16
IS YOUR ORGANISATIONAL QUALITY SYSTEM SUPPORTING YOU TO MEET THE NEW ACCREDITATION REQUIREMENTS? Dr Cathy Balding 1 www.cathybalding.com
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | shannon-hall |
| View: | 219 times |
| Download: | 3 times |

1
IS YOUR ORGANISATIONAL QUALITY SYSTEM SUPPORTING YOU TO MEET THE NEW ACCREDITATION REQUIREMENTS?
Dr Cathy Balding
www.cathybalding.com
Falls account for up to 75% of adverse events
in some settings
Errors with medications and blood are key threats to patients
18% patients in hospitals Have at least one pressure ulcer and a stage 4 ulcer costs approx $80k
CABG costs 3x as much if
the patient gets an infection
The quality game changed in 1995…
Blood clots (VTE) kill
three times more people
than die on Australian
roads
The 1995 QAHC Study found that 16.6% patients are harmed in Australian hospitals
10,000 people
worldwide are
harmed by medical
error every day
2

• Adverse events increase the case cost up to 7X; and $1 in every $7 spent on healthcare in Australia is used to treat a healthcare-associated injury
• (Ehsani J, Jackson T, Duckett S (2006) The Incidence and Cost of Adverse Events in Victorian Hospitals, 2003–04. MJA, vol 184 no 11, pp. 551–55)
• 27% patients experience healthcare-associated harm in the US in 2012 - 48% of these are preventable
• (US Office of Inspector General, 2012 study of Medicare patients in 189 hospitals)
• Up to 83% incidents are not reported • (U.S. Office of Inspector General Medicare patients study, 2012)
• 57% of patients receive care based on best available evidence via guidelines • (Runciman WB et al. CareTrack: assessing the appropriateness of healthcare delivery in Australia. Medical Journal of
Australia 2012;197(2):100-105)
Since then?

4
Our Risk Systems improved…
But our quality systems?...
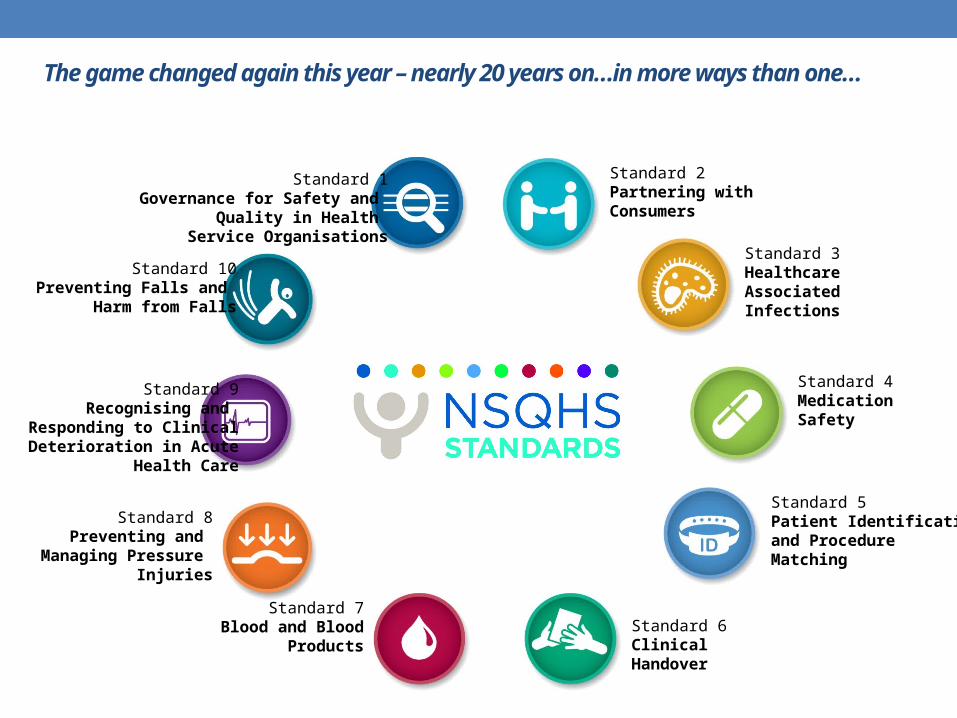
Standard 7Blood and Blood
Products
Standard 10Preventing Falls and
Harm from Falls
The game changed again this year – nearly 20 years on…in more ways than one…
Standard 1Governance for Safety and
Quality in Health Service Organisations
Standard 2Partnering withConsumers
Standard 4Medication Safety
Standard 3Healthcare AssociatedInfections
Standard 8Preventing and
Managing Pressure Injuries
Standard 9Recognising and
Responding to ClinicalDeterioration in Acute
Health Care
Standard 5Patient Identificationand ProcedureMatching
Standard 6ClinicalHandover

