Intraoperative Segmentation and Nonrigid Registration for Image Guided Therapy Simon K. Warfield , Arya Nabavi , Torsten Butz , Kemal Tuncali , Stuart G. Silverman , Peter McL. Black , Ferenc A. Jolesz , and Ron Kikinis Surgical Planning Laboratory http://www.spl.harvard.edu Department of Radiology, Department of Surgery, Harvard Medical School and Brigham and Women’s Hospital, 75 Francis St., Boston, MA 02115 USA, Signal Processing Laboratory, Swiss Federal Institute of Technology at Lausanne, 1015 Lausanne, Switzerland. warfield,arya,butz,ktuncali,jolesz,kikinis @bwh.harvard.edu, [email protected], [email protected]Abstract. Our goal was to improve image guidance during minimally invasive image guided therapy by developing an intraoperative segmentation and nonrigid registration algorithm. The algorithm was designed to allow for improved navi- gation and quantitative monitoring of treatment progress in order to reduce the time required in the operating room and to improve outcomes. The algorithm has been applied to intraoperative images from cryotherapy of the liver and from surgery of the brain. Empirically the algorithm has been found to be robust with respect to imaging characteristics such as noise and intensity inhomogeneity and robust with respect to parameter selection. Serial and paral- lel implementations of the algorithm are sufficiently fast to be practical in the operating room. The contributions of this work are an algorithm for intraoperative segmentation and intraoperative registration, a method for quantitative monitoring of cryother- apy from real-time imaging, quantitative monitoring of brain tumor resection by comparison to a preoperative treatment plan and an extensive validation study assessing the reproducibilityof the intraoperative segmentation. We have evalu- ated our algorithm with six neurosurgical cases and two liver cryotherapy cases with promising results. Further clinical validation with larger numbers of cases will be necessary to determine if our algorithm succeeds in improving intraoper- ative navigation and intraoperative therapy delivery and hence improves therapy outcomes. 1 1 Introduction Image guided surgical techniques are used in operating rooms equipped with special purpose imaging equipment. The development of image guided surgical methods over the past decade has provided a major advance in minimally invasive therapy delivery. Early work such as that reviewed by Jolesz [1] has established the importance and value of image guidance through better determination of tumor margins, better localization of lesions, and optimization of the surgical approach. 1 This paper will appear at MICCAI 2000: Third International Conference on Medical Robotics, Imaging And Computer Assisted Surgery
Transcript
Intraoperative Segmentation and Nonrigid Registrationfor Image Guided Therapy
Abstract. Our goalwasto improve imageguidanceduring minimally invasiveimageguidedtherapy by developinganintraoperativesegmentationandnonrigidregistrationalgorithm.Thealgorithmwasdesignedto allow for improved navi-gationandquantitative monitoringof treatmentprogressin orderto reducethetime requiredin theoperatingroomandto improveoutcomes.Thealgorithmhasbeenappliedto intraoperative imagesfrom cryotherapy of theliver and from surgery of the brain. Empirically the algorithmhasbeenfoundto be robust with respectto imagingcharacteristicssuchasnoiseandintensityinhomogeneityandrobustwith respectto parameterselection.Serialandparal-lel implementationsof the algorithmare sufficiently fast to be practicalin theoperatingroom.Thecontributionsof this work areanalgorithmfor intraoperative segmentationandintraoperative registration,amethodfor quantitative monitoringof cryother-apy from real-timeimaging,quantitative monitoringof braintumorresectionbycomparisonto a preoperative treatmentplan andan extensive validationstudyassessingthereproducibilityof the intraoperative segmentation.We have evalu-atedour algorithmwith six neurosurgical casesandtwo liver cryotherapy caseswith promisingresults.Furtherclinical validationwith larger numbersof caseswill benecessaryto determineif our algorithmsucceedsin improving intraoper-ative navigationandintraoperative therapy delivery andhenceimprovestherapyoutcomes.1
Researchin imageguidedtherapy hasbeendrivenby theneedfor improvedvisu-alization.Qualitative judgementsby expertsin clinical domainshave beenrelieduponasquantitative andautomatedassessmentof intraoperative imagingdatahasnot beenpossiblein thepast.In orderto provide thesurgeonor interventionalradiologistwithasrich a visualizationenvironmentaspossiblefrom which to derive suchjudgements,existing work hasbeenconcernedprimarily with imageacquisition,visualizationandregistrationof intraoperativeandpreoperativedata.Intraoperativesegmentationhasthepotentialto be a significantaid to the intraoperative interpretationof imagesand toenablepredictionof surgicalchanges.
