72
Isolation Precautions Allison McGeer, MSc, MD, FRCPC Mount Sinai & Princess Margaret Hospitals, Toronto Routine Practices and Additional Precautions Infection Prevention and Control
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | lesley-thornton |
| View: | 220 times |
| Download: | 2 times |
Isolation Precautions Isolation Precautions
Allison McGeer, MSc, MD, FRCPC
Mount Sinai & Princess Margaret Hospitals, Toronto
Allison McGeer, MSc, MD, FRCPC
Mount Sinai & Princess Margaret Hospitals, Toronto
Routine Practices and Additional Precautions Infection Prevention and Control
Why worry about hospitals and Why worry about hospitals and infection?infection?
Pathogens are concentrated (people with them require admission)
Susceptible hosts are concentrated (ill people are susceptible, medical care makes them more so)
Contact is concentrated (many people in proximity; hands on care)
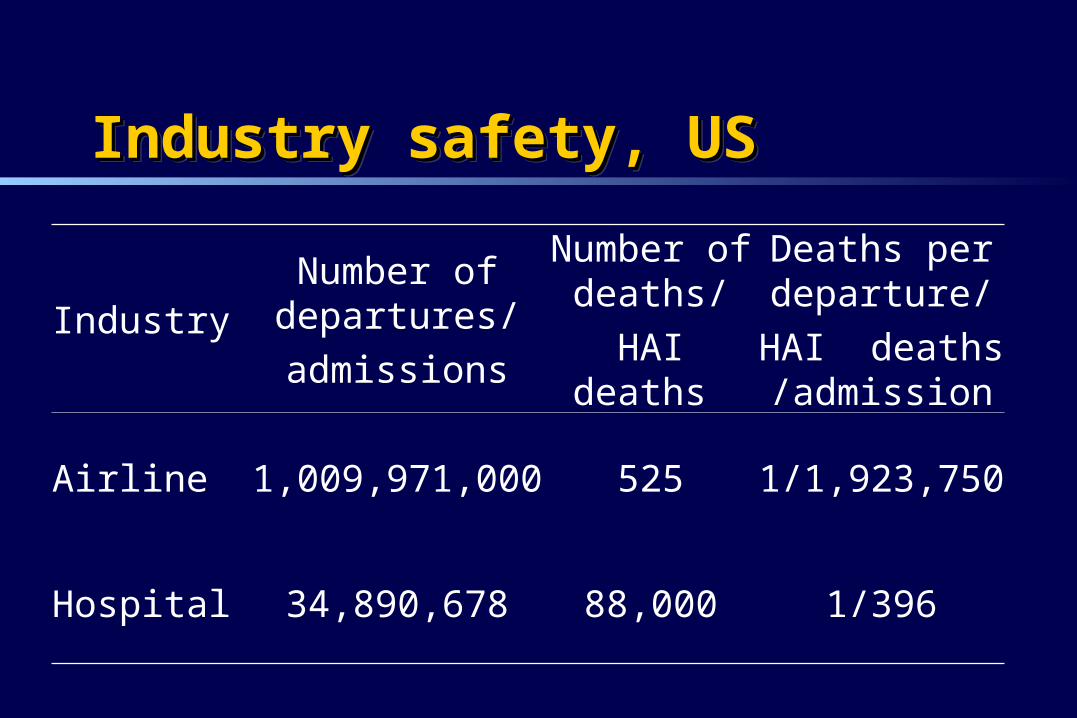
Industry safety, USIndustry safety, USIndustry safety, USIndustry safety, US
IndustryNumber of departures/
admissions
Number of deaths/
HAI deaths
Deaths per departure/
HAI deaths /admission
Airline 1,009,971,000 525 1/1,923,750
Hospital 34,890,678 88,000 1/396
Hospital-acquired Infections Hospital-acquired Infections Hospital-acquired Infections Hospital-acquired Infections
One in every 8 people who are admitted to a Canadian hospital develop an infection associated with their care
Once an hour, someone in Canada dies of a hospital-acquired infection
Once every 35 minutes, a new hospital patient in a Ontario becomes colonized with MRSA
One in every 8 people who are admitted to a Canadian hospital develop an infection associated with their care
Once an hour, someone in Canada dies of a hospital-acquired infection
Once every 35 minutes, a new hospital patient in a Ontario becomes colonized with MRSA
Infection controlInfection controlInfection controlInfection control Hospital design
– Prevention of legionellosis, aspergillosis, SSIs– Support for safe practice
Maintenance of practice to prevent infection– Surgery
prevention of SSI
– Procedures prevention of CRBSI, urinary tract infections, needlestick injuries
– Prevention of person to person transmission of pathogens Hand hygiene, additional precautions etc.
Hospital design– Prevention of legionellosis, aspergillosis, SSIs– Support for safe practice
Maintenance of practice to prevent infection– Surgery
prevention of SSI
– Procedures prevention of CRBSI, urinary tract infections, needlestick injuries
– Prevention of person to person transmission of pathogens Hand hygiene, additional precautions etc.
