Intraocular lens implantation in infants with congenital cataracts - Abhay Vasavada, M.S., F.R.C.S., Harsha Chauhan, M.S.(Ophth.) ABSTRACT We evaluated 21 eyes of 13 infants between two and eight months old who had primary posterior chamber intraocular lens (IOL) implantation for congenital cat- aracts between 1988 and 1993. Twelve eyes had a posterior capsulorhexis or plaque peeling at the time of implantation and one eye had a vitrectomy. Eight eyes had no posterior capsule procedure during the initial surgery. Follow-up ranged from six months to five years. All eyes developed one or multiple posterior syn- echias and all, except one, required secondary capsulectomy and vitrectomy between one month and one year. Twenty eyes attained stable IOL fixation and a clear visual axis. In one eye, the IOL decentered downward. Patients with bilateral cataracts had greater visual improvement than those with a cataract in one eye only. No patient could manage spectacles postoperatively. Our findings show the benefits of posterior capsulectomy and anterior vitrectomy done in the early post- operative period and that IOL implantation in infants is a reasonable treatment in some parts of the world. Key Words: cataract extraction, congenital cataract, intraocular lens implantation, pediatric, posterior capsulectomy, vitrectomy Managing congenital cataracts in pediatric patients remains a challenge. Treatment is often time consuming and expensive. 1 Despite modern instrumentation, sur- gical techniques, and lens power calculation, treatment for dense amblyopia yields poor results, 2 especially in children younger than one year. 3 The child's developing visual structures and the many underlying causes of the cataracts make them harder to manage than in the adult population. 4 Early treatment is one of the most important factors in visual outcome. 5 In infants a congenital cataract, in one or both eyes, causes significant visual deprivation; thus, timing of the treatment is critical. Several animal studies 6 - 9 have shown that visual deprivation from birth to three months of age results in predictable changes in the visual pathways and correcting the deprivation dur- ing that time can modify these changes. Currently, three methods are used to correct aphakia in infants: spectacles, contact lenses, and intraocular lens (IOL) implantation. Epikeratophakia is not an op- tion at this time. Although spectacle correction is the safest, it is impractical in the infant population, espe- cially in those with unilateral aphakia. Contact lenses are expensive and require consistent ophthalmic care rarely available to many of our patients, who are often poor and uneducated and come from rural communities. 10 - 12 Lens insertion and removal is often traumatic, and tol- erance and compliance decrease with time and changes in the family's economic situation. Although some studies have reported good results with contact lenses, 13 - 16 most have found visual out- come unsatisfactory. 17 • 18 Success requires a treatment facility with a motivated staff and parents who are will- ing to comply strictly with the protocol. 19 • 2 0 The keratolens for epikeratophakia is no longer com- mercially available. When epikerataphakia is done in three-month-old eyes, the central visual axis clouds be- cause of postoperative corneal haze. 2 • 4 Intraocular lens implantation avoids many of these complications yet carries its own risks. 17 • 21 - 25 The main objective of cataract extraction, especially in the pedi- atric population, is to prevent deprivation amblyopia and to preserve and develop vision, with the goal of fusion. 26 - 30 Presented at the Symposium on Cataract, IOL and Refractive Surgery, Boston, Apri/1994. Reprint requests to Abhay Vasavada, M.S., F.R.C.S., 1/adevi Cataract & IOL Research Centre, Raghudeep Eye Clinic, Gurukul Road, Memnagar, Ahmedabad 380052, India. 592 J CATARACT REFRACT SURG-VOL 20, NOVEMBER 1994
Transcript
Intraocular lens implantation in infants with congenital cataracts -
ABSTRACT We evaluated 21 eyes of 13 infants between two and eight months old who had primary posterior chamber intraocular lens (IOL) implantation for congenital cataracts between 1988 and 1993. Twelve eyes had a posterior capsulorhexis or plaque peeling at the time of implantation and one eye had a vitrectomy. Eight eyes had no posterior capsule procedure during the initial surgery. Follow-up ranged from six months to five years. All eyes developed one or multiple posterior synechias and all, except one, required secondary capsulectomy and vitrectomy between one month and one year. Twenty eyes attained stable IOL fixation and a clear visual axis. In one eye, the IOL decentered downward. Patients with bilateral cataracts had greater visual improvement than those with a cataract in one eye only. No patient could manage spectacles postoperatively. Our findings show the benefits of posterior capsulectomy and anterior vitrectomy done in the early postoperative period and that IOL implantation in infants is a reasonable treatment in some parts of the world.
