I International Journal oi Psychiatry in Clinical Practice, 2007; 11(3): 222-232 ORIGINAL ARTICLE informa healthcare The "Seroquel" Outcomes Study (SOS): Efficacy and tolerability oí quetiapine in a long-term, naturalistic study oí patients with schizophrenia JUAN GIBERT1, JosÉ GINER2, JULIO BOBES3, MÓNICA TAFALl.A\ SANTIAGO HERRANZ\ CARMEN OVEJER05 & FERNANDO RICO-VIllADEMOROS5 for the SOS GROUP* 1 Facultad de Medicina, Departamento de Farmacología, Cádiz, Spain, 2Departamento de Psiquiatría, Hospital Universitario "Virgen Macarena", Universidad de Sevilla, Sevilla, Spain, 3Departamento de Psiquiatría, Facultad de Medicina, Universidad de Oviedo, Oviedo, Spain, 4Departamento Médico, AstraZeneca, Madrid, Spain, and 5Biométrica, Madrid, Spain Abstraet Objective. The "Seroquel" Outcomes Study (SOS) aimed to assess the efficacy and tolerability of quetiapine in patients with schizophrenia in the clinical practice setting. Methods. A 6-month, non-comparative, open-label study in adults with schizophrenia in a standard care setting in Spain. Outpatients received tlexibly dosed quetiapine. Efficacy was evaluated using the BriefPsychiatry Rating Scale (BPRS) and the Clinical Globallmpression (CGI) scale. BPRS response was defined as ~30% decrease from baseline. Tolerability was assessed using the Simpson-Angus Scale (SAS) and a modified Udvalg for Kliniske Undersogelser (UKU) side-effeets scale. Results. A total of 2029 patients enrolled. Significant changes from baseline to Month 6 were recorded for BPRS total and subscale scores (P <0.001). Compared with doses of~600 mg/day, doses of <400 mg/day were a strong predictor of a lower response rate (OR 0.62; 95% CI: 0.48, 0.82) and higher withdrawal rate (OR 3.3; 95% CI; 2.5, 4.4). Mean change in weight was minimal (+0.4 kg). Somnolence (26.7%), asthenia (12.5%), and constipation (9.8%) were the most common adverse events. Conclusion. Quetiapine was found to improve symptoms of schizophrenia, as indicated by a significant decrease in BPRS scores, and was well tolerated by patients in clinical practice. Key Words: Quetiapine, antipsychotics, schizophrenia, naturalistic, outpatient Introduction Schizophrenia is a chronic and debilitating illness that impacts on the cognitive, affective, behavioural, and motivational functioning of patients [1]. The World Health Organization has reported a world- wide prevalence rate of 0.1-1.7% [2], while in the US, the lifetime prevalence of the disease is esti- mated at 1% [3]. The development of the so-caBed "atypical" antipsychotics in the 1990s extended the treatment options for patients with schizophrenia. In addition to effectively treating the positive symptoms of schizophrenia, these agents are effective against negative, affective and cognitive symptoms. Their * See Appendix for tbe complete list of SOS Group members. broad therapeutic profile and improved tolerability compared with the conventional antipsychotics, particularly with regard to extrapyramidal symptoms (EPS), means that the atypical antipsychotics are considered first-line treatment for schizophrenia in most clinical situations [4]. The modero standard for evaluating new medi- cines is the randomised clínical tríal [5]. Although the use of proper controls, randomisation and blinding decreases bias and the potential for error, the condi- tions under which such trials are conducted differ from everyday clínical practice [6,7]. In the "real- life" setting, the typical patient often presents with comorbid disorder(s), has not responded to previous treatment efforts, and may require a number of different treatments. Further, trial patients are usually carefully selected and must meet strict study Correspondence: Mónica Tafalla, MD, Medical Department, AstraZeneca, Parque Norte, Edificio Roble, Serrano Galvache 56, 28033 Madrid, Spain. Tel.: +34 91 301 9647. Fax: +3491 301 9104. E-mail: [email protected](Received 10 February 2006; accepted 7 December 2006) ISSN 1365-1501 print/lSSN 1471-1788 online iD 2007 Taylor & Francis DOI: 10.1080/13651500601176963
Transcript
IInternational Journal oi Psychiatry in Clinical Practice, 2007; 11(3): 222-232
ORIGINAL ARTICLE
informahealthcare
The "Seroquel" Outcomes Study (SOS): Efficacy and tolerability oíquetiapine in a long-term, naturalistic study oí patients withschizophrenia
JUAN GIBERT1, JosÉ GINER2, JULIO BOBES3, MÓNICA TAFALl.A\SANTIAGO HERRANZ\ CARMEN OVEJER05 & FERNANDO RICO-VIllADEMOROS5for the SOS GROUP*
1Facultad de Medicina, Departamento de Farmacología, Cádiz, Spain, 2Departamento de Psiquiatría, Hospital Universitario
"Virgen Macarena", Universidad de Sevilla, Sevilla, Spain, 3Departamento de Psiquiatría, Facultad de Medicina,
Universidad de Oviedo, Oviedo, Spain, 4Departamento Médico, AstraZeneca, Madrid, Spain, and 5Biométrica, Madrid,
Spain
AbstraetObjective. The "Seroquel" Outcomes Study (SOS) aimed to assess the efficacyand tolerability of quetiapine in patients withschizophrenia in the clinical practice setting. Methods. A 6-month, non-comparative, open-label study in adults withschizophrenia in a standard care setting in Spain. Outpatients received tlexibly dosed quetiapine. Efficacy was evaluatedusing the BriefPsychiatry Rating Scale (BPRS) and the Clinical Globallmpression (CGI) scale. BPRS response was definedas ~30% decrease from baseline. Tolerability was assessed using the Simpson-Angus Scale (SAS) and a modified Udvalgfor Kliniske Undersogelser (UKU) side-effeets scale. Results. A total of 2029 patients enrolled. Significant changes frombaseline to Month 6 were recorded for BPRS total and subscale scores (P <0.001). Compared with doses of~600 mg/day,doses of <400 mg/day were a strong predictor of a lower response rate (OR 0.62; 95% CI: 0.48, 0.82) and higherwithdrawal rate (OR 3.3; 95% CI; 2.5, 4.4). Mean change in weight was minimal (+0.4 kg). Somnolence (26.7%), asthenia(12.5%), and constipation (9.8%) were the most common adverse events. Conclusion. Quetiapine was found to improvesymptoms of schizophrenia, as indicated by a significant decrease in BPRS scores, and was well tolerated by patients inclinical practice.
Schizophrenia is a chronic and debilitating illnessthat impacts on the cognitive, affective, behavioural,and motivational functioning of patients [1]. TheWorld Health Organization has reported a worldwide prevalence rate of 0.1-1.7% [2], while in theUS, the lifetime prevalence of the disease is estimated at 1% [3].
The development of the so-caBed "atypical"antipsychotics in the 1990s extended the treatmentoptions for patients with schizophrenia. In additionto effectively treating the positive symptoms ofschizophrenia, these agents are effective againstnegative, affective and cognitive symptoms. Their
* See Appendix for tbe complete list of SOS Group members.
broad therapeutic profile and improved tolerabilitycompared with the conventional antipsychotics,particularly with regard to extrapyramidal symptoms(EPS), means that the atypical antipsychotics areconsidered first-line treatment for schizophrenia inmost clinical situations [4].
