45
A New View of HIM: Introducing the Core Model Review Draſt REVIEW DRAFT
A New View of HIM: Introducing the Core ModelReview DraftREVIEW
DRAFT
HIMCore_9-28.indd 1 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 2
DRAFTREVIEW
ContentsExecutive Summary______________________________________________3
Introduction ____________________________________________________5
A Call for a New Professional Core Model _______________________5
Background - Developing the New Core Model ___________________6
A New HIM Profession Core Model _____________________________6
Functional Components and Statements __________________________8
Data Capture, Validation & Maintenance ________________________8
Data / Information Analysis, Transformation & Decision Support _____8
Information Dissemination & Liaison ____________________________8
Health Information Resource Management & Innovation ___________9
Information Governmance and Stewardship ______________________9
Core Model Extensions __________________________________________9
Research ___________________________________________________9
Policy ______________________________________________________9
Education __________________________________________________9
Standards ________________________________________________ 10
Settings of Practice for Health Information Management ________ 10
Roles and Value ______________________________________________ 11
Data Capture, Validation and Maintenance ____________________ 11
Data/Information Analysis, Transformation and Decision Support __ 11
Function: Information Dissemination & Liaison __________________ 12
Health Information Resource Management and Innovation _______ 12
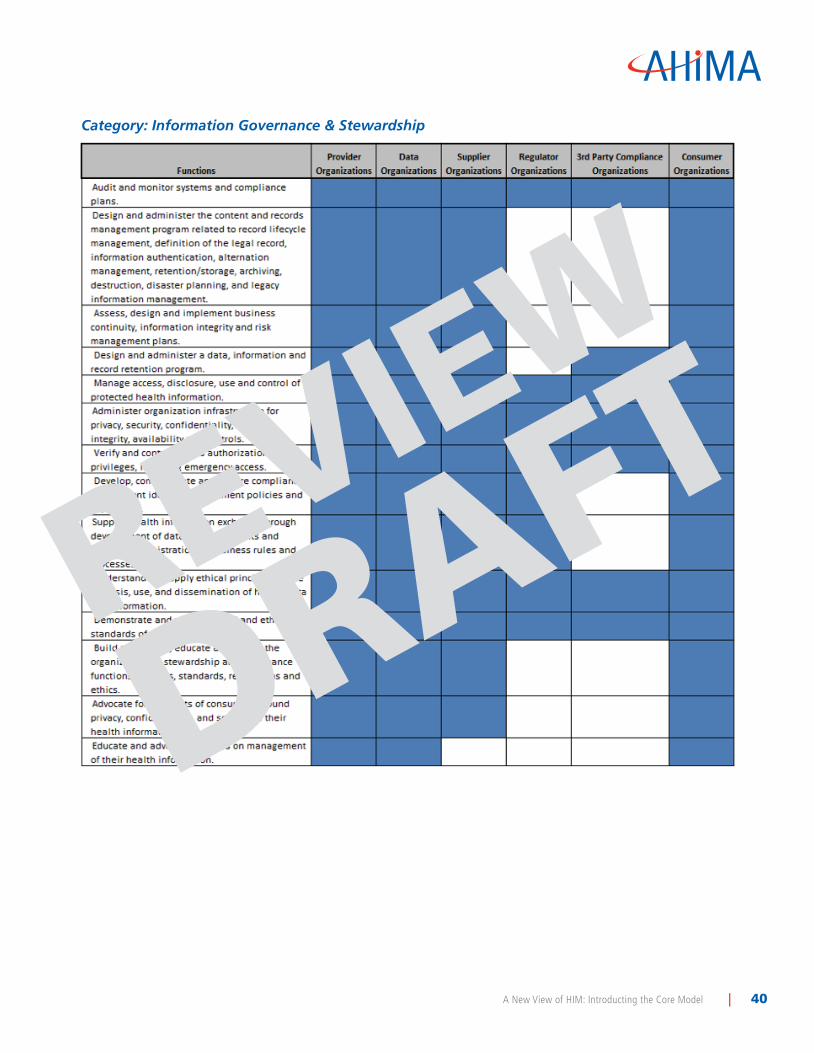
Function: Information Governance and Stewardship _____________ 13
Bibliography _______________________________________________ 16–24
Appendix A ________________________________________________ 25–35
Appendix B ________________________________________________ 36–40
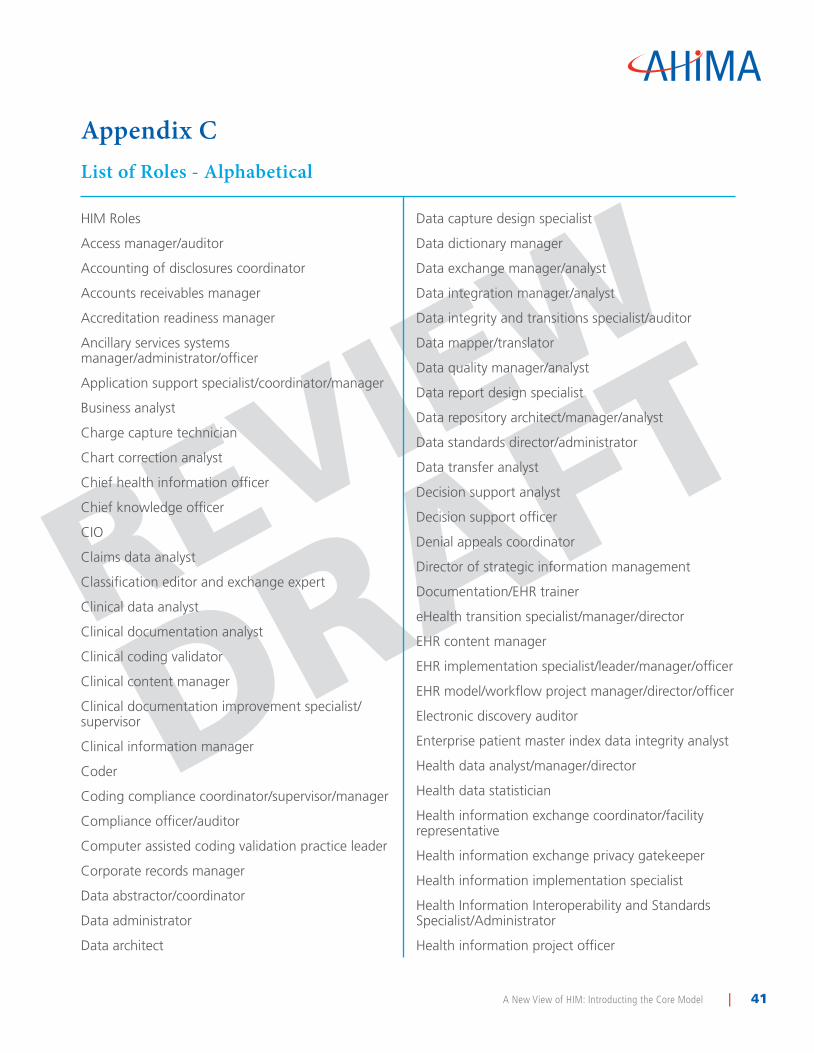
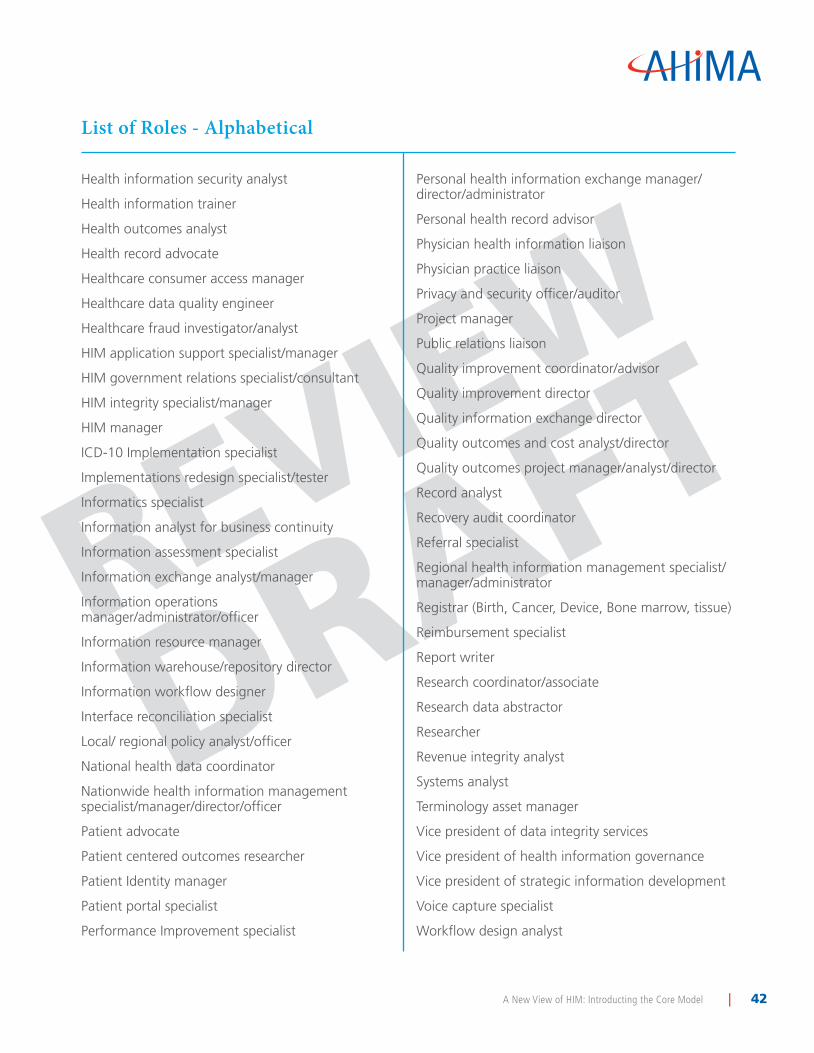
Appendix C ________________________________________________ 41–42
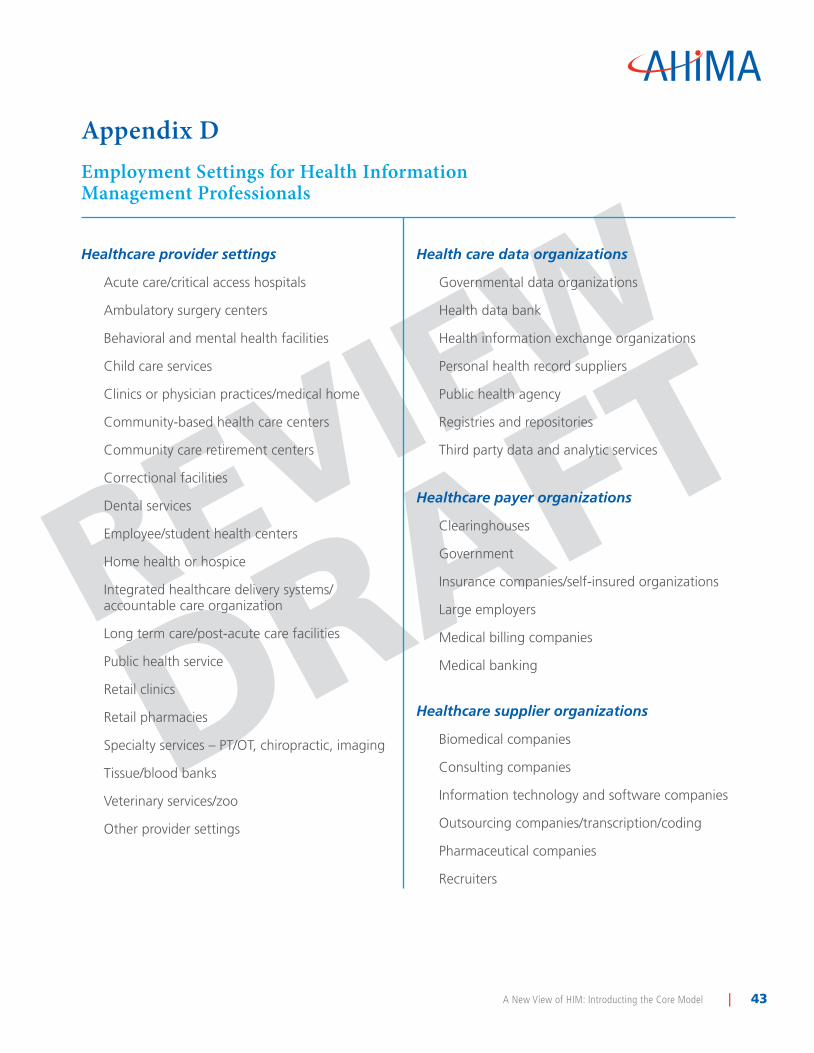
Appendix D ________________________________________________ 43–44
The American Health Information Management Association is the worldwide professional
association of recognized leaders in health information management, informatics, heath data
technology, and innovation. To learn more about AHIMA visit www.ahima.org. ©2011
HIMCore_9-28.indd 2 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 3
DRAFTREVIEW
Executive SummaryIn the last year the AHIMA Board of Directors undertook the challenge of developing a new view of Health Information Management (HIM)—one that addressed changing practice roles, settings, and functions emerging from increased automation, changing regulations, and dissemination of data.
The result, with input from AHIMA members, industry experts, and AHIMA staff is a draft HIM Core Model to describe a robust set of functions and opportunities open to current and future HIM professionals. This Core Model has been extended to include an inventory of inventory of HIM functions and a description of a desired future state of health information management’s roles across the healthcare industry over the next 10 years.
This white paper represents an AHIMA consensus of the future functions and roles of health information management. It:
• Extends the core model description of HIM to ensure inclusion of a complete and comprehensive set of future HIM functions
• Addresses major health settings in which health information must be managed, mapping future HIM functions to future HIM practice settings across the industry
• Transfers interim ideas to AHIMA programs to advance members, the HIM profession, and AHIMA
• Leads to and enables, but does not include, follow-on work to publish future-state HIM roles, functions, and value to external agencies, organizations, and communication channels
Throughout the process, AHIMA has continued to collect feedback from its members and industry experts to further refine the model. The publication of this draft version, intended for AHIMA members, represents the next step in this ongoing professional dialogue.
In the Core Model, the primary role of the HIM professional is focused on five main functional areas of health information:
• Data capture, validation, and maintenance
• Data/information analysis, transformation, and decision support
• Information dissemination and liaison
• Health information resource management and innovation
• Information governance and stewardship
Functional statements were then developed for each of the core elements of the model.
HIMCore_9-28.indd 3 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 4
DRAFTREVIEW
In addition, the model identifies four areas of HIM practice that do not include direct interaction with patient level health information but require an understanding of HIM and additional unique knowledge, leadership, and innovation. These “extenders” serve two purposes. First, they describe additional roles for HIM professionals outside but related to the core functions. Second, they describe operations that enhance and extend the core functions. Education, policy, research, and standards are key enablers that support, advance, extend and contribute to the evolution of the functional components and of the Core Model as a whole. The second purpose of the model extenders is to describe the roles HIM professionals take in performing these functions. The functional statements and descriptions of extenders are attached as Appendix A.
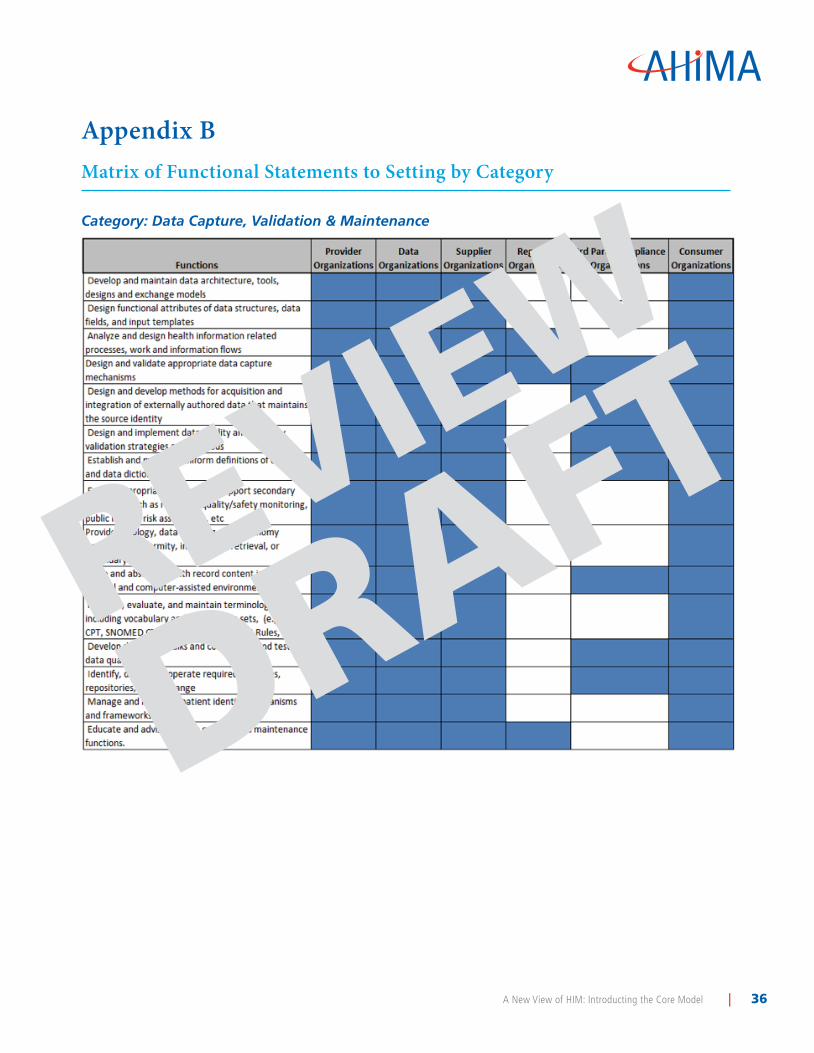
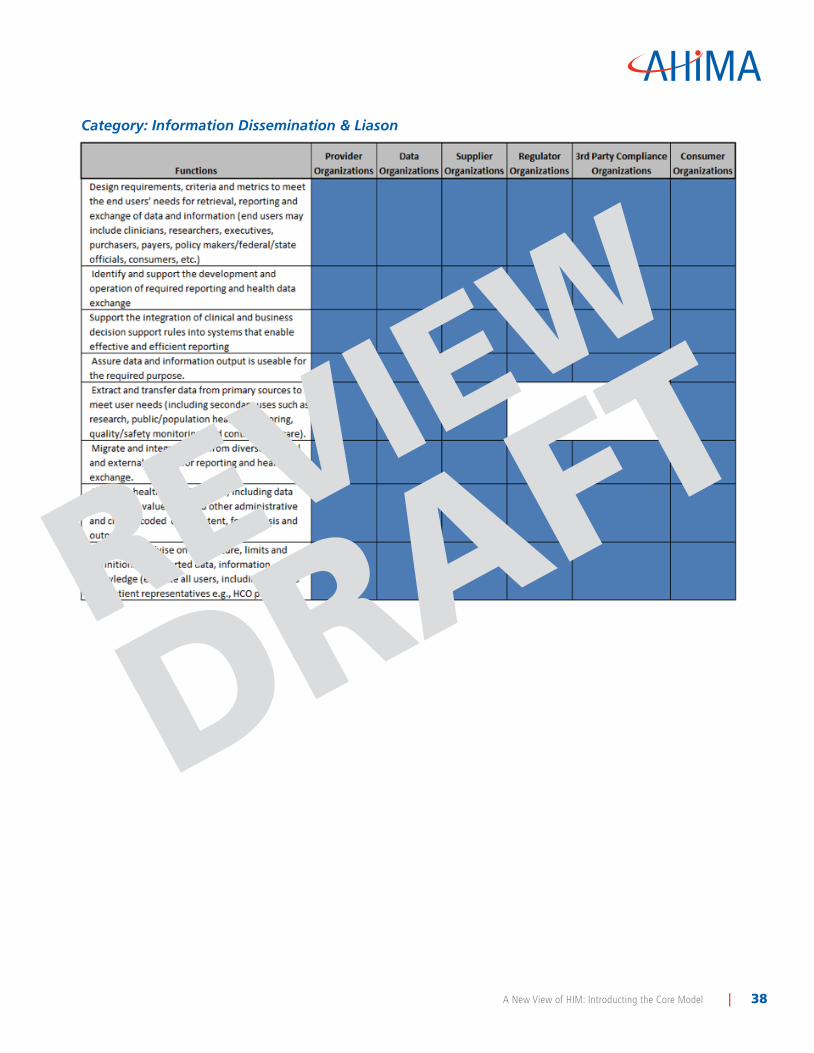
The functional statements were also reviewed from the perspective of the multiple settings in which HIM professionals work today and are anticipated to work in the future. Specific settings were identified and then grouped into nine categories. A matrix of functional statements to settings is attached as Appendix B.
Finally, HIM roles were identified for each element of the Core Model. They were cross matched against healthcare settings to express what roles are or could be present in each healthcare setting. For a list of roles in alphabetic order, see Appendix C.
The Core Model described in this white paper identifies many current and future roles for HIM professionals across the healthcare continuum. It is designed to provoke thoughtful discussion, ideas, and challenges as AHIMA and the HIM profession continue to envision and move toward the future. To send us your feedback, write to us at “Core Model” via AHIMA, 233 N. Michigan Avenue, 21st floor, Chicago, IL 60601 or [email protected].
HIMCore_9-28.indd 4 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 5
DRAFTREVIEW
IntroductionAHIMA’s Pocket Glossary of Health Information Management and Technology defines health information management (HIM) as “an allied health profession that is responsible for ensuring the availability, accuracy, and protection of the clinical information that is needed to deliver healthcare services and to make appropriate healthcare-related decisions.”
As healthcare evolves and becomes more dependent on technology, a contemporary view of HIM and the role of the HIM professional must evolve. Health information management is the practice of collecting, assessing the completeness of, maintaining, and sharing (as authorized) patient information through paper-based and electronic means. It is practiced in provider, payer, research, and governmental settings, as well as in health information exchanges and other settings that provide healthcare or maintenance of health records. With the widespread adoption of electronic health records and other technology-based information sources and the use of the electronically available data for healthcare management measurement purposes, research functions, and governmental initiatives, health informatics and health information technology are being increasingly utilized in HIM practices in the healthcare industry.
A Call for a New Professional Core ModelAs a profession, HIM must become savvy in its use of technology and data analytic tools in order to better serve patients, inform policy leaders, and move into the 21st century and beyond. To meet the needs of various healthcare organizations in their use of emerging technologies, HIM professionals need to be involved at an executive level where decisions are made regarding the design, implementation, and use of technology from a systems approach.
From an operational perspective this would suggest involvement in the adoption and implementation of systemwide technology; the use of data to improve patient care and reduce cost; and a role as leaders who define future policies and procedures as they relate to the privacy and security of the organization.
