Technical Developments and Instrumentation Interventional Techniques to Shorten and Lengthen Central Venous Catheters to Preserve Edward A. Lebowitz, MD Patricia E. Burrows, MD Frederic A. Hoffer, MD Taylor Chung, MD Index terms: Catheters and catheterization, central venous access, 9462.1269,9462.458 In- terventional procedures, in infants and children, 9462.1269,9462.458 JVIR 1996; 7:441444 From the Department of Radiology, The Children's Hospital, Boston, MA. Received Octo- ber 18,1995; revision requested November 16; re- vision received February 23, 1996; accepted Feb- ruary 26. Address correspondence to E.A.L., Department of Diagnostic Imaging, Santa Clara Valley Medical Center, 751 S Bascom Ave, San Jose, CA 95128. O SCVIR, 1996 With increasing use uf long-term cath- eters for central venous access, associ- ated complications are increasingly prevalent 11-3). When long-term venous access is required, catheter function is preserved when possible to slow the progressive loss of venous access sites (4). The purpose of the present article is to report the results in two patients in whom interventional techniques were used to shorten and lengthen central venous catheters in order to preserve their function. I CASE REPORTS Case 1. Central venous catheter short- ening.- A boy who is 9 years 1 month of age has required central venous access for parenteral nutrition from 5 months of age until the present. By 5 years 5 months of age, the patient had devel- oped bilateral subclavian venous occlu- sion and superior vena caval stenosis. At this time, a central venous catheter was placed by operative insertion through the right greater saphenous vein with a subcutaneous tunnel from the anterior abdominal wall. This was subsequently exchanged twice, with the latest cath- eter a 7-F, double-lumen, Silastic (Dow Corning, Midland, Mich) Hickman cath- eter. At 8 years 8 months of age, the pa- tient presented with a 5-day history of right abdominal and flank pain, and a 2- 3-week history of difficulty infusing medications and inability to obtain blood return through the catheter. At that time, no blood could be aspirated from either lumen of the catheter, and the right-sided abdominal and flank pain could be elicited with infusion through the catheter. An abdominal radiograph and subsequent ultrasound (US) scan demonstrated the catheter tip in the right renal vein (Fig la). The interven- tional radiology service was consulted to confirm the position of the catheter and to try to reposition its tip in the inferior vena cava. Following induction of general anes- thesia, both groins and the exlcriorizcd portion of the Hickman catheter were prepared and draped with use of sterile technique. No prophylactic antibiotics were administered. Contrast material injections demonstrated that both cath- eter lumens were patent and eonfinned that the catheter tip was in a branch of the right renal vein. The Ieft common femoral vein was then catheterized with a 5-F sheath. Through the sheath, a 5-F pigtail catheter was advanced into the inferior vena cava, and an inferinr vena cavogram was obtained. This showed no evidence of inferior vena caval thrombo- sis. The tip of the pigtail calheler was then used to snare the Hickman cath- eter, which was then pulled into the in- ferior vena cava, where it immediately assumed the proper position with its tip a t the junction of the inferior vena cava and right atrium (Fig lbi. Two weeks later, the patient pre- sented with recurrent right abdominal and flank pain. A contrast material in- jection again demonstrated that the Hickman catheter was malpositioned in the right renal vein. Replacing the exist- ing catheter with one that did not have the "memory" of the malposition in the right renal vein was considered. How- ever, because of difficulty encountered in passing the existing catheter into the in- ferior vena cava when it was originally inserted, the surgeon preferred that we shorten the catheter rather than at- tempt another complete exchange. A Doppler US examination demon- strated patency with some narrowing of the right common femoral vein. Follow- ing induction of general anesthesia, the right groin was prepared and draped. No antibiotics were administered. The right femoral vein was catheterized percuta- neously with an 11-F sheath. The central venous catheter was snared by using a 4-F cobra catheter as a guide for a 2.5-F urological basket snare device (Cook, Bloomington, Ind) The tip of the Silastic Hickman catheter was then exteriorized by withdrawing it through the sheath.
