68
HealthVisions Delmarva improved health, healthcare quality and experience, lower healthcare costs and improved provider experience

HealthVisionsDelmarva
improved health, healthcare quality and experience, lower healthcare costs and improved provider experience

Barbara J. Connors, DO, MPH, CMS Chief Medical Officer Region 3Dr. Connors has served as Chief Medical Officer at The Centers for Medicare & Medicaid Services Region III, for tenyears. During her tenure, she also served as the Acting Associate Regional Administrator for the Division of Survey andCertification in CMS Northeast Consortium Regions I, II and III.As the Chief Medical Officer, she is responsible for ensuring the provider community is cognizant of CMS health carequality improvement initiatives, reporting requirements, and the provisions in the ACA that impact the providercommunity. Dr. Connors interests are in population health and quality reporting.Dr. Connors graduated from the New York College of Osteopathic Medicine and received her Masters of Public Healthfrom the Medical College of Wisconsin. She trained in internal medicine at Monmouth Medical Center in New Jersey.As a Public Health Service scholarship recipient, she practiced Internal Medicine in a physician shortage area in NYCfor several years. She also held the position of Medical Director for Occupational Medicine, at the West Jersey HealthSystem. Prior to joining CMS, Dr. Connors was a consultant with Federal Occupational Health where she served as theReviewing Medical Officer for several federal agencies including the Mine Safety Health Administration, CustomsBorder Protection, and the IRS.Dr. Connors is Board Certified by the American Board of Internal Medicine and the American Board of PreventiveMedicine.
Dr. Barbara Connors has indicated that she has no financial conflicts of interest relevant to this presentation.

Identify the components of the Quality Payment Program Final Rule Describe how to successfully participate in MIPS Define what is considered an Advanced Alternative Payment Model under the Final
Rule
Quality Payment Program
Barbara Connors, D.O., M.P.H.
November 15, 2016
The Quality Payment Program and Health Care Payment Reform

Quality Payment Program
The Quality Payment Program
• The Quality Payment Program policy will reform Medicare Part B payments for more than 600,000 clinicians across the country, and is a major step in improving care across the entire health care delivery system.
• Clinicians can choose how they want to participate in the Quality Payment Program based on their practice size, specialty, location, or patient population.
Two tracks to choose from:

Quality Payment Program
What Is the Quality Payment Program Timeline?
• First Payment Year – 2019
– Based on first performance period of 2017
• 2017 Pick Your Pace Options
– Four options to help clinicians avoid negative payment adjustments:
1. Test Pace
2. Partial Year
3. Full Year
4. Participate in an Advanced APM
Quality Payment Program
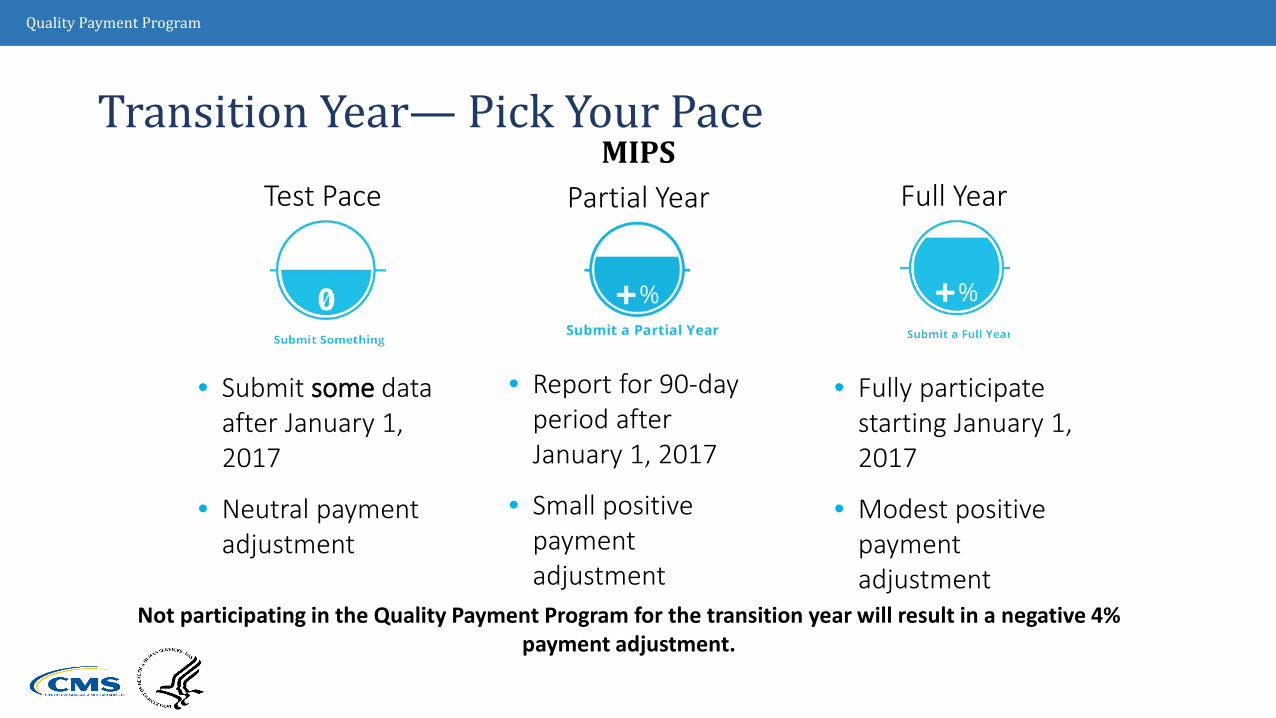
Transition Year— Pick Your Pace
• Report for 90-day period after January 1, 2017
• Small positive payment adjustment
• Fully participate starting January 1, 2017
• Modest positive payment adjustment
• Submit some data after January 1, 2017
• Neutral payment adjustment
Test Pace Partial Year Full YearMIPS
Not participating in the Quality Payment Program for the transition year will result in a negative 4% payment adjustment.
Quality Payment Program
Choosing to Test for 2017
• If you submit a minimum amount of 2017 data to Medicare (for example, one quality measure or one improvement activity), you can avoid a downward adjustment
– Clinicians must submit some data after January 1, 2017
Submit 1 quality measure or 1 Improvement activity or 5 advancing care information measures
For both MIPS and Advanced APMs:1. No penalties for clinicians who participate in any one of the options
• Only clinicians who do not submit any data receive negative payment adjustment
Quality Payment Program
Partial Participation for 2017
• If you submit 90 days of 2017 data to Medicare, you may earn a neutral or small positive payment adjustment.
• That means if you’re not ready on January 1, you can choose to start anytime between January 1 and October 2, 2017. Whenever you choose to start, you'll need to send in performance data by March 31, 2018.
• They must report more than one quality measure, more than one improvement activity, or more than the 5 required measures in the advancing care information performance category in order to avoid a negative MIPS payment adjustment and to possibly receive a positive MIPS payment adjustment.