The modero standard for evaluating new medicines is the randomised clínical tríal [5]. Although theuse of proper controls, randomisation and blindingdecreases bias and the potential for error, the conditions under which such trials are conducted differ
from everyday clínical practice [6,7]. In the "reallife" setting, the typical patient often presents withcomorbid disorder(s), has not responded to previoustreatment efforts, and may require a number ofdifferent treatments. Further, trial patients areusually carefully selected and must meet strict study
(Received 10 February 2006; accepted 7 December 2006)
ISSN 1365-1501 print/lSSN 1471-1788 online iD 2007 Taylor & FrancisDOI: 10.1080/13651500601176963
inclusion/exclusion criteria. Naturalistic studies closely mirror daily clinical practice, but have thedisadvantage of being uncontrolled and as they areobservational are potentially open to bias. How a newmedicine performs in clinical practice is a properindication of its ttue benefit to risk ratio [8]. It is,therefore, important for the prescribing clinician toconsider clinical trial data in conjunction with datafrom naturalistic studies as well as his/her ownexperience when selecting an atypical antipsychoticfor a given patient [9].
Quetiapine is a dibenzothiazepine atypical antipsychotic with affinity for various neurotransmitterreceptors including serotonin, dopamine, histamine,and adrenergic receptors and its chemical struetureis similar to that of clozapine [10]. Three pivotal,randomised, double-blind clinical trials demonstrated that quetiapine efIectively reduces psychoticsymptoms in patients with schizophrenia as indicated by significant difIerences between quetiapineand placebo on the Brief Psychiatty Rating Scale(BPRS) total, BPRS positive-symptom, Scale for theAssessment of Negative Symptoms (SANS) andClinical Global Impression (CGI) severity of illnessscales [11-13]. Quetiapine has shown comparableefficacy to chIorpromazine [14] and haloperidol[15,16]. The main objective of the "Seroquel"Outcomes Study (SOS) was to assess the efficacyand tolerability of the atypical antipsychotic, quetiapine ("Seroquel"), in a large representative group ofpatients with schizophrenia under naturalistic conditions. It also assessed factors relevant to the use ofquetiapine in the clinical setting, such as the reduction of side efIects in patients who had switched toquetiapine from previous antipsychotic medications.
Methods
Patients
Male or female outpatients aged ~ 18 years with aDSM-IV diagnosis of schizophrenia or schizophreniform disorder for whom study investigators prescribed quetiapine as part of their normal clinicalpractice were included in the study. Patients wereexcluded if contraindicated by the quetiapine product label, for example, known hypersensitivity tothe medication or any of its ingredients.
This study was conducted in accordance with theDeclaration of Helsinki [17]. Written informedconsent was obtained from all patients prior toenrolment and the study was reported to theMinistty of Health in accordance with Spanishregu1ations at the time of the trial.
Study design and dosing
This was a non-comparative, open-Iabel, naturalistic, multicentre study conducted in Spain and
NaturaJistic study of quetiapine for schizophrenia 223
involved 279 investigators (see Appendix). Eligiblepatients received open treatment with quetiapine(flexiblydosed according to the clinical judgement ofthe study investigator) and were followed for 6months (Figure 1). The use of concomitant medications was permitted at the discretion of the clinician.
Patients were categorised into two groups atbaseline: (1) patients not currently receiving antipsychotic treatment (first or breakthrough episode);(2) patients currently receiving antipsychotic treatment and requiring combination treatment withquetiapine or a switch to quetiapine due to aninadequate response or intolerable adverse events.Inadequate response was defined as persistent positive, negative, cognitive or severe depressive symptoms, persistent agitation, or treatment-refractoryschizophrenia. Intolerable adverse events were determined by the psychiatrist and included sedation,weight gain, EPS, cognitive, anticholinergic, cardiovascular or sexual/reproductive adverse events, tardive dyskinesia or neuroleptic malignant syndrome.
Efficacy assessments
The primary efficacy assessments were changes frombaseline on the BPRS [18] total and subscale scoresand the CGI [19] severity of illness scale at Months1,3 and 6. The BPRS comprises 16 items coveringgeneral, positive and negative symptoms and isscored on a severity scale of 1-7 (higher scoresindicate more severe symptoms). The CGI severityof illness scale has a seven-point scale (1 is normaland 7 is extremely ill). Secondary efficacy variablesincluded the BPRS response rate (response wasdefined as a ~ 30% decrease from baseline in BPRSscore) and the CGI improvement scale, whichmeasures the change in the state of the patient'sillness relative to baseline scored from 1 (very muchimproved) to 7 (very much worse) and was completed at each visitoIn addition, a CGI improvementof side efIects scale (a scale identical to the CGIimprovement scale used for the efficacy assessment)was fulfilled at each visit for patients with intolerableadverse efIects to previous antipsychotic treatment.A CGI global improvement rating of at least "muchimproved" constituted a therapeutic response forboth an improvement in the illness and an improvement in side efIects. Investigators also recorded ifpatients exhibited any of the following: aggression/violence, agitation/excitement, insomnia, dysphoria,suicidal behaviour, comorbid substance abuse, cognitive difficulties or other problems. Categories wereprimarily based on those described in the ExpertConsensus Guideline for the Treatment of Schizophrenia [19].
At the end of the study, patients completed aLikert-type scale (7 points) to report their satisfaction with treatment, where 1 indicated "extremely
224 J Gibert et al.
Withdrawn N=142:
Lost to follow-up, N=48Adversa event, N=5Lack of efflcacy, N=46Palient withdrew consent, N=27Other, N=16
Withdrawn N=175:
Lost to follow-up, N=46Adverse event, N=18Lack of efficacy, N--43Palient withdrew cansent, N=40Other, N=28
Withdrawn N=155:
Lost to follow-up, N=15Adversa event, N=46Lack of efficacy, N=22Palient withdrew consen!, N=52Other, N=20
5 PIs not available at Month 1
Withdrawn N=l42:Lost to follow-up, N=48Adversa event, N=5Lack of efflcacy, N=46Patient withdrew cansent, N=27Other, N=16
Withdrawn N=174:Lost to follow-up, N=45Adversa event, N= 18Lack of efficacy, N=43Patient withdrew cansent, N=40Other, N=28
Withdrawn N=120:
Lost to follow-up, N=3Adversa event, N=40Lack of efficacy, N=22Patient withdrew cansen!, N=42Other, N=13
5 pis not available at Month 1
Excluded N=109
Missing baselinevisit 3 (0.1%)
Missing post-baselinevisit 68 (3.3%)
No post-basaline efficacyevaluation 38 (1.9%)
5 pis not available at Month 3but available al Month 6
5 PIs not available at Month 3but avaiJable at Month 6
Figure l. Patient disposition.
satisfied", 4 "neither satisfied nor dissatisfied", and7 "extremely dissatisfied" with treatment.
Tolerability assessments
Medical and psychiatric histories were taken atbase1ine and a physical examination was carriedout. Vital signs and weight were measured by theinvestigators using their normal clinical practicemethods (non-standardised procedures) at baselineand at Months 1,3 and 6. Body mass index (BMI)was calculated. Weight gain was defmed as anyincrease in weight (kg) from baseline. TheSimpson-Angus Scale (SAS), a 10-point scalemeasuring EPS using standardised clinical assessment of parkinsonian side-effects including tremor,rigidity and salivation, was completed at baselineand at each follow-up visito Treatment-emergentadverse events, including sedation and cognitiveside effects, were identified by patient report throughopen questioning ("Have you had any discomfortthat could be related to the antipsychotic medication?") and categorised by the investigator using amodified Udvalg for K1iniskeUndersogelser [UKU]Side Effect Rating Scale [20], a 23-point scalecovering cognitive, whole body abnormalities andsexual dysfunction, at baseline and each follow-upvisitoThe investigators used their own judgement todetermine the probability of a causal relationship ofan adverse event to the medication as "absent","possible", or "probable". In addition, adverse
events classed as "intolerable", such as tardivedyskinesia, were evaluated by the clinician usingthe CGI improvement of side effects scale asdescribed above.