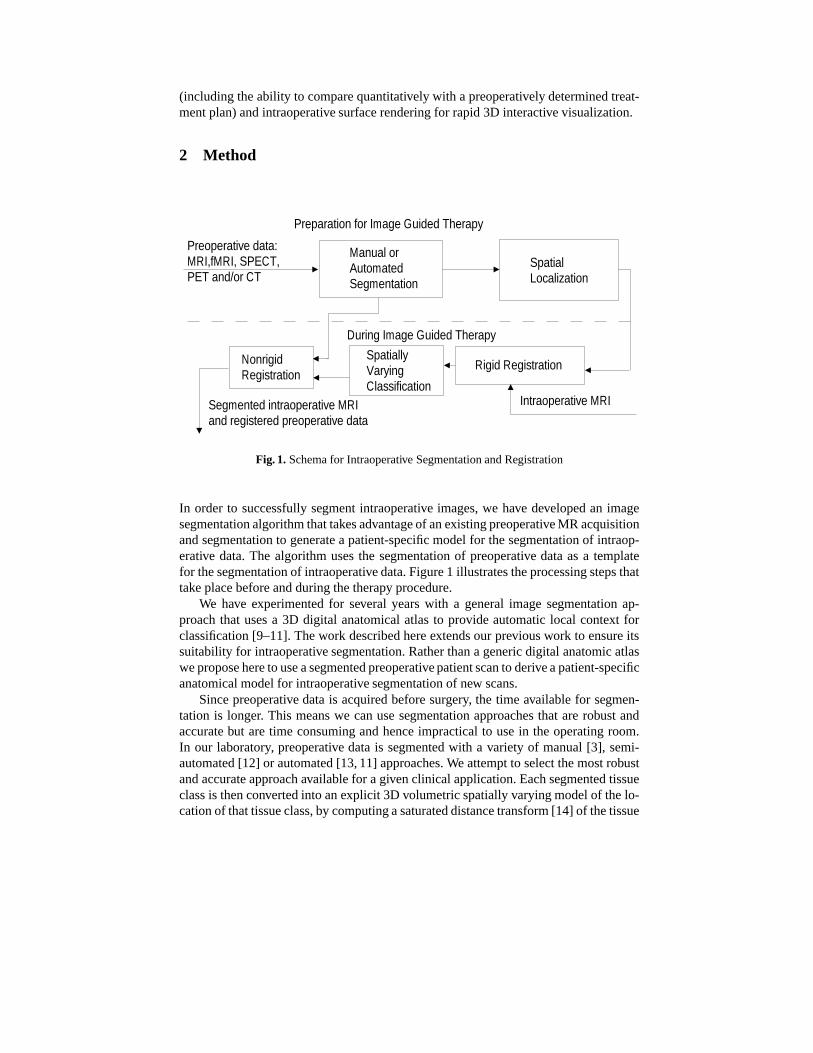
(includingtheability to comparequantitatively with a preoperatively determinedtreat-mentplan)andintraoperativesurfacerenderingfor rapid3D interactivevisualization.
2 Method
Preoperative data:MRI,fMRI, SPECT,PET and/or CT
Manual or AutomatedSegmentation
SpatialLocalization
Preparation for Image Guided Therapy
Intraoperative MRI
Rigid Registration
During Image Guided Therapy
SpatiallyVaryingClassification
NonrigidRegistration
Segmented intraoperative MRIand registered preoperative data
We have experimentedfor several yearswith a generalimagesegmentationap-proachthat usesa 3D digital anatomicalatlasto provide automaticlocal context forclassification[9–11].Thework describedhereextendsour previouswork to ensureitssuitability for intraoperativesegmentation.Ratherthana genericdigital anatomicatlasweproposeheretouseasegmentedpreoperativepatientscanto deriveapatient-specificanatomicalmodelfor intraoperativesegmentationof new scans.