Quality Payment Program
Full Participation for 2017
• If you submit a full year of 2017 data to Medicare, you may earn a moderate positive payment adjustment. The best way to earn the largest positive adjustment is to participate fully in the program by submitting information in all the MIPS performance categories.
Key Takeaway:
• Positive adjustments are based on the performance data on the performance information submitted, not the amount of information or length of time submitted.

Quality Payment Program
Full Year Participation
• Full participation in the MIPS would mean that clinicians should, at least,meet the following criteria:
1. Report 6 Quality Measures
2. Report 4 medium weighted or 2 high-weighted improvement activities
3. Report 5 advancing care information measures
• MIPS eligible clinicians who are exceptional performers in MIPS, as shown by the practice information that they submit, are eligible for an additional positive adjustment for each year of the first 6 years of the program.
Quality Payment Program
Who Is Eligible for MIPS?
• Medicare Part B clinicians billing more $30,000 and providing care to more than 100 Medicare patients per year.
• Known as “eligible clinicians”
• Voluntary option for all other clinicians not included in transition year
Physicians Physician Assistants
Nurse Practitioners
Clinical Nurse Specialists
Certified Registered Nurse
Anesthetists

Quality Payment Program
Who Is Exempt from MIPS?• Clinicians who:
•Are newly enrolled in Medicare•Do not meet thresholds:
– < $30,000 in Medicare charges OR
– < 100 Medicare patients•Are significantly participating in an Advanced APM
• MIPS doesn’t apply to hospital-based or facility-based payment programs
This means that clinicians with >$30,000 AND >100 Medicare patients would be included unless they met other exclusions.The threshold is measured at the group level for group reporting and individual level for individual reporting.

Quality Payment Program
Non-Patient Facing Clinicians
• Non-patient facing clinicians are eligible to participate in MIPS as long as they exceed the low-volume threshold, are not newly enrolled, and are not a qualifying APM participant (QP) or partial QP that elects not to report data to MIPS
• The non-patient facing MIPS-eligible clinician threshold for individual MIPS-eligible clinicians is < 100 patient facing encounters in a designated period
• A group is non-patient facing if > 75% of NPIs billing under the group’s TIN during a performance period are labeled as non-patient facing
• There are special reporting requirements for non-patient facing clinicians

Quality Payment Program
OPTIONS
Individual Group
How Do Clinicians Participate in MIPS?
1. Individual – under an NPI number and TIN where they reassign benefits
2. As a Group –a) 2 or more clinicians (NPIs) who have reassigned their billing rights
to a single TIN*b) As a MIPS APM entity
* If clinicians participate as a group, they are assessed as group across all 4 MIPS performance categories
Quality Payment Program
When Does MIPS Officially Begin?
First Performance Period
January 1, 2017 through
December 31, 2017
First Payment Year
2019
Based on 2017 performance

Quality Payment Program
How Are MIPS Performance Categories Weighted?Weights assigned to each category based on a 1 to 100 point scale
Transition Year Weights%
Quality
60%
Improvement Activities
15%
Advancing Care Information
25%
Cost
0%
NOTE: These are defaults weights; the weights can adjust in certain circumstances

Quality Payment Program
MIPS Performance Category: Quality
Category Requirements• Replaces PQRS and Quality Portion of the Value Modifier• 60% of final score• Select 6 of about 300 quality measures (minimum of 90 days); 1 must be:
– Outcome measure OR– High-priority measure – defined as outcome measure, appropriate use measure,
patient experience, patient safety, efficiency measures, or care coordination • May also select specialty-specific set of measures• Readmission measure for group submissions that have > 15 clinicians and a sufficient
number of cases (no requirement to submit)• Different requirements for groups reporting CMS Web Interface or those in MIPS-APMs

Quality Payment Program
MIPS Performance Category: Quality –Reporting
Individual clinicians may report through:• Qualified Registry• Electronic Health Record (EHR)• Qualified Clinical Data Registry (QCDR)• Claims
Groups may report measures through:• Qualified Registry • EHR• QCDR• CMS Web Interface (groups of 25 or
more)• CAHPS for MIPS Survey
– Counts as 1patient experience measure
– Must submit 5 other measures through a different mechanism above

Quality Payment Program
MIPS Performance Category: Cost
• No reporting requirement; 0% of final score in 2017
• Clinicians assessed on Medicare claims data
• Uses measures previously used in the Physician Value-Based Modifier program or reported in the Quality and Resource Use Report (QRUR), but scoring is different

Quality Payment Program
MIPS Performance Category: Cost – Reporting
Cost Measures from VM• Medicare Spending Per Beneficiary (MSPB)
• Evaluates the costs of care related to inpatient hospital visits • Total Per-Capita Cost for All Attributed Beneficiaries
• Evaluates the annual overall patient costs
For a measure to be applied, a clinician must either:• Bill for certain attributable services (Episode Group) Example: Aortic valve replacement• Provide services a minimum number of times
• > 35 times for MSPB• > 20 times for all other measures
Quality Payment Program
MIPS Performance Category: Improvement Activities • Assesses participation in activities that improve clinical practice
• Examples: Shared decision making, patient safety, coordinating care, increasing access
• Clinicians choose from about 90+ activities under 9 subcategories:
1. Expanded Practice Access
2. Population Management
3. Care Coordination
4. Beneficiary Engagement
5. Patient Safety and Practice Assessment
6. Participation in an APM
7. Achieving Health Equity
8. Integrating Behavioral and Mental Health
9. Emergency Preparedness and Response
Quality Payment Program
• Most participants: Attest that you completed up to 4 improvement activities for a minimum of 90 days.
• Groups with 15 or fewer participants or if you are in a rural or health professional shortage area: Attest that you completed up to 2 activities for a minimum of 90 days.
MIPS Performance Category: Improvement Activities

Quality Payment Program
General Rule (no special considerations)• Choose 1 of the following combinations:
– 2 high-weighted activities
– 1 high-weighted activity and 2 medium-weighted activities
– At least 4 medium-weighted activities • A sample combination could include:
– 1 medium-weighted activity from Beneficiary Engagement
– 1 medium-weighted activity from Patient Safety and Practice Assessment
– 1 high-weighted activity from Integrated Behavioral Health
MIPS Performance Category: Improvement Activities

Quality Payment Program
Practices with 15 or Fewer Clinicians, Rural or Geographic HPSA, and Non-patient FacingChoose 1 of the following combinations:
• 1 high-weighted activity OR
• 2 medium-weighted activities
MIPS Performance Category: Improvement Activities

Quality Payment Program
• APM designated as a Medical Home Model: You will automatically earn full credit.
• Participants in certain APMs under the APM scoring standard, such as Shared Savings Program Track 1 or the Oncology Care Model: You will automatically receive points based on the requirements of participating in the APM. For all current APMs under the APM scoring standard, this assigned score will be full credit. For all future APMs under the APM scoring standard, the assigned score will be at least half credit.
MIPS Performance Category: Improvement Activities