In 2011 AHIMA brought together HIM experts to identify the roles, settings, and impact of the profession through the next decade. The group extended and advanced a draft core model of HIM functions into a description of the desired future state of HIM roles as they will be performed across the healthcare industry. The group’s aim was to articulate desired HIM professional roles across industry settings in order to:
• Identify and specify the future scope of HIM practice functions and roles
• Identify and specify the value of such roles to society, the health industry, current and future employers of HIM professionals, and current and future HIM professionals
• Differentiate HIM from other related disciplines
• Provide a professional scope of practice that clarifies the role of AHIMA in serving the industry
• Enable follow-on work (phases)
HIMCore_9-28.indd 5 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 6
DRAFTREVIEW
Background - Developing the New Core Model To address the evolving definition of the HIM professional and their role, the AHIMA Board of Directors engaged in a comprehensive environmental scan of the health information landscape. Through scenario planning and alternate future analysis, it became apparent that a new view of HIM was required to address changing practice roles, settings, and functions emerging from increased automation, changing regulations, and dissemination of data. The Board conducted initial work to redefine a model for HIM practice. A draft HIM Core Model was developed to describe a robust set of functions and opportunities open to current and future HIM professionals. The draft model was validated and refined with stakeholders including state association leaders, committee members, members attending CSA meetings and AHIMA professional staff. The input resulted in a broadening of the model components and functional statements to better reflect the HIM profession. To further vet the model, the AHIMA House of Delegates compared and contrasted the of HIM professionals functions in applied health informatics roles and other informatics disciplines.
To further refine the model and ensure it accurately captured emerging HIM functions, roles, and settings, a task force was charged to research and evaluate up-and-coming roles in healthcare in the next 10 years, health informatics functions within the HIM domain, and the broad array of settings where HIM professionals work today and in the future. Review of the HIM Core Model was coordinated with the Canadian Health Information Management Association staff and members to discuss future functions within HIM. This discussion resulted in further refinement of the model, particularly with regard to data display and interpretation. The final vetting of the HIM Core Model was conducted in March 2011 at the AHIMA Winter Team Talks in Washington, DC, and Las Vegas.
HIMCore_9-28.indd 6 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 7
A New HIM Profession Core ModelThe new HIM Core Model embodies current and emerging roles and functions for the profession (Diagram 1). As an October 2011 Journal of AHIMA article by Cassidy et al. states, at the center of the Core Model is the HIM professional’s direct interaction with patient level health information. The interactions are shaped by information governance and stewardship responsibilities. HIM’s skills in managing the resources, processes, and innovations within the health information environment continue to be a valued function and role into the future. A focus on quality and patient safety was also added and will be explored in later iterations.
Diagram 1:The HIM Profession Core Model
Functional Components and Statements A combination of extensive literature review, domain expert input, and collaboration with the Canadian Health Information Management Association, informed the development of the model’s functional components. Each functional component of the model is further defined by a set of functional statements. The functional statements were designed from with a broad perspective in mind to accommodate the multiple settings in which HIM professionals work. A comprehensive list of functional statements is contained in Appendix A.