Sincepreoperative datais acquiredbeforesurgery, the time availablefor segmen-tation is longer. This meanswe canusesegmentationapproachesthat arerobust andaccuratebut aretime consumingandhenceimpracticalto usein the operatingroom.In our laboratory, preoperative datais segmentedwith a variety of manual[3], semi-automated[12] or automated[13,11] approaches.We attemptto selectthemostrobustandaccurateapproachavailablefor agivenclinical application.Eachsegmentedtissueclassis thenconvertedinto anexplicit 3D volumetricspatiallyvaryingmodelof thelo-cationof thattissueclass,by computingasaturateddistancetransform[14] of thetissue
class.Thismodelis usedto providerobustautomaticlocalcontext for theclassificationof intraoperativedatain thefollowing way.
During surgery, intraoperative datais acquiredandthe preoperative data(includ-ing any MRI/fMRI/PET/SPECT/MRAthatis appropriate,thetissueclasssegmentationandthespatiallocalizationmodelderivedfrom it) is alignedwith theintraoperativedatausinganMI basedrigid registrationmethod[15,3]. Theintraoperativeimagedatathentogetherwith the spatiallocalizationmodel forms a multichannel3D dataset.Eachvoxel is thena vectorhaving componentsfrom the intraoperative MR scan,the spa-tially varyingtissuelocationmodelandif relevantto theparticularapplication,any oftheotherpreoperativeimagedatasets.For thefirst intraoperativescanto besegmenteda statisticalmodelfor theprobabilitydistribution of tissueclassesin the intensityandanatomicallocalizationfeaturespaceis built. Thestatisticalmodelis encodedimplicitlyby selectinggroupsof prototypicalvoxelswhich representthetissueclassesto beseg-mentedintraoperatively (lessthanfiveminutesof userinteraction).Thespatiallocationof theprototypevoxelsis recordedandis usedto updatethestatisticalmodelautomati-cally whenfurtherintraoperativeimagesareacquiredandregistered.Thismultichanneldatasetis thensegmentedwith a spatiallyvaryingclassification[10,13,16].
Segmentationof intraoperative datahelpsto establishexplicitly the regionsof tis-suesthatcorrespondin the preoperative andintraoperative data.It is thenstraightfor-wardtoapplyourpreviouslydescribed[17,18]andvalidated[19] multi-resolutionelas-tic matchingalgorithm.Oncethenonrigidtransformationmappingfrom thepreopera-tive to the intraoperative datahasbeenestablished,the mappingis appliedto eachoftherelevantpreoperativedatasetsto bring theminto alignmentwith theintraoperativescan.
3 Results
In thissectionillustrative segmentationsandtwo validationexperimentsarepresented.Duringinterventionalproceduresin theliverandbrain,intraoperativeMRI (IMRI) datasetswereacquiredandstored.Our segmentationandnonrigid registrationalgorithmwasappliedto thesedatasetsafter therapy delivery in orderto allow us to assesstherobustness,accuracy andtime requirementsof the approach.In the future we intendto carry out segmentation,nonrigid registrationandvisualizationusingthe approachdescribedhereduringthe interventionalprocedureswith thegoalof improving imageguidedtherapy outcomes.
