60
Is Your Facility Clean? DAZO Knows Sandra Von Behren 03/26/2010 1 TSICP
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | tyrell-manfull |
| View: | 214 times |
| Download: | 0 times |
Is Your Facility Clean?DAZO Knows
Sandra Von Behren
03/26/2010 1TSICP

Objectives
• Discuss the role of the environment in the transmission of healthcare-associated infections (HAIs) and multi-drug resistant organisms (MDROs)
• Identify available methods to evaluate environmental cleanliness
• Discuss strategies to improve environmental cleaning and decrease the risk of MDRO and HAI transmission
03/26/2010 TSICP 2
Philip C. Carling, MD
• Boston University School of Medicine
• Department of Epidemiology,Carney Hospital
• Boston, MA
03/26/2010 TSICP 3

The Environment as a Source of Pathogens
• S. aureus– Dancer et al; JHI 2006; 62: 200-206
• MRSA– Boyce et al, ICHE 1997; 18:622-627
• VRE– Bhalla et al, ICHE 2004; 25: 164-167– Hayden, et al, ICHE 2008; 29: 149-154
03/26/2010 TSICP 4

Environmental Contamination: Is There A Link to HAI
Acqusition?
Patients admitted to rooms previously occupied by patients with MRSA, VRE, Acinetobacter baumanii are at risk of acquiring organisms from the environment
03/26/2010 TSICP 5
Huang, et al; Arch Intern Med 2006; 166: 1945-1951Hardy , et al; ICHE 2006; 27: 127-132Sexton et al; JHI 2006; 62: 187-194Martinez, et al; Arch Intern Med 2003; 163: 1905-1912
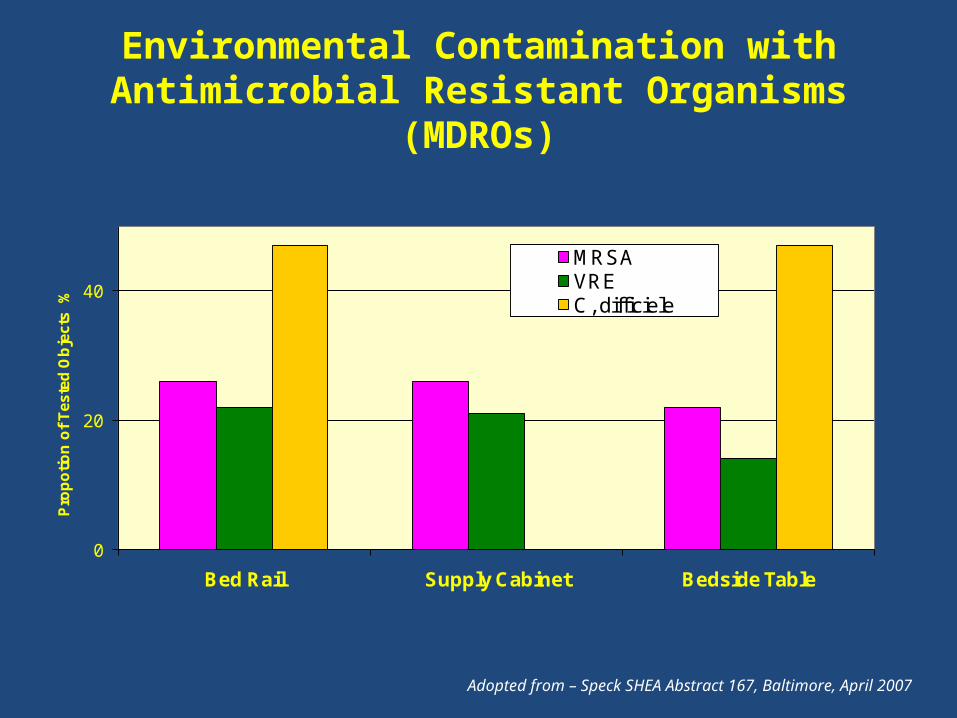
Environmental Contamination with Antimicrobial Resistant Organisms (MDROs)
0
20
40
Bed Rail Supply Cabinet Bedside Table
Pro
po
tio
n o
f T
es
ted
Ob
jec
ts
%
MRSAVREC, difficiele
Adopted from – Speck SHEA Abstract 167, Baltimore, April 2007
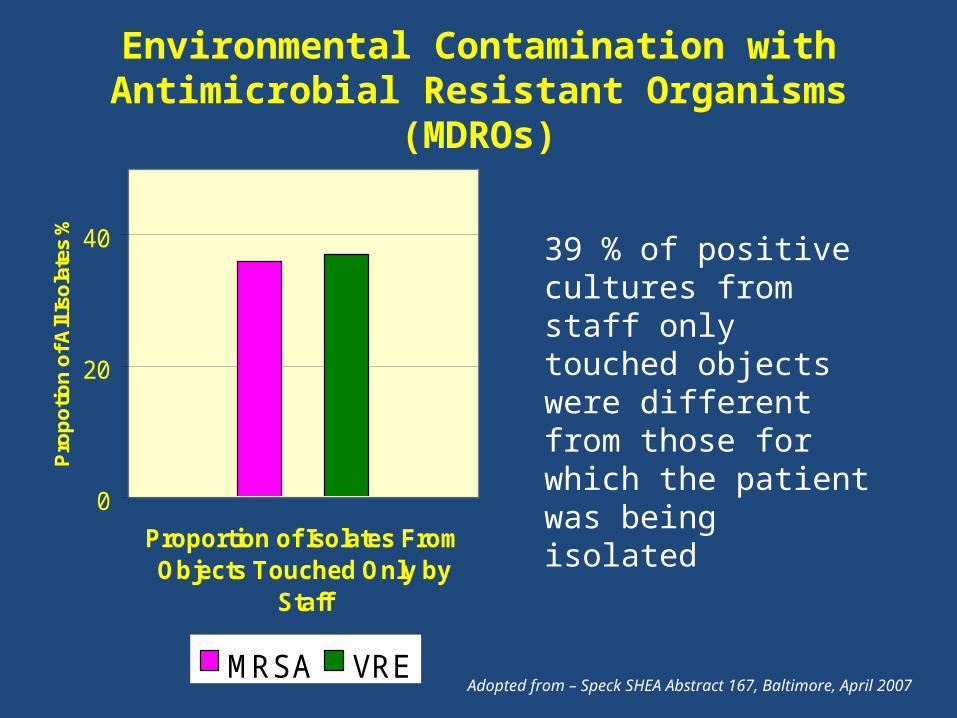
Environmental Contamination with Antimicrobial Resistant Organisms (MDROs)
0
20
40
Proportion of Isolates FromObjects Touched Only by
Staff
Pro
po
tion
of A
ll Is
ola
tes
%
MRSA VREAdopted from – Speck SHEA Abstract 167, Baltimore, April 2007
39 % of positive cultures from staff only touched objects were different from those for which the patient was being isolated