Transcript
Technical Developments and Instrumentation
Interventional Techniques to Shorten and Lengthen Central Venous Catheters to Preserve
Edward A. Lebowitz, MD Patricia E. Burrows, MD Frederic A. Hoffer, MD Taylor Chung, MD
Index terms: Catheters and catheterization, central venous access, 9462.1269,9462.458 In- terventional procedures, in infants and children, 9462.1269,9462.458
JVIR 1996; 7:441444
From the Department of Radiology, The Children's Hospital, Boston, MA. Received Octo- ber 18,1995; revision requested November 16; re- vision received February 23, 1996; accepted Feb- ruary 26. Address correspondence to E.A.L., Department of Diagnostic Imaging, Santa Clara Valley Medical Center, 751 S Bascom Ave, San Jose, CA 95128.
O SCVIR, 1996
With increasing use uf long-term cath- eters for central venous access, associ- ated complications are increasingly prevalent 11-3). When long-term venous access is required, catheter function is preserved when possible to slow the progressive loss of venous access sites (4). The purpose of the present article is to report the results in two patients in whom interventional techniques were used to shorten and lengthen central venous catheters in order to preserve their function.
I CASE REPORTS
Case 1. Central venous catheter short- ening.- A boy who is 9 years 1 month of age has required central venous access for parenteral nutrition from 5 months of age until the present. By 5 years 5 months of age, the patient had devel- oped bilateral subclavian venous occlu- sion and superior vena caval stenosis. At this time, a central venous catheter was placed by operative insertion through the right greater saphenous vein with a subcutaneous tunnel from the anterior abdominal wall. This was subsequently exchanged twice, with the latest cath- eter a 7-F, double-lumen, Silastic (Dow Corning, Midland, Mich) Hickman cath- eter.
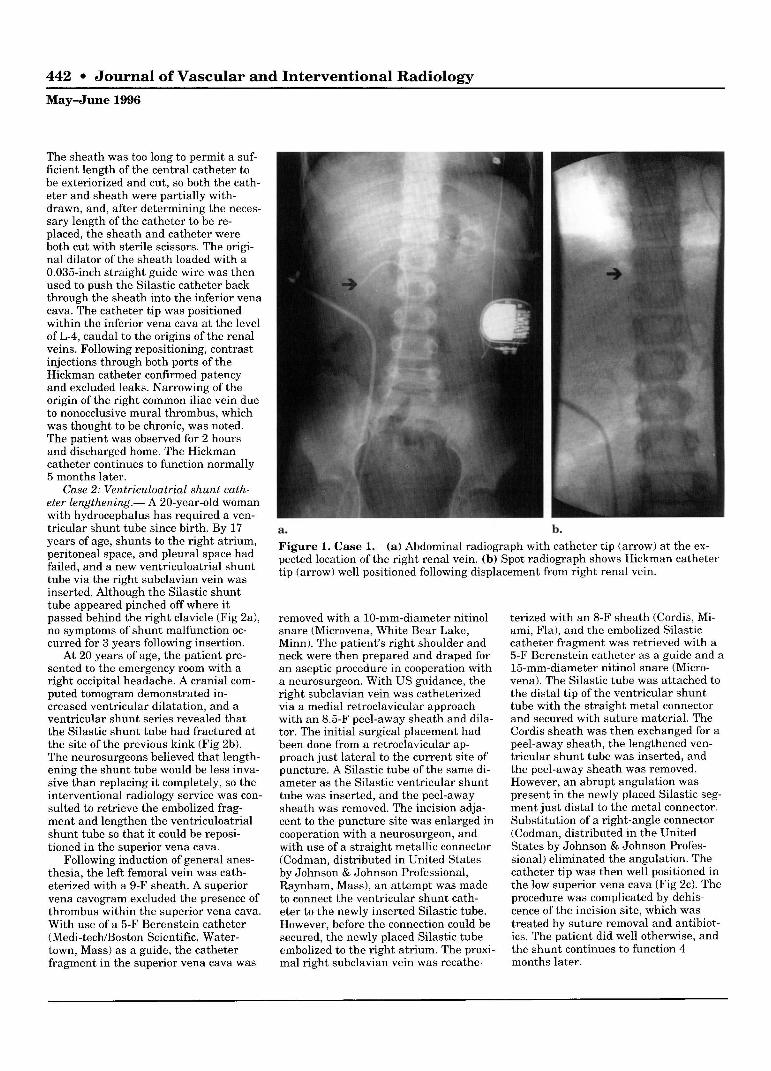
At 8 years 8 months of age, the pa- tient presented with a 5-day history of right abdominal and flank pain, and a 2- 3-week history of difficulty infusing medications and inability to obtain blood return through the catheter. At that time, no blood could be aspirated from either lumen of the catheter, and the right-sided abdominal and flank pain could be elicited with infusion through the catheter. An abdominal radiograph and subsequent ultrasound (US) scan demonstrated the catheter tip in the right renal vein (Fig la) . The interven- tional radiology service was consulted to confirm the position of the catheter and to try to reposition its tip in the inferior vena cava.