DRAFTREVIEW
HIMCore_9-28.indd 7 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 8
DRAFTREVIEW
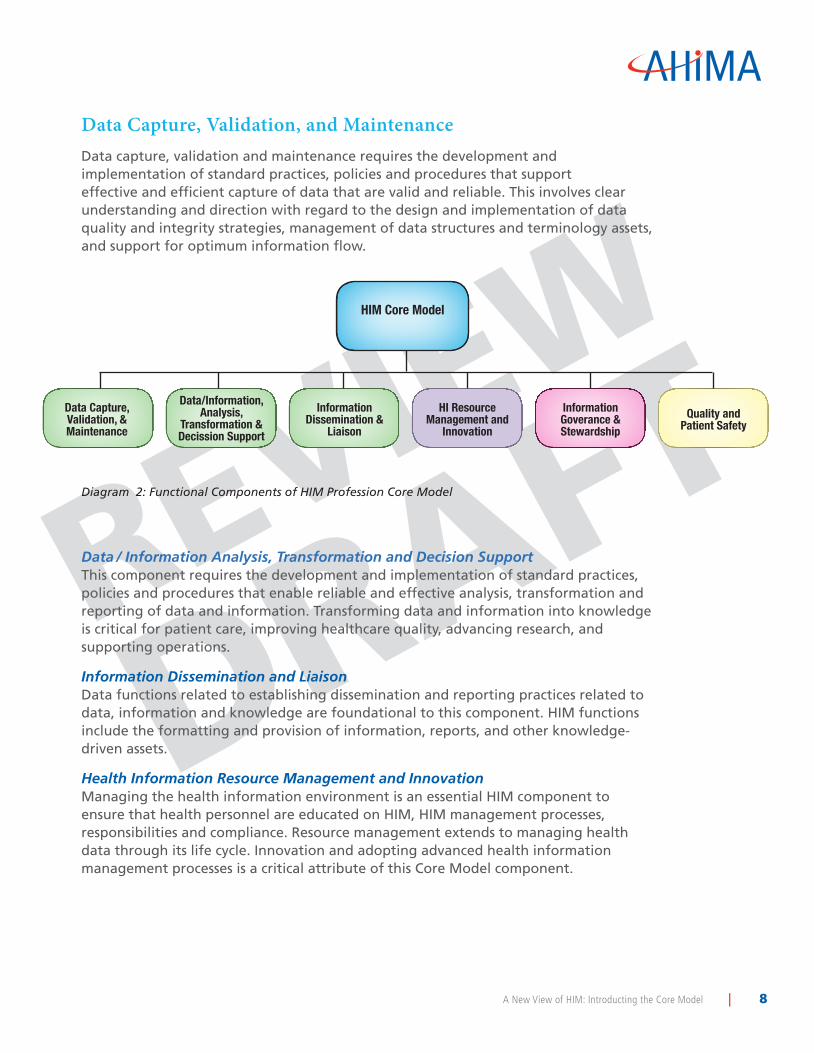
Data Capture, Validation, and MaintenanceData capture, validation and maintenance requires the development and implementation of standard practices, policies and procedures that support effective and efficient capture of data that are valid and reliable. This involves clear understanding and direction with regard to the design and implementation of data quality and integrity strategies, management of data structures and terminology assets, and support for optimum information flow.
Diagram 2: Functional Components of HIM Profession Core Model
Data / Information Analysis, Transformation and Decision SupportThis component requires the development and implementation of standard practices, policies and procedures that enable reliable and effective analysis, transformation and reporting of data and information. Transforming data and information into knowledge is critical for patient care, improving healthcare quality, advancing research, and supporting operations.
Information Dissemination and LiaisonData functions related to establishing dissemination and reporting practices related to data, information and knowledge are foundational to this component. HIM functions include the formatting and provision of information, reports, and other knowledge-driven assets.
Health Information Resource Management and InnovationManaging the health information environment is an essential HIM component to ensure that health personnel are educated on HIM, HIM management processes, responsibilities and compliance. Resource management extends to managing health data through its life cycle. Innovation and adopting advanced health information management processes is a critical attribute of this Core Model component.
Data/Information, Analysis,
Transformation & Decission Support
HIM Core Model
Data Capture, Validation, & Maintenance
Information Dissemination &
Liaison
HI Resource Management and
Innovation
Information Goverance & Stewardship
Quality and Patient Safety
HIMCore_9-28.indd 8 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 9
DRAFTREVIEW
Information Governance and StewardshipInformation governance provide a foundation the other data-driven functions in the Core Model by providing parameters based on organizational and compliance policies, processes, decision-rights and responsibilities. Governance functions and stewardship ensure the use and management of health information is compliant with jurisdictional law, regulation, standards, and organizational policies. As stewards of health information, HIM roles and functions strive to protect and assure the ethical use of health information.
Core Model ExtensionsFour areas of HIM practice were identified that do not include direct interaction with patient level health information, but require an understanding of HIM and additional unique knowledge, leadership, and innovation. These “extenders” serve two purposes. First, to describe additional roles for HIM professionals outside but related to the core functions. Second, to describe operations that enhance and extend the core functions. Education, policy, research, and standards are key enablers that support, advance, extend and contribute to the evolution of the functional components and of the core model as a whole.
ResearchHIM research advances and validates best practice. Research also increases and enhances HIM’s contribution to patient safety and the quality of care. It identifies areas of risk and where improvements in practice are required. The research extension serves to understand and advance the practice. HIM researchers need to be proficient in research methodology and statistics.
PolicyThe healthcare industry is highly regulated in order to protect patients and the public interest. HIM policy is expressed in laws and regulations that protect patients and their privacy. Regulations control the appropriate flow of public funds and regulate the insurance industry. Policy is also important in establishing public health standards and to codify best practice. The policy extension of the Core Model addresses the advancement of HIM principles and professional standards by influencing government policy and shaping and leading HIM policy at all levels of healthcare organizations. Along with standards, this extension interfaces with a variety of other industry stakeholders to a high degree.
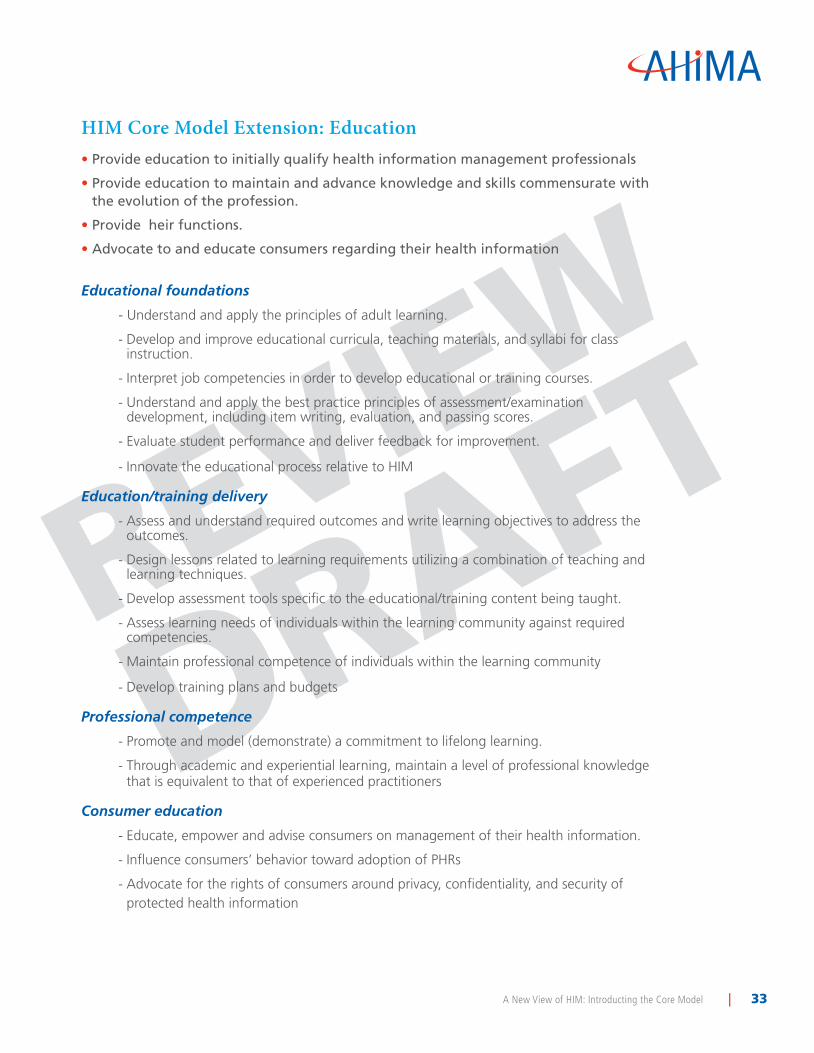
EducationHIM education defines and builds competence for those entering and working in the field. It promulgates best practice and creates professionals for the future. The education extension of the model addresses the formal academic education that is provided in colleges and universities as well as the delivery of continuing professional education. Where there are HIM professionals whose primary function is to develop and deliver training to end users or to consumers, these functions are included in this extension. The functions in this extension also apply to all HIM professionals who have an obligation to maintain their professional competence through a commitment to lifelong learning.