Statistical analysis
Al1efficacyanalyses were performed on the intentionto treat (fIT) sample using a last observation carriedforward approach (LOCF). The ITT populationcomprised patients who met the study entry criteria,were prescribed quetiapine and had at least one postbaseline efficacy evaluation. For inclusion of patientdata in the ITT sample for multi-item scales such asthe BPRS, data for at least 80% of all items wasrequired. Logistic regression analysis was carried outto determine the relationship between patients'clinical characteristics, dose of quetiapine at endpoint (categorised as low, <400; intermediate,~400 to <600; and high, ~600 mglday) andresponse rateo A Student's paired t-test was used toanalyse changes from baseline to endpoint in theBPRS total and clusters scores. AlI statistical testswere two-tailed with a P value of ~0.05 consideredstatistically significant [21].
Descriptive statistics were used to summarisemodified UKU and SAS total score data for thetolerability population (all patients who enteredthe study and had at least one follow-up visit).Any increase from the baseline severity score in aUKU item rated as possibly or probably related to
quetiapine was considered to be an adverse event;missing evaluations of causal relationship were alsoconsidered possibly related to quetiapine. For theSAS, changes from baseline scores were assigned tothree categories: "improved" (change <O), "nochange" (change =0) and "worsened" (change>0), and the frequency distributions of the cate
gories calculated for each study visitoA logistic regression analysis was performed to
investigate the relationship between patients' clínicalcharacteristics and quetiapine dose with regard toresponse rateo The following risk factors were included: age, sex, first episode, breakthrough episode,inadequate response to previous treatment, intolerable adverse reactions to previous treatment, inadequate response and intolerable adverse reactions toprevious treatment, treatment -refractory schizophrenia, dose (categorised as "low", "intermediate" and"high"; see definitions above), prominent depression(BPRS item #9 score >4), prominent hostility symptoms (BPRS item #10 score >4), prominent anxietysymptoms (BPRS item #2 score >4), diagnosticcomplications as defined above were introduced asdichotomous variables, and finally the total BPRSscore at baseline.
Results
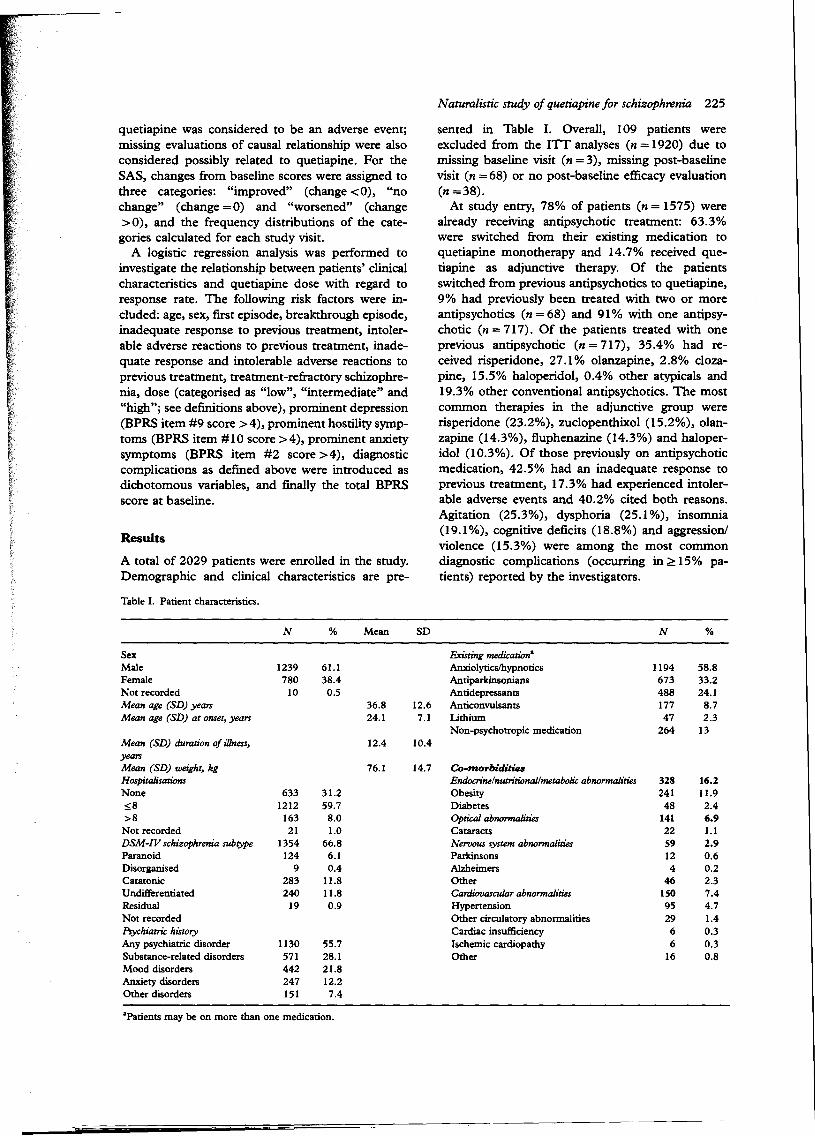
A total of 2029 patients were enrolled in the study.Demographic and clínical characteristics are pre-
Table I. Patient charaeteristics.
Naturalistic study of quetiapine for schizophrenia 225
sented in Table 1. Overall, 109 patients wereexcluded from the ITT analyses (n =1920) due tomissing base1ine visit (n =3), missing post-baselinevisit (n = 68) or no post-baseline efficacy evaluation(n =38).
At study entry, 78% of patients (n = 1575) werealready receiving antipsychotic treatment: 63.3%were switched from their existing medication toquetiapine monotherapy and 14.7% received quetiapine as adjunctive therapy. Of the patientsswitched from previous antipsychotics to quetiapine,9% had previously been treated with two or moreantipsychotics (n =68) and 91% with one antipsychotic (n = 717). Of the patients treated with oneprevious antipsychotic (n = 717), 35.4% had received risperidone, 27.1% olanzapine, 2.8% clozapine, 15.5% haloperidol, 0.4% other atypicals and19.3% other conventional antipsychotics. The mostcommon therapies in the adjunctive group wererisperidone (23.2%), zuclopenthixol (15.2%), olanzapine (14.3%), fluphenazine (14.3%) and haloperidol (10.3%). Of those previously on antipsychoticmedication, 42.5% had an inadequate response toprevious treatment, 17.3% had experienced intolerable adverse events and 40.2% cited both reasons.Agitation (25.3%), dysphoria (25.1 %), insomnia(19.1%), cognitive deficits (18.8%) and aggression/violence (15.3%) were among the most commondiagnostic complications (occurring in ~ 15% patients) reported by the investigators.