Following induction of general anes- thesia, both groins and the exlcriorizcd portion of the Hickman catheter were prepared and draped with use of sterile technique. No prophylactic antibiotics were administered. Contrast material injections demonstrated that both cath- eter lumens were patent and eonfinned that the catheter tip was in a branch of the right renal vein. The Ieft common femoral vein was then catheterized with a 5-F sheath. Through the sheath, a 5-F pigtail catheter was advanced into the inferior vena cava, and an inferinr vena cavogram was obtained. This showed no evidence of inferior vena caval thrombo- sis. The tip of the pigtail calheler was then used to snare the Hickman cath- eter, which was then pulled into the in- ferior vena cava, where it immediately assumed the proper position with its tip a t the junction of the inferior vena cava and right atrium (Fig lbi.
Two weeks later, the patient pre- sented with recurrent right abdominal and flank pain. A contrast material in- jection again demonstrated that the Hickman catheter was malpositioned in the right renal vein. Replacing the exist- ing catheter with one that did not have the "memory" of the malposition in the right renal vein was considered. How- ever, because of difficulty encountered in passing the existing catheter into the in- ferior vena cava when it was originally inserted, the surgeon preferred that we shorten the catheter rather than at- tempt another complete exchange.
A Doppler US examination demon- strated patency with some narrowing of the right common femoral vein. Follow- ing induction of general anesthesia, the right groin was prepared and draped. No antibiotics were administered. The right femoral vein was catheterized percuta- neously with an 11-F sheath. The central venous catheter was snared by using a 4-F cobra catheter as a guide for a 2.5-F urological basket snare device (Cook, Bloomington, Ind) The tip of the Silastic Hickman catheter was then exteriorized by withdrawing it through the sheath.
442 Journal of Vascular ant
May-June 1996
The sheath was too long to permit a suf- ficient length of the central catheter to be exteriorized and cut, so both the cath- eter and sheath were partially with- drawn, and, after determining the neces- sary length of the catheter to be re- placed, the sheath and catheter were both cut with sterile scissors. The origi- nal dilator of the sheath loaded with a 0.035-inch straight guide wire was then used to push the Silastic catheter back through the sheath into the inferior vena cava. The catheter tip was positioned within the inferior vena cava a t the level of L-4, caudal to the origins of the renal veins. Following repositioning, contrast injections through both ports of the Hickman catheter confirmed patency and excluded leaks. Narrowing of the origin of the right common iliac vein due to nonocclusive mural thrombus, which was thought to be chronic, was noted. The patient was observed for 2 hours and discharged home. The Hickman catheter continues to function normally 5 months later.
Case 2: Ventriculoatrial shunt cath- eter lengthening.- A 20-year-old woman with hydrocephalus has required a ven- tricular shunt tube since birth. By 17 years of age, shunts to the right atrium, peritoneal space, and pleural space had failed, and a new ventriculoatrial shunt tube via the right subclavian vein was inserted. Although the Silastic shunt tube appeared pinched off where it passed behind the right clavicle (Fig 2a), no symptoms of shunt malfunction oc- curred for 3 years following insertion.