Managing congenital cataracts in pediatric patients remains a challenge. Treatment is often time consuming and expensive. 1 Despite modern instrumentation, surgical techniques, and lens power calculation, treatment for dense amblyopia yields poor results, 2 especially in children younger than one year. 3 The child's developing visual structures and the many underlying causes of the cataracts make them harder to manage than in the adult population. 4
Early treatment is one of the most important factors in visual outcome. 5 In infants a congenital cataract, in one or both eyes, causes significant visual deprivation; thus, timing of the treatment is critical. Several animal studies6- 9 have shown that visual deprivation from birth to three months of age results in predictable changes in the visual pathways and correcting the deprivation during that time can modify these changes.
Currently, three methods are used to correct aphakia in infants: spectacles, contact lenses, and intraocular lens (IOL) implantation. Epikeratophakia is not an option at this time. Although spectacle correction is the safest, it is impractical in the infant population, espe-
cially in those with unilateral aphakia. Contact lenses are expensive and require consistent ophthalmic care rarely available to many of our patients, who are often poor and uneducated and come from rural communities. 10- 12
Lens insertion and removal is often traumatic, and tolerance and compliance decrease with time and changes in the family's economic situation.
Although some studies have reported good results with contact lenses, 13- 16 most have found visual outcome unsatisfactory. 17•18 Success requires a treatment facility with a motivated staff and parents who are willing to comply strictly with the protocol. 19•20
The keratolens for epikeratophakia is no longer commercially available. When epikerataphakia is done in three-month-old eyes, the central visual axis clouds because of postoperative corneal haze. 2•4
Intraocular lens implantation avoids many of these complications yet carries its own risks. 17•21 - 25 The main objective of cataract extraction, especially in the pediatric population, is to prevent deprivation amblyopia and to preserve and develop vision, with the goal of fusion.26- 30
Presented at the Symposium on Cataract, IOL and Refractive Surgery, Boston, Apri/1994.
Reprint requests to Abhay Vasavada, M.S., F.R.C.S., 1/adevi Cataract & IOL Research Centre, Raghudeep Eye Clinic, Gurukul Road, Memnagar, Ahmedabad 380052, India.
592 J CATARACT REFRACT SURG-VOL 20, NOVEMBER 1994
After trying several methods to manage congenital cataracts in our infant patients (including lensectomy and contact lenses), we decided that IOL implantation was the best solution, despite the problems of changing refraction and nearly 100% posterior capsule opacification. 31 We present a retrospective study of 21 infant eyes with congenital cataracts that had cataract extraction and IOL implantation.
MATERIALS AND METHODS
We evaluated the results of cataract extraction and IOLimplantation in 21 eyes of 13 infants(lO male) who had cataract extraction and IOL implantation between April 1988 and August 1993. Excluded were children with systemic disorders (e.g., galactosemia or congenital heart disease) or ocular disorders (e.g., persistent hyperplastic primary vitreous, uveal inflammation, microphthalmos, coloboma).
Average age at the time of surgery was four months (range two to eight months). Eight had bilateral cataracts (Figure 1 ). Except for two membranous cataracts (Figure 2) in one infant, all patients had fairly advanced cataracts.
Before surgery, all patients were examined under anesthesia after pupil dilation. The type of cataract and corneal diameter were noted. Intraocular pressure was recorded with a hand-held applanation tonometer. Whenever possible, binocular indirect ophthalmoscopy was done. An anesthesiologist and a pediatrician gave all children a thorough physical examination and took a detailed postpartum history of the mother.
Axial length measurement and a diagnostic A-scan were performed at the same time. We relied solely on axial length measurement to determine IOL power using the SRK formula. 32 Because myopia increases rapidly in the infant eye33,34 and even more quickly in a pseudophakic eye,35 our goal was undercorrection. Using 22.0 mm as the standard axial length and 22.0 diopters
Fig. 1. (Vasavada) Bilateral advanced cataracts in a 5-month-old infant.
Fig. 2. (Vasavada) Membranous cataract in a 7-month-old infant.
(D) as the standard IOL power, we modified the SRK formula for the infant eye. Instead of adding 2.5 D for every 1 mm decrease in axial length, we added 1.0 D to the standard 22.0 D, resulting in a 60% undercorrection.
Preoperative visual assessment was extremely difficult. We used basic methods of evaluation and tried to elicit fixation and following movements to a light, an attractive target, or both. We also noted pupillary reflexes and looked for an afferent pupil defect.
Parents were instructed to administer tobramycin eyedrops four times a day beginning two days before surgery. Cyclopentolate hydrochloride 1% and phenylephrine hydrochloride 10% were given every half hour for three hours before surgery. Atropine 1% eyedrops were administered an hour before surgery.
All patients had surgery under general anesthesia. A glycopyrrolate intramuscular injection, 0.05 mg to 0.1 mg depending on weight, and an oral dose of trimeprazine tartrate 2.5 mg/kg syrup were given one hour before surgery. General anesthesia was induced with oxygen, nitrous oxide, and halothane mixture. After endotracheal intubation, anesthesia was maintained with oxygen, nitrous oxide, halothane, and a nondepolarizing neuromuscular blocking agent (pancuronium bromide) with moderate hyperventilation.