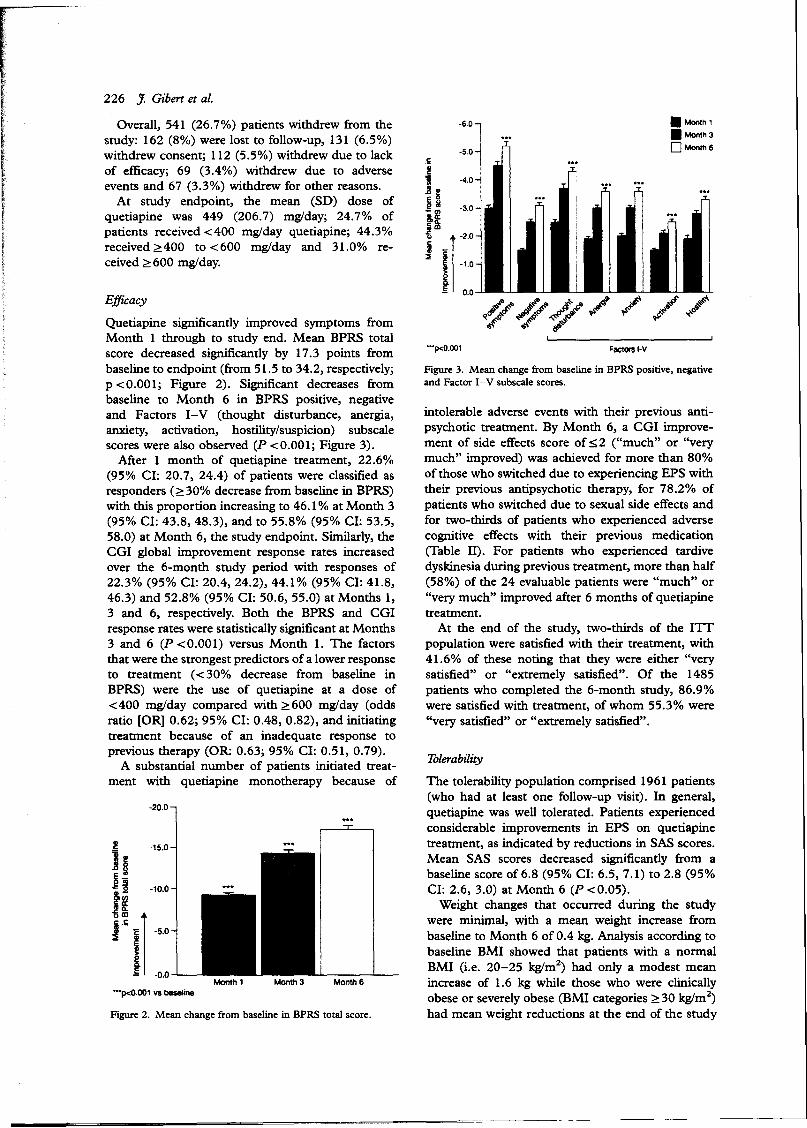
Figure 3. Mean change froro baseline in BPRS positive, negativeand Factor 1-V subscale scores.
1blerability
The tolerability population comprised 1961 patients(who had at least one follow-up visit). In general,quetiapine was well tolerated. Patients experiencedconsiderable improvements in EPS on quetiapinetreatment, as indicated by reductions in SAS scores.Mean SAS scores decreased significantly from abaseline score of6.8 (95% CI: 6.5, 7.1) to 2.8 (95%CI: 2.6, 3.0) at Month 6 (P <0.05).
Weight changes that occurred durlng the studywere mínimal, with a mean weight increase frombaseline to Month 6 of 0.4 kg. Analysis according tobaseline BMI showed that patients with a normalBMI (Le. 20-25 kglm2) had only a modest meanincrease of 1.6 kg while those who were clinicallyobese or severely obese (BMI categories ~30 kglm2)had mean weight reductions at the end of the study
• Monlh1
• Monlh3
O Monlh6
F~Qr$I·V
·6.0
·5.0
"·p<O.OOl
.s
j ~ ·4.0~li
- CI) ·3.0
f~-1.2.0
~ -1.0
~.É 0.0
intolerable adverse events with their previous antipsychotic treatment. By Month 6, a CGI improvement of side efIects score of:::;;2 ("much" or "verymuch" improved) was achieved for more than 80%of those who switched due to experiencing EPS withtheir previous antipsychotic therapy, for 78.2% ofpatients who switched due to sexual side efIects andfor two-thirds of patients who experienced adversecognitive efIects with their previous medication(Table 11). For patients who experienced tardivedyskinesia during previous treatment, more than half(58%) of the 24 evaluable patients were "much" or"very much" improved after 6 months of quetiapinetreatment.
At the end of the study, two-thirds of the lITpopulation were satisfied with their treatment, with41.6% of these noting that they were either "verysatisfied" or "extreme1y satisfied". Of the 1485patients who completed the 6-month study, 86.9%were satisfied with treatment, of whom 55.3% were"very satisfied" or "extremely satisfied".
Overall, 541 (26.7%) patients withdrew from thestudy: 162 (8%) were lost to follow-up, 131 (6.5%)withdrew consent; 112 (5.5%) withdrew due to lackof efficacy; 69 (3.4%) withdrew due to adverseevents and 67 (3.3%) withdrew for other reasons.
At study endpoint, the mean (SD) dose ofquetiapine was 449 (206.7) mg/day; 24.7% ofpatients received <400 mg/day quetiapine; 44.3%received ~400 to <600 mg/day and 31.0% received ~ 600 mg/day.
Bfficacy
Quetiapine significantly improved symptoms fromMonth 1 through to study end. Mean BPRS totalscore decreased significantly by 17.3 points frombase1ineto endpoint (from 51.5 to 34.2, respective1y;p <0.001; Figure 2). Significant decreases frombaseline to Month 6 in BPRS positive, negativeand Factors I-V (thought disturbance, anergia,anxiety, activation, hostility/suspicion) subscalescores were also observed (P <0.001; Figure 3).
After 1 month of quetiapine treatment, 22.6%(95% CI: 20.7, 24.4) of patients were c1assifiedasresponders (~30% decrease from baseline in BPRS)with this proportion increasing to 46.1 % at Month 3(95% CI: 43.8, 48.3), and to 55.8% (95% CI; 53.5,58.0) at Month 6, the study endpoint. Similarly, theCGI global improvement response rates increasedover the 6-month study period with responses of22.3% (95% CI: 20.4, 24.2), 44.1% (95% CI; 41.8,46.3) and 52.8% (95% CI: 50.6, 55.0) at Months 1,3 and 6, respectively. Both the BPRS and CGIresponse rates were statistically significant at Months3 and 6 (P <0.001) versus Month 1. The factorsthat were the strongest predictors of a lower responseto treatment (< 30% decrease from baseline inBPRS) were the use of quetiapine at a dose of<400 mg/day compared with ~600 mg/day (oddsratio [OR] 0.62; 95% CI; 0.48, 0.82), and initiatingtreatment because of an inadequate response toprevious therapy (OR: 0.63; 95% CI: 0.51, 0.79).
A substantial number of patients initiated treatment with quetiapine monotherapy because of
-20.0
Figure 2. Mean change froro baseline in BPRS total score.