3.1 Intraoperative Segmentation for Neurosurgery
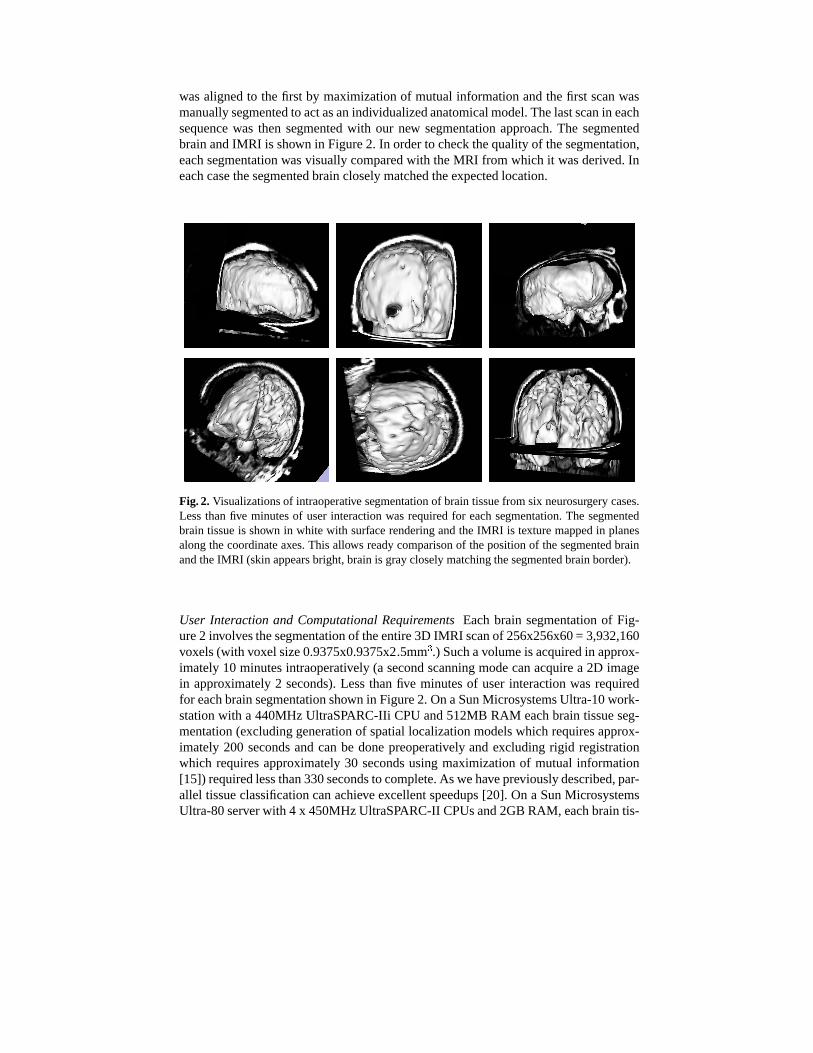
Figure2 illustratesthesegmentationof six neurosurgerycasesusingour intraoperativesegmentationalgorithm.In eachcase,several volumetricMRI scanswerecarriedoutduringsurgery. Thefirst scanwasacquiredatthebeginningof theprocedurebeforeanychangesin theshapeof thebraintook place,andthenover thecourseof surgeryotherscanswereacquiredasthesurgeoncheckedtheprogressof tumorresection.Thefinalscanin eachsequenceexhibits significantnonrigiddeformationandlossof tissuedueto tumor resection.In order to testour segmentationapproacheachsubsequentscan
wasalignedto thefirst by maximizationof mutualinformationandthefirst scanwasmanuallysegmentedto actasanindividualizedanatomicalmodel.Thelastscanin eachsequencewas then segmentedwith our new segmentationapproach.The segmentedbrainandIMRI is shown in Figure2. In orderto checkthequalityof thesegmentation,eachsegmentationwasvisually comparedwith theMRI from which it wasderived.Ineachcasethesegmentedbraincloselymatchedtheexpectedlocation.
Fig. 2. Visualizationsof intraoperative segmentationof braintissuefrom six neurosurgerycases.Lessthanfive minutesof userinteractionwasrequiredfor eachsegmentation.The segmentedbraintissueis shown in white with surfacerenderingandtheIMRI is texturemappedin planesalongthecoordinateaxes.This allows readycomparisonof thepositionof thesegmentedbrainandtheIMRI (skinappearsbright,brainis graycloselymatchingthesegmentedbrainborder).