HIMCore_9-28.indd 9 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 10
DRAFTREVIEW
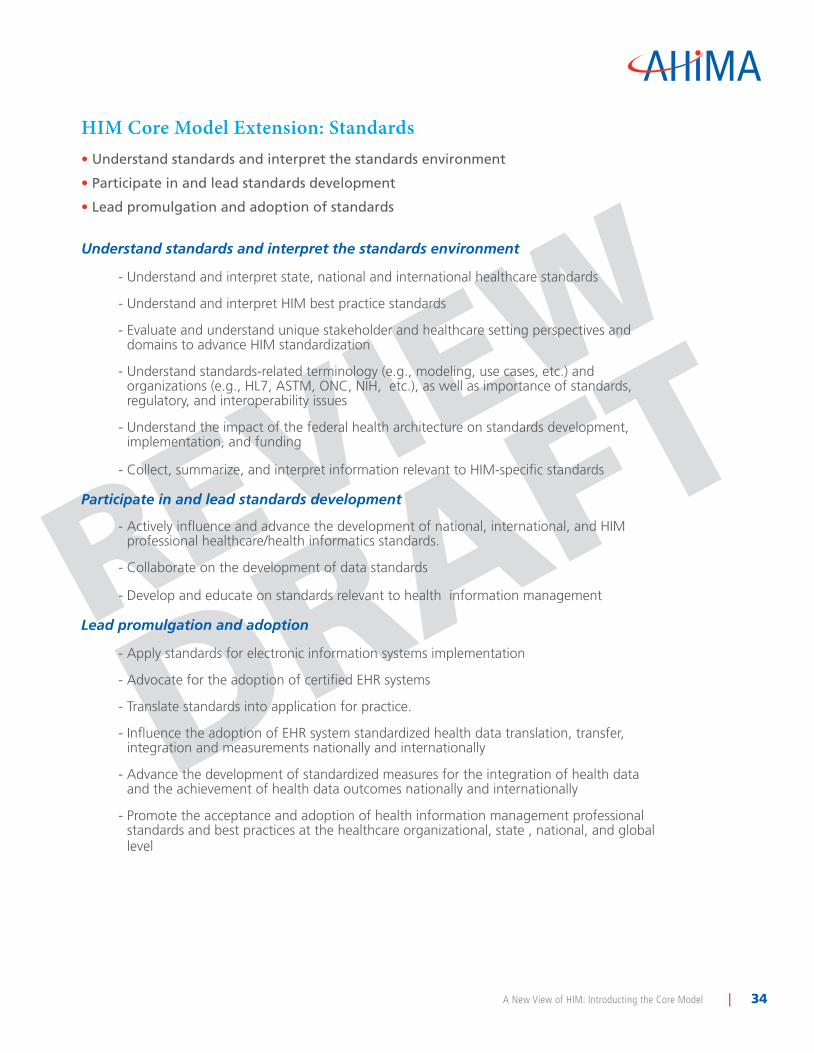
StandardsStandards advance HIM practice by creating uniform approaches to interoperability at the technical and semantic level. Standards reduce costs and support the transfer of information to support care. Standards also streamline development and adoption of technology and data methods. The Standards extension requires an understanding of the unique stakeholder and healthcare setting perspectives and domains to advance HIM standardization. These domains have been defined by the Office of the National Coordinator for Health Information Technology as provider perspective; consumer perspective; public health perspective; care management and delivery domain; health information domain; confidentiality, privacy and security domain; infrastructure, interoperability and exchange domain; administrative and financial domain; and quality measurement and assessment domain.
Settings of Practice for Health Information ManagementAs the delivery of healthcare has diversified over the last 30 years from acute care hospitals to a wide spectrum of ambulatory and specialty centers, health information management professionals’ work settings have followed a similar diversification pattern. These changes continue as new models for healthcare delivery, payment, and monitoring are formed. Added to that is the increased production of and reliance on healthcare data generated by electronic health records and ancillary data capture systems. This expansion of the availability of personal health information now extends to the patient themselves. As health information is shared and used more widely, HIM work settings expand accordingly.
HIM functions are performed where personal health information exists, where there is a need for health data and/or information, and where products and services for managing health data and/or information are designed. Where there is health information, there is HIM. To identify the near-future state work settings where HIM professionals will add value, the team examined three sources of data in addition to knowledge of the changes occurring in healthcare delivery. The literature review suggested some settings, a search of job postings specifically to identify new work settings and a search of the AHIMA profile database to identify those “other” job settings identified by current members that suggest future potential. Specific settings were identified and then grouped into nine categories:
• Healthcare Provider Organizations
• Healthcare Data Organizations
• Healthcare Payer Organizations
• Healthcare Supplier Organizations
• Planning Organizations, Regulators, and Industry Support
• Educational Institutions
• Research Institutions
• Third-Party Compliance Organizations
• Consumer Organizations
HIMCore_9-28.indd 10 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 11
DRAFTREVIEW
Roles and Value HIM roles were identified for each element of the core model. They were cross matched against healthcare settings to express what roles are or could be present in each healthcare setting. The value of each function and role were discussed and are expressed in the table below.
Data Capture, Validation, and Maintenance
Roles
Chart correction analyst
Classification editor and exchange expert
Clinical coding validator
Clinical content manager
Clinical documentation improvement specialist/supervisor
Coder
Coding compliance coordinator/supervisor/manager
Computer assisted coding validation practice leader
Data architect
Data capture design specialist
Data dictionary manager
Data integrity and transitions specialist/auditor
Data mapper/translator
Data quality manager/analyst
Documentation/EHR trainer
EHR content manager
Enterprise patient master index data integrity analyst
ICD-10 implementation specialist
Information workflow designer
Patient identity manager
Registrar (Birth, Cancer, Device, Bone marrow, tissue)
Research coordinator/associate
Research data abstractor
Terminology asset manager
Voice capture specialist
Value
• Increased revenue potential by assuring accurate coding supported by documentation
• Improved cash flow caused by first time claims processing with few denials and appeals required
• Improved efficiency of data capture through section and implementation of technology
• Decreased operational costs by efficiencies gained in workflow
• Increased patient safety and satisfaction by reduction of duplicate records
• Increase in patient safety and satisfaction through standardized data collection across systems and sites
• Improved research outcomes through optimized data capture and abstraction.
• Increased value and accuracy of information through planning for the capture of discrete data
HIMCore_9-28.indd 11 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 12
DRAFTREVIEW
Data/Information Analysis, Transformation, and Decision Support
Roles
Business analyst
Claims data analyst
Clinical data analyst
Clinical content manager
Data abstractor/coordinator
Data architect
Data integration manager/analyst
Data integrity and transitions specialist/auditor
Data quality manager/analyst
Data repository architect/manager/analyst
Decision support analyst
Decision support officer
Health data analyst/manager/director
Health data statistician
Health outcomes analyst
Healthcare data quality engineer
Information warehouse/repository director
Interface reconciliation specialist
Patient centered outcomes researcher
Quality outcomes and cost analyst/director
Physician practice liaison
Record analyst
Referral specialist
Regional health information management specialist/manager/administrator
Registrar (Birth, Cancer, Device, Bone
marrow, tissue)
Report writer
Research coordinator/associate
Values
• Increased strategic value of data through informed presentation of payor mix and case mix index
• Compliance with mandated reporting requirements
• Information available to assess and improve patient care delivery and outcomes
• Information provided for marketing to the public
• Minimize the risk of exposure to the practice by improving the quality outcomes
HIMCore_9-28.indd 12 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 13
DRAFTREVIEW
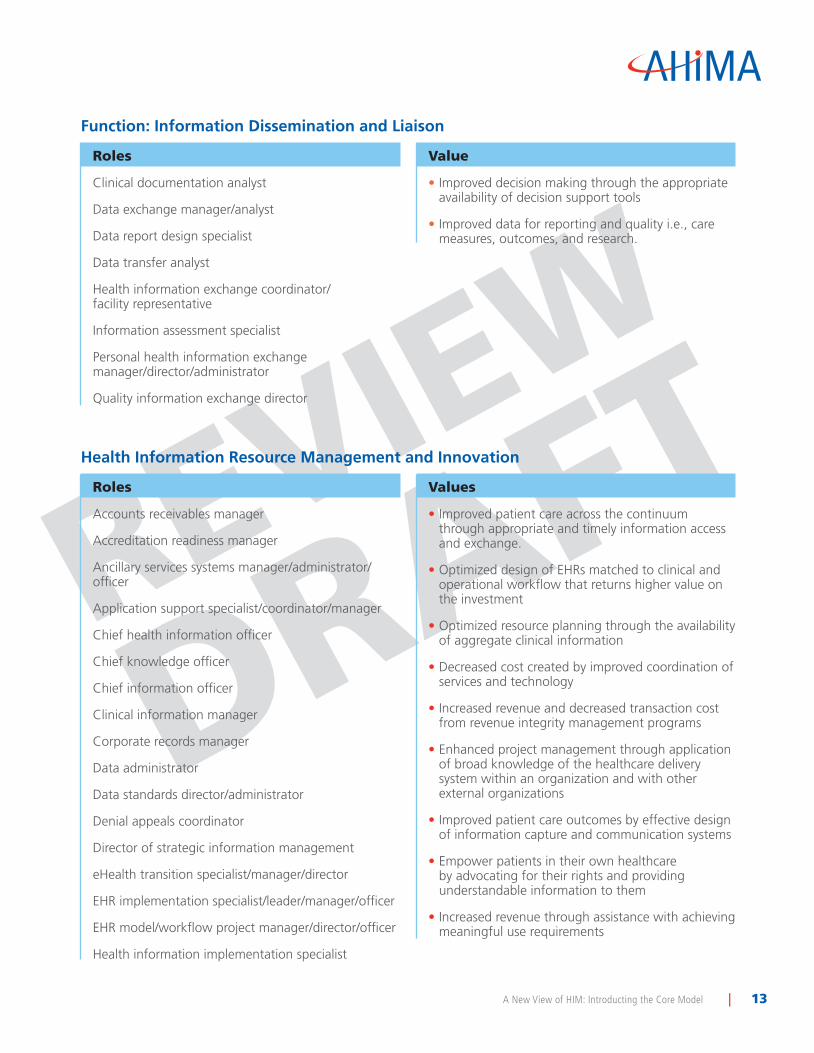
Function: Information Dissemination and Liaison
Roles
Clinical documentation analyst
Data exchange manager/analyst
Data report design specialist
Data transfer analyst
Health information exchange coordinator/ facility representative
Information assessment specialist
Personal health information exchange manager/director/administrator
Quality information exchange director
Value
• Improved decision making through the appropriate availability of decision support tools
• Improved data for reporting and quality i.e., care measures, outcomes, and research.
