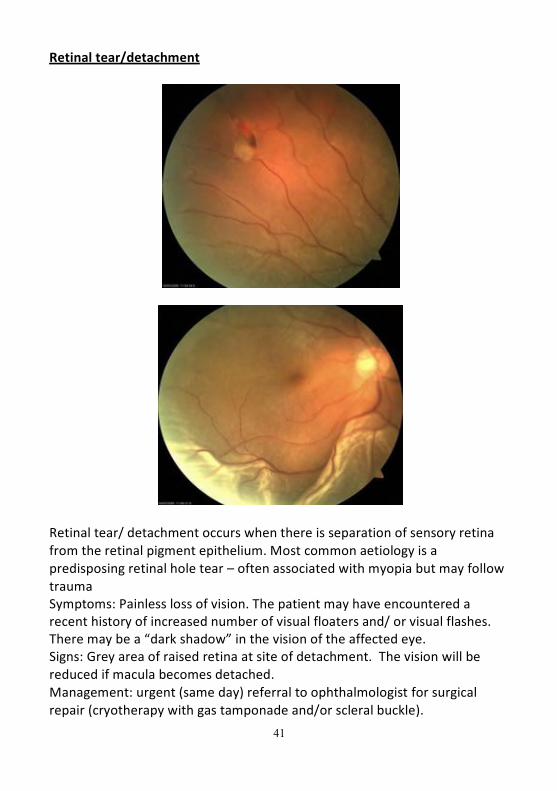
Retinaltear/detachment
Retinaltear/detachmentoccurswhenthereisseparationofsensoryretinafromtheretinalpigmentepithelium.Mostcommonaetiologyisapredisposingretinalholetear–oftenassociatedwithmyopiabutmayfollowtraumaSymptoms:Painlesslossofvision.Thepatientmayhaveencounteredarecenthistoryofincreasednumberofvisualfloatersand/orvisualflashes.Theremaybea“darkshadow”inthevisionoftheaffectedeye.Signs:Greyareaofraisedretinaatsiteofdetachment. Thevisionwillbereducedifmaculabecomesdetached.Management:urgent(sameday)referraltoophthalmologistforsurgicalrepair(cryotherapywithgastamponadeand/orscleralbuckle).
Page 42
42
Centralretinalarteryocclusion
Blockedbloodflowinthecentralretinalartery,whichoftenoccursinoneeye.Symptoms:Suddenandpainlesslossofvision.Signs:Thevisualacuityisverypoor,atbestperceptionoflightorhandmovements,togetherwithaRelativeAfferentPupillaryDefect(RAPD).Fundusexamination:Paleretina(abnormalandasymmetricalredreflex),cherry-redspotatmaculaduetocilioretinalsparing.Delayedarterialfillingonfluoresceinangiogram.Investigation:urgent(sameday)ESRandCRPtoexcludegiantcellarteritis.
Page 43
43
Management:Urgent(sameday)referraltoophthalmologisttoseewhetheranyimmediatetreatmentispossible.Intensiveintraocularpressurelowering(ACinhibitorsandparacenthesis)mayhelpinsomecases.Awork-upforcausesofTransientIschaemicAttackswillneedtobearranged.