FundamentalsFundamentalsPrevention of transmissionPrevention of transmissionFundamentalsFundamentalsPrevention of transmissionPrevention of transmission
Hospital design Education Hand hygiene Routine practices and additional precautions Occupational Health
Hospital design Education Hand hygiene Routine practices and additional precautions Occupational Health
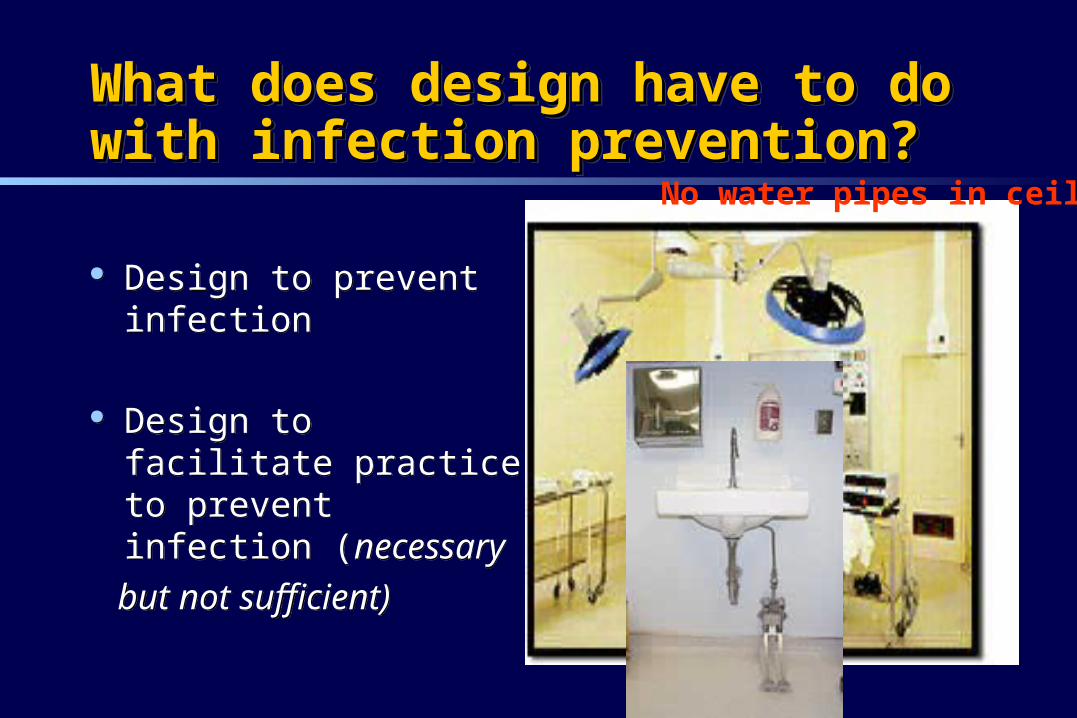
What does design have to do with What does design have to do with infection prevention?infection prevention?What does design have to do with What does design have to do with infection prevention?infection prevention?
Design to prevent infection
Design to facilitate practice to prevent infection (necessary
but not sufficient)
Design to prevent infection
Design to facilitate practice to prevent infection (necessary
but not sufficient)
No water pipes in ceiling
Mechanisms of transmissionMechanisms of transmissionMechanisms of transmissionMechanisms of transmission Airborne
Droplet