Quality Payment Program
• Must perform selected activities for 90 consecutive days
• Must attest each activity performed for 90-day period by selecting “Yes” during reporting
• May report activities through:
• Qualified Registry
• Electronic Health Record (EHR)
• Qualified Clinical Data Registry (QCDR)
• CMS Web Interface (for groups of 25 clinicians or more)
• Attestation data submission methods
MIPS Performance Category: Improvement Activities – Reporting

Quality Payment Program
MIPS Performance Category: Advancing Care Information
• Promotes patient engagement and interoperability using certified EHR technology
• Replaces the Medicare EHR Incentive Program
• Greater flexibility in choosing measures
• In 2017, there are 2 measure sets for reporting based on EHR edition:
1. Advancing Care Information Objectives and Measures
2. 2017 Advancing Care Information Transition Objectives and Measures

Quality Payment Program
MIPS Performance Category: Advancing Care Information — Reporting
For those using EHR Certified to the 2015 Edition:
Option 1: Advancing Care Information Objectives and Measures
Option 2: Combination of the two measure sets
For those using 2014 Certified EHR Technology:
Option 1: 2017 Advancing Care Information Transition Objectives and
Measures
Option 2: Combination of the two measure sets
Clinicians must use certified EHR technology to report
Quality Payment Program
2017 Advancing Care Information Transition Objectives and Measures:
Base Score Required Measures
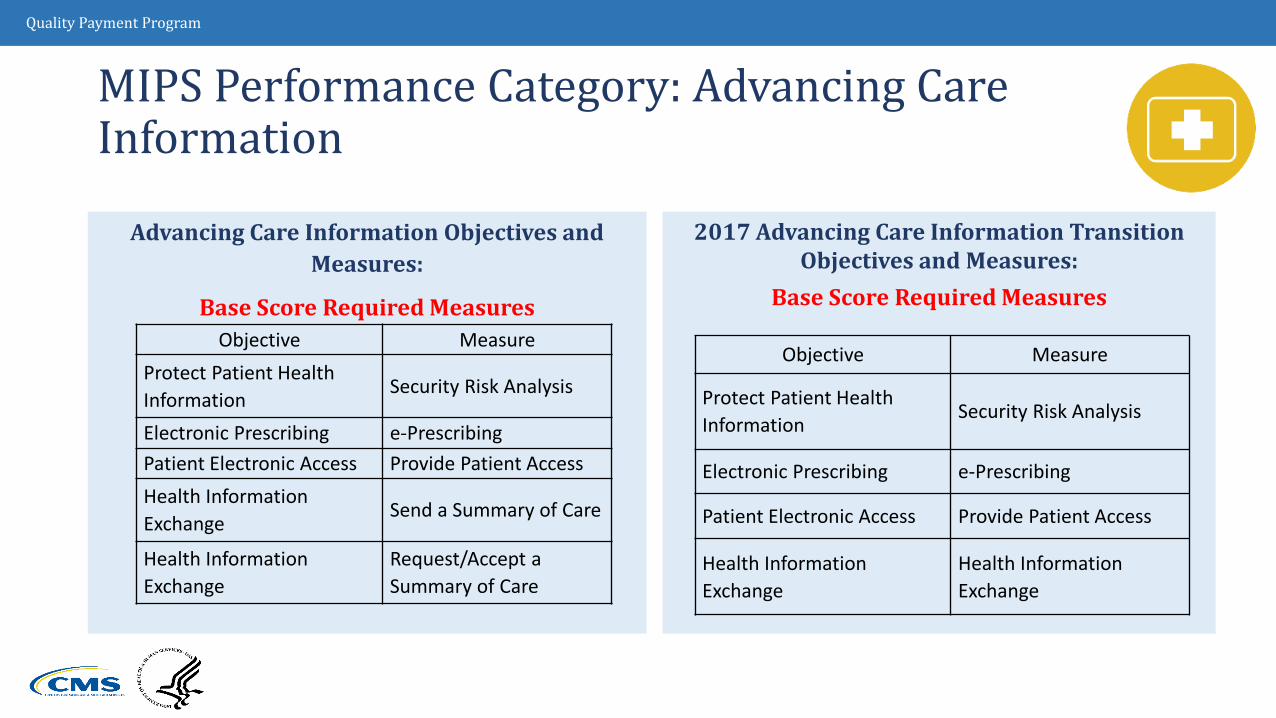
MIPS Performance Category: Advancing Care Information
Advancing Care Information Objectives and Measures:
Base Score Required MeasuresObjective Measure
Protect Patient Health Information
Security Risk Analysis
Electronic Prescribing e-PrescribingPatient Electronic Access Provide Patient AccessHealth Information Exchange
Send a Summary of Care
Health Information Exchange
Request/Accept a Summary of Care
Objective Measure
Protect Patient Health Information
Security Risk Analysis
Electronic Prescribing e-Prescribing
Patient Electronic Access Provide Patient Access
Health Information Exchange
Health Information Exchange

Quality Payment Program
MIPS Performance Category: Advancing Care Information
Advancing Care Information Objectives andMeasures
Objective Measure
Patient Electronic Access Provide Patient Access*
Patient Electronic Access Patient-Specific EducationCoordination of Care through Patient Engagement
View, Download and Transmit (VDT)
Coordination of Care through Patient Engagement
Secure Messaging
Coordination of Care through Patient Engagement
Patient-Generated Health Data
Health Information Exchange Send a Summary of Care*
Health Information ExchangeRequest/Accept a Summary of Care*
Health Information Exchange Clinical Information Reconciliation
Public Health and Clinical Data Registry Reporting
Immunization Registry Reporting
2017 Advancing Care Information Transition Objectives and Measures
Objective Measure
Patient Electronic Access Provide Patient Access*
Patient Electronic AccessView, Download and Transmit (VDT)
Patient-Specific Education Patient-Specific Education
Secure Messaging Secure Messaging
Health Information ExchangeHealth Information Exchange*
Medication Reconciliation Medication Reconciliation
Public Health ReportingImmunization Registry Reporting

Quality Payment Program
MIPS Performance Category: Advancing Care Information – Completion Alternatives• Clinicians have the opportunity to earn a bonus score 2 ways:
• Earn a 5% bonus for reporting to additional Public Health and Clinical Data Registry Reporting measures (aside from the Immunization Registry Reporting measure)
• Earn a 10% bonus for using CEHRT to complete certain activities within the Improvement Activities performance category