Rapid recontamination with MRSA of the environment of an intensive care unit after decontamination with
hydrogen peroxide vapour
0
2
4
6
8
10
12
WeekBefore
BeforeCleaning
AfterCleaning
AfterHPV
24Hr.post
4 WeeksPost
6 WeeksPost
MRSA Contamination
Patients Colonized
Adapted from - Hardy KJ et.al J Hosp. Infections 66,360 August 2007

C. Difficile Environmental Contamination
0
3000
6000
PT HANDS NEARENVIRONMENT
DISTANTENVIRONMENT
HCW HANDS
PCR
CO
LON
Y C
OU
NTS
/10c
m2
CDAD + PATIENT WARDS
CDAD - PATIENT WARDS
Mutters R, etal. J Hosp Infect. 2009; 71: 43-48
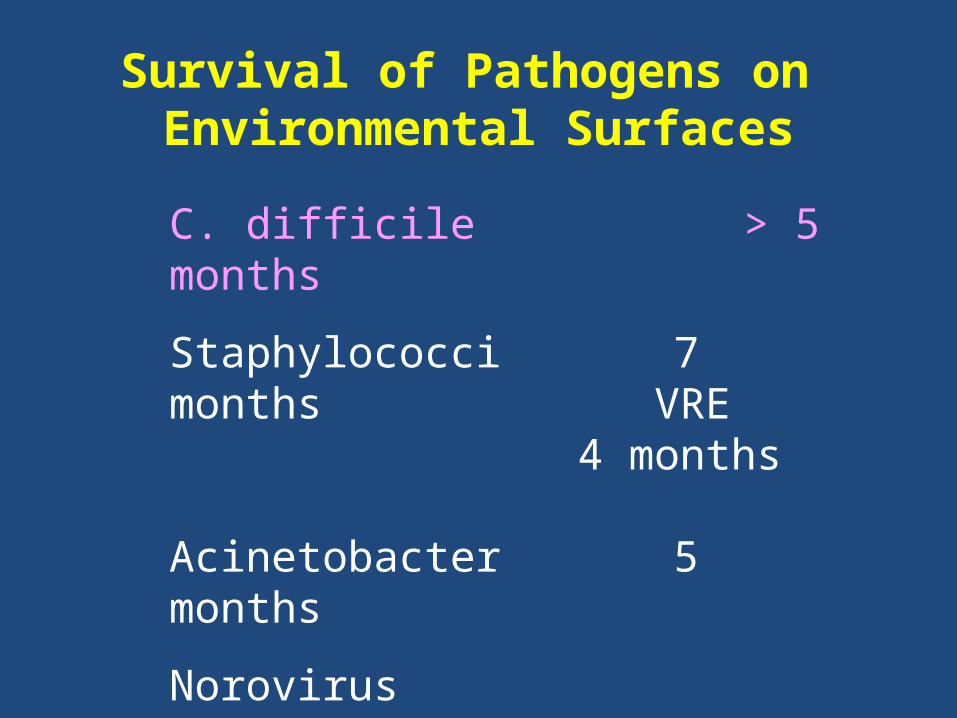
Survival of Pathogens on Environmental Surfaces
C. difficile > 5 months
Staphylococci 7 months VRE 4 months Acinetobacter 5 months
Norovirus 3 weeks Adenovirus 3 months Rotavirus 3 months SARS, HIV etc. days to week
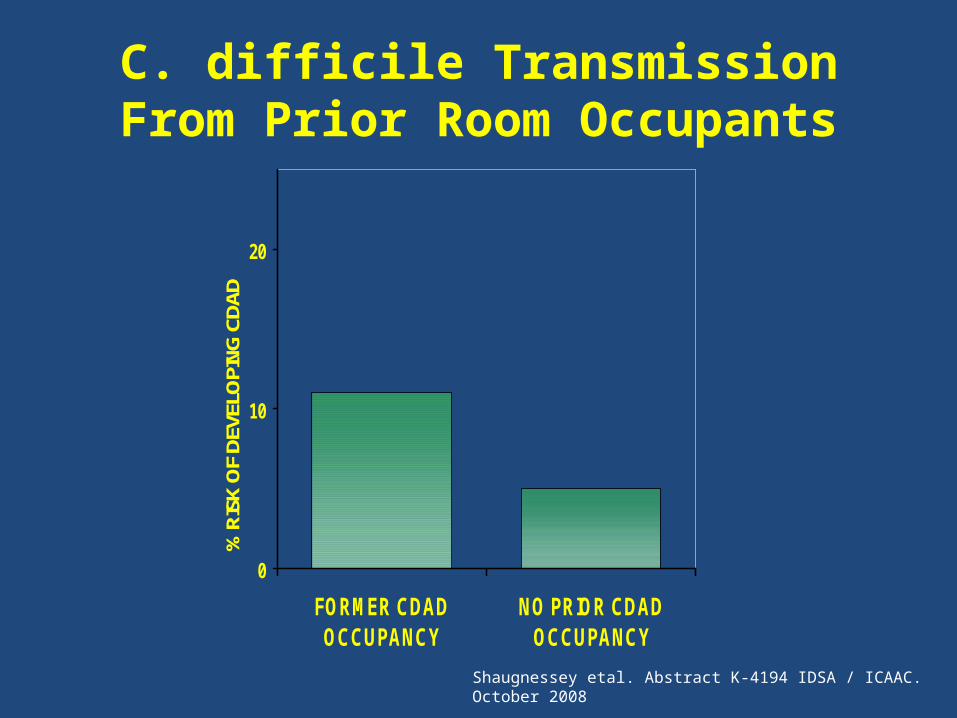
C. difficile Transmission From Prior Room Occupants
0
10
20
FORMER CDADOCCUPANCY
NO PRIOR CDADOCCUPANCY
% R
ISK
OF
DEVE
LOPI
NG C
DAD
Shaugnessey etal. Abstract K-4194 IDSA / ICAAC. October 2008