Contact (direct and indirect)
Airborne
Droplet
Contact (direct and indirect)
Protection from Airborne Infection Protection from Airborne Infection Protection from Airborne Infection Protection from Airborne Infection
Overall ventilation Adequate numbers of airborne isolation
rooms– Emergency department– Endoscopy suite– ICU– Medical/surgical wards
Overall ventilation Adequate numbers of airborne isolation
rooms– Emergency department– Endoscopy suite– ICU– Medical/surgical wards
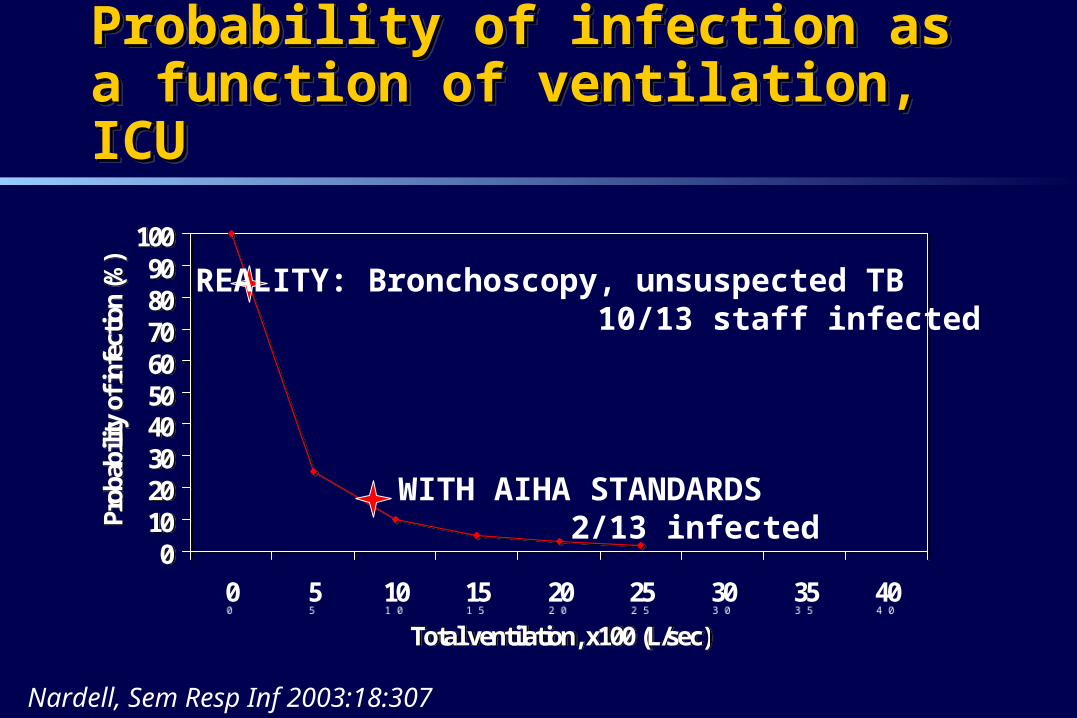
Probability of infection as a function of Probability of infection as a function of ventilation, ICUventilation, ICUProbability of infection as a function of Probability of infection as a function of ventilation, ICUventilation, ICU
0102030405060708090
100
0 5 10 15 20 25 30 35 40
Total ventilation, x100 (L/sec)
Prob
abili
ty o
f inf
ectio
n (%
)
0102030405060708090
100
0 5 10 15 20 25 30 35 40
Total ventilation, x100 (L/sec)
Prob
abili
ty o
f inf
ectio
n (%
)