Quality Payment Program
MIPS Performance Category: Advancing Care Information 1.Clinicians recognized as participating in a MIPS-APM entity will automatically
receive a 50% score in the category • Clinicians need to earn the remaining 50% to receive full credit in the category
2.If objectives and measures are not applicable to a clinician, CMS will reweight the category to zero and assign the 25% to the other performance categories to offset difference in the MIPS final score
3.If clinicians face a significant hardship and are unable to report advancing care information measures, they can apply to have their performance category score weighted to zero
4.Hospital-based MIPS eligible clinicians may choose to report under the Advancing Care Information Performance Category
Quality Payment Program
MIPS Vendor Reporting
• Health information technology (HIT) vendors submit data on behalf of clinicians for:
Quality
Improvement Activities
Advancing Care Information
• If data for activities is derived from CEHRT, vendors must indicate data source and transmit data in a CMS-specified form and manner
Quality Improvement Activities
Advancing Care

Quality Payment Program
MIPS Scoring for Quality (60% of Final Score)
Select 6 of the approximately 300 available quality measures (minimum of 90 days)
• Or a specialty set
• Or CMS Web Interface measures
• Readmission measure is included for group reporting with groups with at least 16 clinicians and sufficient cases

Quality Payment Program
MIPS Scoring for Quality (60% of Final Score)
• Clinicians receive 3 to 10 points on each quality measure based on performance against benchmarks
– Benchmarks based on historical data (if available); or performance period if historical benchmark is not available
– Failure to submit performance data for a measure = 0 points
Transition year participants automatically receive 3 points for completing and submitting a measure

Quality Payment Program
MIPS Scoring for Quality (60% of Final Score)
Bonus Points
Clinicians receive bonus points for either of the following:
1. Submitting an additional high-priority measure
2 bonus point for each additional outcome and patient experience measure
1 bonus point for each additional high-priority measure
2. Using CEHRT to submit measures to registries or CMS
1 bonus point for submitting end-to-end
Quality Payment Program
MIPS Scoring for Quality (60% of Final Score)
– Maximum Number of Points
CMS Web Interface Reporter total score
– 120 points for groups with complete reporting and the readmission measure
– 110 points for groups with complete reporting and no readmission measure
Other submission mechanisms total score
– 70 points for 6 measures + 1 readmission measure
– 60 points if readmission measure does not apply

Quality Payment Program
MIPS Scoring for Cost (0% of Final Score in Transition Year)• Clinicians can earn maximum 10 points per episode Cost measure
based on performance compared to benchmark within performance period
• No submission requirements
• Clinicians assessed through claims data

Quality Payment Program
MIPS Scoring for Advancing Care Information(25% of Final Score) • Base score
• Clinicians must submit a numerator/denominator OR Yes/No combination for each of the following measures:
• Protect Patient Health Information
• Electronic Prescribing
• Patient Electronic Access
• Health Information Exchange: Send Summary of Care
• Health Information Exchange: Request/Accept Summary of Care
Failure to meet reporting requirements will result in base score of 0
Quality Payment Program
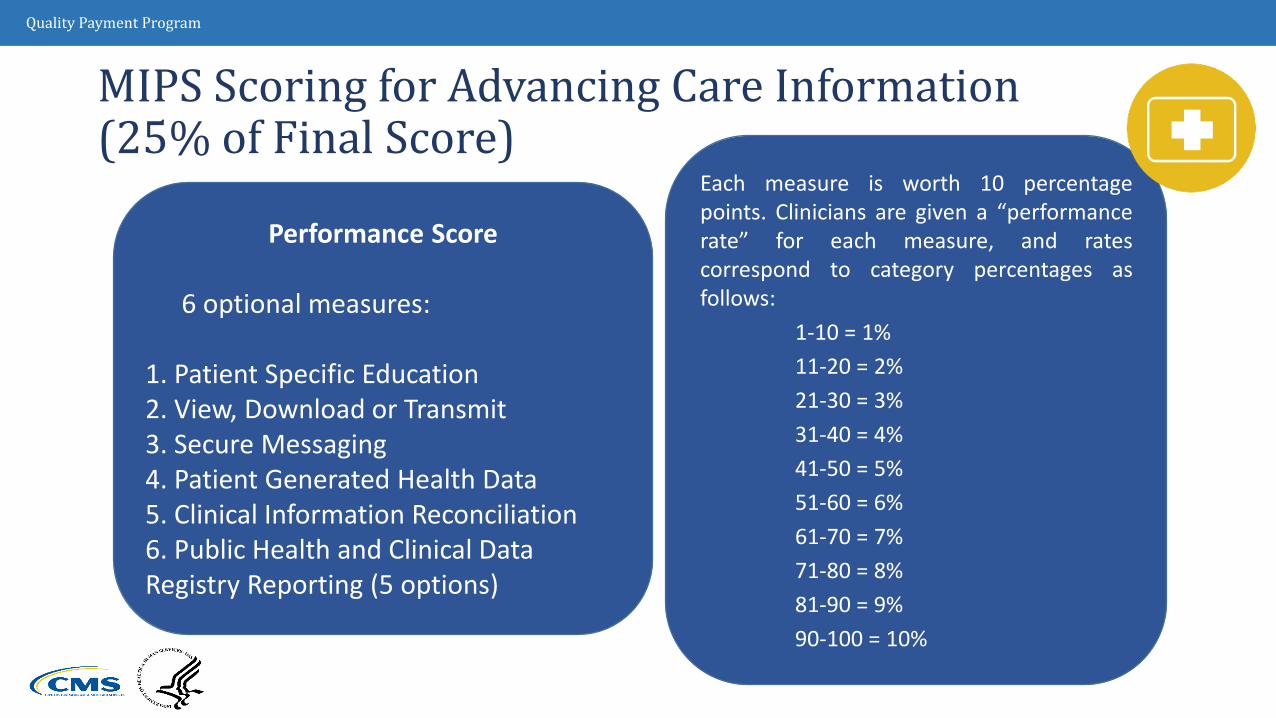
MIPS Scoring for Advancing Care Information(25% of Final Score)
Each measure is worth 10 percentagepoints. Clinicians are given a “performancerate” for each measure, and ratescorrespond to category percentages asfollows:
1-10 = 1%11-20 = 2%21-30 = 3%31-40 = 4%41-50 = 5%51-60 = 6%61-70 = 7%71-80 = 8%81-90 = 9%90-100 = 10%
Performance Score
6 optional measures:
1. Patient Specific Education2. View, Download or Transmit3. Secure Messaging4. Patient Generated Health Data5. Clinical Information Reconciliation6. Public Health and Clinical Data Registry Reporting (5 options)

Quality Payment Program
MIPS Scoring for Advancing Care Information(25% of Final Score) Bonus Points
1. 5% bonus for reporting on any of these registry measures:
– Syndromic Surveillance Reporting
– Electronic Case Reporting
– Public Health Registry Reporting
– Clinical Data Registry Reporting2. 10% bonus for using CEHRT to report Improvement Activities
Advancing Care Information Performance Category Score =
Base score + Cumulative performance score + Bonus points