During surgery, patients were on continuous EEG monitor and pulse oximeter with infusion line of an isotonic solution (Isolyte J>®) 7 cc/kg of body weight/hour. Anesthesia was reversed with atropine 0.025 mg/kg and neostigmine 0.050 mg/kg intravenously. We did no eye massage or ocular compression.
Surgical Technique In our first series of surgeries (n = 7), a 6.5 mm wide
limbal incision groove was made with two entries into the anterior chamber at both the ends, leaving an incisional bridge in between. This helped maintain the anterior chamber throughout the lens extraction procedure. The cortex was aspirated manually using a modified reverse Simcoe two-way cannula.
J CATARACT REFRACT SURG-VOL 20, NOVEMBER 1994 593
We later switched to a scleral tunnel, no-stitch approach, with an external incision 2 mm from the clear limbus and an internal incision 1 mm inside clear cornea. The cataract was extracted using a phacoemulsification machine (Alcon Universal) set on irrigation/ aspiration (1/ A). The phaco probe was used only when necessary.
In all cases, the capsulotomy was done under a viscoelastic and a capsulorhexis was initiated. In most cases, the capsulorhexis had to be completed with multipunctures or the help of scissors. Only in two eyes could we achieve a continuous curvilinear capsulorhexis (CCC).
The posterior capsule was scraped and vacuum cleaned using Jenson's sand-blasted, olive-tipped cannula. When possible, the anterior capsule was scraped with Nightingale's ring scraper. 36
After the incision was widened, a posterior chamber IOL was implanted under viscoelastic. We used 14 onepiece IOLs (overall size 12.0 mm; optic 5.5 mm) and seven three-piece IOLs (overall size 13.0 mm; optic 6.0 mm).
One peripheral iridectomy was performed whenever cortex clean-up was inadequate. Limbal incisions were closed by interrupted 10-0 monofilament nylon.
At the end of surgery, some viscoelastic was left inside the anterior chamber. No miotic was used to constrict the pupil. A subconjunctival injection of gentamicin 20 mg and dexamethasone 2.0 mg was given.
Posterior Capsule Management Prir:zary Management. ~uring the initial surgery, the
postenor capsule was clear m 1 7 eyes and central dense plaque present in four eyes. After IOL insertion and incision closure, we performed plaque peeling in four eyes and posterior CCC in eight eyes with clear capsules using the technique developed by GimbeP7 (H.V. Gimbel, M.D., "Posterior Continuous Circular Capsulorhexis," presented at the Storm Eye Institute Ophthalmology Update Meeting, Charleston, SC, April 1989).
A viscoelastic was injected into the anterior chamber and between the posterior capsule and the IOL. The posterior capsulorhexis was performed with the help of a bent cystotome and forceps. We could not make an adequate capsulorhexis in one eye in which the anterior vitreous was disturbed. We performed an anterior vit~ectomy and capsulectomy in that eye. In the remaining etght eyes, the clear posterior capsule was left untreated.
Secondary Management. Except the eye in which primary vitrectomy was performed, all eyes required subsequent opening of the posterior capsule (Table 1). The average time between the first and second surgery was four months (range one month to one year).
Twenty eyes required a posterior capsulectomy and anterior vitrectomy. All eyes in which we performed plaque peeling, posterior CCC, or both developed a secondary membrane that covered the initial posterior capsulorhexis. These eyes had a secondary membranectomy
Table l. Secondary posterior capsule management: Incidence of posterior capsulectomy and anterior vitrectomy.
Follow-up (Months)
0-3 4-6 7-9
10-12
Eyes (n)
9
7
2
2
and anterior vitrectomy through a limbal (n = 18) or pars plana (n = 2) approach.
All patients received dexamethasone 0.1% six times a day for a month and three times a day for another month. In addition, they were given cyclopentolate I% drops on alternate days. When necessary, a short course of atropine eyedrops was prescribed.
During the two days the patients remained in the hospital, occlusion therapy began and parents were instructed on the technique. The sound eye was occluded for no more than 50% of waking hours. 38
Follow-up was at one week and then every month for the first six months to a maximum of five years (average 17 months). At each visit, the child was anesthetized for a short period and examined. Intraocular pressure was measured with a hand-held applanation tonometer during the first visit only.
RESULTS Preoperative visual assessment revealed good fixation
and orthophoria in 15 eyes (Table 2), which was surprising considering the advanced nature of the cataracts. Average axial length was 18.44 mm (range 16.00 mm to 22.71 mm). Average IOL power was 25.0 D (range 21.0 D to 28.0 D). Overall visual outcome was similar for both IOL types.