At 20 years of age, the patient pre- sented to the emergency room with a right occipital headache. A cranial com- puted tomogram demonstrated in- creased ventricular dilatation, and a ventricular shunt series revealed that the Silastic shunt tube had fractured at the site of the previous kink (Fig 2b). The neurosurgeons believed that length- ening the shunt tube would be less inva- sive than replacing it completely, so the interventional radiology service was con- sulted to retrieve the embolized frag- ment and lengthen the ventriculoatrial shunt tube so that it could be reposi- tioned in the superior vena cava.
Following induction of general anes- thesia, the left femoral vein was cath- eterized with a 9-F sheath. A superior vena cavogram excluded the presence of thrombus within the superior vena cava. With use of a 5-F Berenstein catheter (Medi-tech/Boston Scientific, Water- town, Mass) as a guide, the catheter fragment in the superior vena cava was
d Interventional Radiology
a. b. Figure 1. Case 1. (a) Abdominal radiograph with catheter tip (arrow) a t the ex- pected location of the right renal vein. (b) Spot radiograph shows Hickman catheter tip (arrow) well positioned following displacement from right renal vein.
removed with a 10-mm-diameter nitinol snare (Microvena, White Bear Lake, Minn). The patient's right shoulder and neck were then prepared and draped for an aseptic procedure in cooperation with
A
a neurosurgeon. With US guidance, the right subclavian vein was catheterized - via a medial retroclavicular approach with an 8.5-F peel-away sheath and dila- tor. The initial surgical placement had been done from a retroclavicular ap- proach just lateral to the current site of puncture. A Silastic tube of the same di- ameter as the Silastic ventricular shunt tube was inserted, and the peel-away sheath was removed. The incision adja- cent to the puncture site was enlarged in cooperation with a neurosurgeon, and with use of a straight metallic connector (Codman, distributed in United States by Johnson & Johnson Professional, Raynham, Mass), an attempt was made to connect the ventricular shunt cath- eter to the newly inserted Silastic tube. However, before the connection could be secured, the newly placed Silastic tube embolized to the right atrium. The proxi- mal right subclavian vein was recathe-
terized with an 8-F sheath (Cordis, Mi- ami, Fla), and the embolized Silastic catheter fragment was retrieved with a 5-F Berenstein catheter as a guide and a 15-mm-diameter nitinol snare (Micro- vena). The Silastic tube was attached to the distal tip of the ventricular shunt tube with the straight metal connector and secured with suture material. The Cordis sheath was then exchanged for a peel-away sheath, the lengthened ven- tricular shunt tube was inserted, and the peel-away sheath was removed. However, an abrupt angulation was present in the newly placed Silastic seg- ment just distal to the metal connector. Substitution of a right-angle connector (Codman, distributed in the United States by Johnson & Johnson Profes- sional) eliminated the angulation. The catheter tip was then well positioned in the low superior vena cava (Fig 2c). The procedure was complicated by dehis- cence of the incision site, which was treated by suture removal and antibiot- ics. The patient did well otherwise, and the shunt continues to function 4 months later.
Lebowitz et a1 443
Volume 7 Number 3
a. b. C.
Figure 2. Case 2. (a) Chest radiograph obtained following ventriculoatrial shunt procedure a t 17 years of age. Note that new Silastic shunt tube is pinched off (single black arrow). Course of the shunt in the right subclavian vein is difficult to visualize but is demarcated by open white arrows. An old catheter fragment within a chronically occluded right internal jugular vein (white arrowheads) and a metal connector from a n abandoned ventricular shunt within the chest wall (double black arrows) are also visible. (b) Chest radiograph obtained a t 20 years of age on presentation with shunt malfunction. Silastic shunt tube has frac- tured where i t had previously been pinched off (large arrow). The distal fragment was lodged in the superior vena cava and was easily visible a t fluoroscopy. The old catheter fragment (arrowheads) and metal connector (small arrows) are still present. ( c ) Chest radiograph obtained 1 month after the procedure with right-angle connector eliminating catheter angulation and the catheter tip in low superior vena cava (arrow). The old catheter fragment and metal connector noted above are still present.