User Interaction and ComputationalRequirementsEachbrain segmentationof Fig-ure2 involvesthesegmentationof theentire3D IMRI scanof 256x256x60= 3,932,160voxels(with voxel size0.9375x0.9375x2.5mm
�.) Suchavolumeis acquiredin approx-
imately10 minutesintraoperatively (a secondscanningmodecanacquirea 2D imagein approximately2 seconds).Lessthanfive minutesof userinteractionwasrequiredfor eachbrainsegmentationshown in Figure2. OnaSunMicrosystemsUltra-10work-stationwith a 440MHzUltraSPARC-IIi CPUand512MB RAM eachbraintissueseg-mentation(excludinggenerationof spatiallocalizationmodelswhich requiresapprox-imately 200 secondsandcanbe donepreoperatively andexcluding rigid registrationwhich requiresapproximately30 secondsusingmaximizationof mutual information[15]) requiredlessthan330secondsto complete.As wehavepreviouslydescribed,par-allel tissueclassificationcanachieve excellentspeedups[20]. On a SunMicrosystemsUltra-80serverwith 4 x 450MHzUltraSPARC-II CPUsand2GBRAM, eachbraintis-
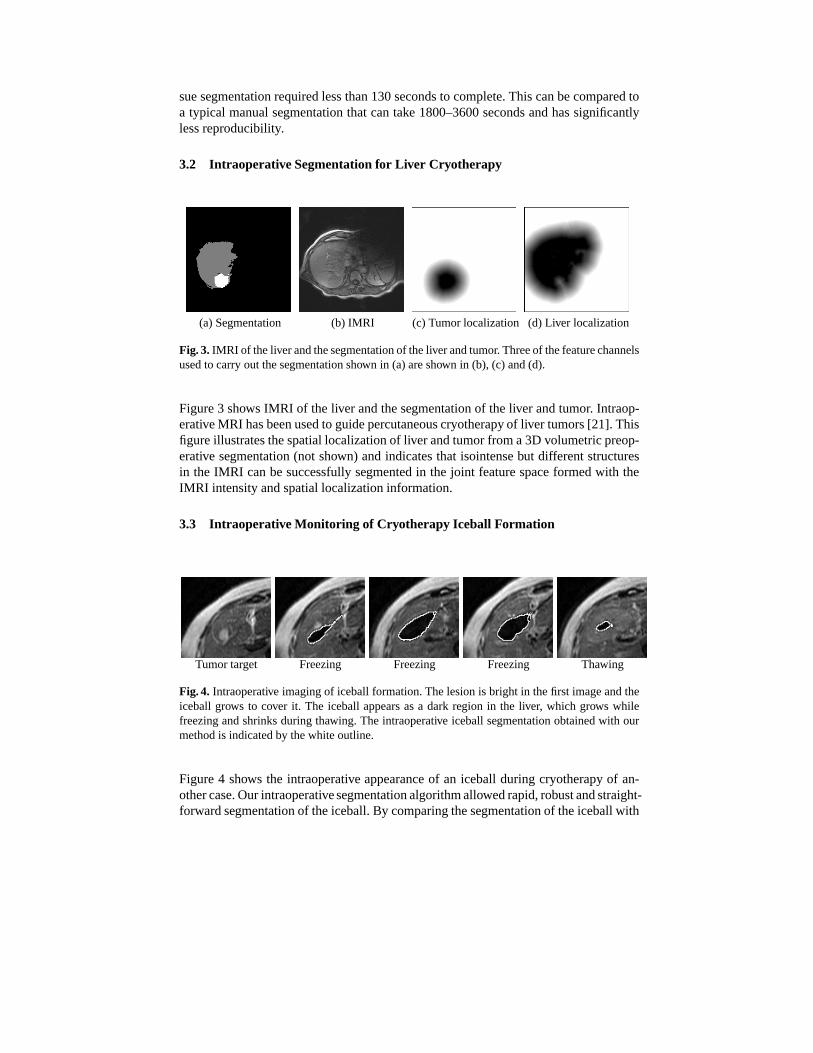
Fig. 3. IMRI of theliverandthesegmentationof theliverandtumor. Threeof thefeaturechannelsusedto carryout thesegmentationshown in (a)areshown in (b), (c) and(d).