Month 1
"'1><0.001 vs b8se1ine
,Naturalistic study 01quetiapine lor schizophrenia 227
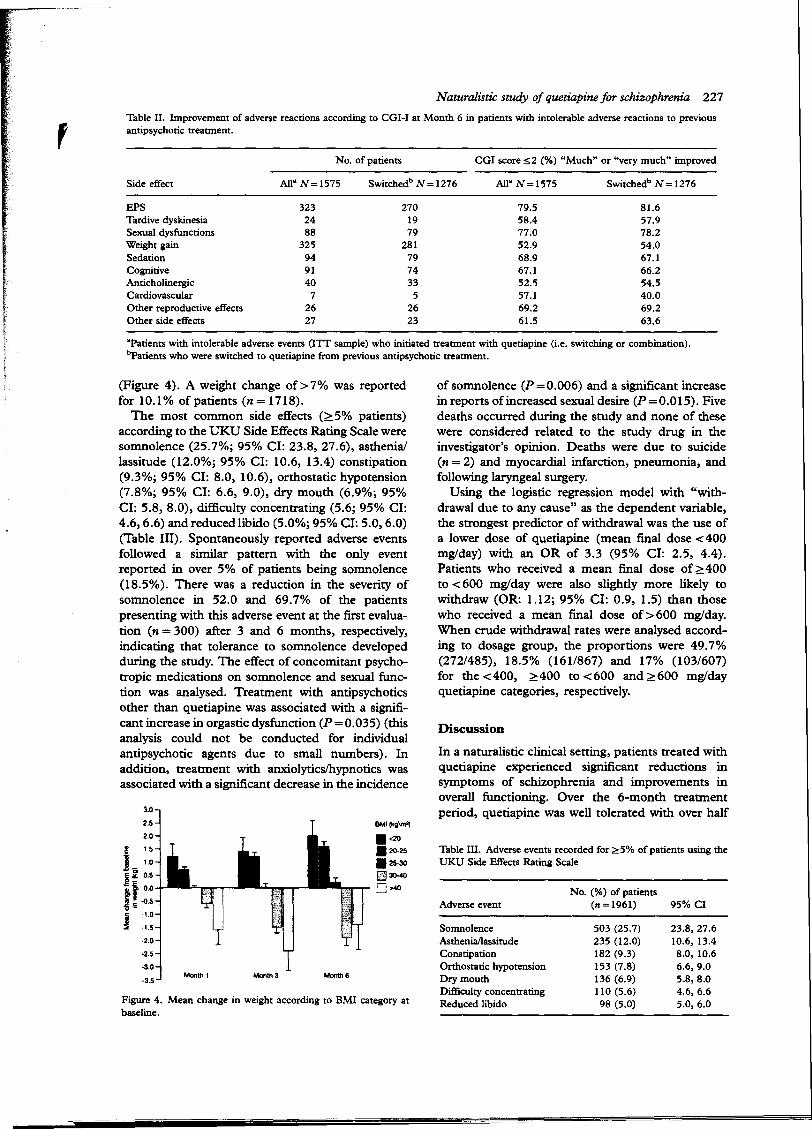
Table II. Improvement of adverse reactions according to CGI-I at Month 6 in patients with intolerable adverse reactions to previousantipsycbotic treatment.
No. of patients CGI score:S;2 (%) "Much" or "very much" improved
Side effect AlI" N=1575 Switcbedb N = 1276 AlI" N=1575 Switcbedb N = 1276
EPS
Tardive dyskinesiaSexual dysfunctions
Weight gainSedation
CognitiveAnticholinergicCardiovascular
Other reproductive effectsOther side effeets
3232488
325949140
72627
2701979
281797433
52623
79.558.477.052.968.967.152.557.169.261.5
81.657.978.254.067.166.254.540.069.263.6
'Patients with intolerable adverse events (ITT sample) who initiated treatment with quetiapine (Le. switching or combination).bpatients who were switcbed to quetiapine from previous antipsychotic treatment.
Figure 4. Mean change in weight according to BMI category atbaseline.
(Figure 4). A weight change of>7% was reportedfor 10.1% ofpatients (n= 1718).
The most common side effects (~5% patients)according to the UKU Side Effects Rating Scale weresomnolence (25.7%; 95% CI: 23.8, 27.6), asthenia/lassitude (12.0%; 95% CI: 10.6, 13.4) constipation(9.3%; 95% CI: 8.0, 10.6), orthostatic hypotension(7.8%; 95% CI: 6.6, 9.0), dry mouth (6.9%; 95%CI: 5.8, 8.0), difficulty concentrating (5.6; 95% CI:4.6,6.6) and reduced libido (5.0%; 95% CI: 5.0,6.0)(Table lII). Spontaneously reported adverse eventsfollowed a similar pattern with the only eventreported in over 5% of patients being somnolence(18.5%). There was a reduction in the severity ofsomnolence in 52.0 and 69.7% of the patientspresenting with this adverse event at the first evaluation (n = 300) after 3 and 6 months, respectively,indicating that tolerance to somnolence developedduring the study. The effect of concomitant psychotropic medications on somnolence and sexual function was analysed. Treatment with antipsychoticsother than quetiapine was associated with a significant increase in orgastic dysfunction (P=0.035) (thisanalysis could not be conducted for individualantipsychotic agents due to small numbers). Inaddition, treatment with anxiolyticsJhypnotics wasassociated with a significant decrease in the incidence
Table III. Adverse events recorded for ;?:5% of patients using theUKU Side Effeets Rating Scale
In a naturalistic clínical setting, patients treated withquetiapine experienced significant reductions insymptoms of schizophrenia and improvements inoverall functioning. Over the 6-month treatmentperiod, quetiapine was well tolerated with over half
ofsomnolence (P=0.006) and a significant increasein reports ofincreased sexual desire (P=0.015). Fivedeaths occurred during the study and none of thesewere considered related to the study drug in theinvestigator's opínion. Deaths were due to suicide(n = 2) and myocardial infarction, pneumonia, andfollowing laryngeal surgery.
Using the logistic regression model with "withdrawal due to any cause" as the dependent variable,the strongest predictor of withdrawal was the use ofa lower dose of quetiapine (mean final dose <400mg/day) with an OR of 3.3 (95% CI: 2.5, 4.4).Patients who received a mean final dose of ~ 400to <600 mg/day were also slightly more likely towithdraw (OR: 1.12; 95% CI: 0.9, 1.5) than thosewho received a mean final dose of>600 mg/day.When crude withdrawal rates were analysed according to dosage group, the proportions were 49.7%(272/485), 18.5% (161/867) and 17% (103/607)for the <400, ~400 to <600 and ~600 mg/dayquetiapine categories, respectively.
BMI(kglm'l
.<20
.20-25
.2S-30~30-400>40
Monlh 6Month3Monlh 1
3.0
2.5
2.0
.! 1.5
J- 1.0
j~ 0.5
s.f. 0.0le .o.S
i-·1.03 ·1.5
-2.0
-2.5
·3.0
-3.5
I228 J. Gibert et al.
the population of patients who completed the studyindicating a high degree of satisfaction (very orextremely satisfied) with the treatment that theyreceived.
The response rate of 55.8% obtained in the studywas very similar to that reported in trials by Arvanitiset al (51% with 300 mg/day quetiapine) and Smallet al (50% with <250 mg/day quetiapine and 53%with ~250 to :::;;750mg/day quetiapine) using thesame criteria of a ~ 30% reduction in BPRS totalscore [11,13]. However, it is important to note thata substantial proportion of patients in our studyínitiated treatment with quetiapine solely because ofthe presence of intolerable side efIects with previousantipsychotics. In addition, our study included agreater proportion of patients with comorbiditiesand, possibly, more treatment-refractory patients.Over 30% of patients who were classed as nonresponders (:::;;30%decrease in BPRS score) reported that they were satisfied with treatment. Thissuggests that it is important to use both objective andsubjective measures to assess patient response totreatment in a naturalistic clínical setting.
A low withdrawal rate of26. 7% was observed. Thisis comparable with the 26.5% withdrawal rateencountered with olanzapine in the same settingwith a 6-month study duration [22] but substantiallylower than that observed elsewhere [23]. A CochraneGroup review of 42 trials of quetiapine reporteddropout rates of 36-64%, despite the fact that mostofthe trials were short term [23]. More recently, theCATIE [24] (Clínical Antipsychotic Trials of Intervention EfIectiveness) study, reported that 74% of allpatients discontinued antipsychotic treatment before18 months; in the quetiapine group 82% of patientsdiscontinued treatment (the mean modal dose ofquetiapine was 543.4 mg/day). Although a naturalistic design, CATIE was a double-blind clínical trialand the design and duration of follow-up may haveimpacted on withdrawal rates. In addition, it wasrelatively easy for patients to switch treatments. Onecan only speculate about the reasons for this difIerence in withdrawal rates, since many factors afIecttreatment compliance. Logistic regression analysisundertaken in the present study indicated thatdropouts were associated with the use of quetiapineat doses of <400 mg/day when controlling the baseline difIerences between dose groups. This is animportant finding because, in clínical practice, withdrawal from treatment could be considered to be ameasure of treatment efIectiveness.