In the eyes with the no-stitch incision, the anterior chamber remained well formed intraoperatively; however, postoperatively, there was no difference between incision methods. There was no wound leakage or shal-low anterior chambers in the no-stitch group. ·
One month to one year after surgery, posterior capsule opacification occurred in 20 eyes. We did a posterior capsulectomy and anterior vitrectomy in all. The one eye that had an anterior vitrectomy with posterior capsulectomy during the initial surgery did not need a second procedure.
Table 2. Preoperative visual assessment.
Assessment
Good fixation with orthophoria
Good fixation with esotropia
Doubtful fixation with nystagmus
Wandering fixation
Eyes (n)
15
2 2
2
594 J CATARACT REFRACT SURG-VOL 20, NOVEMBER !994
After the second surgery, no eye required further treatment of the posterior capsule. All eyes maintained a clear central visual axis.
Postoperative Visual Assessment We used the following subjective criteria to assess
postoperative vision: ( 1) looking at and picking up small rubber toys placed at various distances, (2) following and picking up rolling wooden beads of different colors, (3) ability to recognize family members, and ( 4) parent observations.
Twenty eyes showed marked improvement as measured by these subjective criteria. It was difficult to assess the outcome in the one eye in which the IOL was severely decentered and subsequently explanted. Improvement measured subjectively was greatest in children with bilateral cataracts.
We were able to assess vision objectively in seven eyes. All had more than two years of follow-up, with an average residual refractive error of -3.25 D (range 0.50 D to -5.00 D). Five eyes had a best corrected visual acuity of20/200 and two of20/80. None of the parents in this group continued satisfactory occlusion treatment at home.
Complications There were no serious intraoperative complications.
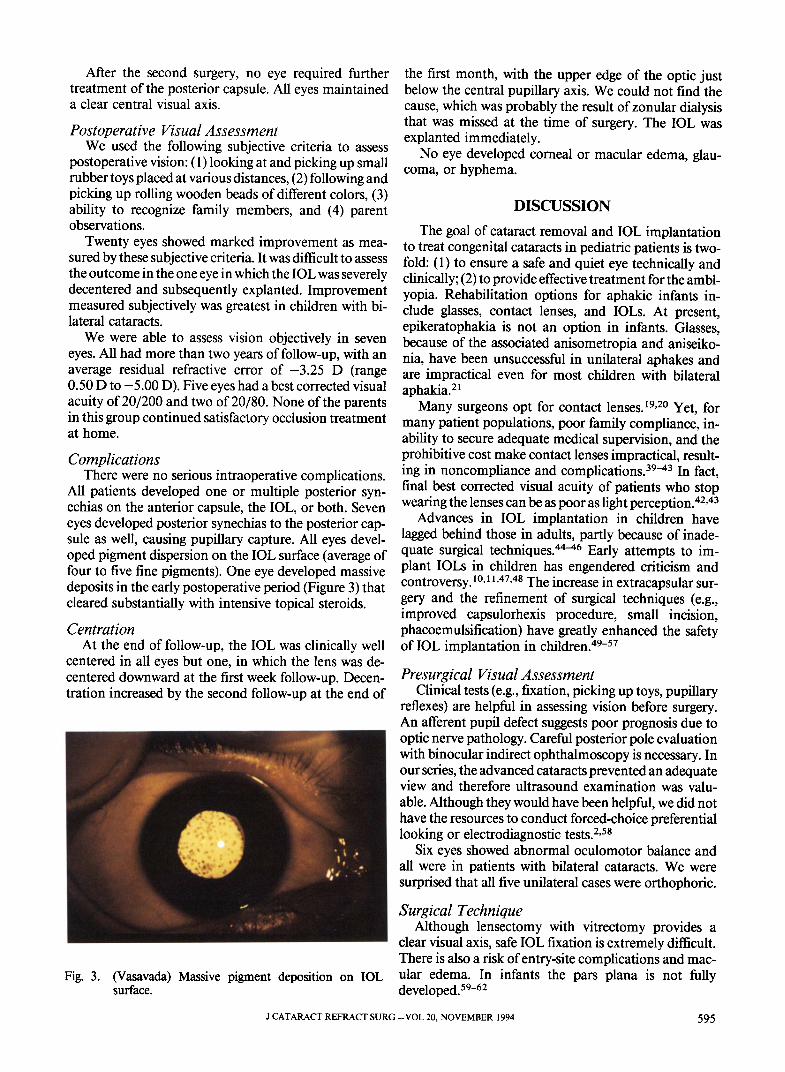
All patients developed one or multiple posterior synechias on the anterior capsule, the IOL, or both. Seven eyes developed posterior synechias to the posterior capsule as well, causing pupillary capture. All eyes developed pigment dispersion on the IOL surface (average of four to five fine pigments). One eye developed massive deposits in the early postoperative period (Figure 3) that cleared substantially with intensive topical steroids.