REALITY: Bronchoscopy, unsuspected TB 10/13 staff infected
WITH AIHA STANDARDS 2/13 infected
Nardell, Sem Resp Inf 2003:18:307
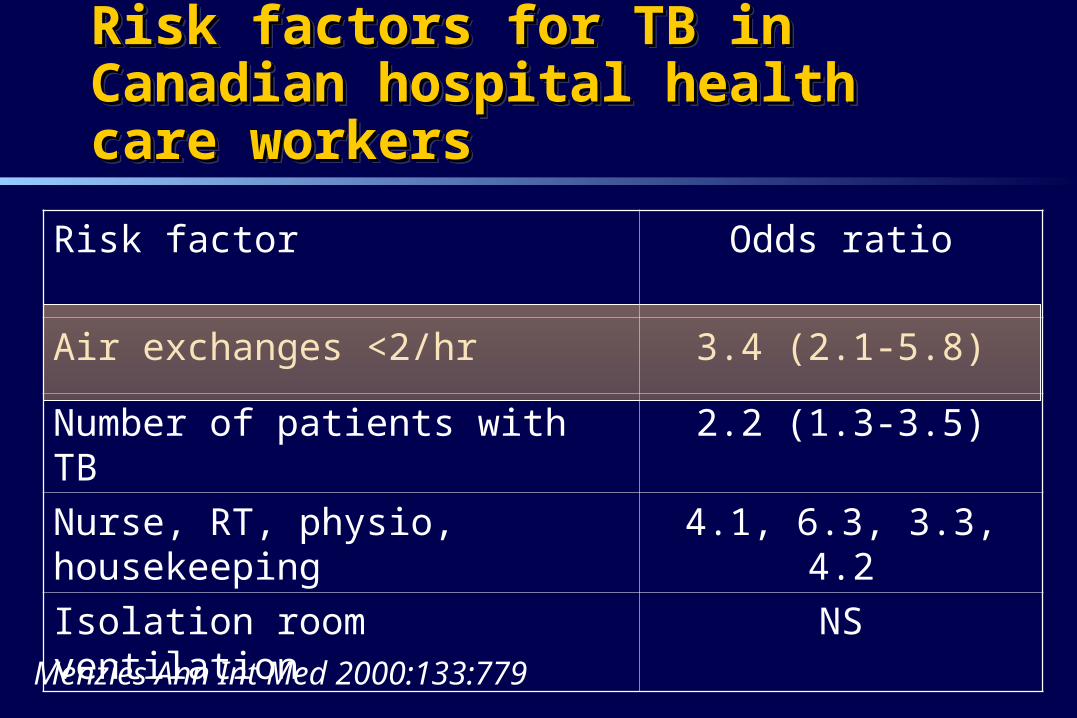
Risk factors for TB in Canadian hospital Risk factors for TB in Canadian hospital health care workershealth care workersRisk factors for TB in Canadian hospital Risk factors for TB in Canadian hospital health care workershealth care workers
Menzies Ann Int Med 2000:133:779
Risk factor Odds ratio
Air exchanges <2/hr 3.4 (2.1-5.8)
Number of patients with TB 2.2 (1.3-3.5)
Nurse, RT, physio, housekeeping 4.1, 6.3, 3.3, 4.2
Isolation room ventilation NS
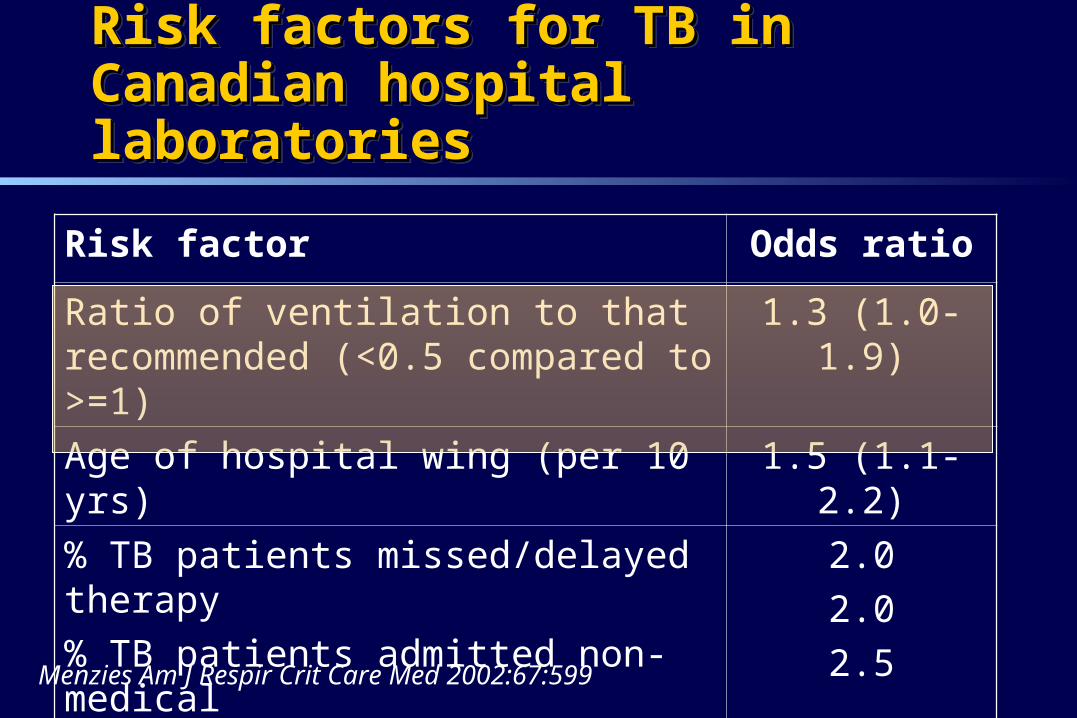
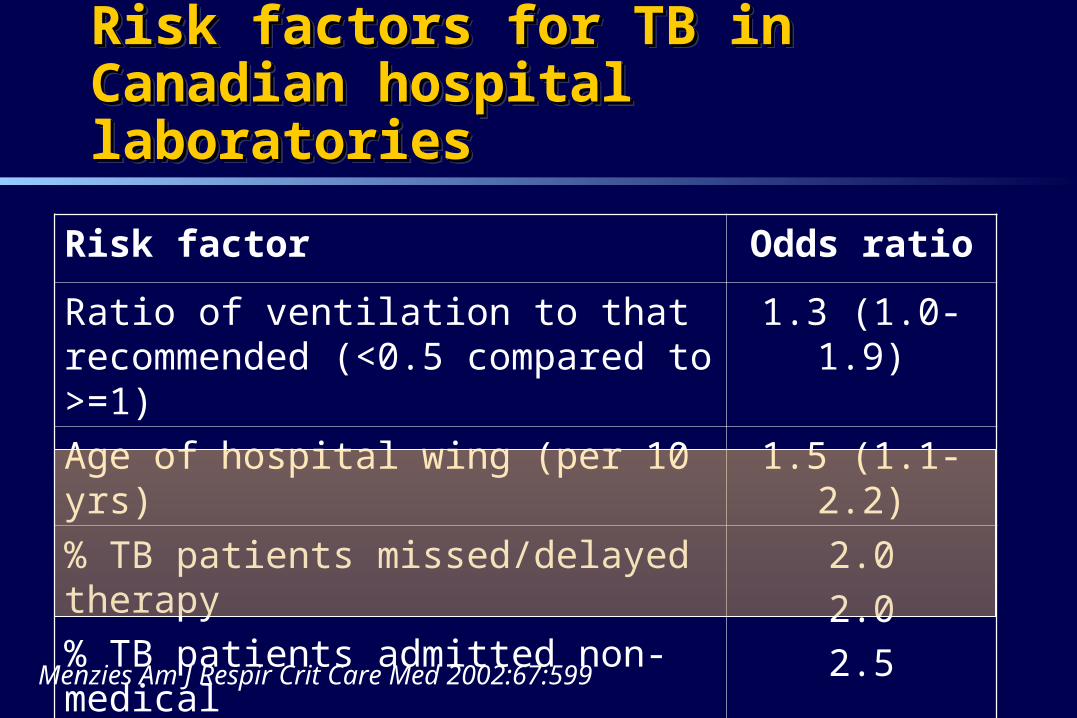
Risk factors for TB in Canadian hospital Risk factors for TB in Canadian hospital laboratorieslaboratoriesRisk factors for TB in Canadian hospital Risk factors for TB in Canadian hospital laboratorieslaboratories
Menzies Am J Respir Crit Care Med 2002:67:599
Risk factor Odds ratio