In clinical practice, addressing adverse events thatmay occur with antipsychotics is problematic. Several therapeutic strategies are available for themanagement of adverse events, including adjustingthe dose, using an antidote (e.g., antiparkinsonianmedications, amantadine, nizatidine, bromocriptine)or switching to another antipsychotic [1,25]. Theactual management of antipsychotic-induced side
efIects in the clinical setting is therefore an interesting matter to investigate. In the present naturalisticstudy, we found that more than two-thirds ofpatients who experienced EPS, sexual side efIects,other hormonal efIects (e.g., amenorrhoea), cognitive side efIects or sedation with their previousantipsychotic medication experienced considerableimprovement in these adverse events when switchedto quetiapine. Significant improvements in EPS havealso been reported in a previous naturalistic study inpatients with schizophrenia switched from otherantipsychotics to quetiapine [26]. Significant increases in weight have been reported for clozapineand olanzapine [27,28]. While there was a slightincrease in mean patient weight of 0.4 kg during the6-month treatment period in our study, this is amínimal change compared with that observed withclozapine and olanzapine [29,30]. In addition, inpatients who were switched to quetiapine from otherantipsychotics, weight gain was improved or verymuch improved in over 50% of patients. Furthermore, when weight gain was stratified by baselineBMI, most weight gain occurred in those who wereunderweight, whereas there was an overall reductionin weight in patients who were clínically obese.Greater increases in weight were reported in aretrospective analysis of weight change in 661patients treated with quetiapine for at least 26 weeks(mean duration of treatment = 17.8 months) [31];the mean weight change in this analysis was 2.3 kg.As observed in the present study, the greatest weightgain occurred in patients who were underweight atbase1ine, with no significant change in those whowere clínically obese. The prevalence of obesity inthe studied population would afIect the mean weightchange and could be an indirect reflection ofselective prescribing pattems in the observationalstudies.
The incidences of somnolence and asthenia in ourstudy were slightly higher than previously reportedin placebo-eontrolled trials [13,15,32], although arecent pooled analysis of eight placebo-controlledstudies reported a similar rate of somnolence(25.6%) [33]. No concomitant psychotropic medication appeared to be significantly associated with anincrease in somnolence but, as this was an uncontrolled trial, a clear relationship to quetiapine treatment could not be ascertained. Reduced libido wasthe only common (~5% of patients) sexual sideefIect reported, despite the use of concomitant drugsthat are associated with a significant increase insexual desire (anxiolytics) and orgastic dysfunction(other antipsychotics). A similar rate of reducedlibido (3.7%) was reported in another Spanishnaturalistic study in patients with schizophreniausing a difIerent evaluation method, the Psychotropic-Related Sexual Dysfunction Questionnaire [34].
Numerous naturalistic studies have been carriedout with the atypical antipsychotics, and used to
(supplement and expand on the data from randomised controlled trials [35]. The open-Iabel QUESTstudy compared the efficacy and tolerability of3 months' treatment with quetiapine or risperidonein 728 patients with psychosis [36]. The resultssuggest that overall, both agents have similar efficacyand tolerability, but that quetiapine has a morefavourable EPS profile. Similarly, in a naturalisticstudy comparing risperidone and olanzapine inpatients with first-episode schizophrenia, there weresignificant reductions in the severity of illness andpatient functioning with both agents, but the incidence of EPS was significantIy higher in the risperidone group [37]. In a large, pan-European study of8400 outpatients with schizophrenia, patients treatedwith risperidone were significantIy more likely toexperience EPS and sexual dysfunction, while patients treated with olanzapine and elozapine hadsignificantIy greater weight gain [38].
Naturalistic studies have a number of limitations.An open-Iabe1, uncontrolled, non-randomised design means that caution must be exercised wheninterpreting results and drawing conelusions. In thepresent study, investigators were requested to inelude consecutive patients; however, selection biasexists due to the lack of randomisation and becausethe study aimed to elose1yreflect elinical practice in a"real-life setting" [39]. In addition, the uncontrolleddesign of the study limits defmitive conclusions, aseffects such as regression to the mean cannot bediscounted.
Conversely, an important strength of our study isthat it is representative of clinical practice, or at thevery least, of clinical practice in Spain (the demographics and clinical characteristics of our patientsare very similar to those included in another large,naturalistic Spanish study of olanzapine [40]). Inaddition, by looking at patient characteristics (e.g.,psychiatric comorbidity, use of concomitant medications) it appears that most patients would not havebeen included in clinical trials of quetiapine nor anyother antipsychotic due to strict enrolment criteria.Our study not only supports the effectiveness ofquetiapine (measured by scales such as the BPRS,CGI, SAS and UKU, previously reported in randomised, controlled clinical trials), but also suggeststhat the efficacy and tolerability results obtained withquetiapine in carefully selected trial populationsremain valid in a naturalistic setting.
Conclusions
This study demonstrated that quetiapine was welltolerated and improved symptoms in patients duringa 6-month study in a naturalistic care setting inSpain. A quetiapine dose of <400 mglday was astrong predictor of lower BPRS changes « 30%decrease) and higher withdrawals than a dose of;::;:600mglday, suggesting that higher doses are
Naturalistic study 01quetiapine lor schizophrenia 229
associated with increased benefits. The results fromthis open-Iabel, naturalistic study indicated thatpatients with schizophrenia who were treated withquetiapine experienced symptom improvement andreduced side effects.
Key points
• The main objective of the study was to assessthe efficacy and tolerability of the atypicalantipsychotic, quetiapine, in a large representative group of patients with schizophrenia undernaturalistic conditions
• Quetiapine treatment was associated with significant and progressive improvement in overallsymptomatology at 1,3 and 6 months
• Quetiapine < 400 mglday was a strong predictorof lower BPRS changes «30% decrease) andhigher withdrawals than doses ;::;:600mglday,suggesting that higher doses are associated withincreased benefits
• Patients experienced considerable improvements in EPS on quetiapine treatment, asindicated by reduetions in SAS scores
• Weight changes that occurred during the studywere minimal, with a mean weight increasefrom baseline at 6 months of 0.4 kg
Acknowledgements
We thank Jocelyn Woodcock, MPhil, from CMC,who provided editing assistance funded by AstraZeneca.
Statement of interest
This study was supported by AstraZeneca, Madrid,Spain.
References
[1] Kane JM. Management issues in schizophrenia. London:Taylor & Francis (A Martín Dunitz Book); 2000.
[2] Barbato A. Schizophrenia and public health. World HealthOrganization, Geneva, 1998. Accessed 27 May 2005 [available at: http://www.who.intlmentaChealth!mediaJen/55.pdf).
[3] National Institute of Clínical Excellence. Schizophrenia:core interventions in the treatment and management ofschizophrenia in primary and secondary careo 2002. Accessed 27 May 2005 [available at: http://www.nice.org.uk].
[4] McEvoy ]P, Scheifler PL, Frances A. Expert ConsensusGuideline Series. Treatment of schizophrenia. J Clin Psychiatry 1999;60(Suppl 11):8-80.
[6] Fleischhacker WW, Hummer M. Do phase In trials havec1ínicalvalue? J Clin PsychopharmacoI1999;19:391-2.
[7] Norquist G, Lebowitz B, Hyman S. Expanding the frontierof treatment research. Prevention and treatment. Vol. 2,Article OOOla, 1999, posted 21 March. Accessed 27 May2005 [available at: http://www.journals.apa.org/prevention/volume2/pre002000 1a.htm1].
(
230 J Gibert et al.
[8) Awad AG. Quality of life of schizophrenic patients onmedications and implications for new drug trials. HospCornmunity Psychiatry 1992;43:262-5.