Centration At the end of follow-up, the IOL was clinically well
centered in all eyes but one, in which the lens was decentered downward at the first week follow-up. Decentration increased by the second follow-up at the end of
Fig. 3. (Vasavada) Massive pigment deposition on IOL surface.
the first month, with the upper edge of the optic just below the central pupillary axis. We could not find the cause, which was probably the result of zonular dialysis that was missed at the time of surgery. The IOL was explanted immediately.
No eye developed corneal or macular edema, glaucoma, or hyphema.
DISCUSSION
The goal of cataract removal and IOL implantation to treat congenital cataracts in pediatric patients is twofold: ( 1) to ensure a safe and quiet eye technically and clinically; (2) to provide effective treatment for the amblyopia. Rehabilitation options for aphakic infants include glasses, contact lenses, and IOLs. At present, epikeratophakia is not an option in infants. Glasses, because of the associated anisometropia and aniseikonia, have been unsuccessful in unilateral aphakes and are impractical even for most children with bilateral aphakia.21
Many surgeons opt for contact lenses. 19•20 Yet, for many patient populations, poor family compliance, inability to secure adequate medical supervision, and the prohibitive cost make contact lenses impractical, resulting in noncompliance and complications. 39-43 In fact, final best corrected visual acuity of patients who stop wearing the lenses can be as poor as light perception. 42•43
Advances in IOL implantation in children have lagged behind those in adults, partly because of inadequate surgical techniques.44- 46 Early attempts to implant IOLs in children has engendered criticism and controversy. 10•11 •47•48 The increase in extracapsular surgery and the refinement of surgical techniques (e.g., improved capsulorhexis procedure, small incision, phacoemulsification) have greatly enhanced the safety of IOL implantation in children.49- 57
reflexes) are helpful in assessing vision before surgery. An afferent pupil defect suggests poor prognosis due to optic nerve pathology. Careful posterior pole evaluation with binocular indirect ophthalmoscopy is necessary. In our series, the advanced cataracts prevented an adequate view and therefore ultrasound examination was valuable. Although they would have been helpful, we did not have the resources to conduct forced-choice preferential looking or electrodiagnostic tests. 2•58
Six eyes showed abnormal oculomotor balance and all were in patients with bilateral cataracts. We were surprised that all five unilateral cases were orthophoric.
Surgical Technique Although lensectomy with vitrectomy provides a
clear visual axis, safe IOL fixation is extremely difficult. There is also a risk of entry-site complications and macular edema. In infants the pars plana is not fully developed. 59- 62
J CATARACT REFRACT SURG-VOL 20, NOVEMBER 1994 595
Lens Aspiration For the first surgeries, we made two small incisions
and performed manual cortex aspiration. We later switched to a no-stitch tunnel incision and used a phacoemulsification machine to extract the cataract, which made the lens much easier to remove.63
Whatever surgical technique is used, the infant eye presents unique challenges.
1. Capsulotomy. Because of the extreme elasticity of the capsule,64 low scleral rigidity, increased intravitreal pressure, and small size, it is very difficult to perform a CCC in the infant eye. When the cataract is mature, as most in our study were, intralenticular pressure is high. This forces soft lens matter through even a small opening in the capsule, obscuring visibility. In most eyes in our study, we were not able to achieve a complete CCC, which would ensure bag fixation, stabilize the IOL, improve centration, and reduce uveal response, including pigment and cell deposits on the IOL surface.
2. Maintenance of the anterior chamber. Low rigidity of the sclera and increased pressure of relatively solid vitreous make it difficult to maintain the anterior chamber. The self-sealing tunnel incision and automated I/ A phacoemulsification mode helped us overcome this problem.
3. Uveal response. We have found that pupils in infant eyes do not dilate well and that intraoperative mechanical stimulation makes them even smaller. Preoperative and postoperative instillation of atropine can help. Fibrinous membrane formation, previously a common complication of pediatric implantation,21·22·65-67 is now rare, probably because of better technique and the "no uveal touch" aspect of closed chamber surgery.
All eyes in our study showed finely pigmented deposits on the IOL surface and posterior synechias, probably resulting from the intense inflammatory response of these small eyes. In some cases, this was exacerbated by our inability to fixate the lens completely in the bag. Seven eyes developed iris capture as a result of posterior synechia formation on the posterior capsule.
We used topical steroids and atropine to reduce uveal response. We have no experience using systemic corticosteroids in infants. Perhaps inflammatory response could be reduced further with systemic corticosteroids.
4. Posterior capsule opacification. Thickening of the posterior lens capsule, common after lens extraction in children,22 occurs almost without exception and extremely rapidly in infants. This opacification often occurs during a critical period in visual development and is one of the main causes of amblyopia. 1 There are two options: ( 1) a capsulectomy with anterior vitrectomy just before or after the IOL implantation or (2) subsequent posterior capsulectomy with anterior vitrectomy.