C. difficile Transmission to Prior Room Occupants
0
10
20
FORMER CDADOCCUPANCY
NO PRIOR CDADOCCUPANCY
% R
ISK
OF
DEVE
LOPI
NG C
DAD
Shaugnessey etal. Abstract K-4194 IDSA / ICAAC. October 2008
110% Increased risk
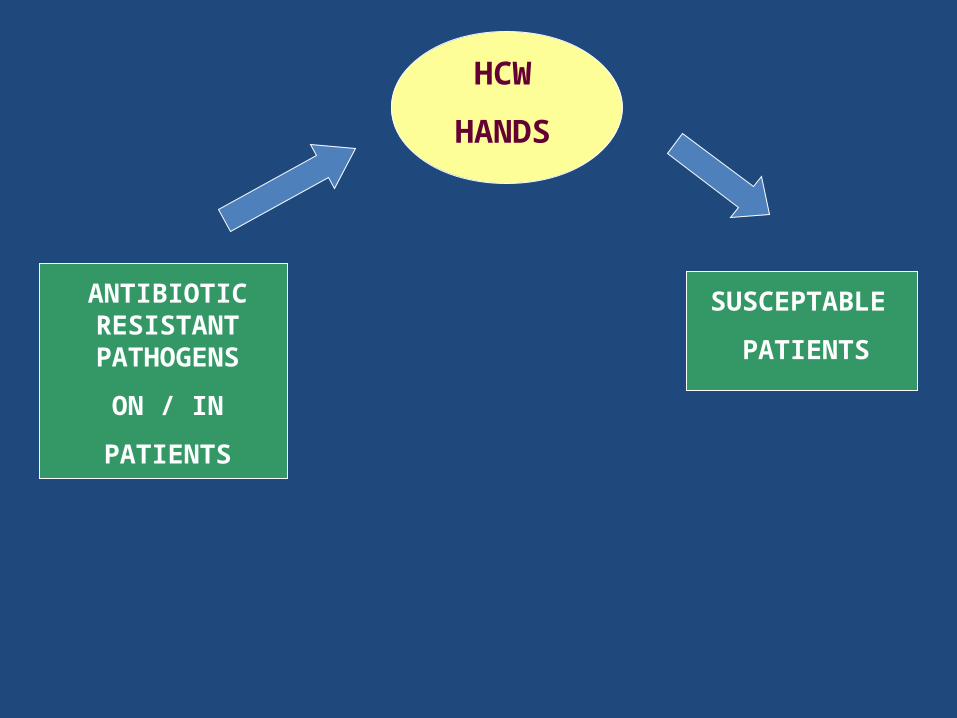
ANTIBIOTIC RESISTANT
PATHOGENS
ON / IN
PATIENTS
HCW
HANDS
SUSCEPTABLE
PATIENTS