Health Information Resource Management and Innovation
Roles
Accounts receivables manager
Accreditation readiness manager
Ancillary services systems manager/administrator/officer
Application support specialist/coordinator/manager
Chief health information officer
Chief knowledge officer
Chief information officer
Clinical information manager
Corporate records manager
Data administrator
Data standards director/administrator
Denial appeals coordinator
Director of strategic information management
eHealth transition specialist/manager/director
EHR implementation specialist/leader/manager/officer
EHR model/workflow project manager/director/officer
Health information implementation specialist
Values
• Improved patient care across the continuum through appropriate and timely information access and exchange.
• Optimized design of EHRs matched to clinical and operational workflow that returns higher value on the investment
• Optimized resource planning through the availability of aggregate clinical information
• Decreased cost created by improved coordination of services and technology
• Increased revenue and decreased transaction cost from revenue integrity management programs
• Enhanced project management through application of broad knowledge of the healthcare delivery system within an organization and with other external organizations
• Improved patient care outcomes by effective design of information capture and communication systems
• Empower patients in their own healthcare by advocating for their rights and providing understandable information to them
• Increased revenue through assistance with achieving meaningful use requirements
HIMCore_9-28.indd 13 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 14
DRAFTREVIEW
Health Information Resource Management and Innovation (continued)
Roles
Health information interoperability and standards specialist/administrator
Health information project officer
Health information trainer
HIM application support specialist/manager
HIM integrity specialist/manager
HIM manager
Implementations redesign specialist/tester
Informatics specialist
Information operations manager/administrator/officer
Information resource manager
Local/ regional policy analyst/officer
National health data coordinator
Nationwide health information management specialist/manager/ director/officer performance improvement specialist
Project manager
Quality improvement coordinator/advisor
Quality improvement director
Quality outcomes project manager/analyst/director
Physician health information liaisons
Regional health information management specialist/manager/administrator
Registrar (Birth, Cancer, Device, Bone marrow, tissue)
Reimbursement specialist
Revenue integrity analyst
Systems analyst
Vice president of data integrity services
Vice president of strategic information development
Workflow design analyst
Values
• Reduced healthcare costs by ensuring reliable data that eliminates duplicate tests and record keeping practices
• Improved adoption of EHRs through effective training
• Enhanced relationship between hospitals and physicians through coordinated HIM resources
HIMCore_9-28.indd 14 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 15
DRAFTREVIEW
Function: Information Governance and Stewardship
Roles
Access manager/auditor
Accounting of disclosures coordinator
Compliance officer/auditor
Electronic discovery auditor
Health information exchange privacy gatekeeper
Health record advocate
Healthcare consumer access manager
Healthcare fraud investigator/analyst
Health information security analyst
HIM government relations specialist/consultant
Information analyst for business continuity
Patient advocate
Personal health record advisor
Privacy and security officer/auditor
Public relations liaison
Recovery audit coordinator
Vice president of health information governance
Value
• Decreased risk of litigation based on appropriate retention of data
• Increased compliance with current laws and regulations
• Decreased liability and enhanced reputation through reduction of breaches
• Decreased liability through maintenance of an accurate and complete clinical record
• Optimized access to information through processes and technology that maintain confidentiality and security
HIMCore_9-28.indd 15 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 16
DRAFTREVIEW
BibliographyAkesson, Kerstin M., Britt-Inger Saveman, and Gunilla Nilsson. “Health Care Consumers’ Experi-ences of Information Communication Technology--A Summary of Literature.” International Jour-nal of Medical Informatics 76, no. 9 (September 2007): 633-645. http://www.ncbi.nlm.nih.gov/pubmed/16931133.
Alamantariotou, Kleopatra, and Dimitra Zisi. “Consumer Health Informatics and Interactive Visual Learning Tools for Health.” International Journal of Electronic Healthcare 5, no. 4 (2010): 414-424. http://www.ncbi.nlm.nih.gov/pubmed/21041179.
Alpay, Laurence, John Verhoef, Bo Xie, Dov Te’eni, and J. H. M. Zwetsloot-Schonk. “Current Chal-lenge in Consumer Health Informatics: Bridging the Gap between Access to Information and Infor-mation Understanding.” Biomedical Informatics Insights 2, no. 1 (January 1, 2009): 1-10. http://www.ncbi.nlm.nih.gov/pubmed/20419038.
American Health Information Management Association. House of Delegates. Health Information Management Higher Education and Workforce Team. “Clinical Practice Sites/Professional Practice Experience (PPE) Guide.” (January 2011). http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_048644.pdf
AHIMA House of Delegates Forum. Health Informatics: Definition and Discussion (October 2010). Available in the AHIMA Communities of Practice.
AHIMA. Pocket Glossary of Health Information Management and Technology. Chicago, IL: 2010.
AHIMA. “Profile Results Show Members Thrive in Non-traditional Settings.” AHIMA Advantage (June 2005). Available in the AHIMA Communities of Practice.
American Medical Informatics Association. “Informatics Academic and Training Programs.” https://www.amia.org/informatics-academic-training-programs
Australian Health Informatics Education Council. “Strategic Work Plan, 2009-10 and Beyond.” June 2009. http://www.ahiec.org.au/docs/AHIEC%20Workplan%20v2_2%2022%20June.doc
Bakker, Theodora A., Andrea N. Ryce, Robert A. Logan, Tony Tse, and Lidia Hutcherson. “A Con-sumer Health Informatics (CHI) Toolbox: Challenges and Implications.” AMIA ... Annual Symposium Proceedings / AMIA Symposium. AMIA Symposium (2005): 21-25. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1479846/?tool=pubmed
Barr, Paul J., James C. McElnay, and Carmel M. Hughes. “Connected Health Care: The Future of Health Care and the Role of the Pharmacist.” Journal of Evaluation in Clinical Practice (August 3, 2010). http://www.ncbi.nlm.nih.gov/pubmed/20698917.
Bernstam, Elmer V., Jack W. Smith, and Todd R. Johnson. “What is Biomedical Informatics?” Journal of Biomedical Informatics 43, no. 1 (February 2010): 104-110. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2814957/.
Bernstam, Elmer V., William R. Hersh, Ida Sim, David Eichmann, Jonathan C. Silverstein, Jack W. Smith, and Michael J. Becich. “Unintended Consequences of Health Information Technology: A Need for Biomedical Informatics.” Journal of Biomedical Informatics 43, no. 5 (October 2010): 828-830. http://www.ncbi.nlm.nih.gov/pubmed/19508898.
HIMCore_9-28.indd 16 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 17
DRAFTREVIEW
BibliographyCaballero Muñoz, Erika, and Carola M. Hullin Lucay Cossio. “Engaging Clinicians in Health Informat-ics Projects.” Studies in Health Technology and Informatics 151 (2010): 195-206. http://www.ncbi.nlm.nih.gov/pubmed/20407162.
Canadian Health Information Management Association. Learning Outcomes for Health Information Management. Diploma/Degree Programs. 2010. https://www.echima.ca/media/documents/2010_LO-HIM_Final.pdf
Carty, Barbara, and Kathleen Kenney. “Consumer informatics in Primary Care.” Studies in Health Technology and Informatics 122 (2006): 36-37. http://www.ncbi.nlm.nih.gov/pubmed/17102213.
Cassidy, Bonnie S., et al. “Teaching the Future: An Educational Response to the AHIMA Core Model.” Journal of AHIMA 82, no.10 (October 2011): 34-38. Available in the AHIMA Body of Knowledge.
Cooper, H. “Changing Roles of Health Information Managers: an Education Perspective.” Health Information Management Journal 38, no. 3 (2009): 38-42. http://www.himaa.org.au/ members/jour-nal/HIMJ_38_3_2009/Cooper_Changing_roles_of_HIMs.pdf.