[9) Stahl SM. Selecting an atypical antipsychotic by combiningclinical experience with guidelines from clinical trials. J ClinPsychiatry 1999;60(Suppll0):31-41.
[10) Nemeroff CB, Kinkead B, Goldstein J. Quetiapine: preclinical studies, pharmacokinetics, drug interactions, anddosing. J Clin Psychiatry 2002;63(SuppI13):5-1 1.
[11) Arvanitis LA, Miller BG, and the Seroquel Trial 13 studygroup. Multiple fixed doses of "Seroquel" (quetiapine) inpatients with acute exacerbation of schizophrenia: a comparison with haloperidol and placebo. Biol Psychiatry1997;42:233-46.
[12) Borison RL, Arvanitis LA, Miller BG, and the US SeroquelStudy Group. ICI 204,636, an atypical antipsychotic:efficacy and safety in a multicenter, placebo-controlled trialin patients with schizophrenia. J Clin Psychopharmacol1996;16:158-69.
[l3) Small JG, Hirsch SR, Arvanitis LA, Miller BG, Link CGG,and the Seroquel Study Group. Quetiapine in patients withschizophrenia. A high- and low-dose double-blind comparison with placebo. Arch Gen Psychiatry 1997;54:549-57.
[14) Peuskens J, Link CGG. A comparison of quetiapine andchlorpromazine in the treatment of schizophrenia. ActaPsychiatr Scand 1997;96:265-73.
[15) Copolov DL, Link CGG, Kowalcyk B. A multicentre,double-blind, randomized comparison of quetiapine (ICI204,636, "Seroquel") and haIoperidol in schizophrenia.Psychol Med 2000;30:95-105.
[l6) Emsley RA, Raniwalla J, Bailey PJ, Jones AM, on behalf ofthe PRIZE Study Group. A comparison of the effeets ofquetiapine ("Seroquel") and haloperidol in schizophrenicpatients with a history of and a demonstrated, partialresponse to conventional antipsychotic treatment. Int ClinPsychopharmacoI2000;15:121-31.
[17) World Medical Association Declaration of Helsinki: ethicalprincipies for medical research involving human subjeets(revised 7 Oetober 2000). HIV Clin Trials 2001;2:92-5.
[l8) Overall]E, Gorham DR The Brief Psychiatric Rating Scale.Psychol Rep 1962;10:799-912.
[19) Guy W ECDEU. Assessment Manual for Psychopharmacology -Revised (DHEW Publ No ADM 76-338). Rockville,MD: US Department of Health, Education, and Welfare,Public Health Service, Alcohol, Drug Abuse, and MentalHealth Administration, NIMH Psychopharmacology Research Branch, Division of Extramural Research Ptograms;1976. p 218-22.
[20) Lingjaerde O, Ahlfors UG, Bech P, Dencker SJ, EIgen K.The UKU side effeet rating scale. A new comprehensiverating scale for psychotropic drugs and a cross-sectionalstudy of side effeets in neuroleptic-treated patients. ActaPsychiatr Scand 1987;334:1-100.
[21) A1tman DG. Practical statistics for medical research. London: Chapman and Hall; 1991.
[22) Gomez JC, Sacristan JA, Hemandez J, et al. The safety ofolanzapine compared with other antipsychotic drugs: resultsof an observational prospective study in patients withschizophrenia (EFESO Study). PharmacoepidemiologicStudy of Olanzapine in Schizophrenia. J Clin Psychiatry2000;61 :335-43.
[23) Srisurapanont M, Disayavanish C, Taimkaew K. Quetiapinefor schizophrenia. Cochrane Database ofSystematic Reviews2000; CD000967.
[24) Lieberman JA, Stroup TS, McEvoy]P, et al. Effectiveness ofantipsychotic drugs in patients with chronic schizophrenia.New Engl J Med 2005;353:1209-23.
[25) Wirshing DA, Danovitch 1, Erhart SM, Pierre JM, WirshingWC. Update on atypicals: practical tips to manage cornmonside effects. Curr Psychiatry (accessed 3 April 2004) [http://www.currentpsychiatry.coml2003_03/0303_antipsych.asp).
[26) De Nayer A, Windhager E, lrmansyah, et al. Efficacy andtolerability of quetiapine in patients with schizophreniaswitched from other antipsychotics. Int J Psychiatry ClinPraet 2003;7:59-66.
[27) AIlison DB, Mentore JL, Heo M, et al. Antipsychoticinduced weight gain: a comprehensive research synthesis.Am J Psychiatry 1999;156:1686-96.
[28) Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities. J ClinPsychiatry 1999;60:358-63.
[29) Eli Lilly and Company. Zyprexa® olanzapine tabletsIUSprescribing information. 2005 [http://pi lilIycomluslzyprexapipdf].
[30) Lamberti JS, Bellnier T, Schwarzkopf SB. Weight gainamong schizophrenic patients treated with clozapine. Am JPsychiatry 1992;149:689-90.
[31) Brecher M, Leong R, Osterling-Koskinen L, Jones M. Longterm weight change with quetiapine in schizophrenia: datareview. Poster presented at the American Psychiatric Association Annual Meeting, Atlanta, GA, USA; 2005. PosterNR262.
[32) Buckley PF. Efficacy of quetiapine for the treatment ofschizophrenia: a combined analysis of three placebo-controlled trials. Curr Med Res Opin 2004;20:1357-63.
[33) Goldstein J, Paulsson B, Sweitzer D, Zhong K. A review ofthe evidence for somnolence with quetiapine treatment.158th Annual Meeting of the American Psychiatric Association, Atlanta, GA, USA, 21-26 May; 2005. NR 259.
[34) Montejo Gonzalez AL, Rico-VilIademoros F, Tafalla M,Majadas S, Spanish Working Group for the Study ofPsychotropic-related Sexual Dysfunction. A 6-month prospective observational study on the effeets of quetiapine onsexual functioning. J Clin Psychopharmacol 2005;25:533538.
[35) Sebastian CS, Glazer W, Buckley PE Naturalistic studies ofsecond generation antipsychotics in the treatment of schizophrenia. Curr Med Chem 2004;11:329-42.
[36) MullenJ,Jibson MD, Sweitzer D, the QUEST StudyGroup.A comparison of the rclative safety, efficacy, and tolerabilityof quetiapine and risperidone in outpatients with schizophrenia and other psychotic disorders: the QuetiapineExperience with Safety and Tolerability (QUEST) study.Clin Ther 2001;23:1839-54.
[37) Montes JM, Ciudad A, Gascon J, Gomez JC, EFESO StudyGroup. Safety, effcctiveness, and quaiity of life of olanzapinein first-episode schizophrenia: a naturalistic study. ProgNeuropsychopharmacol Biol Psychiatry 2003;27:667 -74.
[38) Lambert M, Haro JM, Novick D, et al. Olanzapine vs. otherantipsychotics in actual out-patient settings: six monthstolerability results from the European Schizophrenia Outpatient Health Outcomes study. Acta Psychiatr Scand 2005;111:232-43.
[39) Tognoni G, Laporte ]R. From clinical trails to drugutiJization. In: Dukes MNG, editor. Drug utiJization studies.Methods and uses. WHO Regional Publications European:World Health Organization; 1993.
[40) Gomez JC, Sacristan JA, Hemandez J, et al. The safety ofolanzapine compared with other antipsychotic drugs: resultsof an observational prospective study in patients withschizophrenia (EFESO Study). PharmacoepidemiologicStudy of Olanzapine in Schizophrenia. J Clin Psychiatry2000;61 :335-43.