Ratio of ventilation to that recommended (<0.5 compared to >=1)
1.3 (1.0-1.9)
Age of hospital wing (per 10 yrs) 1.5 (1.1-2.2)
% TB patients missed/delayed therapy
% TB patients admitted non-medical
% TB patients who died
2.0
2.0
2.5
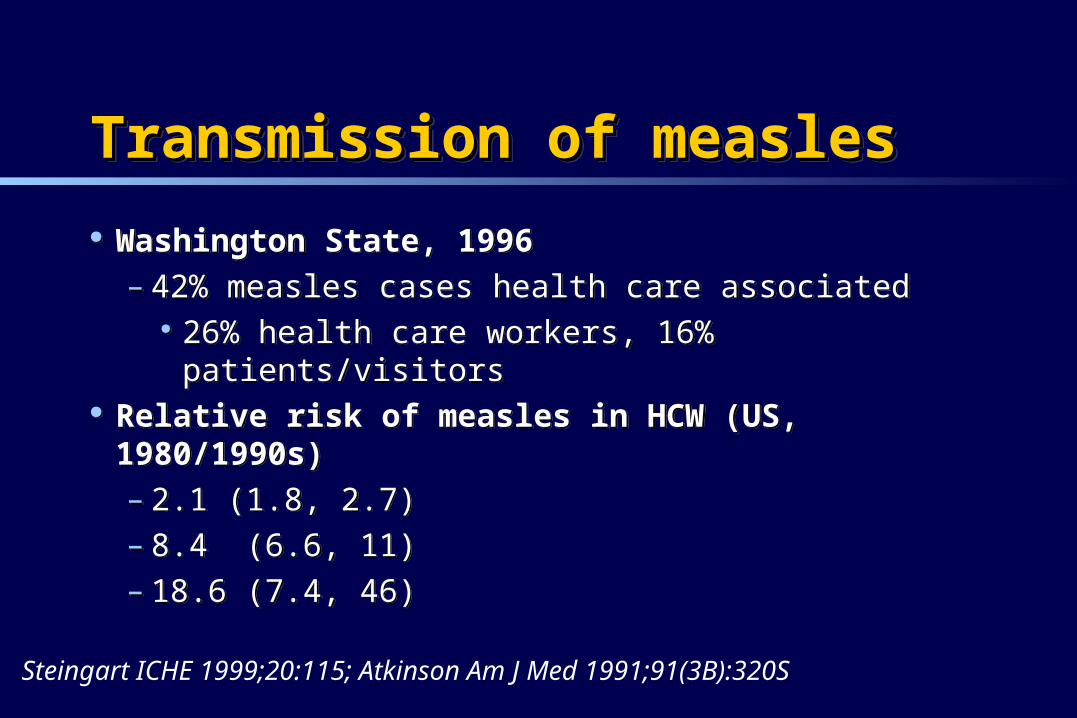
Transmission of measlesTransmission of measlesTransmission of measlesTransmission of measles
Washington State, 1996– 42% measles cases health care associated
26% health care workers, 16% patients/visitors Relative risk of measles in HCW (US, 1980/1990s)
– 2.1 (1.8, 2.7)– 8.4 (6.6, 11)– 18.6 (7.4, 46)
Washington State, 1996– 42% measles cases health care associated
26% health care workers, 16% patients/visitors Relative risk of measles in HCW (US, 1980/1990s)
– 2.1 (1.8, 2.7)– 8.4 (6.6, 11)– 18.6 (7.4, 46)
Steingart ICHE 1999;20:115; Atkinson Am J Med 1991;91(3B):320S
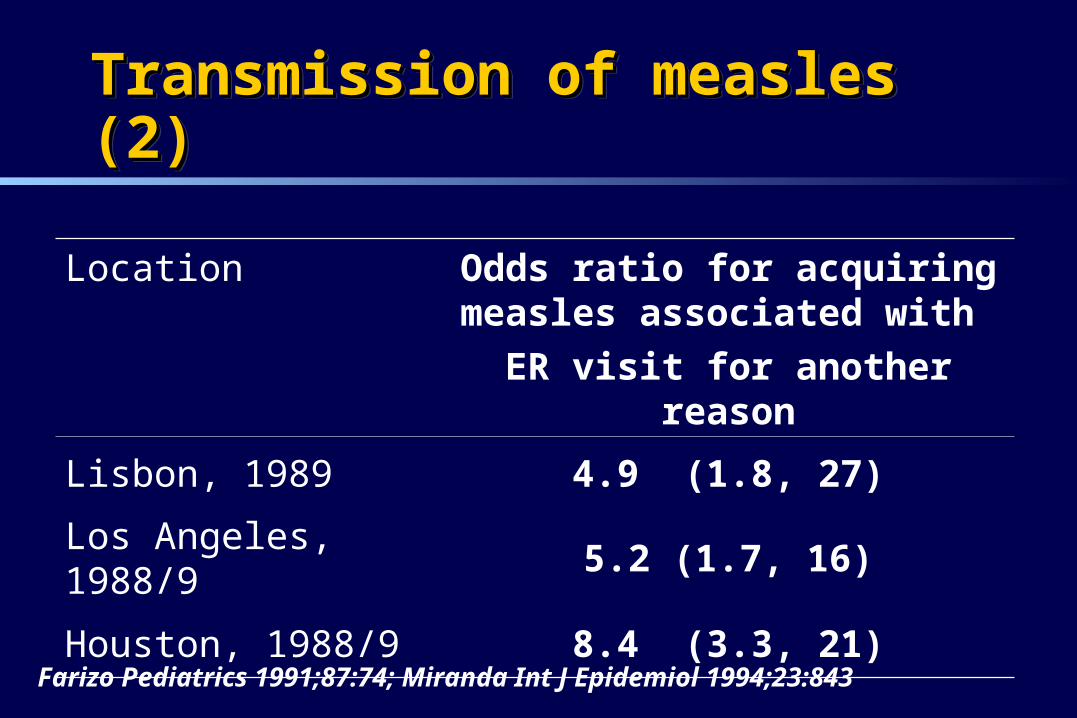
Transmission of measles (2)Transmission of measles (2)Transmission of measles (2)Transmission of measles (2)