Figure3 shows IMRI of theliver andthesegmentationof theliver andtumor. Intraop-erativeMRI hasbeenusedto guidepercutaneouscryotherapy of liver tumors[21]. Thisfigureillustratesthespatiallocalizationof liverandtumorfrom a3D volumetricpreop-erative segmentation(not shown) andindicatesthat isointensebut differentstructuresin the IMRI canbesuccessfullysegmentedin the joint featurespaceformedwith theIMRI intensityandspatiallocalizationinformation.
3.3 Intraoperative Monitoring of Cryotherapy Iceball Formation
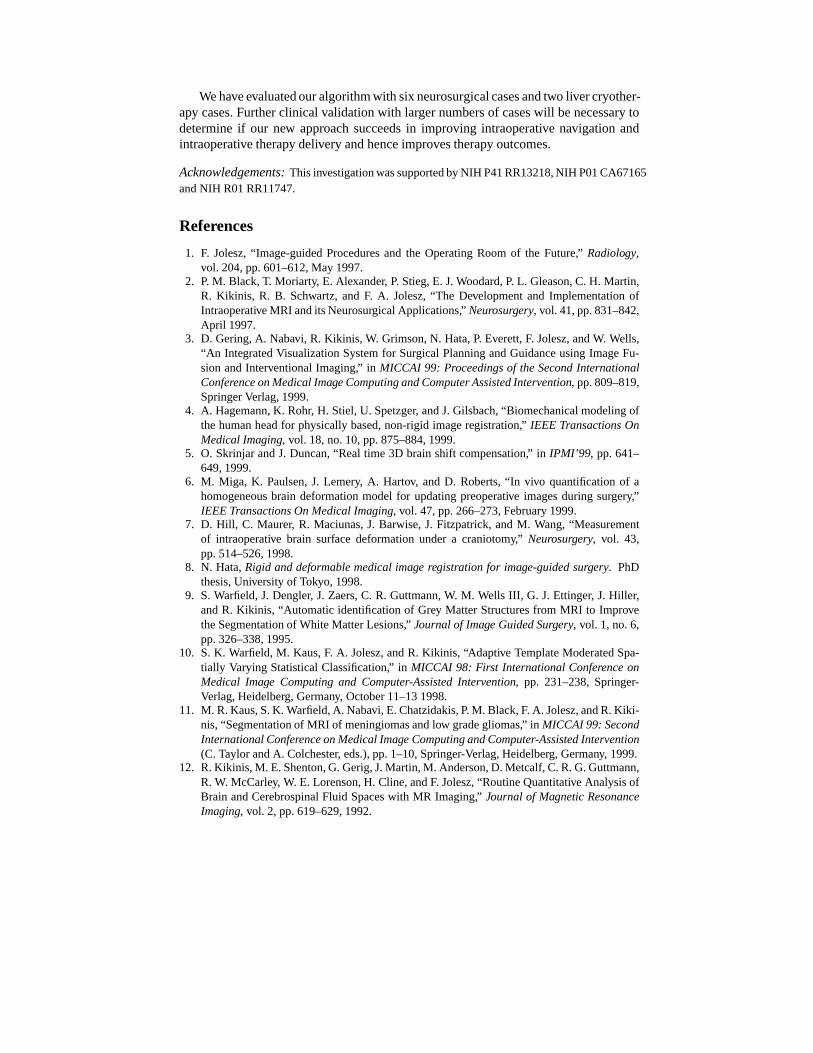
Tumortarget Freezing Freezing Freezing Thawing
Fig. 4. Intraoperative imagingof iceballformation.Thelesionis bright in thefirst imageandtheiceball grows to cover it. The iceball appearsasa dark region in the liver, which grows whilefreezingandshrinksduringthawing. The intraoperative iceball segmentationobtainedwith ourmethodis indicatedby thewhiteoutline.
Figure4 shows the intraoperative appearanceof an iceball during cryotherapy of an-othercase.Ourintraoperativesegmentationalgorithmallowedrapid,robustandstraight-forwardsegmentationof theiceball.By comparingthesegmentationof theiceballwith
a preoperativeplanof thedesirediceballsizeandlocationthetherapy progresscanbemonitoredquantitatively.