Appendix
SOS Group membersAntonio Agüera Fernández, MD; Cristina del
Álamo Jiménez, MD; Mercedes Alba Vallejo, MD;Ángeles Albarrán Barrado, MD; Jesús Alberdi Sudupe, MD; Beatriz Allue Torra, MD; Luis Almenar
(Gay, MD; Yolanda Alonso de Armiño Fernandez,MD; Susana Álvarez Avelló, MD; Luis MiguelAlvárez Carmona, MD; Pablo Álvarez Lobato,MD; César Antón Saiz, MD; Enrique Aragués Ortizde Zárate, MD; Juan José Arechederra Aranzadi,MD; José Ramón Arteaga Darías, MD; JavierAztarain Diez, MD; José Vicente Baeza Alemán,MD; Maria Montserrat Bañuelos Piñol, MD; IvánBaques Rebull, MD; Concepció Bardoleti Casas,MD; Ignacio Basurte Villamor, MD; Miguel Bautista Parraga, MD; Francisco Bellver Fradas, MD;CarIes Berche Cruz, MD; José Manuel BertolinGuillén, MD; José Javier Blanco Blanco, MD; JoanManuel Blanqué López, MD; Moisés Bolívar Peralvarez, MD; Antonio Bordallo Aragón, MD; JuanF. Bort Ruiz, MD; David Busse i Olivé, MD; PedroBustos de Abajo, MD; Carmen Busuldo Vega, MD;Arturo Cabezas Sánchez, MD; Rodrigo CabreraGárate, MD; Joan Cadevall Dieguez, MD; RománCalabuig Crespo, MD; Manuel Camacho Muñoz,MD; José María Cámara Teruel, MD; ManuelCamarero Candela, MD; Rossend Camon Solsona,MD; Mateo Campillo Agusti, MD; SalustianoCampos Velázquez, MD; Jose Cañete Crespillo,MD; José Carmona Calvo, MD; Carlos CarmonaPalau, MD; Esther Carrasco Parrado, MD; AlfonsoCasas Losada, MD; Ma Rosario Cejas Méndez,MD; Ramón Collado Bayona, MD; Jesús M. CuestaBascones, MD; Pastora Cuevas Muñoz, MD; Miguel Ángel Cuquerella Benavent, MD; Amando deBernardo Barrio, MD; José de BIas Soto, MD;Consuelo de Dios Perrino, MD; Jaime de La TorreHernández, MD; Ma Teresa de Lucas Taracena,MD; Miguel Ángel de Uña Mateos, MD; Tomás deVicente Muñoz, MD; José Francisco Delgado González, MD; Antonio Delgado Martel, MD; JuanCarlos Diaz del Valle, MD; Marina Diaz Marsá,MD; Francisco Doce Feliz, MD; Jordi DomingoRibas, MD; María Echeveste Portugal, MD; NabilEl Jada Qawashi, MD; Vicente Elvira Cruañes, MD;Ma Luisa Embid Martin, MD; BIas Erkizia Amiliria,MD; Manuel Espiñeira Álvarez, MD; José VicenteEstalrich Canet, MD; Jose Antonio FernándezBenítez, MD; Juan Fernández Hierro, MD; LuisFernández Menéndez, MD; José Luis FernándezSastre, MD; Andrés Fernández-Cuevas Vicario,MD; Isabel Florez Fernández, MD; Eva FontovaCarbonell, MD; Joan Franch Barcelo, MD; IsabelFreire Santos, MD; Ma Asunción Fresno Gonzalez,MD; Javier Frometa Pérez, MD; Antonio GalbisOlivares, MD; José Mariano Galletero López, MD;Alberto Gangoiti Gurtubay, MD; Juan Carlos García Álvarez, MD; Javier García Campayo, MD; JuanAntonio García Mellado, MD; Blanca García Montañez, MD; Gorka García Serrano, MD; Ma JesúsGarrido Machiñena, MD; Jose Gascon Barrachina,MD; Francisco Gazquez Martinez, MD; MiguelGelabert Camarasa, MD; Susana Gil Flores, MD;Patxi Gil López, MD; Mar Gil Villa, MD; Angel
Naturalistic study o/ quetiapine /or schizophrenia 231
Gilabert Senar, MD; José Manuel Giménez García,MD; Juan Carlos Giménez Morales, MD; JoséGimillo Asensio, MD; Josep M. Giralt Coll, MD;María José Gómez del Castillo, MD; Isidro GómezPérez, MD; Felisa Gómez Robina, MD; EstherGómez Rodriguez, MD; Gixane González García,MD; Antonio P. González González, MD; FelixAndrés González Lorenzo, MD; Emilio GonzálezPablos, MD; Lidia González Segura (Residente),MD; Ana Isabel González Vázquez, MD; MicaelaGonzález-Quiros Menéndez de Luarca, MD; EvaGracia Peligero, MD; Oded Graizer Rebhuhn, MD;Basilia Guerra Amador, MD; Antonio GuerreroRomero, MD; Joaquin Guinart Prados, MD; AlbertGuiral Torner, MD; Miguel ÁngelHaza Duaso, MD;Miguel Ángel Hernández Lasheras, MD; Jose LuisHernández Fleta, MD; Cristina Hernández Herrero,MD; Miguel Hernández Viadel, MD; Jose HerreraArroyo, MD; Oscar Herreros Rodriguez, MD; Carmen Hidalgo Moratal, MD; Raúl Guillermo IbáñezCorrales, MD; Lorenzo Iglesias, MD; Celso IglesiasGarcía, MD; Ma Laura Iglesias Victor, MD; JoseManuel Jaquotot Arnaiz, MD; Fernando JiménezMazo, MD; Luis María Larrazabal Salazar, MD; Ma
Teresa Lázaro Casasus, MD; Jon Lizárraga Sobrino,MD; Patricia Uorens Rodríguez, MD; Francisco JLópez Ibor Aliño, MD; Ángeles López López, MD;Juan José López Plaza, MD; Luis López Sánchez,MD; Rufino Losantos Pascual, MD; Elena LozanoSan Martin, MD; José Ángel Macías Fernández,MD; Iñaki Madariaga Zamalloa, MD; Pedro Malabia Lieb, MD; Juan José Mancheño Barba, MD; JoséFelix Marcos Frías, MD; Enrique Marcos González,MD; José Luis Marín Morales, MD; Manel Márquez Rowe, MD; Félix Martin Herguedas, MD;Rafael Martin Muñoz, MD; Sara Martinez Barrondo, MD; Antonio Martinez Fernández, MD; JoséLuis Martinez Fernández, MD; Ricardo MartinezGallardo, MD; Manuel Martinez García de Castro,MD; Miguel Martinez Roig, MD; Adolf Mas-Yebra iReverter, MD; Teresa Mayans Vázquez, MD; Sacramento Mayoral Moyano, MD; Pedro AntonioMegia López, MD; Desiderio Mejias Verdú, MD;Roger Mercade Sales, MD; María Jesús MerinoGarcía, MD; Luis Minguez Martin, MD; RamónMira Sempere, MD; Juan José Molina Castillo, MD;José María Mongil San Juan, MD; Ángel LuisMontejo González, MD; Jose Luis Montero Horche,MD; José Manuel Montes Rodríguez, MD; MaríaIsabel Montes Santana, MD; Ma Virtudes MoralesContreras, MD; Carmen Rosa Morales García, MD;José Luis Morell Ocaña, MD; Crístina MorenoCorona, MD; Pablo Luis Moreno Flores, MD; JesúsMorillas Ariño, MD; Carlos Morillo-Velarde Quintero, MD; José Antonio Muñoz Martinez, MD; J.Javier Mz. de Morentin Barajoan, MD; Maria Carmen Natividad Hernández, MD; Rafael NavarroPichardo, MD; Sergio Ocio León, MD; José ManuelOlivares Diez, MD; Jorge Alejandro Oliver Paez,