20
INSTITUTE OF OCCUPATIONAL MEDICINE . Edinburgh . UK www.iom-world.org Interpretation of dermal exposure measurements & model outputs John Cherrie
| Date post: | 28-Jan-2018 |
| Category: |
Health & Medicine |
| Upload: | oh-world |
| View: | 54 times |
| Download: | 0 times |
INSTITUTE OF OCCUPATIONAL MEDICINE . Edinburgh . UK www.iom-world.org
Interpretation of dermal exposure measurements
& model outputs
John Cherrie
Summary…
• Methodological and quality issues
• Contextual information
• Data analysis, what do the results mean?
What do we assess?
• Interception measurements assess cumulative amount of contaminant on skin
• In many cases they are unrealistic
• Removal samples recover what’s left
• They are more realistic but may underestimate because of losses
• Fluorescent monitoring is useful for assessing the area exposed
• May overestimate mass for reasons similar to interception sampling
• Biological monitoring integrates all routes
• It is difficult to interpret for this reason
Models…
• Dermal exposure models are generally poor at estimating exposure
• Generally overestimate exposure
• May be best for screening
• Multiple independent assessments reduces variability
• DREAM / Gulf DREAM are useful for assessing possible impacts of controls
• Conceptual model can help understanding

Measurements…
• No real standardisation of methods
• Quality assurance procedures are necessary, e.g. assessment of recovery efficiency
• Interception samplers will give results that may be an order of magnitude higher than recovery samples
• Preliminary data from Gorman-Ng et al
Ng, M. G., de Poot, S., Schmid, K., Cowie, H., Semple, S., & Van Tongeren, M. (2014). A preliminary
comparison of three dermal exposure sampling methods: rinses, wipes and cotton gloves. Environmental