ANTIBIOTIC RESISTANT
PATHOGENS
ON / IN
PATIENTS
HCW
HANDS
SUSCEPTABLE
PATIENTS
ISOLATION

ANTIBIOTIC RESISTANT
PATHOGENS
ON / IN
PATIENTS
HCW
HANDS
SUSCEPTABLE
PATIENTS
ISOLATIONHAND
HYGENE

ANTIBIOTIC RESISTANT
PATHOGENS
ON / IN
PATIENTS
ENVIRONMENTAL SURFACES
HCW
HANDS
SUSCEPTABLE
PATIENTS
ISOLATIONHAND
HYGENE

ANTIBIOTIC RESISTANT
PATHOGENS
ON / IN
PATIENTS
ENVIRONMENTAL SURFACES
HCW
HANDS
SUSCEPTABLE
PATIENTS
ISOLATIONHAND
HYGENE

ANTIBIOTIC RESISTANT
PATHOGENS
ON / IN
PATIENTS
ENVIRONMENTAL SURFACES
HCW
HANDS
SUSCEPTABLE
PATIENTS
ISOLATIONHAND
HYGENE
DISINFECTION CLEANING

Prevent Transmission:Hand Hygiene
• Many facilities have had significant improvements
• Microbial resurgence is rapid following HH• Logistical limitations in a complex
environment
03/26/2010 TSICP 20

HH in Complex Intense Environments is Very Difficult
30 to 40 HH “Moments” per Hour during direct patient care
Isolation
• Difficult to implement and maintain• When to Begin—When to stop• Unintended consequences
03/26/2010 TSICP 22

Isolation is Difficult
Our review of the literature demonstrates that contact precautions have unintended consequences that are potentially deleterious to the patient. Measures to ameliorate these deleterious consequences of contact precautions are urgently needed.
Am J Infect Control. 2009 (May); 37: 85-91

What can we do??
Improve effectiveness of environmental cleaning/disinfection patient environment
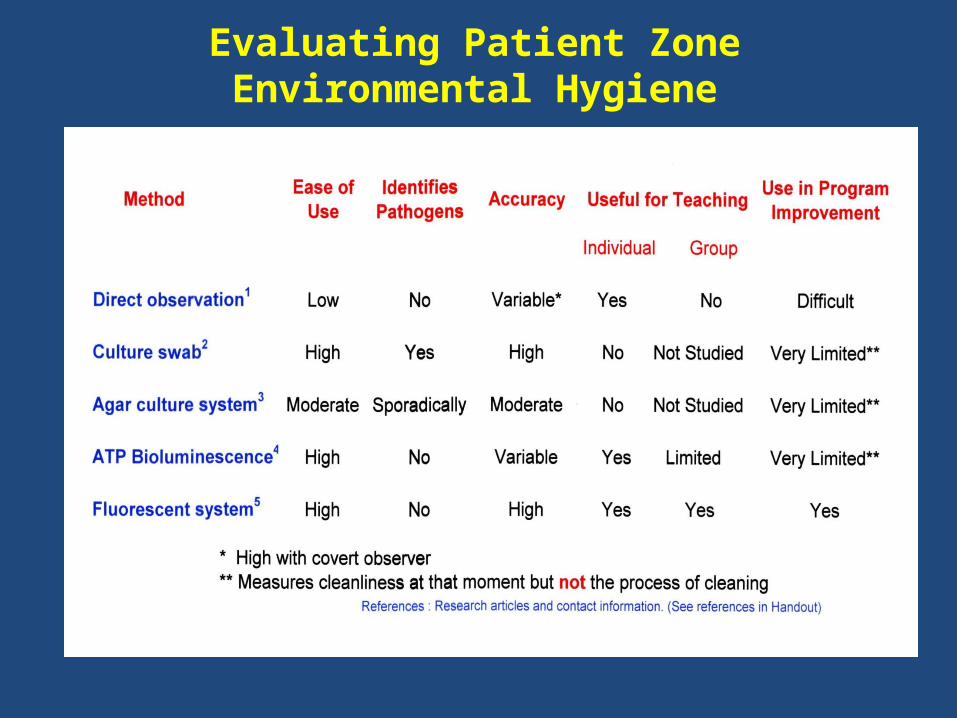
How Can We Evaluate Environmental Cleaning
• Direct observation• Culture the environment• ATP bioluminescence Tool• Fluorescent marking tool
03/26/2010 TSICP 26
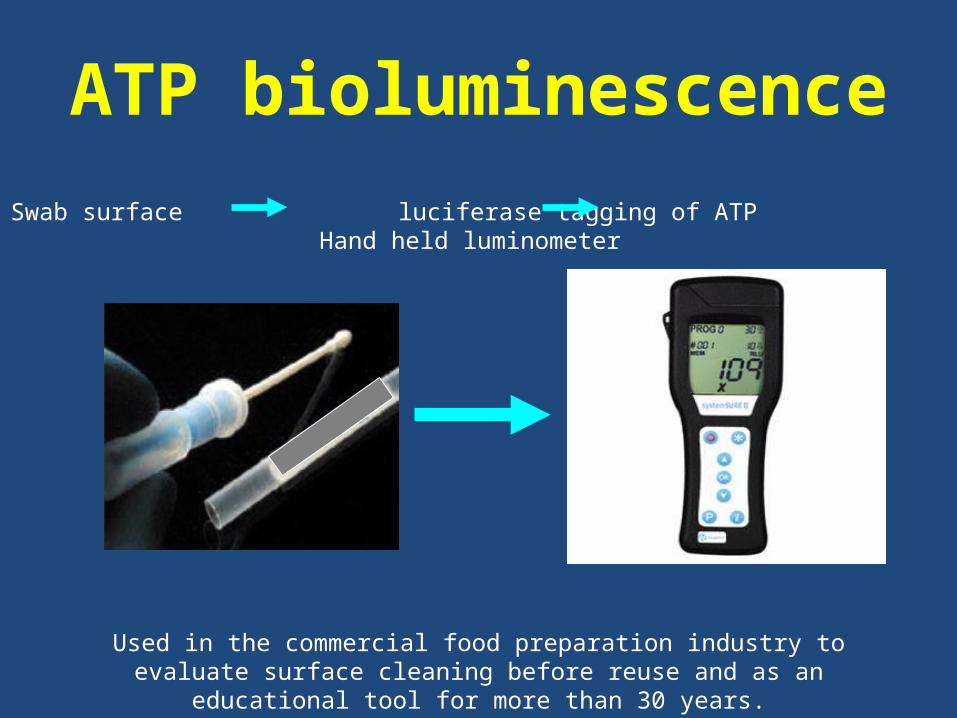
ATP bioluminescence
Swab surface luciferase tagging of ATP Hand held luminometer
Used in the commercial food preparation industry to evaluate surface cleaning before reuse and as an educational tool for more than 30 years.
ATP Bioluminescence Testing in Healthcare Settings
Potential usefulness:Has been used as a surrogate for environmental culturing
Provides an estimate of cleanliness
Can rapidly define how clean an object is…. but non-microbial ATP is also evaluated
Standards to optimize predictive values are still being evaluated
Can be used to do one-on-one education of ES staff