Reproducibility: Variations in prototype selection Table1 recordsthevariability ofbrain segmentationfrom a singleneurosurgerycasewhenthe setof prototypevoxelsmodelingthetissuecharacteristicsis varied.Thesetof prototypesusedfor thesegmen-tationwassubsampledby randomlyselecting90%of theprototypes100 times.Eachof the100subsetssimulatesdifferentuserprototypeselection.EachsubsetwasusedtosegmenttheIMRI usingthenew methodandthevolumeof thebrainsegmentationwasrecorded.Themean,minimumandmaximumvolumerecordedareshown in thetablealongwith thecoefficient of variation(C.V.) of thevolumeof segmentation(which islessthan1%). This indicatesthe segmentationis extremelyrobust in the presenceofvariability in theprototypevoxel selection.
Reproducibility: Variations in preoperative model alignment In orderto determinetheinfluenceof thealignmentof thepreoperativesegmentationupontheintraoperativesegmentation,we selecteda neurosurgerycaseandsegmentedthe brain asdescribedabove.Wethenappliedasetof translationsandrotationsto thepreoperativesegmenta-tion sothatit wasno longercorrectlyregisteredto theIMRI to besegmented.For eachtranslationandrotationweappliedoursegmentationmethodandobtaineda segmenta-tion of thebrain.We thencomparedthevolumeof tissuesegmentedasbrain for eachmisalignedpositionwith thatobtainedwith thecorrectalignmentandrecordedtheratioof thenew segmentationvolumeto theoriginal segmentationvolume.Thevariationinsegmentationwith translationsalongeachof thecoordinateaxesis shown in Figure5.Similar results(not shown) wereobtainedfor rotationsaroundeachof thecoordinateaxes.
Intrapatientregistrationwith maximizationof mutualinformationhasa typical ac-curacy smallerthanonevoxel (in this case0.9375x0.9375x2.5mm
�). Theperturbation
of theregistrationof thepreoperativesegmentationdoesnotcausea significantchangein the intraoperative segmentationuntil this misalignmentreachesaround �� �� mm,which indicatesour intraoperative segmentationmethodis robust to misalignmenter-rorsandalsoto errorsin thepreoperativesegmentation.
1. F. Jolesz,“Image-guidedProceduresand the OperatingRoom of the Future,” Radiology,vol. 204,pp.601–612,May 1997.
2. P. M. Black,T. Moriarty, E. Alexander, P. Stieg, E. J.Woodard,P. L. Gleason,C. H. Martin,R. Kikinis, R. B. Schwartz, and F. A. Jolesz,“The Developmentand ImplementationofIntraoperativeMRI andits NeurosurgicalApplications,” Neurosurgery, vol. 41,pp.831–842,April 1997.
3. D. Gering,A. Nabavi, R. Kikinis, W. Grimson,N. Hata,P. Everett,F. Jolesz,andW. Wells,“An IntegratedVisualizationSystemfor Surgical PlanningandGuidanceusingImageFu-sionandInterventionalImaging,” in MICCAI 99: Proceedingsof theSecondInternationalConferenceonMedicalImageComputingandComputerAssistedIntervention, pp.809–819,SpringerVerlag,1999.
4. A. Hagemann,K. Rohr, H. Stiel,U. Spetzger, andJ.Gilsbach,“Biomechanicalmodelingofthehumanheadfor physicallybased,non-rigid imageregistration,” IEEE TransactionsOnMedicalImaging, vol. 18,no.10,pp.875–884,1999.
5. O. SkrinjarandJ. Duncan,“Real time 3D brainshift compensation,” in IPMI’99, pp. 641–649,1999.
6. M. Miga, K. Paulsen,J. Lemery, A. Hartov, andD. Roberts,“In vivo quantificationof ahomogeneousbrain deformationmodel for updatingpreoperative imagesduring surgery,”IEEETransactionsOnMedicalImaging, vol. 47,pp.266–273,February1999.
7. D. Hill, C. Maurer, R. Maciunas,J. Barwise,J. Fitzpatrick,andM. Wang,“Measurementof intraoperative brain surface deformationundera craniotomy,” Neurosurgery, vol. 43,pp.514–526,1998.