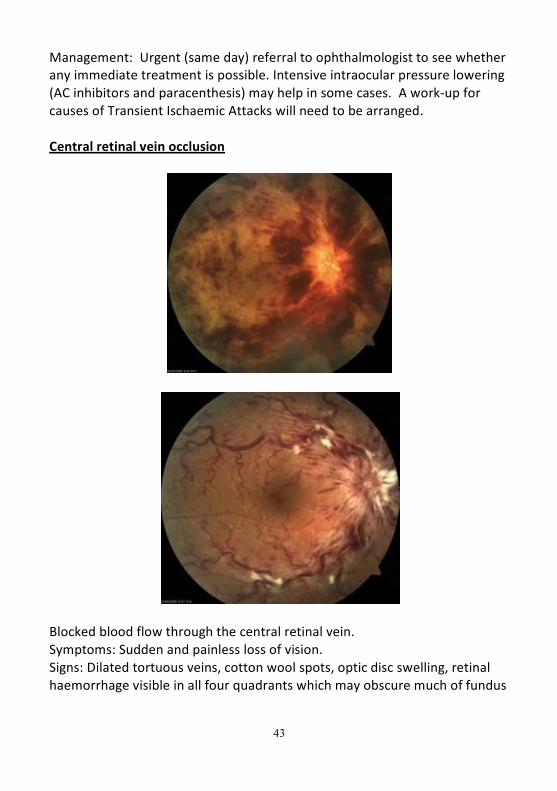
Centralretinalveinocclusion
Blockedbloodflowthroughthecentralretinalvein.Symptoms:Suddenandpainlesslossofvision.Signs:Dilatedtortuousveins,cottonwoolspots,opticdiscswelling,retinalhaemorrhagevisibleinallfourquadrantswhichmayobscuremuchoffundus
Page 44
44
detail. Predisposingfactorsincludeincreasingage,hypertensionanddiabetes,aswellasraisedintraocularpressure.InvestigationandManagement:Screenfordiabetesandhypertension,excludeglaucoma.Routinereferralforanophthalmologicalopinion.Fluoresceinangiographyisoftenperformedtoinvestigatehowischaemicthefundusis,andlasercanbeindicatedtopreventneovascularglaucomaandrecurrentvitreoushaemorrhage.
Papillitis
Page 45
45
Acuteinflammationofopticnerveisassociatedwithmoderatetoseverevisionloss.Longlastingpapillitisleadstoopticatrophy.Symptoms:suddenreducedvision,discomfortuponeyemovement.Signs:centralvisualfielddefect,opticdiscswelling,RelativeAfferentPupillaryDefect(RAPD).Management:excludemultiplesclerosis,infectionofmeninges,orbitaltissuesorparanasalsinuses.Intensivesystemiccorticotherapymayhelp.
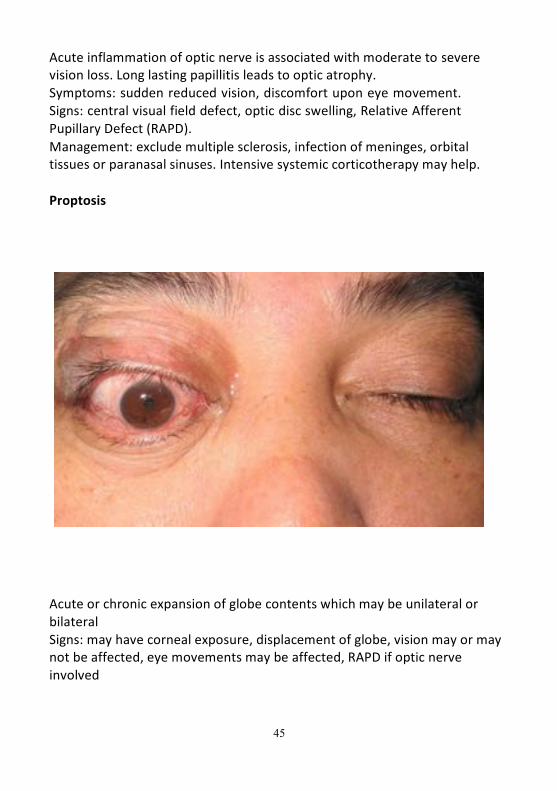
Proptosis
AcuteorchronicexpansionofglobecontentswhichmaybeunilateralorbilateralSigns:mayhavecornealexposure,displacementofglobe,visionmayormaynotbeaffected,eyemovementsmaybeaffected,RAPDifopticnerveinvolved
Page 46
46
Management:imagingtodefinecauseofpropotosis.Investigationsasappropriatedependingonwhichorbitalstructuresareinvolvedwhichmayincludethyroidfunctiontestsandorbitalbiopsy
VIInervepalsy
Mainproblemforeyeisfailureofeyeidclosure socornealexposure.Maybeidiopathic(Bell’spalsy)orcausedbytrauma,tumour,infection,inflammationSigns:Varyinseveritybutfailuretocloseeyelidisthekeysign,maybeothersignsofVIIthnervepalsyManagement:ensureeyeclosureandlubricate.Mayrecover.Ifnotmayrequireprocedurestohelpwiththisegtarrsorraphy,weightsonupperlid.