Location Odds ratio for acquiring measles associated with
ER visit for another reason
Lisbon, 1989 4.9 (1.8, 27)
Los Angeles, 1988/9 5.2 (1.7, 16)
Houston, 1988/9 8.4 (3.3, 21)
Farizo Pediatrics 1991;87:74; Miranda Int J Epidemiol 1994;23:843
Ventilation for protection Ventilation for protection Ventilation for protection Ventilation for protection
Meet AIHA guidelines– http://www.aia.org/publications/guidelinesabout.asp
Specific areas of concern– ER waiting room– Areas where bronchoscopy performed– Areas where unrecognized, infected patients are
most likely
Meet AIHA guidelines– http://www.aia.org/publications/guidelinesabout.asp
Specific areas of concern– ER waiting room– Areas where bronchoscopy performed– Areas where unrecognized, infected patients are
most likely
Airborne Isolation RoomsAirborne Isolation Rooms- Characteristics- CharacteristicsAirborne Isolation RoomsAirborne Isolation Rooms- Characteristics- Characteristics
Anteroom with sink Bathroom (off room) Negative pressure Requisite air changes (clean or filtered) AIR FLOW from staff to patient to exhaust
or filter
Be practical
Anteroom with sink Bathroom (off room) Negative pressure Requisite air changes (clean or filtered) AIR FLOW from staff to patient to exhaust
or filter
Be practical
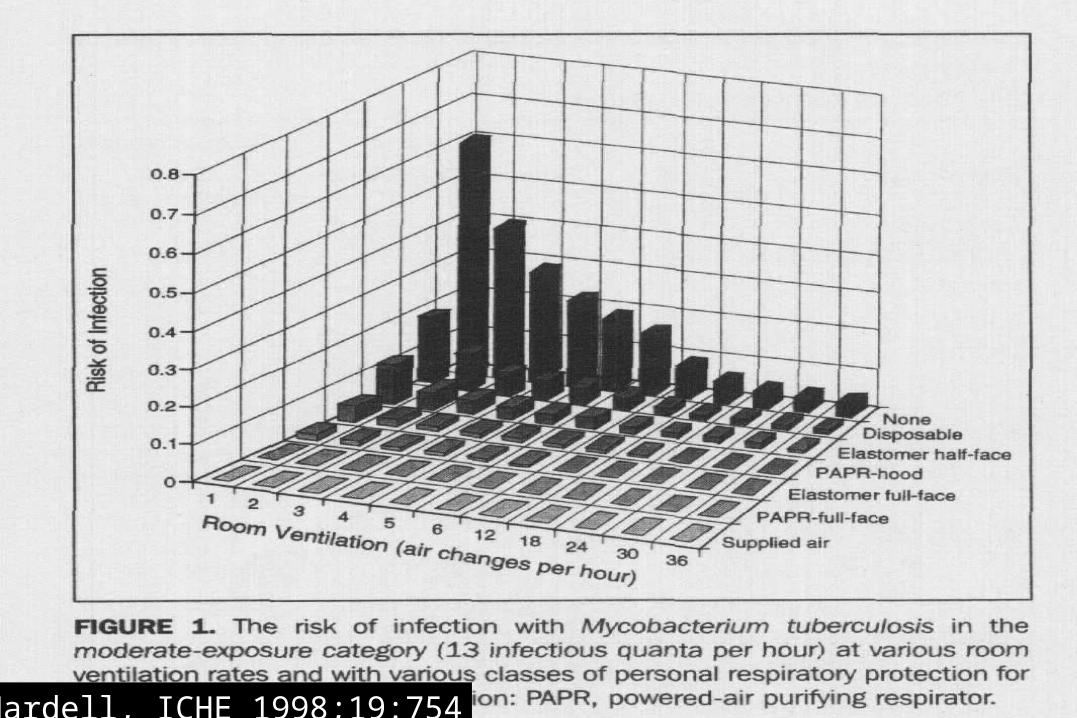
Nardell, ICHE 1998;19:754
Private roomsPrivate rooms
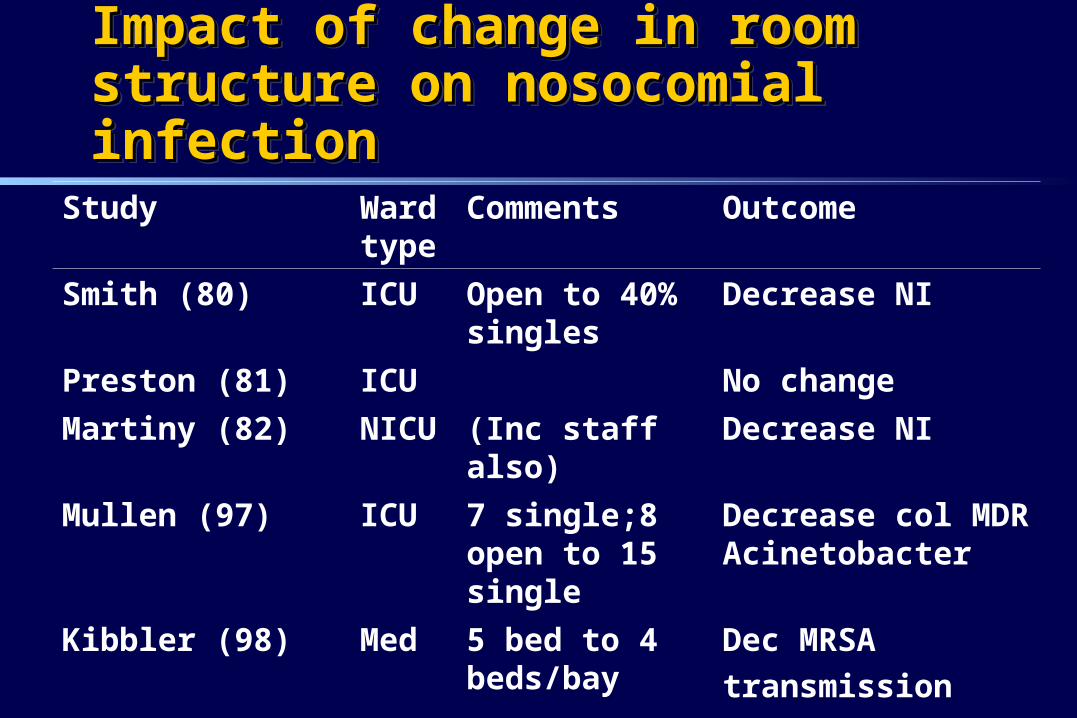
Impact of change in room structure on Impact of change in room structure on nosocomial infectionnosocomial infectionImpact of change in room structure on Impact of change in room structure on nosocomial infectionnosocomial infection
Study Ward type
Comments Outcome
Smith (80) ICU Open to 40% singles
Decrease NI
Preston (81) ICU No change
Martiny (82) NICU (Inc staff also) Decrease NI
Mullen (97) ICU 7 single;8 open to 15 single
Decrease col MDR Acinetobacter
Kibbler (98) Med 5 bed to 4 beds/bay
Dec MRSA
transmission
Ben-Abraham (02) PICU Decrease NI
P
P
P
ATM
OutpatientEntrance
