Page 1
Introduction to
Neuro Rehab Modalities
Paul Chuwn Lim, M.D.Medical Director of Swedish Rehabilitation Services
Swedish Health Services
Swedish Physical Medicine & Rehabilitation
Medical Director of Swedish Neurological Rehabilitation Medicine
Swedish Medical Group
May 14th, 2021
14th Annual Cerebrovascular Symposium
Page 2
Outline
• Understand the evolution of rehab modalities & devices
• Cursory description of devices (low → high tech)
• Compare conventional rehab to newer strategies
• Barriers to wide-spread use of newer modalities
• No Disclosures
2
Page 4
Traditional Devices
Walkers
Crutches
Canes
Splints
Page 5
Widely Available Devices
Body Weight Wheelchairs
Supported Treadmill
Orthotics
FES
Page 6
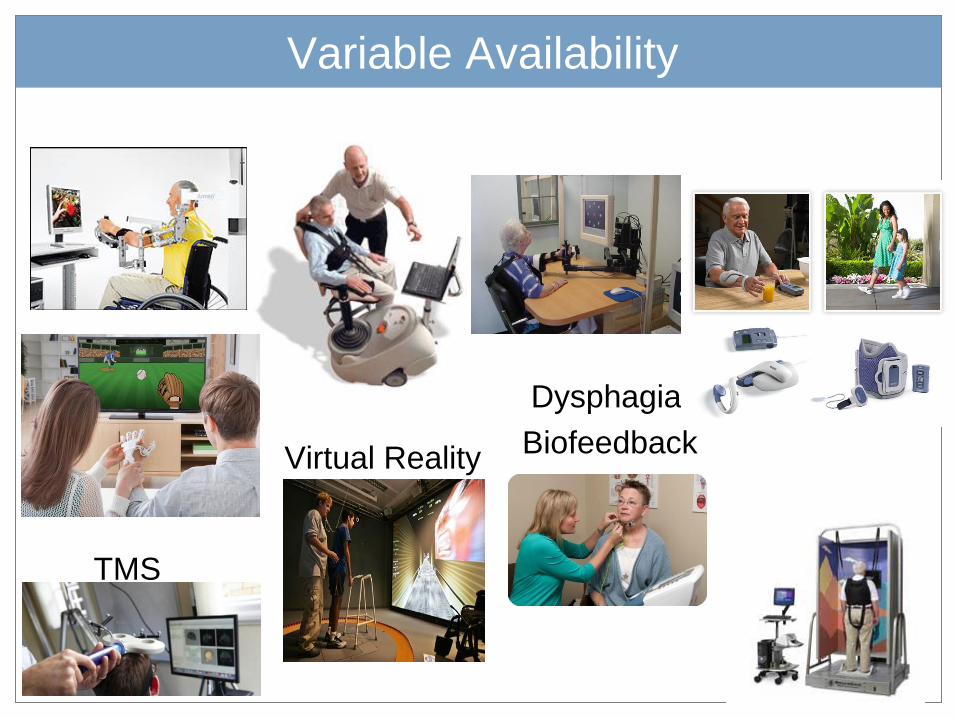
Variable Availability
Virtual Reality
TMS
Dysphagia
Biofeedback
Page 7
Many, Many More Devices
Page 8
Limits of Conventional Therapies
• Requires hours of therapy time
– Increasing therapy labor costs
• UK: ~10% of national stroke budget
• Aging population (ex: Japan) relative to trained therapists
– Rural access to specialists
• Frequent safety risks for patients & therapists
• Lacks repetition found to optimize neuroplasticity
– Body Weight Supported training vs conventional over-ground
– Up to 1000 gait cycles in 30 min vs <50 cycles
• Low Compliance: home > hospital
– Less engaging/entertaining, 1:1 hands-on supervision
8
Page 9
Benefits of Conventional Therapies
• Teaches compensatory strategies
– Hemi technique for walking, dressing, eating, and other ADLs
• Easily adaptable and personalized
• Whole body > segmental approach
• Compensate for abnormal movement patterns
• Accounts for emotional & clinical status quickly
• Accounts for cognitive and sensory deficits
– Complex tasks such as stairs, toileting, gait on uneven terrain, etc.
– Performance of actual tasks instead of simulated tasks
• Use of cheaper and more available assistive devices
9
Page 10
Rehabilitation Methods
• Muscle Re-education Approach (1920s)
• Neurodevelopmental Approach (1940-70s)
– Sensorimotor Approach (Rood, 1940s)
– Movement Therapy Approach (Brunnstrom, 1950s)
– NeuroDevelopmental Technique (Bobath, 1960-70s)
– Proprioceptive Neuromuscular Facilitation (Knott/Voss, 1960-70s)
• Motor Relearning Program for Stroke (Carr/Shephard, 1980s)
• Constrained Induced Movement Therapy (Taub, 1980s)
• Contemporary Task-Oriented Approach (Shumway-
Cook/Woolacott, 1990s)
• High-Intensity Gait Training 2010s-present
Page 11
High-Intensity Gait Training
• Conventional inpatient PT works on progressive function
– Static/dynamic sitting and standing balance, transfers, pre-gait
– If sufficiently improved enough, then will start gait activities
– Gait activities also slowly advanced progressively
• Emphasis shifting towards earlier and higher intensity gait
training – paradigm shift for older inpatient PTs
– Much more therapy minutes dedicated for gait >> pre-gait activities
• Practice, practice, practice – intensity makes perfect
• Aim to correct biomechanical and kinematic errors earlier
• Emphasis on repetition, gait efficiency, overall function
• Recommended by the Academy of Neurologic Physical
Therapy with a Clinical Practice Guideline in Jan 2020
11
Page 12
Paradigm Shift
• Conventional therapy shifting
towards earlier gait and
technology assisted rehab
• Move away from hospital care to
home/clinic based care
• Technological advances– Smaller processors, more complex software
– Light weight/stronger materials, better batteries
– Telemedicine: distant supervision, multiple pts
– Innovative human-machine interfaces
– Accurate physiological sensors and actuators
• Haptics, gyroscopes, EMG, FES, electrocortical
12
Page 13
Cutting Edge Technology
Exoskeleton Devices
Robotic Gait
Prosthetics
Brain Computer Interfaces
EEG Intracortical
EMG/FES NASA
+/- mirrors
Page 14
Paradigm Shift
• Economic and marketing forces
– Marketing advantage for rehab facilities (East/Midwest > West)
– Widespread use leads to cheaper gaming devices
– Commercialization of devices
– Patients and families drawn to new technology
– ? ultimate rationale: escalating labor costs
• Debate on its inevitability
• Benefits of robotics
• Simulated tasks when actual tasks are dangerous
• More entertaining therapy (increase compliance)
• Increased repetition to promote neuroplasticity
• Replace missing or damaged body parts
• Psychological benefits
14
Page 15
Barriers to Wide Spread Use
• Expensive devices generally not covered by insurance
– No compelling evidence of its superiority
• Primarily viewed as an adjunct to conventional therapy
– Era of healthcare cost containment
– Primarily at large rehab centers (east > mid-west > west)
• Generally from research or rehab facility marketing funds
• No additional therapy billing charges
• Marketing advantage primarily in competitive rehab environments
– Limited ability for out-of-pocket purchase by vast majority of pts
15