Covvey, H. Dominic, David Zitner, and Robert M. Bernstein. Pointing the Way: Competencies and Curricula in Health Informatics, 2001. http://www.cs.uwaterloo.ca/health_info/health_docs/ Curricu-laMASTERDocumentVersion1Final.zip.
D’Avolio, Leonard W., Wildon R. Farwell, and Louis D. Fiore. “Comparative Effectiveness Research and Medical Informatics.” The American Journal of Medicine 123, no. 12 (December 2010): e32-37. http://www.ncbi.nlm.nih.gov/pubmed/21184865.
DeShazo, Jonathan, Donna LaVallie, and Fredric Wolf. “Publication Trends in the Medical Informatics Literature: 20 years of ‘Medical Informatics’ in MeSH.” BMC Medical Informatics and Decision Mak-ing 9, no. 1 (2009): 7. http://www.biomedcentral.com/1472-6947/9/7.
Detmer, Don, Meryl Bloomrosen, Brian Raymond, and Paul Tang. “Integrated Personal Health Re-cords: Transformative Tools for Consumer-centric Care.” BMC Medical Informatics and Decision Mak-ing 8 (2008): 45. http://www.ncbi.nlm.nih.gov/pubmed/18837999.
Dey, Aditi. “Consumer Health Informatics: An Overview of Patient Perspectives on Health In-formation Needs.” The HIM Journal 33, no. 4 (2004): 121-126. http://www.ncbi.nlm.nih.gov/pubmed/18239231.
DiLaura, Robert, Fran Turisco, Cherri McGrew, Stephanie Reel, John Glaser, and William F. Crow-ley. “Use of Informatics and Information Technologies in the Clinical Research Enterprise within US Academic Medical Centers: Progress and Challenges from 2005 to 2007.” Journal of Investigative Medicine: The Official Publication of the American Federation for Clinical Research 56, no. 5 (June 2008): 770-779. http://www.ncbi.nlm.nih.gov/pubmed/18525452.
Feldman, Sue S., and William Hersh. “Evaluating the AMIA-OHSU 10x10 Program to Train Health-care Professionals in Medical Informatics.” AMIA ... Annual Symposium Proceedings / AMIA Symposium. AMIA Symposium (2008): 182-186. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2656028/?tool=pubmed.
Fox, Brent I. “Informatics and the Medication Use Process.” In Building Core Competencies in Phar-macy Informatics. Portland, OR: American Pharmacists Assn., 2010. http://www.pharmacist.com/AM/Template.cfm?Section=Home2&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=23921.
HIMCore_9-28.indd 17 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 18
DRAFTREVIEW
BibliographyFriede, A., H. L. Blum, and M. McDonald. “Public Health Informatics: How Information-Age Technol-ogy Can Strengthen Public Health.” Annual Review of Public Health 16 (1995): 239-252. http://www.ncbi.nlm.nih.gov/pubmed/7639873.
Friedman, C., and U. Abbas. “Is Medical Informatics a Mature Science? A Review of Measurement Practice in Outcome Studies of Clinical Systems.” Int J Med Inform 69, no. 2 (2003): 261 - 72. http://www.ncbi.nlm.nih.gov/pubmed/2405204.
Friedman, Charles P. “A ‘Fundamental Theorem’ of Biomedical Informatics.” Journal of the American Medical Informatics Association: JAMIA 16, no. 2 (April 2009): 169-170. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2649317.
Gassert, Carole A. “Technology and Informatics Competencies.” The Nursing Clinics of North America 43, no. 4 (December 2008): 507-521, v. http://www.ncbi.nlm.nih.gov/pubmed/18940408.
Geyer, Enid M., and D. Elizabeth Irish. “Isolated to Integrated: An Evolving Medical Informatics Cur-riculum.” Medical Reference Services Quarterly 27, no. 4 (2008): 451-461. http://www.ncbi.nlm.nih.gov/pubmed/19042724.
Giuse, Nunzia B., Annette M. Williams, and Dario A. Giuse. “Integrating Best Evidence into Pa-tient Care: A Process Facilitated by a Seamless Integration with Informatics Tools.” Journal of the Medical Library Association: JMLA 98, no. 3 (July 2010): 220-222. http://www.ncbi.nlm.nih.gov/pubmed/20648255.
Golob, Joseph F., Adam M. A. Fadlalla, Justin A. Kan, Nilam P. Patel, Charles J. Yowler, and Jeffrey A. Claridge. “Validation of Surgical Intensive Care-Infection Registry: A Medical Informatics System for Intensive Care Unit Research, Quality of Care Improvement, and Daily Patient Care.” Journal of the American College of Surgeons 207, no. 2 (August 2008): 164-173. http://www.ncbi.nlm.nih.gov/pubmed/18656042.
Greenes, R. A., and E. H. Shortliffe. “Medical Informatics. An Emerging Academic Discipline and Institutional Priority.” JAMA 263, no. 8 (1990): 1114 - 1120. http://www.ncbi.nlm.nih.gov/pubmed/2405204.
Greenes, Robert A., and Edward H. Shortliffe. “Commentary: Informatics in Biomedicine and Health Care.” Academic Medicine: Journal of the Association of American Medical Colleges 84, no. 7 (July 2009): 818-820. http://www.ncbi.nlm.nih.gov/pubmed/19550167.
Greenes, Robert A. “Informatics and a Health Care Strategy for the Future--General Directions.” Studies in Health Technology and Informatics 149 (2009): 21-28. http://www.ncbi.nlm.nih.gov/pubmed/19745469.
Guenther, J. T. “Mapping the Literature of Nursing Informatics.” J Med Libr Assoc 94, no. 2 (2006): E92 - E98. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1463042/pdf/i1536-5050-094-02S-0092.pdf.
Hagland, Mark. “Is there a Pharmacist in the House?” Healthcare Informatics 27, no. 12 (December 2010): 18, 20, 22.
Hagland, Mark. “Rowing Together.” Healthcare Informatics 27, no. 7 (July 2010): 8-13.
Hagland, Mark. “Two revolutions.” Healthcare Informatics 27, no. 7 (July 2010): 6.
HIMCore_9-28.indd 18 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 19
DRAFTREVIEW
BibliographyHaux, Reinhold. “Health Care and Informatics: On IMIA’s Opportunities and Responsibilities in its 5th Decade.” Yearbook of Medical Informatics (2008): 1-6. http://www.schattauer.de/en/magazine/sub-ject-areas/journals-a-z/imia-yearbook/imia-yearbook-2008/issue/special/manuscript/9809/download.html.
Health Informatics Society of Australia. “A Review of the Australian Health Informatics Workforce.” Melbourne: Australian Department of Health and Aging, Sept. 2009. http://www.hisa.org.au/system/files/u2233/Australian_Health_Informatics_Workforce_Review_v1_1.pdf
Hersh, W. “Medical Informatics: Improving Health Care through Information.” JAMA 288, no. 16 (2002): 1955 - 8. http://www.ncbi.nlm.nih.gov/pubmed/16710469.
Hersh, William R., Ravi Teja Bhupatiraju, Peter Greene, Valerie Smothers, and Cheryl Cohen. “Adopt-ing e-Learning Standards in Health Care: Competency-Based Learning in the Medical Informatics Domain.” AMIA ... Annual Symposium Proceedings / AMIA Symposium. AMIA Symposium (2006): 334-338. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1839696/.
Hersh, William. “A Stimulus to Define Informatics and Health Information Technology.” BMC Medi-cal Informatics and Decision Making 9, no. 1 (2009): 24. http://www.biomedcentral.com/1472-6947/9/24.
Hersh, William. “The Health Informatics Workforce: Unanswered Questions, Needed Answers.” Studies in Health Technology and Informatics 151 (2010): 492-503. http://www.ncbi.nlm.nih.gov/pubmed/20407181.
Hersh, William. “Health and Biomedical Informatics: Opportunities and Challenges for a Twenty-First Century Profession and Its Education.” Yearbook of Medical Informatics (2008): 157-164. http://www.ncbi.nlm.nih.gov/pubmed/18660890.
Hersh, William, and Adam Wright. “What Workforce is Needed to Implement the Health Informa-tion Technology Agenda? Analysis from the HIMSS Analytics Database.” AMIA ... Annual Symposium Proceedings / AMIA Symposium. AMIA Symposium (2008): 303-307. http://www.ncbi.nlm.nih.gov/pubmed/18998990.
Hersh, William. “The Health Informatics Workforce: Unanswered Questions, Needed Answers.” Studies in Health Technology and Informatics 151 (2010): 492-503. http://www.ncbi.nlm.nih.gov/pubmed/20407181.
Ho, Jessica. “Consumer Health Informatics.” Studies in Health Technology and Informatics 151 (2010): 185-194. http://www.ncbi.nlm.nih.gov/pubmed/20407161.