ATP Bioluminescence Testing in Healthcare Settings
Potential limitations:Secondary cleaning of the site is required to remove
disinfectant induced signal decay or enhancement.
Involvement of the ES staff is implicit since evaluation must be done within minutes of cleaning.
Pre-intervention evaluation of disinfection cleaning is difficult without inducing a Hawthorne effect
Results are individual ES staff / time specific.
Many manufacturers of luminometers and ATP swabs makes interinstitutional standardization difficult

Evaluating Patient Zone Environmental Hygiene

Evaluating Patient Zone Environmental Hygiene

Evaluating Patient Zone Environmental Hygiene
Evaluating Patient Zone Environmental Hygiene

GOAL OF THE PROJECT
To develop a surrogate marking system to evaluate the effectiveness of environmental cleaning/disinfection of the near-patient environment

Dazo Solution(Initially called “GOO”)

Target After Marking

Target Enhanced

The Targeting Solution
• A mixture of several glues, soaps and a targeting dye which: – Dries rapidly – Remains stable – Easily removed with light abrasion and damp cloth
– Inconspicuous
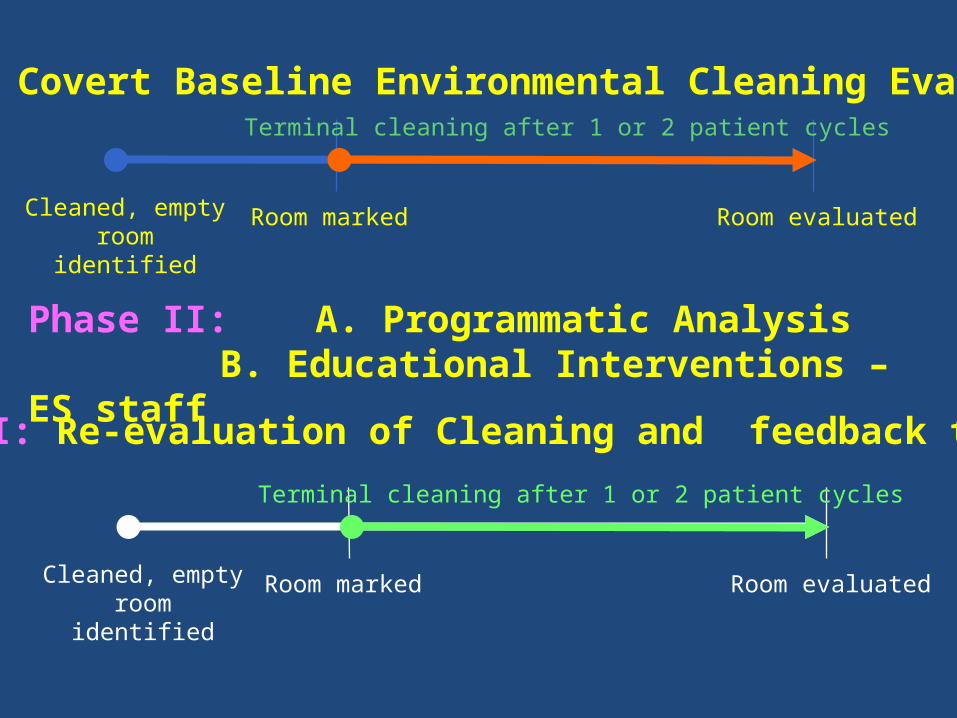
Cleaned, empty room
identified
Room marked Room evaluated
Terminal cleaning after 1 or 2 patient cycles
Phase I: Covert Baseline Environmental Cleaning Evaluation
Phase II: A. Programmatic AnalysisB. Educational Interventions – ES staff
Cleaned, empty room
identified
Room marked Room evaluated
Terminal cleaning after 1 or 2 patient cycles
Phase III: Re-evaluation of Cleaning and feedback to ES
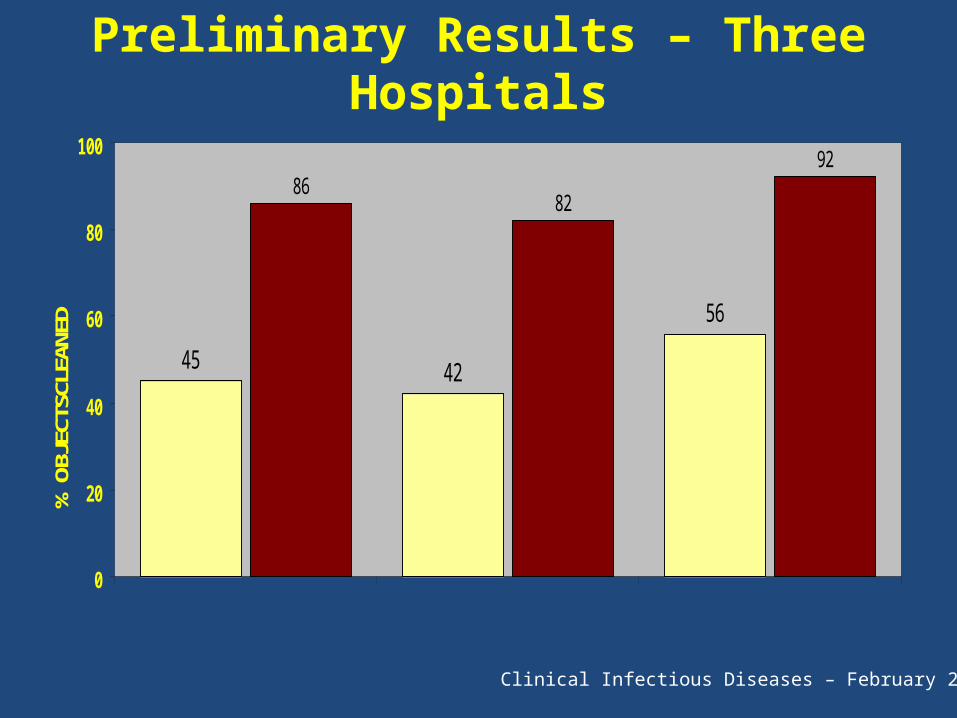
Preliminary Results – Three Hospitals
45 42
56
8682
92
0
20
40
60
80
100
% O
BJEC
TSCL
EANE
D
HOSPITAL A HOSPITAL CHOSPITAL B
Clinical Infectious Diseases – February 2006

On the basis of our preliminary results and presentations at SHEA, APIC and ICAAC conferences we have gathered together a group of hospitals to further evaluate the tool and process improvement programs
The Healthcare Environmental Hygiene Study Group
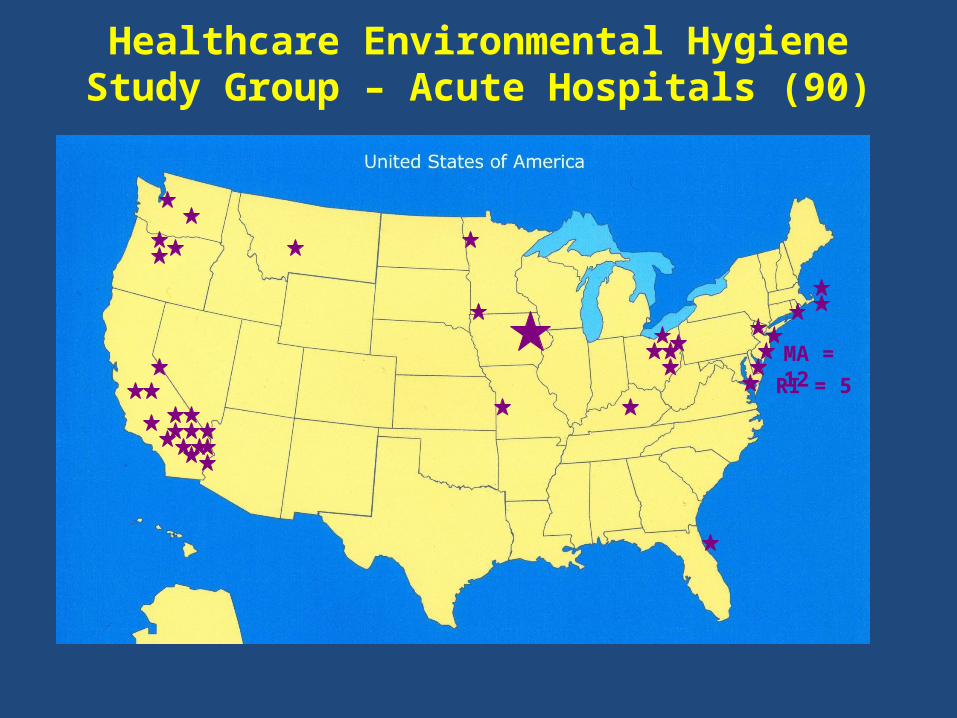
Healthcare Environmental Hygiene Study Group – Acute Hospitals (90)
MA = 12RI = 5


