24
Introduction to Hemolytic Anemias
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | aubrey-bridges |
| View: | 243 times |
| Download: | 3 times |
Introduction to
Hemolytic Anemias
HEMOLYTIC ANEMIASIntroduction
• Definition
• Pathogenesis
• Classification
• General clinical features
• Laboratory evaluation of hemolysis
Hemolytic AnemiasDefinition• A group of disorders leading to anemia
caused by a reduction in red cell life span.• RBC’s normally survive 60 - 120 days . • Bone marrow has the capacity to increase erythropoiesis
6 - 8 times than normal.
• Anemia is the result of premature destruction of red cells exceeding the erythropoietic capacity of the bone marrow.
Hemolytic Anemias
Classification
• Hemolytic anemias may be classified as
I- Hereditary or acquired
or
II- Intracorpuscular or Extracorpuscular
Hemolysis may occur in two compartments
I- Intravascular
or
II- Extravascular ( eg: spleen )
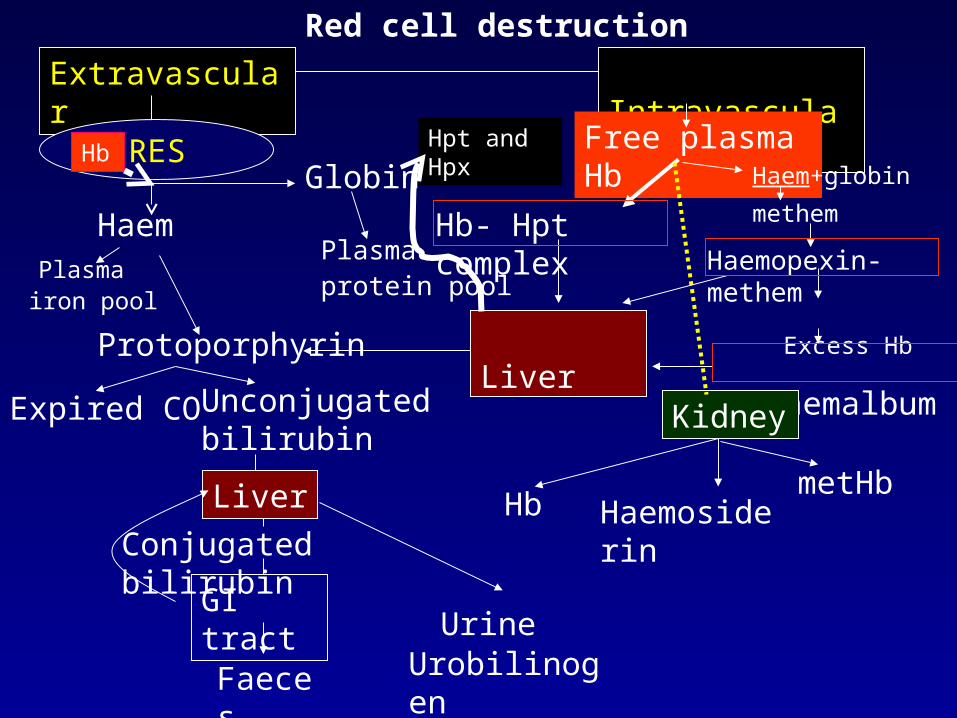
Red cell destruction
Extravascular Intravascular
RES
Haem
Globin
Plasma iron pool
Plasma protein pool
Protoporphyrin
Expired CO Unconjugated bilirubin
Liver
Conjugated bilirubin
GI tract
UrobilinogenFaeces
Urine
Free plasma Hb
Hb- Hpt complex
Liver
Hpt and Hpx
Haemopexin-methem
Excess Hb
methaemalbumin
Kidney
Hb Haemosiderin
Haem+globinHb
methem
metHb
• In some types of hemolytic anemias hemolysis occurs particularly as an intravascular hemolysis.eg: Paroxsysmal nocturnal hemoglobinuria
Traumatic or microangiopathic hem. anemia
(eg:cardiac hemolytic anemia,march hemoglobinuria,TTP)
Acute hemolytic transfusion reaction etc
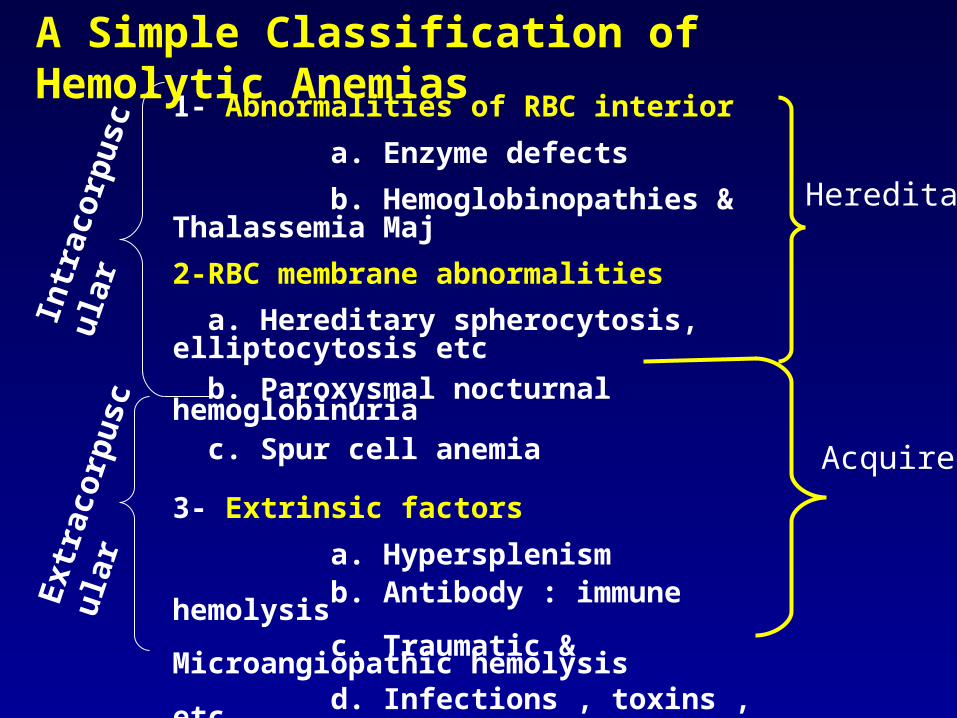
1- Abnormalities of RBC interior
a. Enzyme defects
b. Hemoglobinopathies & Thalassemia Maj
2-RBC membrane abnormalities
a. Hereditary spherocytosis, elliptocytosis etc
b. Paroxysmal nocturnal hemoglobinuria c. Spur cell anemia
3- Extrinsic factors
a. Hypersplenism b. Antibody : immune hemolysis c. Traumatic & Microangiopathic hemolysis d. Infections , toxins , etc
Intr
acor
pusc
ular
Ext
raco
rpus
cula
r
Hereditary
Acquired
A Simple Classification of Hemolytic Anemias
Clinical Manifestations in Summary• Onset may be acute or
insidious
• Symptoms and signs of anemia
• Jaundice
– Acholuric
– Without pruritus
• Symptoms and signs spesific to the type of hemolytic anemia