Although Dahan and Salmenson12 recommend capsulectomy and anterior vitrectomy before lens implantation, we found it difficult to implant an IOL after the posterior capsulectomy and anterior vitrectomy. When
we attempted the procedures immediately after IOL implantation, the IOL decentered intraoperatively. Thus, we began doing posterior capsulectomy with anterior vitrectomy in a subsequent surgery in the early postoperative period. In all 20 eyes that had the secondary procedure, the IOL remained well centered and the central visual axis clear. All eight eyes with primary posterior capsulorhexis and four eyes with plaque peeling developed significant opacification of the central axis and needed secondary capsulectomy with anterior vitrectomy.
We think that, at least in infants, posterior capsularhexis alone is not adequate. Recently, Gimbel68 developed a technique of posterior capsule capture of the IOL optic. The haptics are fixated in the capsular bag and the optic placed posteriorly through the posterior capsularhexis. Although the results in children have been encouraging, the technique's usefulness in patients younger than 18 months has not yet been tested.
Intraocular Lens Power and Changing Refraction Calculating the proper IOL power for children is
difficult. 69 Gordon and Donzis33 found myopia increases rapidly in the growing eyes of infants and small children. Huber35 found evidence of increased axial length in pseudophakic eyes in infants. Dahan34 found that the axial length of the eye with the IOL increases more rapidly than the axial length of the fellow phakic eye and that children younger than one year have a marked myopic shift as the eye grows.
At the time of this study, we did not have a hand-held keratometer and had to rely solely on axial length measurements to calculate IOL power. We adapted the SRK formula to achieve a 60% undercorrection to allow for changing refraction as the eye grows. Gordon and Donzis33 found that the average axial length in children from birth to one year is 19.02 mm. Dahan and Salmenson 12 found that the greatest change in axial length and keratometry occurs during the first 12 to 18 months oflife and recommends 80% undercorrection to achieve emmetropia in children younger than 18 months.70
Using a modified SRK formula, Gordon and Donzis33 found a natural crystalline lens power of 28.7 ± 1 Din children aged birth through one year and recommended an IOL of approximately 23.0 to 24.0 D for implantation in this group. Average IOL power in our study was 25.0 D, a 60% undercorrection. We decided that because myopia progresses faster in younger children, we would undercorrect the younger eyes more than older ones.
Occlusion Therapy We tried to initiate occlusion of the fellow eye by
keeping the child in the hospital for two days postoperatively. The fellow eye was occluded for no more than 50% of waking hours. 38 However, we soon found that because of educational level and socioeconomic conditions, parents could not continue the therapy at home.
596 J CATARACT REFRACT SURG-VOL 20, NOVEMBER 1994
Postoperative Visual Assessment There was a marked subjective improvement in 20
eyes. We were able to do objective assessment on seven eyes and found all had marked improvement in visual acuity. This is particularly surprising considering the advanced nature of most ofthese cataracts. We believe that this is because of early lens aspiration and immediate clearing of posterior capsule opacification.
There has been a disagreement on the best way to treat unilateral congenital cataract because of poor visual outcome in general.26•47•71 Hing and coauthors72 had disappointing visual results in uniocular congenital cataracts. In our study, one child with unilateral cataract achieved a best corrected visual acuity of20/200, which agrees with the good results achieved in other unilateral cataract studies.4•15•26•47 It would have been helpful if we could have continued follow-up of the remaining four children with unilateral cataracts.
Of the three infants with bilateral cataracts, two had a final best corrected visual acuity of 20/200 and one, 20/80. This is not surprising because the cataracts were not very advanced.
Conclusion Our study shows that lens extraction and posterior
chamber IOL implantation in infants can be safe and beneficial if the posterior capsule is treated in all eyes, even in children with bilateral cataracts. We suggest posterior capsulectomy and anterior vitrectomy as a secondary procedure in the early postoperative period and recommend undercorrection when calculating IOL power. There was a noticeable visual improvement in the majority of the eyes. We conclude that primary posterior chamber IOL implantation is a reasonable proposition in some parts of the world.