0
2
4
6
8
1-5% 11-15%
21-25%
31-35%
41-45%
51-55%
61-65%
71-75%
81-85%
91-95%
Baseline Environmental Evaluation of
36 Acute Care Hospitals
% of Objects Cleaned
Hos
pita
ls
Mean = 48.5 %
(20,056 Objects)

PROPORTION OF OBJECTS CLEANED AS PART OF TERMINAL ROOM CLEANING IN 20 ACUTE CARE HOSPITALS
0
20
40
60
80
100
%
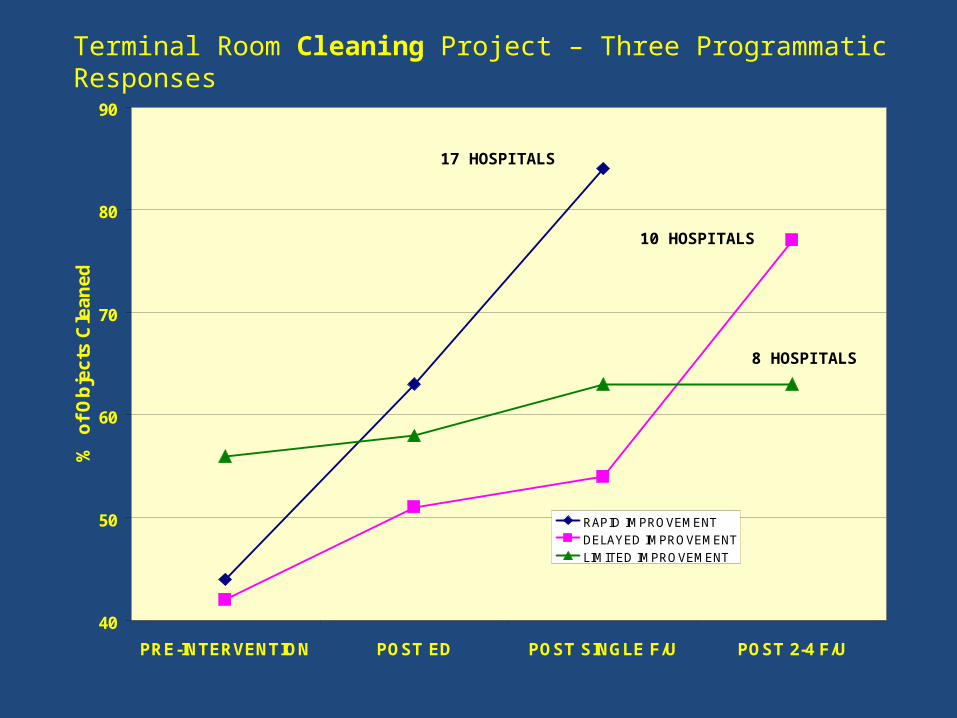
40
50
60
70
80
90
PRE-INTERVENTION POST ED POST SINGLE F/U POST 2-4 F/U
% o
f O
bje
cts
Cle
an
ed
RAPID IMPROVEMENT
DELAYED IMPROVEMENT
LIMITED IMPROVEMENT
17 HOSPITALS
10 HOSPITALS
8 HOSPITALS
Terminal Room Cleaning Project – Three Programmatic Responses
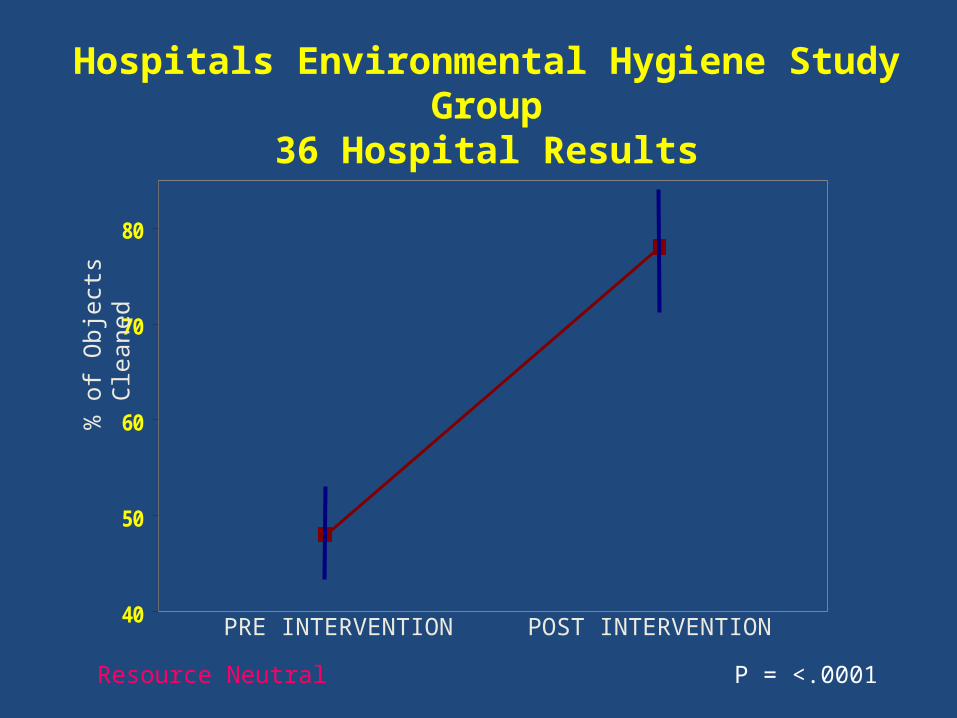
40
50
60
70
80
Hospitals Environmental Hygiene Study Group36 Hospital Results
% o
f Obj
ects
Cle
aned
PRE INTERVENTION POST INTERVENTION
P = <.0001Resource Neutral