Quality Payment Program
Calculating the Final Score Under MIPS[(clinician Quality performance category score x actual Quality performance category
weight) +
(clinician Cost performance category score x actual Cost performance category weight) +
(clinician Improvement Activities performance category score x actual Improvement Activities performance category weight)
+(clinician Advancing Care Information performance category score x actual Advancing Care
Information performance category weight)] x
100

Quality Payment Program
Calculating the Final Score Under MIPS
Reweighting Option • For clinicians that cannot be scored within a MIPS performance
category
– Reduces the reporting burden on clinicians
– Gives clinicians flexibility to focus on categories specific to their practice

Quality Payment Program
Additional Adjustment Factors for MIPS
• Scaling factor to be applied to positive adjustments only
• “Exceptional Performer” category
• Incentive funding of $500,000,000 annually
• Clinicians who meet or exceed the threshold may receive up to a 10% bonus adjustment
• Final scores of 70 or more qualify for additional payment
– Additional payments start at 0.5 percent and increase with the final score
Quality Payment Program
How Are Payment Adjustments Applied?
CMS:
• Applies payment adjustments to each combination of TIN and NPI a clinician uses to bill Medicare (each enrollment)
• Uses logic models for certain rare cases. For example:
1. If a clinician participates in an MIPS-APM entity…
Then the APM entity final score is used
2. If a clinician submits as a group and as an individual (but is not a MIPS-APM entity)…
Then highest final score for TIN/NPI combination is used

Quality Payment Program
When Are MIPS Payment Adjustments Announced?
Transition year payment adjustments:
• Announced December 1, 2018
• Applied to Medicare payments in 2019
Quality Payment Program
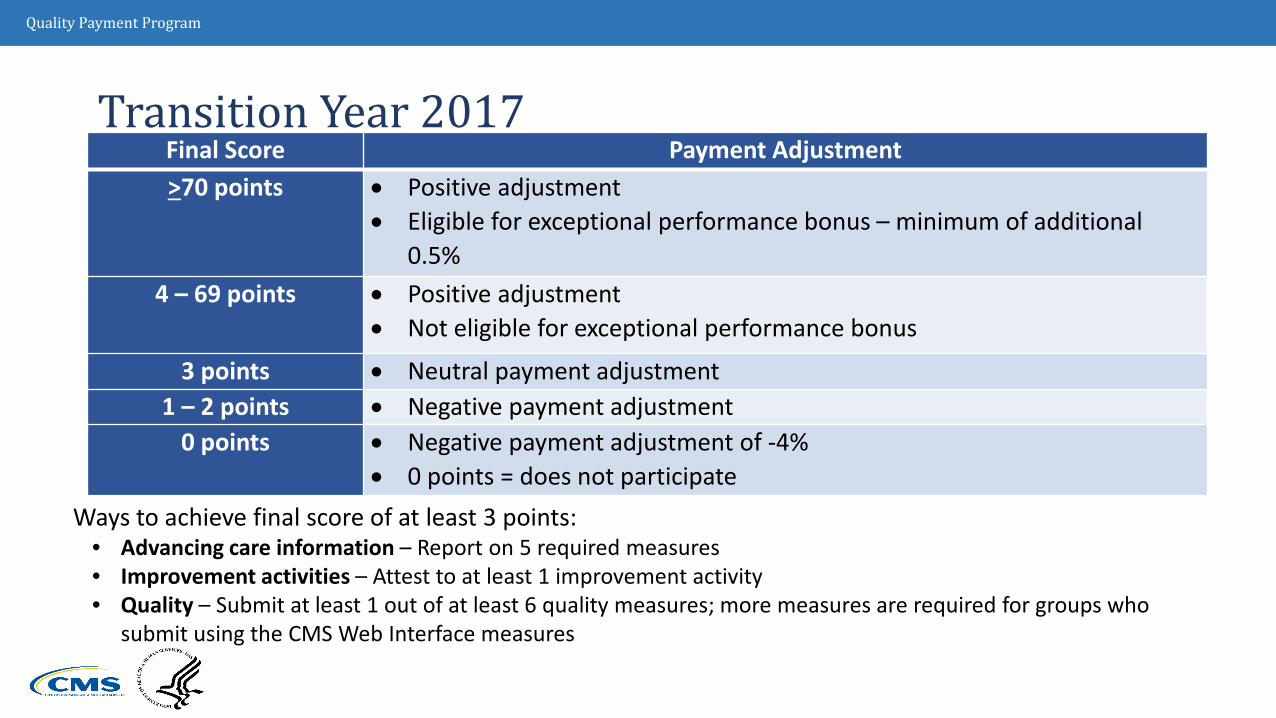
Transition Year 2017Final Score Payment Adjustment>70 points • Positive adjustment
• Eligible for exceptional performance bonus – minimum of additional 0.5%
4 – 69 points • Positive adjustment• Not eligible for exceptional performance bonus
3 points • Neutral payment adjustment1 – 2 points • Negative payment adjustment
0 points • Negative payment adjustment of -4%• 0 points = does not participate
Ways to achieve final score of at least 3 points:• Advancing care information – Report on 5 required measures• Improvement activities – Attest to at least 1 improvement activity• Quality – Submit at least 1 out of at least 6 quality measures; more measures are required for groups who
submit using the CMS Web Interface measures

Quality Payment Program
How Are Payments Adjusted Under MIPS?
• Positive, negative, neutral adjustments
Based on CMS-established threshold
‒ First year threshold = 3 out of 100 points
‒ Clinicians reporting some data will easily achieve this threshold
• Clinicians at or above the performance threshold will receive a neutral or positive adjustment factor based on a linear sliding scale

Quality Payment Program
Can a Clinician Dispute a Final Score or Payment Adjustment?
Mechanism: Targeted (Informal) Review
MIP-eligible clinicians may request a review of the calculation of the:
1. MIPS adjustment factor
2. Additional MIPS adjustment factor, as applicable