REFERENCES
1. Lloyd IC, Goss-Simpson MG, Jeffrey BG, et al. Neonatal cataract: aetiology, pathogenesis and management. Eye 1992; 6:184-196
2. Markham RHC, Bloom PA, Chandna A, Newcomb EH. Results of intraocular lens implantation in paediatric aphakia. Eye 1992; 6:493-498
3. Dutton JJ, Baker JD, Hiles DA, Morgan KS. Visual rehabilitation of aphakic children. Surv Ophthalmol 1990; 34:365-384
4. Morgan KS. Pediatric cataract and lens implantation. Curr Opinion Ophthalmol 1994; 5(1):55-60
5. Taylor D, Vaegan, Morris JA, et al. Amblyopia in bilateral infantile and juvenile cataract. Relationship to timing of treatment. Trans Ophthalmol Soc UK 1979; 99: 170-17 5
6. Rubel DH. Exploration of the primary visual cortex, 1955-78. Nature 1982; 229:515-524
7. Wiesel TN. Postnatal development of the visual cortex and the influence of environment. Nature 1982; 299:583-591
8. Vaegan, Taylor D. Critical period for deprivation amblyopia in children. Trans Ophthalmol Soc UK 1979; 99: 432-439
9. Von Noorden GK, Crawford MU. The sensitive period. Trans Ophthalmol Soc UK 1979; 99:442-446
10. Hoyt CS. The optical correction of pediatric aphakia. Arch Ophthalmol 1986; 104:651-652
11. Nelson LB, Cutler SI, Calhoun JH, et al. Silsoft extended wear contact lenses in pediatric aphakia. Ophthalmology 1985; 92:1529-1531
12. Dahan E, Salmenson BD. Pseudophakia in children: precautions, techniques, and feasibility. J Cataract Refract Surg 1990; 16:75-82
13. Amaya LG, Speedwell L, Taylor D. Contact lenses for infant aphakia. Br J Ophthalmol 1990; 74:150-154
14. Levin A V, Edmonds SA, Nelson LB, et al. Extended-wear contact lenses for the treatment of pediatric aphakia. Ophthalmology 1988; 95:1107-1113
15. Beller R, Hoyt CS, MargE, Odom JV. Good visual function after neonatal surgery for congenital monocular cataracts. Am J Ophthalmol1981; 91:559-565
16. Pratt-Johnson JA, Tillson G. Hard contact lenses in the management of congenital cataracts. J Pediatr Ophthalmol Strabismus 1985; 22:94-96
17. Dahan E, Welsh NH, Salmenson BD. Posterior chamber implants in unilateral congenital and developmental cataracts. Eur J Implant Refract Surg 1990; 2:295-302
18. BenEzra D, Rose L. Intraocular versus contact lenses for the correction of aphakia in unilateral, congenital and developmental cataract. Eur J Implant Refract Surg 1990; 2:303-307
19. Baker JD. Visual rehabilitation of aphakic children. II. Contact lenses. Surv Ophthalmol 1990; 34:366-371
20. Holmstrom G, Speedwell L, Taylor D. Contact lensesstill the only solution for infant aphakia. Eur J Implant Refract Surg 1990; 2:265-267
21. Hiles DA. Visual rehabilitation of aphakic children. III. Intraocular lenses. Surv Ophthalmol 1990; 34:371-379
22. Burke JP, Willshaw HE, Young JDH. Intraocular lens implants for uniocular cataracts in childhood. Br J Ophthalmol 1989; 73:860-864
23. Hiles DA, Cheng KP, Biglan A W. Aphakic optical correction with intraocular lenses for children with traumatic cataracts. Eur J Implant Refract Surg 1990; 2:276-283
24. Hiles DA, Hered RW. Modem intraocular lens implants in children with new age limitations. J Cataract Refract Surg 1987; 13:493-497
25. Yamamoto M. Long-term prognosis of intraocular lens implantation in children. Eur J Implant Refract Surg 1990; 2:291-293
26. Drummond GT, Scott WE, Keech RV. Management of monocular congenital cataracts. Arch Ophthalmol 1989; 107:45-51
27. Gelbart SS, Hoyt CS, Jastrebski G, MargE. Long-term visual results in bilateral congenital cataracts. Am J Ophthalmol1982; 93:615-621
28. Rogers GL, Tishler CL, Tsou BH, et al. Visual acuities in infants with congenital cataracts operated on prior to 6 months of age. Arch Ophthalmol 1981; 99:999-1003
29. Hiles DA. Indications, techniques and complications associated with intraocular lens implantation in children. In: Hiles DA, ed, Intraocular Lens Implants in Children. New York, Grone and Stratton, 1980; 189-268
30. Taylor D. Monocular infantile cataract, intraocular lenses and amblyopia (editorial). Br J Ophthalmol 1989; 73: 857-858
J CATARACT REFRACT SURG-VOL 20, NOVEMBER 1994 597
31. Apple DJ, Kincaid MC, Mamalis N, Olson RJ. Intraocular Lenses; Evolution, Designs, Complications and Pathology. Baltimore, Williams & Wilkins, 1989; 329