• Symptoms related to the underlying disease
• Splenomegaly– Most congenital hem. anemias except
sickle cell– Some of the acquired hem. anemias
• Cholelithiasis (gall stones) symptoms• Leg ulcers (sickle cell, spherocytosis)
• Skeletal abnormalities (thalassemia)
• Crises (chronic hemolytic disease)
– Aplastic crises (HPV-B19)
– Hemolytic
– Megaloblastic
• Changes in urine color
Laboratory findings
I- Increased RBC destruction• Decreased RBC life span• Increased haem(heme)
catabolism– Increased serum
unconjugated bilirubin*– Increased endogenous CO
production– Increased urobilinogen excretion
• Increased serum LDH* • Absence or decrease of serum
haptoglobin*
• > 1 g /dl /week fall in blood Hb level*
• Reduced glycosylated Hb• Signs of intravascular
hemolysis– Hemoglobinemia*– Hemoglobinuria*– Hemosiderinuria*– Methemalbuminemia– Reduced serum
hemopexin level
*common practice
Laboratory findingsII-Increased bone marrow activity and RBC production
• Blood– Reticulocytosis
– Macrocytosis
– Polychromatophilia
– Erythroblastosis
– Leukocytosis and thrombocytosis
• Bone marrow– Erythroid hyperplasia
• Ferrokinetic– Increased plasma iron
turnover
– Increased RBC iron turnover
• Biochemical– Increased RBC creatine
– Increased activity of RBC enzymes eg: hexokinase, etc
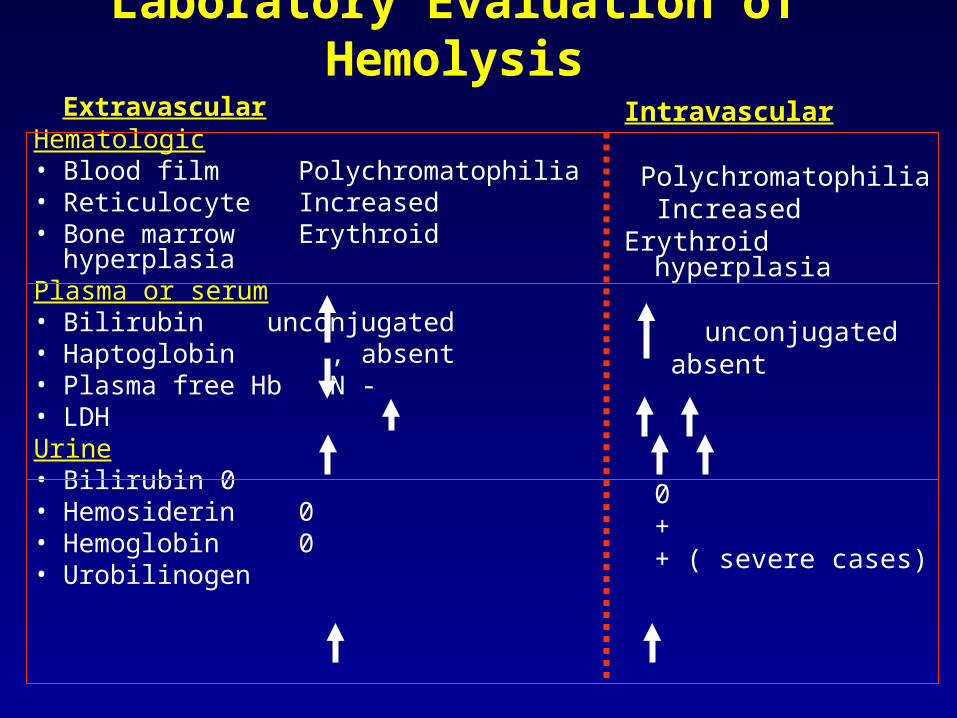
Laboratory Evaluation of Hemolysis
ExtravascularHematologic• Blood film Polychromatophilia• Reticulocyte Increased• Bone marrow Erythroid hyperplasiaPlasma or serum• Bilirubin unconjugated• Haptoglobin , absent• Plasma free Hb N - • LDHUrine• Bilirubin 0• Hemosiderin 0• Hemoglobin 0• Urobilinogen
Intravascular
Polychromatophilia IncreasedErythroid hyperplasia
unconjugated absent
0++ ( severe cases)
Laboratory tests useful in differential diagnosis
• Examination of peripheral blood
• Special Lab. examinations
Morphologic abnormalities in hemolytic anemias
• Polychromasia
• Spherocyte :
• Elliptocytes:
• Stomatocytes:
• Acanthocytes:
• Echinocytes:
: Reticulocytes
Her. Spherocytosis, immune hem. anemia,
burns, chemical injury to RBC
Hereditary ovalocytosis,
Hereditary stomatocytosis, alcoholism
Spur cell anemia with liver disease,
abetalipoproteinemia
Pyruvate kinase deficiency, uremia
Morphologic abnormalities in hemolytic anemias
• Sickle cell:
• Target cels:
• Schistocytes:
• Agglutination:
• Heinz bodies:
Sickle cell anemia
Thalassemia, HbC disease, liver disease,
splenectomy
Microangiopathic hem anemia, uremia, DIC,
malignant hypertesion, eclampsia,
disseminated vasculitis or malignancy,
Cold agglutinin disease
Unstable Hb, G6PD deficiency and oxidant
stress
• Bite cells -Blister cells
– G6PD deficiency
– Unstable Hemoglobin
• RBC fragmentation– Helmet Cell, schistocytes
• Thrombotic Thrombocytopenic Purpura (TTP),
• Hemolytic uremic syndrome (HUS)
• Disseminated Intravascular Coagulation
• Vaskulitis
• Renal graft rejection
• Malignant hypertention
• Burns
• Artificial cardiac valves
• March hemoglobinuria
• Target cells– Liver disease
– Thalassemia
– Hb C
– Splenectomy
– Sickle cell anemia
– Iron deficiency
• Howell-Jolly bodies
– Splenectomy
– Hyposplenism
– Megaloblastic anemia
– Hemolytic anemia
(Nuclear remnants)
• Basophylic stippling
– Lead poisoning– Thalassemia, – Unstable hemoglobines– MDS– Megaloblastic anemia– Other hemolytic anemia
• Eg. 5-Nucleotidase deficiency
Ribosomes/RNA/mitochondrial bodies
• Heinz Bodies
– RBC Enzyme defects– Unstable hemoglobin– Thalassemia– Sickle cell anemia
(Denaturated Hemoglobin)
Special Lab. Examinations• Coombs antiglobulin test - immune hemolysis• Osmotic fragility test - spherocytosis• Autohemolysis- G6PD,PK, spherocytosis• Membrane protein analysis- membrane defects• Red cell sickling- sickle cell anemia • Hemoglobin electrophoresis and HbA2, Hb F , HHb,etc -
Hemoglobinopathies and thalassemias• Red cell enzyme assays- RBC enzyme defects• HAM and sucrose lysis tests and GPI-linked protein analysis by
flow cytometry- PNH• Oxygen dissociation curve- High oxygen affinity Hb
Diagnostic approach
• Is there anemia?
• Detailed history including disease related symptoms, bleeding, drugs,ethnics, occupation , toxic exposure etc. family history
• Physical exam.: Signs of hemolytic anemia (common and specific ) in addition to anemia and any signs of underlying disease
Diagnostic approach• What are the changes in red cell morphology?
– Smear examination– Red cell indexes
• Are there any changes in other cell lines ?
• Is there evidence of increased red cell production? Reticulocytes
• Is there evidence of hemolysis?
• What is the type/diagn. of hemolysis?– Special tests
• Is there evidence of intravascular hemolysis?

