Science: Processes & Impacts, 16(1), 141–147.
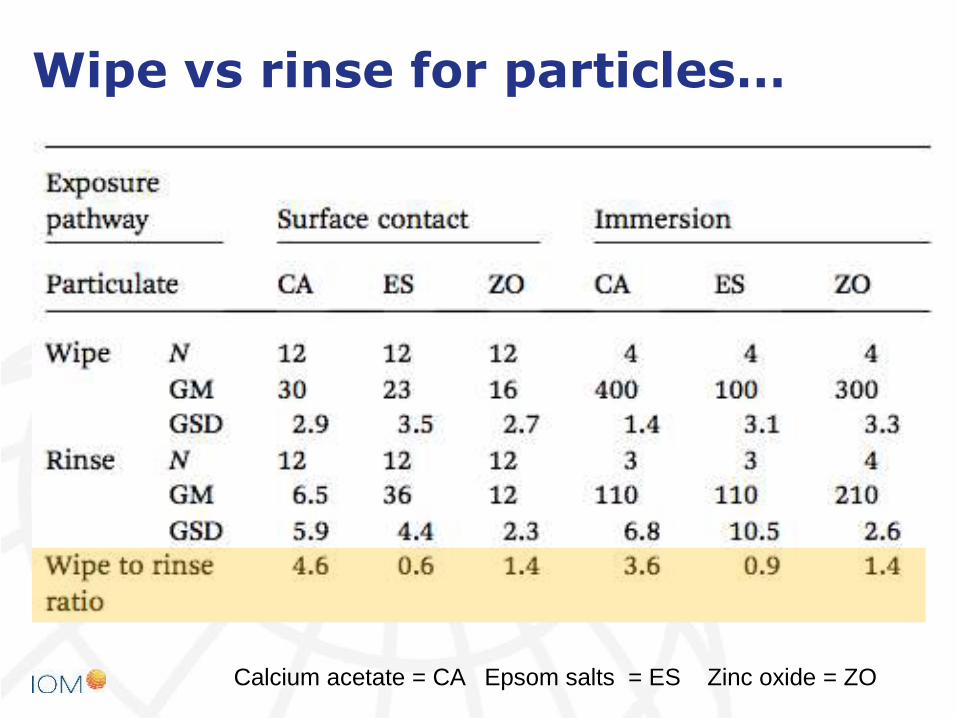
Wipe vs rinse for particles…
Calcium acetate = CA Epsom salts = ES Zinc oxide = ZO
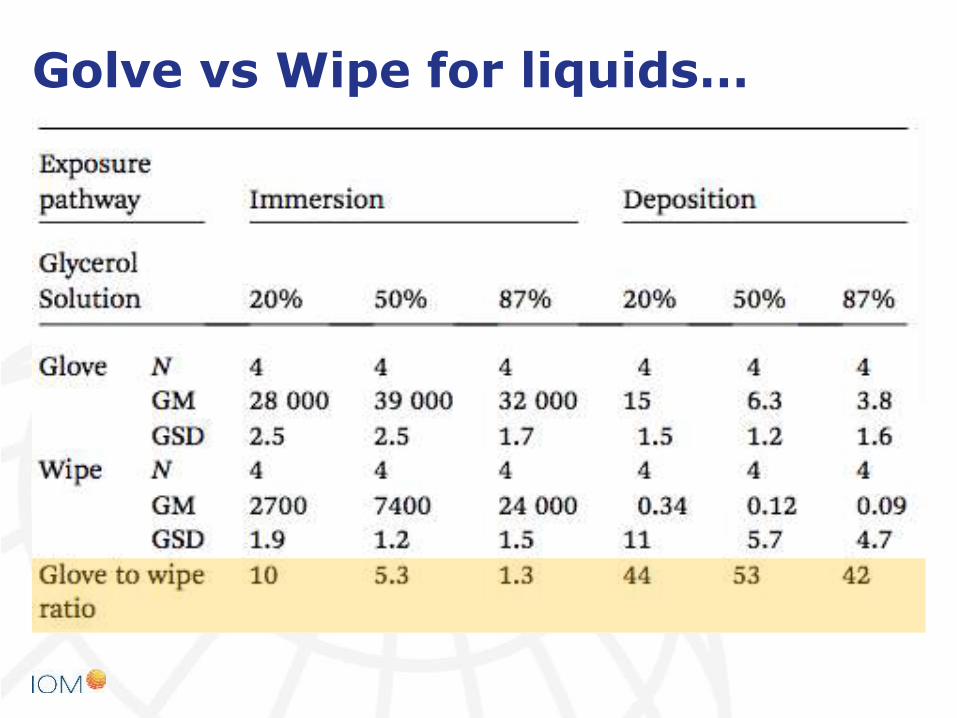
Golve vs Wipe for liquids…
Contextual data…
• Contextual data are necessary to properly interpret measurements or modelled exposure
• The conceptual model from Schenider et al helps guide what data should be collected
• Use of the model to map out the exposure pathways can be helpful
• Linking to air concentrations and surface samples can further help quantify pathways
• Plan measurement survey using the conceptual model

Interpretation of risks…
• We do not generally have a dermal OEL
• Main exception are REACH dermal DNELs
• We can generate a pseudo OEL for skin exposure from the inhalation OEL, e.g. assuming a certain inhaled air volume for the working day
• If OEL is 10 mg/m3 and the worker inhales 10 m3 in the working day then then she will inhale 100 mg of the contaminant
An example…
• Heavy fuel oil (HFO): blended hydrocarbon residues from refinery distillation and cracking processes
• High MW compounds: aromatic, aliphatic and naphthenic hydrocarbons, along with asphaltenes and some heterocyclic compounds containing sulphur, nitrogen and oxygen
• UK crude is predominantly from the North Sea A barrel of North Sea crude oil will usually yield about 12% of HFO
What are the health concerns?
• Prolonged repeated contact with the skin may cause:
• oil acne
• oil folliculitis
• dermatitis.
• HFOs contains compounds that may cause skin cancer, including benzo(a)pyrene and other polycyclic aromatic hydrocarbons (PAHs)
11
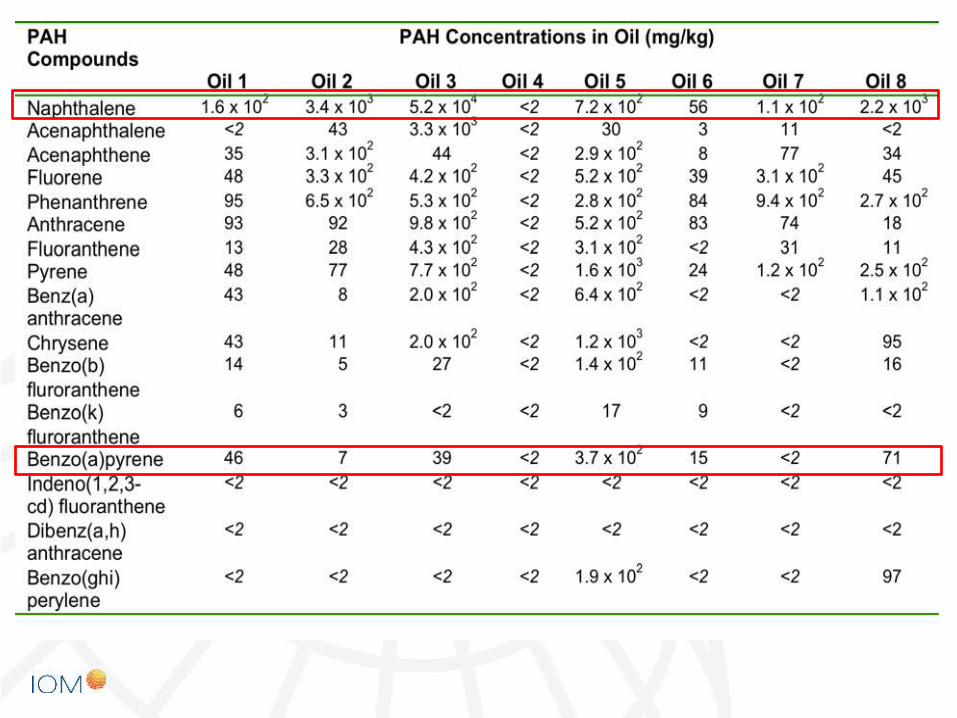
Composition…
Aims of our study…
• To develop a validated method for measuring dermal HFO exposure