8. N. Hata,Rigid anddeformablemedicalimage registration for image-guidedsurgery. PhDthesis,Universityof Tokyo, 1998.
9. S. Warfield,J. Dengler, J. Zaers,C. R. Guttmann,W. M. Wells III, G. J. Ettinger, J. Hiller,andR. Kikinis, “Automatic identificationof Grey Matter Structuresfrom MRI to ImprovetheSegmentationof WhiteMatterLesions,” Journalof Image GuidedSurgery, vol. 1, no.6,pp.326–338,1995.
10. S. K. Warfield,M. Kaus,F. A. Jolesz,andR. Kikinis, “Adaptive TemplateModeratedSpa-tially VaryingStatisticalClassification,” in MICCAI 98: First InternationalConferenceonMedical Image Computingand Computer-AssistedIntervention, pp. 231–238,Springer-Verlag,Heidelberg, Germany, October11–131998.
11. M. R.Kaus,S.K. Warfield,A. Nabavi, E.Chatzidakis,P. M. Black,F. A. Jolesz,andR.Kiki-nis,“Segmentationof MRI of meningiomasandlow gradegliomas,” in MICCAI 99: SecondInternationalConferenceonMedicalImageComputingandComputer-AssistedIntervention(C. TaylorandA. Colchester, eds.),pp.1–10,Springer-Verlag,Heidelberg, Germany, 1999.
12. R.Kikinis, M. E.Shenton,G.Gerig,J.Martin,M. Anderson,D. Metcalf,C.R.G.Guttmann,R. W. McCarley, W. E. Lorenson,H. Cline,andF. Jolesz,“RoutineQuantitativeAnalysisofBrain andCerebrospinalFluid Spaceswith MR Imaging,” Journal of MagneticResonanceImaging, vol. 2, pp.619–629,1992.
13. S.K. Warfield,M. Kaus,F. A. Jolesz,andR. Kikinis, “Adaptive,TemplateModerated,Spa-tially VaryingStatisticalClassification,” Medical Image Analysis, vol. 4, no. 1, pp. 43–55,2000.
14. I. Ragnemalm,“The Euclideandistancetransformin arbitrarydimensions,” PatternRecog-nition Letters, vol. 14,pp.883–888,1993.
15. W. M. Wells,P. Viola, H. Atsumi,S.Nakajima,andR. Kikinis, “Multi-modal volumeregis-trationby maximizationof mutualinformation,” MedicalImage Analysis, vol. 1, pp.35–51,March1996.
16. R. O. DudaandP. E. Hart, PatternClassificationandSceneAnalysis. JohnWiley & Sons,Inc.,1973.
17. J. DenglerandM. Schmidt,“The DynamicPyramid– A Model for Motion AnalysiswithControlledContinuity,” InternationalJournal of Pattern Recognition and Artificial Intelli-gence, vol. 2, no.2, pp.275–286,1988.
18. S.K. Warfield,A. Robatino,J.Dengler, F. A. Jolesz,andR.Kikinis, “NonlinearRegistrationandTemplateDrivenSegmentation,” in Brain Warping(A. W. Toga,ed.),ch.4, pp.67–84,AcademicPress,SanDiego,USA, 1999.
19. D. V. Iosifescu,M. E.Shenton,S.K. Warfield,R. Kikinis, J.Dengler, F. A. Jolesz,andR. W.McCarley, “An AutomatedRegistrationAlgorithm for MeasuringMRI SubcorticalBrainStructures,” NeuroImage, vol. 6, pp.12–25,1997.
20. S. K. Warfield, F. A. Jolesz,andR. Kikinis, “Real-TimeImageSegmentationfor Image-GuidedSurgery,” in Supercomputing1998, pp.1114:1–14,November1998.
21. S.G. Silverman,K. Tuncali,D. F. Adams,E. vanSonnenberg, K. H. Zou,D. F. Kacher, P. R.Morrison,andF. A. Jolesz,“MRI-Guided percutaneouscryotherapy of liver tumors:initialexperience,” Radiology. In press.