TERMINAL ROOM CLEANING INFECTION PREVENTION
TARGETS
Sink and FaucetsToilet SurfacesToilet Flush HandleBedpan CleanerToilet Area HandholdsToilet Area Door Knobs or Push PlatesBedside TableTray TablePatient ChairSide RailsRoom Door KnobsCall BoxTelephoneBathroom Light Switches
Specific Opportunities for Improvement

Focus Group
• Held 4 meetings with Environmental Services (EVS) staff on different shifts– 5-6 staff members in each session– Met for 4 hours– No EVS supervisors present– Meal provided
03/26/2010 TSICP 49
Focus Group Questions
• What recommendations do you have to improve cleaning outcomes?
• What barriers do you see that would prevent implementation of these recommendations?
03/26/2010 TSICP 50

Problems Identified
• Staffing not always adjusted to busiest times• Pressure from nursing staff to “get it done”• Supervisors not visible• Staff on evening shift “on call” from one end
of hospital to the other
03/26/2010 TSICP 51
Recommendations
• More “on the spot” feedback from supervisors• Help from supervisors to prioritize work• Better communication with nursing• Consistency unit to unit• Maintain level of cleaning done when TJC is
expected• Have a quality control officer• Use Dazo as follow-up to classroom orientation• Evaluation of work efficiencies (Organizational
Improvement)
03/26/2010 TSICP 52
ICU Project
• Daily Clean of Isolation Rooms• Marked room and read in or 2 days
03/26/2010 TSICP 53

Possible Interventions?
• How can we improve on daily disinfection cleanings?• Who is responsible for each item?
-Siderail bed control -Table/counter/workspace-Call button -Computer keyboard-Tray table -Storage drawer handle-Monitor control -Room light switch-Vent control - Room door handles-Commode -IV pump-Sink

Item Responsibility
• Environmental Services:– Tray table– Light switch– Room door handles– Sink– Work surface– Cabinet handles– Call button– In-room commode
• ICU Nursing:– Keyboards– Side rails– IV pumps– Monitor control panel
• Respiratory Therapists:– Ventilator Control Panel
Re-evaluation will take place in 3-4 weeksRe-evaluation will take place in 3-4 weeks

Brigham & Woman’s ICU Study
44
71
45
27
0
20
40
60
80
PRE-INTERVENTION
POSTINTERVENTION
%
THOROUGHNESS OF CLEANING
MRSA/VRE CONTAMINATION

Brigham & Woman’s ICU Study
Impact of an Environmental Cleaning Intervention on the Risk of Acquiring MRSA and VRE from Prior Room Occupants (SHEA Abstract 273) 2009
Datta R, Platt R, Kleinman K, Huang SS

Brigham & Woman’s ICU Study
Impact of an Environmental Cleaning Intervention on the Risk of Acquiring MRSA and VRE from Prior Room Occupants (SHEA Abstract 273) 2009
Datta R, Platt R, Kleinman K, Huang SS
“For both MRSA and VRE, absolute risk appeared diminished during the intervention regardless of prior occupant status”

Conclusions
• It is likely that surfaces in the Patient Zone are of relevance in the transmission of Healthcare Associated Pathogens.
• While optimizing hand hygiene and isolation practice is clearly important there is no reason why the effectiveness and thoroughness of environmental hygienic cleaning should not also be optimized, particularly since such an intervention can be essentially resource neutral.
References
1. Hayden MK, Bonten JM, Blom DW, Lyle EA. Reduction in acquisition of Vancomycin-resistant enterococcus after enforcement of routine environmental cleaning measures. Clin Infect Dis 2006; 42:1552-1560.
2. Eckstein BC, Adams DA, et al. Reduction of Clostridium Difficile and vancomycin-resistant Enterococcus contamination of environmental surfaces after an intervention to improve cleaning methods. BMC Infect Dis. 2007 Jun 21;7:61
3. Dancer SJ, White L, Robertson C. Monitoring environmental cleanliness on two surgical wards. Int J Env Health Res 2008; 18: 357-364
4. 195.92.246.148/knowledge_network/documents/Bioluminescence_20070620104921.pdf
5. Carling PC, Parry M, Rupp, M, Po JL,DickB, Von Beheren S. for the Healthcare Environmental Hygiene Study Group. Improving Cleaning of the Environment Surrounding Patients in 36 Acute Care Hospitals. Infection Control and Hospital Epidemiology 2008; 29:11,035-1041

