1 DISCUSSION
Catheter malposition, compression, fracture, and embolization are well- known complications of central venous access (1-5). Standard treatment for the cases reported here would have been catheter removal and replacement. However, both of the patients had chronic conditions requiring long-term venous access and had previously re- quired numerous operative catheter changes. The surgeons responsible for their care did not believe tha t operative treatment would have been straightfor- ward, and requested that the interven- tional service consider other solutions.
The interventional techniques re- ported herein are simple modifications of standard vascular access procedures. The metal connectors and Silastic tub- ing used to lengthen the ventricular shunt are standard operating room sup- plies and are easily obtained. Remain-
ing supplies are routinely available in the interventional laboratory. To our knowledge, however, neither of these interventions has been reported previ- ously.
A difficulty encountered in shorten- ing the malpositioned Hickman catheter was caused by using a sheath that was too long. Shortening the sheath prior to inserting i t into the right femoral vein would have permitted the catheter to be withdrawn and cut without having to cut a segment of the hub end of the sheath. Figure 3 illustrates the pre- ferred technique.
A difficulty encountered in lengthen- ing the ventriculoatrial shunt was loss of the newly placed catheter segment into the right subclavian vein before a secure connection with the proximal segment was made. Connecting the old catheter to the new one prior to placing i t into the subclavian vein would have been safer, and this is what we did in our second attempt. Abrupt angulation
of the catheter was resolved with use of a right-angled connector. Obviously, both straight and right-angled connec- tors should be available.
Fracture and embolization of the ventricular shunt were probably caused by shearing forces similar to those of pinch-off syndrome, which occurs when a subclavian venous catheter passes through the tight anterior portion of the costoclavicular space before entering the vein too medially (5). Catheter pinch-off in our patient occurred poste- rior to a bony process extending from the clavicle toward the coracoid process, well lateral to the usual site, and was apparently due to bony and ligamentous structures a t this location (6). The ulti- mate occurrence of catheter fracture and embolization, however, further sup- port the suggestion that catheters be re- placed, or in this case revised, upon ra- diographic recognition of pinch-off syn- drome, even in the absence of obvious malfunction (5).
444 Journal of Vascular and Interventional Radiology May-June 1996
Figure 3. Diagrammatic illustration of preferred catheter shortening procedure. (a) Venous catheter is snared from ectopic po- sition and pulled into the sheath. Note that sheath is shortened before i t is inserted into the femoral vein. (To avoid confusing overlap, the entry site of the catheter into the greater saphenous vein has been drawn laterally rather than medially.) (b) The exteriorized catheter is cut. ( c ) The remaining portion of the venous catheter is reinserted by pushing it with the guide wire-di- lator combination. (d) The remaining portion of the venous catheter is shown in proper position.
References 1. Mitchell SE, Clark RA. Complications of
central venous catheterization. AJR 1979; 133:467-476.
2. Cassidy F P J r , Zajko AB, Bron KM, Reilly JJ Jr , Peitzman AB, Steed DL. Noninfec- tious complications of long-term central venous catheters: radiologic evaluation and management. AJR 1987; 149:671-675.
3. Wechsler FLJ, Spirn PW, Conant EF, 5. Hinke DH, Zandt-Stastny DA, Goodman Steiner RM, Needleman L. Thrombosis LR, Quebbeman EJ, Krzywda EA, Andris and infection caused by thoracic venous DA. Pinch-off syndrome: a complication catheters: pathogenesis and imaging find- of implantable subclavian venous access ings. AJR 1993; 160:467471. devices. Radiology 1990; 177:353-356.
4. Lund GB, Lieberman RP, Haire WD, 6. Cockshott WP. The coracoclavicular Martin VA, Kessinger A, Armitage JO. joint. Radiology 1979; 131:313-316. Transluminal inferior vena cava catheters for long term venous access. Radiology 1990; 174:31-35.