Improving quality (and achieving the nationals safety and quality standards) can be transactional – doing stuff and ticking boxes…
Improvement:
Improving existing care and services, reacting, reducing
risk
Maintenance and Compliance:
Monitoring quality and risk, ensuring standards and policies are met
What’s the point?
Quality/Clinical Governance Systems
6
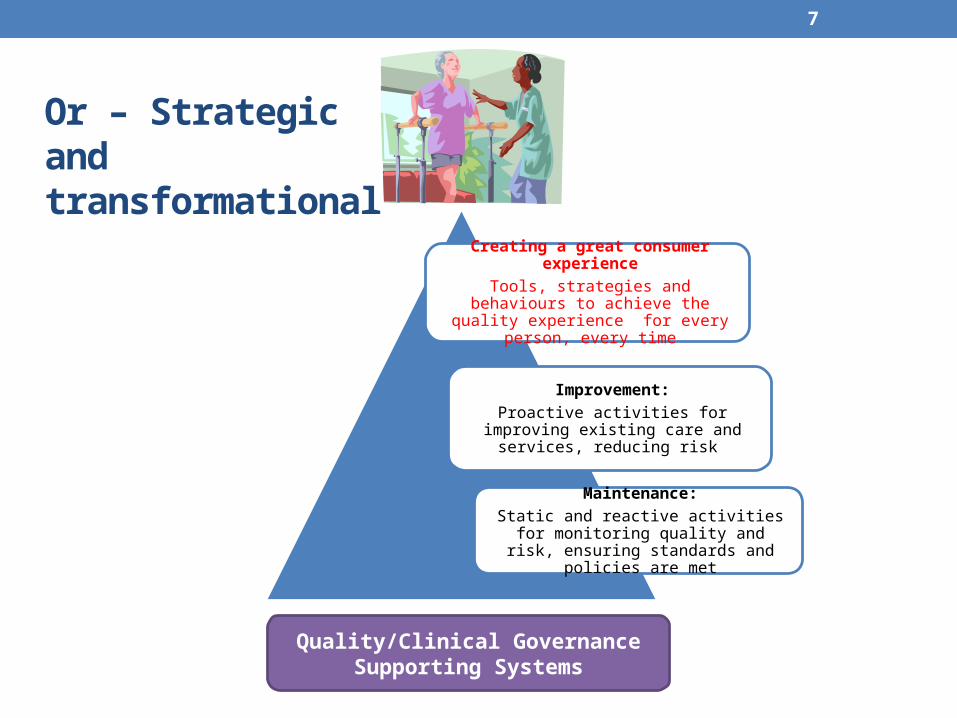
Creating a great consumer experience
Tools, strategies and behaviours to achieve the quality experience for every
person, every time
Improvement:
Proactive activities for improving existing care and services, reducing risk
Maintenance:
Static and reactive activities for monitoring quality and risk, ensuring standards and
policies are met
7
Quality/Clinical Governance Supporting Systems
Or – Strategic andtransformational

8
But…
How do you get from transactional…
to transformational?

Ideal Care
Unacceptable Care
It’s not easy in a complex environment…
Time
9
10
Where are you starting?
Your organisation’s quality framework and plan is?
• A clear map for supporting staff to reach the destination of great care for every consumer every time?
• A series of quality activities heading in different directions?
• A Quality Manager ‘to do’ list?

Health Service Organisational Quality System Maturity Scale (Balding 2013)Maturity Level Characteristics1. Informal • Lack of systematic approach: random improvement activities based on minimal and poor data.
• Managerial response to quality problems largely dependent on staff ‘trying harder’. • Limited staff input into identifying problems and improvements.
2. Compliance
• Problem based and reactive approach with minimal systematic collection or analysis of data on key issues. • Focus on compliance with external/funding requirements. • ‘Doing quality’ is staff code for auditing and other data collection with little implementation or follow up.• Lack of relationship between quality system mechanics and quality of care – ‘quality’ still seen as the responsibility of the quality
manager. 3. Reactive Risk
• Focus on risk management and compliance with accreditation and other external requirements. .• Systematic tracking of key indicators, consumer feedback and incident reporting.• Evidence of some system improvement and follow up. • No agreed change and improvement model in use. • Reliance on policy shifts and education as key change tools. • Leaders are developed to improve safety.
4. Proactive Continuous Improvement
• Quality system is a key component of clinical/quality governance system and is integrated at operational level, with plans for improvement at organisation-wide and local levels.
• Lack of common and uniting goals with the improvement program comprising a series of (possibly unrelated) monitoring, improvement and redesign projects.
• Minimum dataset reported across all quality dimensions, • Data are analysed and reported through the organisational levels to the governing body, and there is evidence of effective systems
improvement as a result. • Strategies in place for developing leaders to engage staff and consumers in improvement across the dimensions of quality.
5. Strategic • The desired quality of the consumer experience at point of care is defined with staff and consumers, and achieving it is a strategic priority.
• The organisational quality plan is designed and systematically implemented to create the defined quality consumer experience, through developing people and improving systems.
• Roles and responsibilities at all levels of the organisation for creating the quality consumer experience are described and supported.
• Governance systems are owned by the governing body and executive team and designed to support staff to create the quality consumer experience.
• A model for change and improvement is in use.
Let’s get concrete!

:And then seek crystal clarity about the What, Who and Why
‘3PQ’ Purpose, People and Pillars for creating great consumer experiences (Balding, 2013)
Purpose:Creating a consumer
experience that is:ResponsiveIntegrated
Safe Effective
QG Pillars
Goals, objectives, measures, data, risk and improvement strategies
Culture, leaders, support, roles, development, training
Evidence, standards, policy, systems, resources
People Empathic Skilled Informed Proactive Accountable
Board and Executive

13
Integrate the quality system as a strategic and operational pillar of your organisation
Goal
Care and services are delivered as a partnership between consumers and staff and based on mutual respect: We listen.
Consumers are not harmed by our care and services: We do not harm.
Care and services experienced by each consumer are right for that person and achieve what they are designed to do: The right thing that works.
Consumers experience our care and services as coordinated and streamlined: No surprises.
Dimension of Quality
Person centred
Safe
Appropriate and Effective
Continuous and Integrated

Make it real
Responsive to each person:
We
listen
No Harm:Our
consumers
are safe
The right thing with the right
outcome:
Get it
right
Coordinated and Smooth:
No
SurprisesDr Cathy Balding 2012 www.cathybalding.com

15
Make it real…

16
THANKYOU!
www.cathybalding.com

