Quality Payment Program
Alternative Payment Models
• An Alternative Payment Model (APM) is a payment approach, developed in partnership with the clinician community, that provides added incentives to clinicians to provide high-quality and cost-efficient care. APMs can apply to a specific clinical condition, a care episode, or a population.
• APMs may offer significant opportunities to eligible clinicians who are not immediately able or prepared to take on the additional risk and requirements of Advanced APMs.
Advanced APMs are a Subset of APMs
APMs
AdvancedAPMs
Quality Payment Program
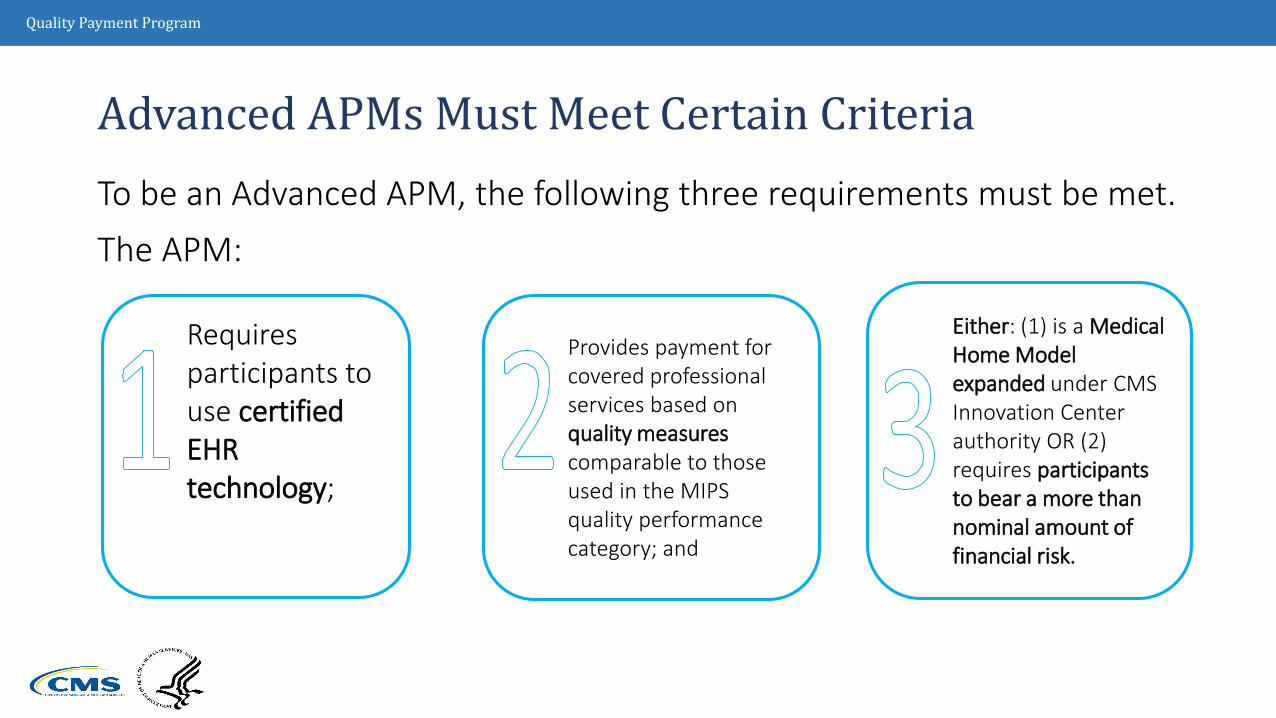
Advanced APMs Must Meet Certain CriteriaTo be an Advanced APM, the following three requirements must be met. The APM:
Either: (1) is a Medical Home Model expanded under CMS Innovation Center authority OR (2) requires participants to bear a more than nominal amount of financial risk.
Provides payment for covered professional services based on quality measures comparable to those used in the MIPS quality performance category; and
Requires participants to use certified EHR technology;
Quality Payment Program
What is a Qualifying APM Participant (QP)?
• Qualifying APM Participants (QPs) are clinicians who have a certain % of Part B payments for professional services or patients furnished Part B professional services through an Advanced APM Entity.
• Beginning in 2021, this threshold % may be reached through a combination of Medicare and other non-Medicare payer arrangements, such as private payers and Medicaid.

Quality Payment Program
Additional Opportunities for APM Participation in 2017 and 2018• On October 25, CMS announced new opportunities for clinicians to join
Advanced APMs in 2017 and 2018
• CMS expects to re-open applications for new practices and payers in the Comprehensive Primary Care Plus (CPC+) model and new participants in the Next Generation Accountable Care Organization (ACO) model for the 2018 performance year
• Innovation Center’s Oncology Care Model with two-sided risk will now be available in 2017, which qualifies as an Advanced APM in the 2017 performance year
• Originally was to be available for the 2018 performance year

Quality Payment Program
How do Eligible Clinicians become Qualifying APM Participants? – Step 1
Qualifying APM Participant determinations are made at the Advanced APM Entity level, with certain exceptions: individuals participating in multiple Advanced APM Entities, none of
which meet the QP threshold as a group, and eligible clinicians on an Affiliated Practitioner List when that list is
used for the QP determination because there are no eligible clinicians on a Participation List for the Advanced APM Entity. For example, gain sharers in the Comprehensive Care for Joint Replacement Model will be assessed individually.
Quality Payment Program
How do Eligible Clinicians become Qualifying APM Participants? – Step 2
Attributed (beneficiaries for whose cost and quality of care the APM Entity is responsible)
Attribution-eligible (all beneficiaries who could potentially be attributed)
These definitions are used for calculating
Threshold Scores under both methods.
CMS will calculate a percentage “Threshold Score” for each Advanced APM Entity using two methods (payment amount and patient count).
Methods are based on Medicare Part B professional services and beneficiaries attributed to Advanced APM
CMS will use the method that results in a more favorable QP determination for each Advanced APM Entity.

Quality Payment Program
How do Eligible Clinicians become Qualifying APM Participants? – Step 3
Requirements for Incentive Paymentsfor Significant Participation in Advanced APMs
(Clinicians must meet payment or patient requirements)Performance Year 2017 2018 2019 2020 2021 2022 and
laterPercentage of Payments through an Advanced APM Percentage of Patients through an Advanced APM
The Threshold Score for each method is compared to the corresponding QP threshold table and CMS takes the better result.

