The University of Sydney Page 1 Interpretation of corneal tomography Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales
Transcript
The University of Sydney Page 1
Interpretation of corneal
tomography
Presented by
Chameen Samarawickrama- Westmead Hospital
- Liverpool Hospital
- University of Sydney
- University of New South Wales
The University of Sydney Page 2
Financial disclosures
– Early Career Research Fellowship (Westmead Charitable Trust)
The University of Sydney Page 3
Uses of corneal tomography
– Cataract
– Toric IOL insertion
– Lens densimetry
– Post-refractive IOL calculations
– Limbal relaxing incisions
– Cornea/refractive
– Ectasias
– Intra-corneal ring segments
– Corneal graft planning
– Ocular surface diseases
– Pterygia
– Scars
– Salzman nodules
– Glaucoma
– Anterior chamber depth
– Angle estimation
The University of Sydney Page 4
Torics at Westmead
– Westmead Hospital Audit
Aug – Oct 2016
– 22 ophthalmologists
– 5 registrars
– 2 fellows
– 22 toric IOL
– Pre-op cyl: 1.61 ± 0.9
– Post-op cyl: 1.23 ± 0.23
Pre-op cyl Post-op cyl Change
4.25 -1.75 -6
-3.50 -1.25 2.25
-1.5 -1 0.5
2.5 0 -2.5
2.25 -1 -3.25
-3 -1.75 1.25
-1.25 -3 -1.75
1.75 -0.75 -2.5
3.5 -3.25 -6.75
1 -0.50 -1.5
2 -0.50 -0.25
1.25 -1.0 -2.25
2 -1.0 -3
2.25 -0.75 -3
1.25 -0.5 -1.75
1 -1 -2
The University of Sydney Page 5
Introduction of a
toric pathway
– Regular astigmatism
– Even bow tie pattern
– Axis of astigmatism
– Match within 15 deg
– Power of astigmatism
– Match within 0.5D
The University of Sydney Page 6
Power of appropriate utilization of tomography
– Feb – April 2018
– 29 torics (25 followed pathway)
– By 1 month
– 26 of 29 had uncorrected vision of 6/12 or better
– 21 (78%) had SER within 0.5D of target
Mean preop versus postop cylinder
Available
data n = 34 Preoperative
1 Month Postoperative
P-value
Refractive Cylinder (D)
Mean ± SD Range
2.77 ± 1.48 1.75 to 5.12
0.89 ± 0.96 0 to 1.75
0.006
The University of Sydney Page 7
Aims
1. Understand differences between tomography and topography
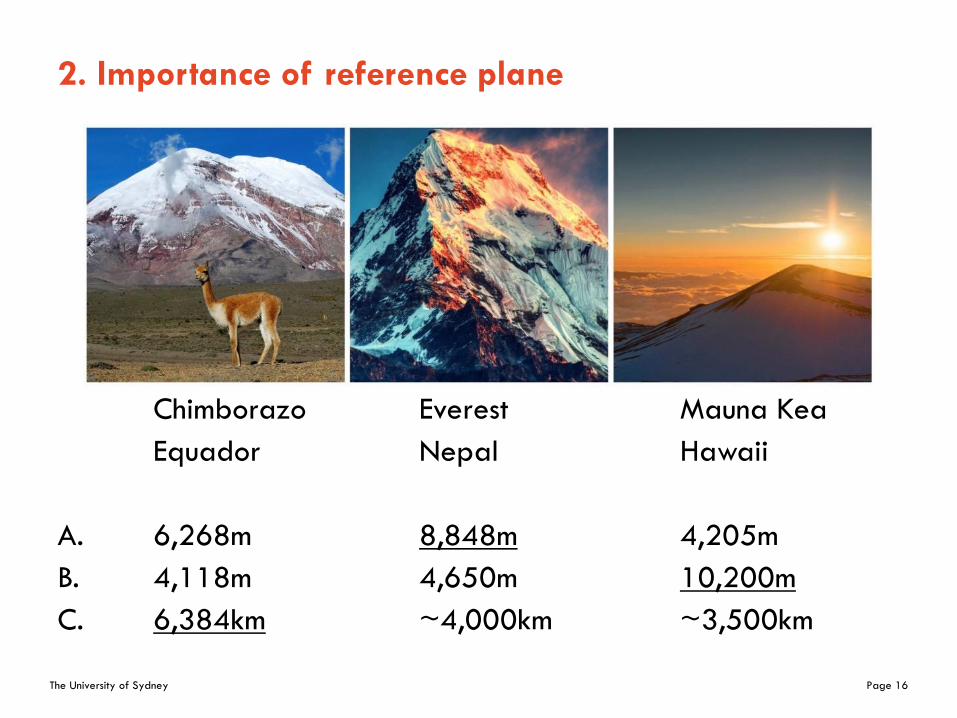
2. Reference plane and standardized settings
3. Systematically read tomography maps
4. Examples of common pathologies
5. Specific maps that are useful for diagnosis of ectasia