Houston, T. K., B. L. Chang, S. Brown, and R. Kukafka. “Consumer Health Informatics: A Consensus Description and Commentary from American Medical Informatics Association Members.” Proceed-ings / AMIA ... Annual Symposium. AMIA Symposium (2001): 269-273. http://www.ncbi.nlm.nih.gov/pubmed/11825193.
Hovenga, Evelyn J. S. “Health Care Services, Information Systems and Sustainability.” Stud-ies in Health Technology and Informatics 151 (2010): 16-29. http://www.ncbi.nlm.nih.gov/pubmed/20407149.
Hovenga, Evelyn J. S., Michael R. Kidd, Sebastian Garde, and Carola Hullin Lucay Cossio. “Health Informatics - An Introduction.” Studies in Health Technology and Informatics 151 (2010): 9-15. http://www.ncbi.nlm.nih.gov/pubmed/20407148.
HIMCore_9-28.indd 19 9/28/11 10:24 AM
A New View of HIM: Introducing the Core Model | 20
DRAFTREVIEW
BibliographyHovenga, E.J.S., M.R. Kidd, S. Garde, and C. Hullin Lucay Cossio. Health Informatics: An Overview. IOS Press, 2010.
Hovenga, Evelyn J.S. National and International Informatics Workforce and Education Initiatives, Methodologies Used and Outcomes Achieved: a Review of the Literature. Australian Health Informat-ics Education Council, January 2010. http://www.ahiec.org.au/docs/HI%20lit%20review%20-%20workforce%20and%20education%20initiatives.docx
Hufnagle, Kristin. “Registered Health Information Administrators are Being Challenged to Fill New and Non-Traditional Health Information Management Roles in the 21st Century.” Capstone Paper, Stephens College, April 2010.
Kaplan, B, and P F Brennan. “Consumer Informatics Supporting Patients as Co-Producers Of Quality.” Journal of the American Medical Informatics Association: JAMIA 8, no. 4 (August 2001): 309-316. http://www.ncbi.nlm.nih.gov/pubmed/11418537.
Keselman, Alla, Allen C. Browne, and David R. Kaufman. “Consumer Health Information Seeking as Hypothesis Testing.” Journal of the American Medical Informatics Association: JAMIA 15, no. 4 (August 2008): 484-495. http://www.ncbi.nlm.nih.gov/pubmed/18436912.
Keselman, Alla, Robert Logan, Catherine Arnott Smith, Gondy Leroy, and Qing Zeng-Treitler. “Devel-oping Informatics Tools and Strategies for Consumer-centered Health Communication.” Journal of the American Medical Informatics Association : JAMIA 15, no. 4 (2008): 473-483. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2442255/.
Khan, Sharib A., Delano J. McFarlane, Jianhua Li, Jessica S. Ancker, Carly Hutchinson, Alwyn Cohall, and Rita Kukafka. “Healthy Harlem: Empowering Health Consumers Through Social Networking, Tailoring and Web 2.0 Technologies.” AMIA ... Annual Symposium Proceedings / AMIA Symposium. AMIA Symposium (2007): 1007. http://www.ncbi.nlm.nih.gov/pubmed/18694106.
Knaup, P., M. Haag, F. J. Leven, and H. Dickhaus. “Challenges in the Evolution of the Medical Infor-matics Program at Heidelberg/Heilbronn (Germany).” Methods of Information in Medicine 48, no. 1 (2009): 66-75. http://www.ncbi.nlm.nih.gov/pubmed/19151886.
Koch, Sabine, and Maria Hägglund. “Health Informatics and the Delivery of Care to Older People.” Maturitas 63, no. 3 (July 20, 2009): 195-199. http://www.ncbi.nlm.nih.gov/pubmed/19487092.
LaVallie, D. L., and F. M. Wolf. “Publication Trends and Impact Factors in the Medical Informatics Literature.” AMIA Annu Symp Proc (2005): 1018. http://www.ncbi.nlm.nih.gov/pubmed/16779305.
Logan, Robert A, and Tony Tse. “A Multidiscipline Conceptual Framework for Consumer Health In-formatics.” Studies in Health Technology and Informatics 129, no. 2 (2007): 1169-1173. http://www.ncbi.nlm.nih.gov/pubmed/17911899.
Lorenzi, Nancy M. “Towards IMIA 2015--The IMIA Strategic Plan.” Yearbook of Medical Informatics (2007): 1-5. http://www.schattauer.de/en/magazine/subject-areas/journals-a-z/imia-yearbook/imia-yearbook-2007/issue/special/manuscript/8401/download.html.
Mantas, John, Elske Ammenwerth, George Demiris, Arie Hasman, Reinhold Haux, William Hersh, Evelyn Hovenga, et al. “Recommendations of the International Medical Informatics Association (IMIA) on Education in Biomedical and Health Informatics. First Revision.” Methods of Information in Medicine 49, no. 2 (January 7, 2010): 105-120. http://www.schattauer.de/en/magazine/subject-areas/journals-a-z/methods/contents/archive/issue/special/manuscript/12538/download.html
2.
HIMCore_9-28.indd 20 9/28/11 10:24 AM

A New View of HIM: Introducing the Core Model | 21
DRAFTREVIEW
BibliographyMarschollek, M. “Advances in Education and Consumer Health Informatics. Findings from the Sec-tion on Education and Consumer Informatics.” Yearbook of Medical Informatics (2007): 95-97. http://www.ncbi.nlm.nih.gov/pubmed/17700911.
McCullagh, P. J., H. Zheng, N. D. Black, R. Davies, S. Mawson, and K. McGlade. “Section 1: Medi-cal Informatics and eHealth.” Technology and Health Care: Official Journal of the European So-ciety for Engineering and Medicine 16, no. 5 (2008): 381-397. http://www.ncbi.nlm.nih.gov/pubmed/19126977.
McDaniel, Anna M., Debra L. Schutte, and Linda Olson Keller. “Consumer Health Informatics: From Genomics To Population Health.” Nursing Outlook 56, no. 5 (October 2008): 216-223.e3. http://www.ncbi.nlm.nih.gov/pubmed/18922271.
McKinney, Maureen. “Beyond the Data: Inaugural Roster of the Top 25 Clinical Informaticists High-lights the Rising Profile and Influence of These Healthcare Professionals.” Modern Healthcare 40, no. 45 (November 8, 2010): 26, 28, 30 passim. http://www.ncbi.nlm.nih.gov/pubmed/21137149.
McLane, Sharon, and James P. Turley. “Informaticians: How They May Benefit Your Healthcare Orga-nization.” The Journal of Nursing Administration 41, no. 1 (January 2011): 29-35. http://www.ncbi.nlm.nih.gov/pubmed/21157241.
Moehr, J. “Evaluation: Salvation or Nemesis of Medical Informatics?” Comput Biol Med 32, no. 3 (2002): 113 - 25. http://www.ncbi.nlm.nih.gov/pubmed/11922929
Moen, Anne, Judith Gregory, and Patricia Flatley Brennan. “Cross-Cultural Factors Necessary to En-able Design of Flexible Consumer Health Informatics Systems (CHIS).” International Journal of Medi-cal Informatics 76 Suppl 1 (June 2007): S168-173. http://www.ncbi.nlm.nih.gov/pubmed/16781188.
Morris, T. “Structural Relationships Within Medical Informatics.” Proc AMIA Symp (2000): 590 - 4. http://www.ncbi.nlm.nih.gov/pubmed/11079952.
Morris, T. A., and K. W. McCain. “The Structure of Medical Informatics Journal Literature.” J Am Med Inform Assoc 5, no. 5 (1998): 448 - 466. http://www.ncbi.nlm.nih.gov/pubmed/11079952.
Morris, Theodore Allan. “Medical Informatics as a Market for IS/IT.” Proceedings / AMIA ... An-nual Symposium. AMIA Symposium (2002): 538-542. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2244169/
NHS Connecting for Health. “Health Informatics Career Framework – Home.” http://www.hicf.org.uk/.
O’Carroll, P.W; Public Health Informatics Competencies Working Group. “Informatics Competencies for Public Health Professionals.” Seattle, WA: Northwest Center for Public Health Practice. (2002) http://www.nwcphp.org/docs/phi/comps/phi_print.pdf
O’Grady, John. “Health Informatics and Health Information Management: Human Resources Report.” Canada Health Infoway, et al. (November 2009). http://www.ictc-ctic.ca/uploadedFiles/Labour_Mar-ket_Intelligence/eHealth/HIHIM_report_E_web.pdf
Ohmann, C., and W. Kuchinke. “Future Developments Of Medical Informatics from the Viewpoint of Networked Clinical Research. Interoperability and Integration.” Methods of Information in Medicine 48, no. 1 (2009): 45-54. http://www.ncbi.nlm.nih.gov/pubmed/19151883.
HIMCore_9-28.indd 21 9/28/11 10:24 AM











DRAFTREVIEW
HIMCore_9-28.indd 45 9/28/11 10:24 AM

