Quality Payment Program
Advanced APM
Advanced APM Entities
Eligible Clinicians
Threshold Scores above
the QP threshold = QP status
Threshold Scores below the QP
threshold = no QPs
All the eligible clinicians in the Advanced APM Entity become QPs for the payment year.
How do Eligible Clinicians become Qualifying APM Participants? – Step 4
Quality Payment Program
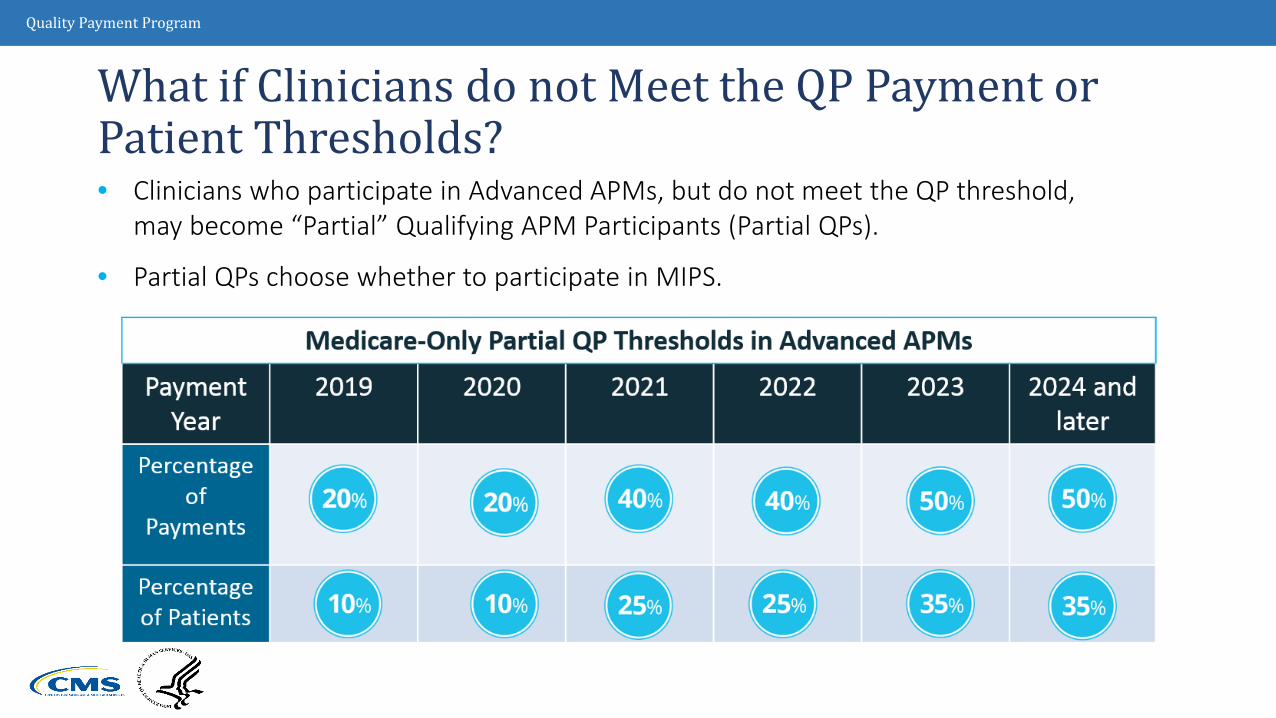
• Clinicians who participate in Advanced APMs, but do not meet the QP threshold, may become “Partial” Qualifying APM Participants (Partial QPs).
• Partial QPs choose whether to participate in MIPS.
What if Clinicians do not Meet the QP Payment or Patient Thresholds?
Quality Payment Program
Advanced APMs in 2017• For the 2017 performance year, the following models are Advanced APMs:
• The list of Advanced APMs is posted at QPP.CMS.GOV and will be updated with new announcements on an ad hoc basis.
Comprehensive End Stage Renal Disease Care Model
(Two-Sided Risk Arrangements)Comprehensive Primary Care Plus (CPC+)
Shared Savings Program Track 2 Shared Savings Program Track 3
Next Generation ACO Model Oncology Care Model(Two-Sided Risk Arrangement)