• To collect exposure data using the validated method
• To collect contextual exposure information and use these data to apply the DREAM model
Methods…
• Removal method using clinical wipes saturated with 70% isopropyl alcohol –three sequential wipes
• 25 cm2 forearm and neck
• Palms of each hand
• Collected following the completion of task and before rest breaks
• Some pre-task samples also collected
• Filed blanks
• GG-MS analysis for marker PAHs
14
Sites investigated…
• Production
• 2 oil refineries
• Distribution
• 2 fuel distribution terminals
• including 1 associated with distribution by shipping
• Use
• 2 Energy providers
• 1 Power plant engine building and repair
15

Dermal exposure by activity…
Hands
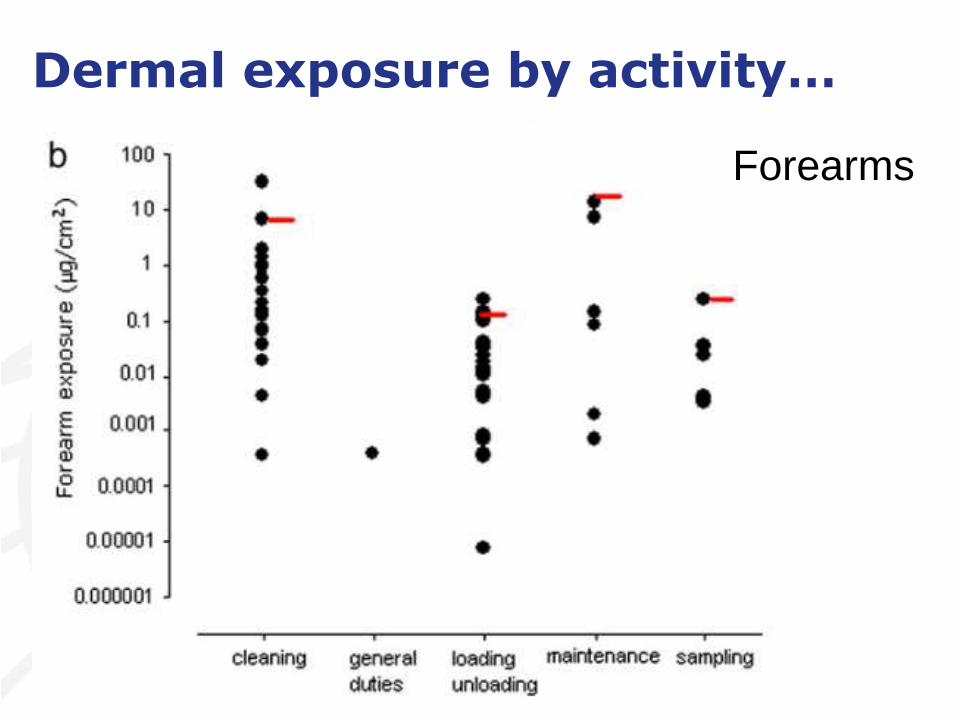
Dermal exposure by activity…
Forearms
How do we interpret these data?
• Exposure levels much lower than predicted by ECETOC TRA
• Assuming the area of hands and arms is 3700 cm2
• Maximum mass of HFO on skin is then around 37 mg
• For comparison workers machining metal typically were exposed to 1400 –1600 mg MWF on hands
DNEL
• Target organ and developmental effects are associated with the types and levels of aromatic constituents
• 8hr dermal DNEL for HFO 0.065 mg/kg, which for a 70kg man would be 4.5 mg
• Maximum exposure 37 mg HFO
• Flux estimated for naphthalene as 0.45 x 10-3 mg/cm2/hr
• 1.6 mg naphthalene could be taken up in 1hr
Jakasa, I., Kezic, S., & Boogaard, P. J. (2015). Dermal uptake of petroleum substances.
Toxicology Letters, 1–17.

Summary…
• Interpretation of dermal exposure measurements is not straightforward
• There is no standardisation and generally no limit values to compare with
• You need to be a bit creative to come to some appropriate conclusions

