33. Gordon RA, Donzis PB. Refractive development of the human eye. Arch Ophthalmol 1985; 103:785-789
34. Dahan E. Lens implantation in microphthalmic eyes of infants. Eur J Implant Refract Surg 1989; 1:9-11
35. Huber C. Increasing myopia in children with intraocular lenses (IOL): an experiment in form deprivation myopia? Eur J Implant Refract Surg 1993; 5:154-158
37. Gimbel HV. Posterior capsule tears using phacoemulsification; causes, prevention and management. Eur J Implant Refract Surg 1990; 2:63-69
38. Wright KW, Matsumoto E, Edelman PM. Binocular fusion and stereopsis associated with early surgery for monocular congenital cataracts. Arch Ophthalmol1992; 110: 1607-1609
39. Rao GN. Complications due to daily wear of soft contact lenses. In: Dabezies OH Jr, ed, Contact Lenses; The CLAO Guide to Basic Science and Clinical Practice. Orlando, Grone and Stratton, 1984; 42.1-42.9
40. Lemp MA, Gold JB. The effects of extended-wear hydrophilic contact lenses on the human corneal epithelium. Am J Ophthalmol 1986; 101:274-277
41. Schoessler JP. Corneal endothelial polymegathism associated with extended wear. Int Contact Lens Clin 1983; 10:148-155
42. Burke JP, Young JDH, Willshaw HE. Monocular infantile cataract, intraocular lenses, and amblyopia. Br J Ophthalmol1979; 73:1019
43. Kushner BJ. Visual results after surgery for monocular juvenile cataracts of undetermined onset. Am J Ophthalmol 1986; 102:468-472
44. Hiles DA, Watson BA. Complications of implant surgery in children. Am Intra-Ocular Implant Soc J 1979; 5:24-32
45. Sinskey RM, Patel J. Posterior chamber intraocular lens implants in children: report of a series. Am Intra-Ocular Implant Soc J 1983; 9:157-160
46. Hiles DA. Intraocular lens implantation in children with monocular cataracts, 1974-1983. Ophthalmology 1984; 91:1231-1237
47. Robb RM, Mayer DL, Moore BD. Results of early treatment of unilateral congenital cataracts. J Pediatr Ophthalmol Strabismus 1987; 24:178-181
48. Choyce DP. Correction of uni-ocular aphakia by means of anterior chamber acrylic implants. Trans Ophthalmol Soc UK 1958; 78:459-470
49. Binkhorst CD, Gobin MH. Treatment of congenital and juvenile cataract with intraocular lens implants (pseudophakoi). Br J Ophthalmol 1970; 54:759-765
50. Hiles DA, Wallar PH, Biglan A W. The surgery and results following traumatic cataracts in children. J Pediatr Ophthalmol 1976; 13:319-325
51. Blumenthal M, Y alon M, Treister G. Intraocular lens implantation in traumatic cataract in children. Am IntraOcular Implant Soc J 1983; 9:40-41
52. Hemo Y, BenEzra D. Traumatic cataracts in young children. Correction of aphakia by intraocular lens implantation. Ophthalmic Paediatr Genet 1987; 8:203-207
53. Aron JJ, Aron-Rosa D. Intraocular lens implantation in unilateral congenital cataract: a preliminary report. Am Intra-Ocular Implant Soc J 1983; 9:306-308
54. BenEzra D, Paez JH. Congenital cataract and intraocular lenses. Am J Ophthalmol 1983; 96:311-314
55. BenEzra D, Paez JH, Frucht Y. Monocular and binocular congenital cataract. Ophthalmic Paediatr Genet 1983; 2: 123-128
56. Tablante RT, Cruz EDG, Lapus JV, Santos AM. A new technique of congenital cataract surgery with primary posterior chamber intraocular lens implantation. J Cataract Refract Surg 1988; 14:149-157
57. Dahan E. Insertion of intraocular lenses in the capsular bag. Metabol Pediatr Syst Ophthalmol 1987; 10:87-88
58. Kriss A, Russell-Eggitt I. Electrophysiological assessment of visual pathway function in infants. Eye 1992; 6: 145-153
59. McLeod D. Congenital cataract surgery: a retinal surgeon's viewpoint. Aust NZ J Ophthalmoll986; 14:79-84
60. Nelson LB. Diagnosis and management of cataracts in infancy and childhood. Ophthalmic Surg 1984; 15:688-697
61. Taylor D. Choice of surgical technique in the management of congenital cataract. Trans Ophthalmol Soc UK 1981; 101:114-117
62. Grossman SA, Peyman GA. Long-term visual results after pars plicata lensectomy-vitrectomy for congenital cataracts. Br J Ophthalmol 1988; 72:601-606
63. Hiles DA, Wallar PH. Phacoemulsification versus aspiration in infantile cataract surgery. Ophthalmic Surg 1974; 5(2):13-16
64. Auffarth GU, Wesendahl TA, Newland TJ, Apple DJ. Capsulorhexis in the rabbit eye as a model for pediatric capsulectomy. J Cataract Refract Surg 1994; 20:188-191