Quality Payment Program
Future Advanced APM Opportunities
• MACRA established the Physician-Focused Payment Model Technical Advisory Committee (PTAC) to review and assess Physician-Focused Payment Models based on proposals submitted by stakeholders to the committee.
• For the 2018 performance year, we anticipate that the following models will be Advanced APMs:
This list may change. Be sure clinicians review the final list that is scheduled to be published on or before January 1, 2018.
Advancing Care Coordination
through Episode Payment Models Track 1 (CEHRT)
New Voluntary Bundled
Payment ModelACO Track 1+
Comprehensive Care for Joint Replacement
Payment Model (CEHRT)
Quality Payment Program
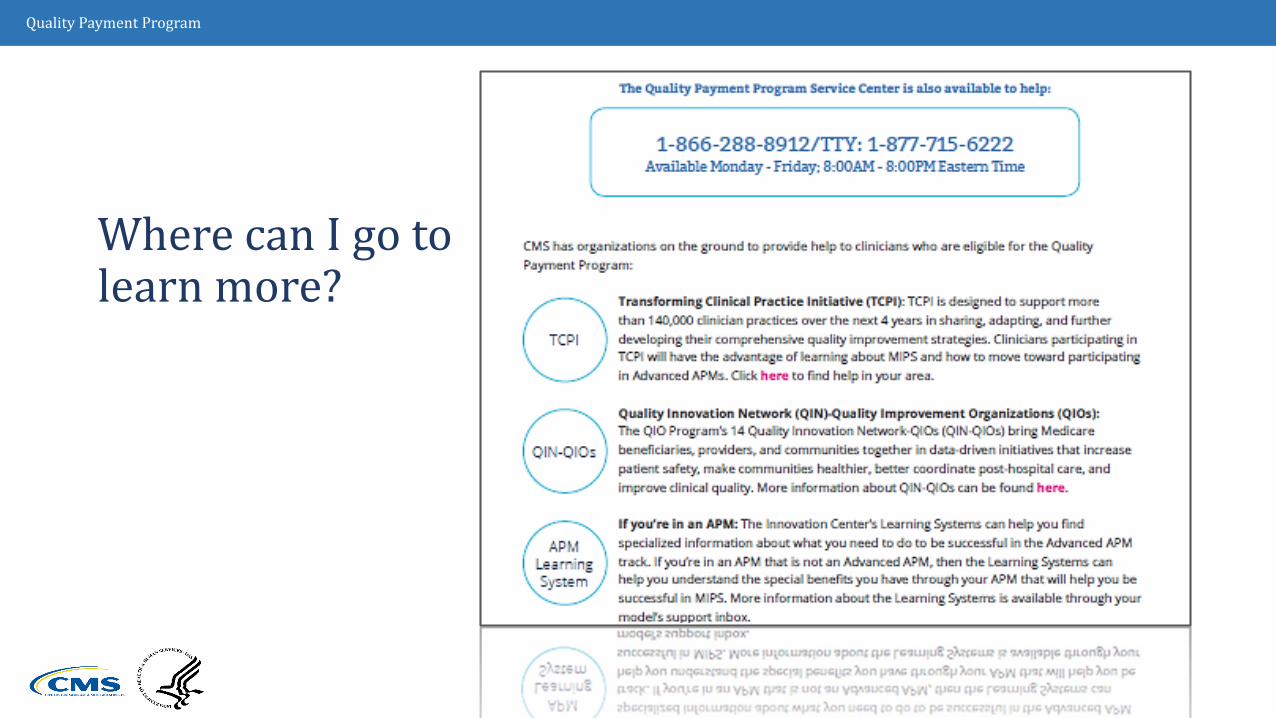
Where can I go to learn more?
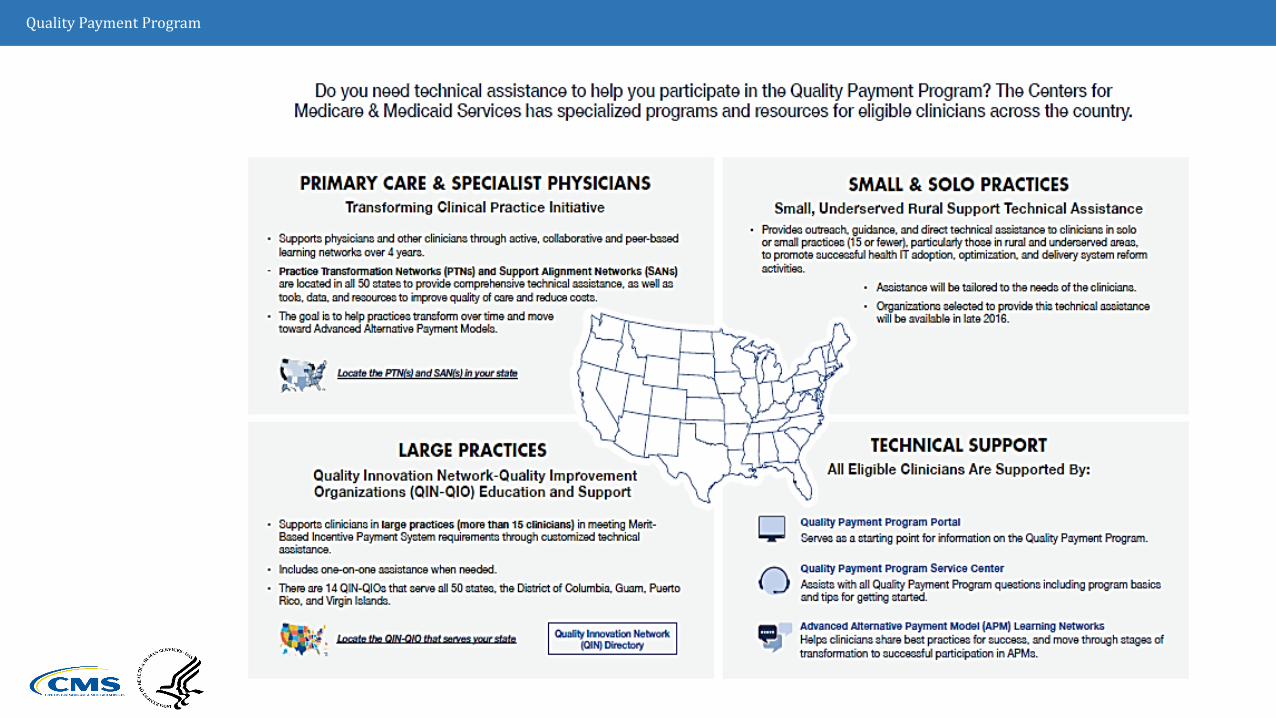
Quality Payment Program
Quality Payment Program
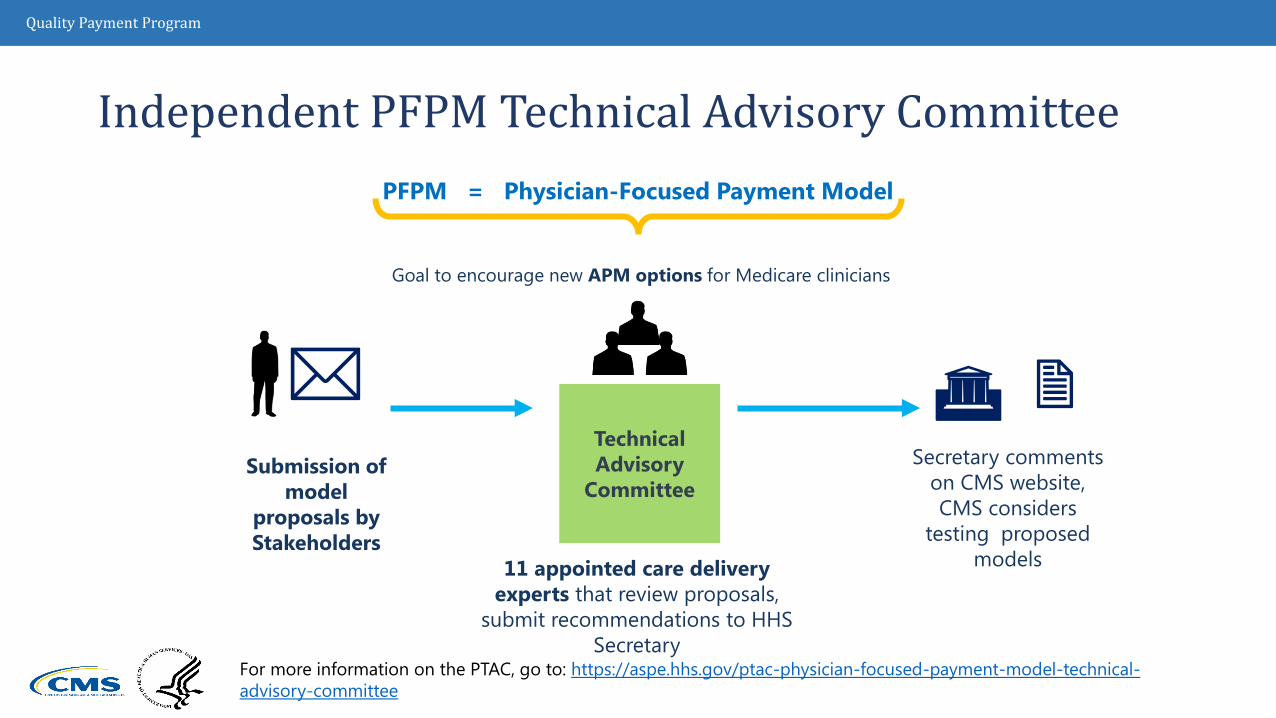
PFPM = Physician-Focused Payment Model
Goal to encourage new APM options for Medicare clinicians
Independent PFPM Technical Advisory Committee
Technical Advisory
CommitteeSubmission of
model proposals by Stakeholders
11 appointed care delivery experts that review proposals,
submit recommendations to HHS Secretary
Secretary comments on CMS website, CMS considers
testing proposed models
For more information on the PTAC, go to: https://aspe.hhs.gov/ptac-physician-focused-payment-model-technical-advisory-committee

Quality Payment Program
Health Care Payment Learning and Action Network Medicare alone cannot drive sustained progress towards alternative payment models (APM)
Success depends upon a critical mass of partners adopting new models
• http://innovation.cms.gov/initiatives/Health-Care-Payment-Learning-and-Action-Network/
The network purpose:
• Convene payers, purchasers, consumers, states and federal partners to establish a common pathway for success
• Identify areas of agreement around movement to APMs
• Collaborate to generate evidence, shared approaches, and remove barriers
• Develop common approaches to core issues such as beneficiary attribution
• Create implementation guides for payers and purchasers
Quality Payment Program
Contact InfoBarbara Connors, D.O., M.P.H.Chief Medical OfficerCMS Philadelphia Regional [email protected]
Patrick Hamilton, M.P.A.Health Insurance Specialist CMS Philadelphia Regional [email protected]
Annese St. LouisHealth Insurance SpecialistCMS Philadelphia Regional [email protected]


