Drug Store EmergencyEntrance
Security EmergencyRegistration
Emergency
Nurse
Admitting
Vending
Machines
Waiting Room
Trauma
Room
Room 1
Room 2
Room 3
Room 4
Room 5
Room 6
Stock
Room
Room 7
Room 8
Room 9
Eye Room
Fracture
Room
Soiled
Linen
Shower
W CW C
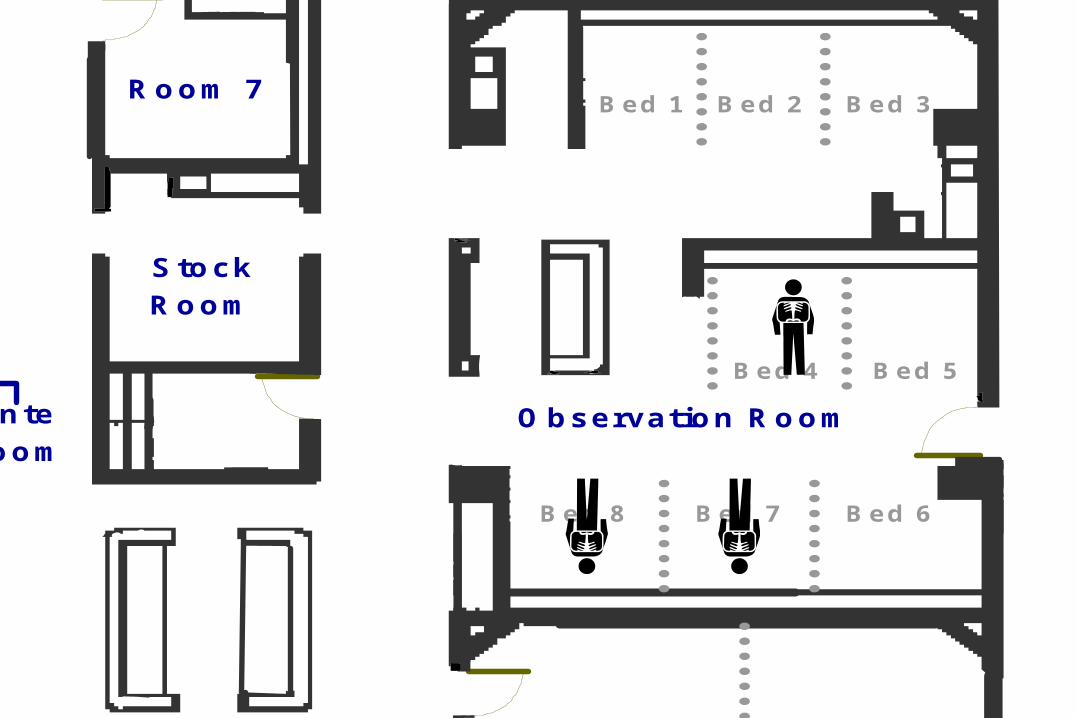
Observation Room
Nursing Station
Ante
Room
Bed 1
Bed 2
Bed 3
Bed 4
Bed 5
Bed 6
Bed 1 Bed 2 Bed 3
Bed 4 Bed 5
Bed 8 Bed 7 Bed 6
Bed 1
Bed 2Bed3
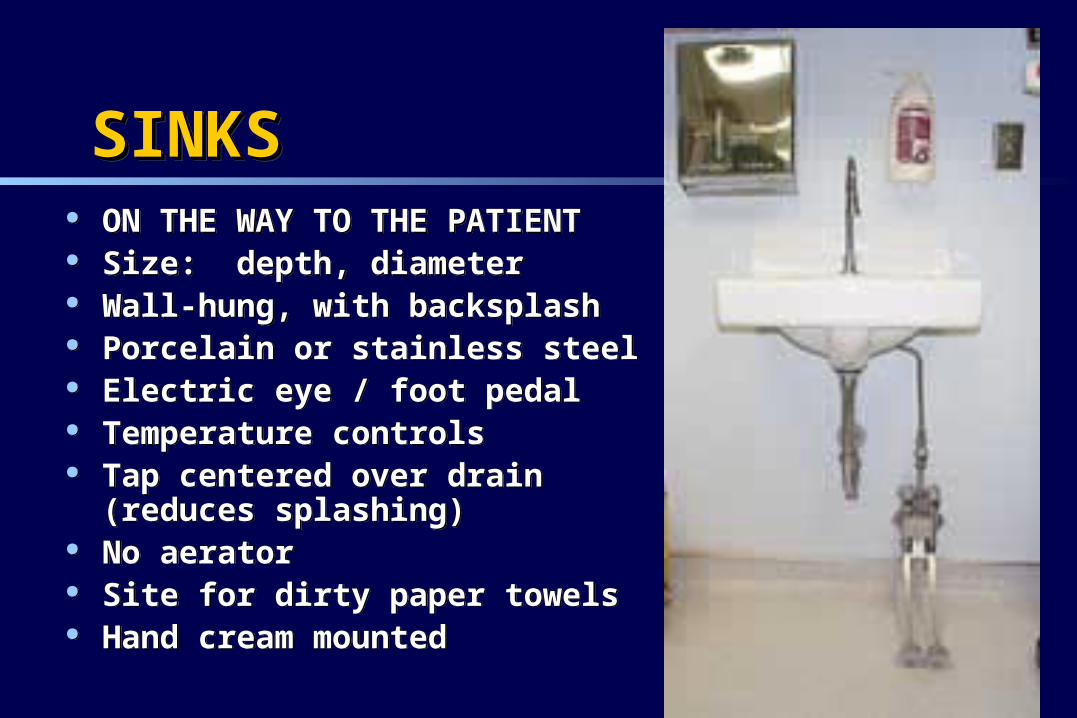
SINKSSINKSSINKSSINKS ON THE WAY TO THE PATIENT Size: depth, diameter Wall-hung, with backsplash Porcelain or stainless steel Electric eye / foot pedal Temperature controls Tap centered over drain (reduces
splashing) No aerator Site for dirty paper towels Hand cream mounted
ON THE WAY TO THE PATIENT Size: depth, diameter Wall-hung, with backsplash Porcelain or stainless steel Electric eye / foot pedal Temperature controls Tap centered over drain (reduces
splashing) No aerator Site for dirty paper towels Hand cream mounted
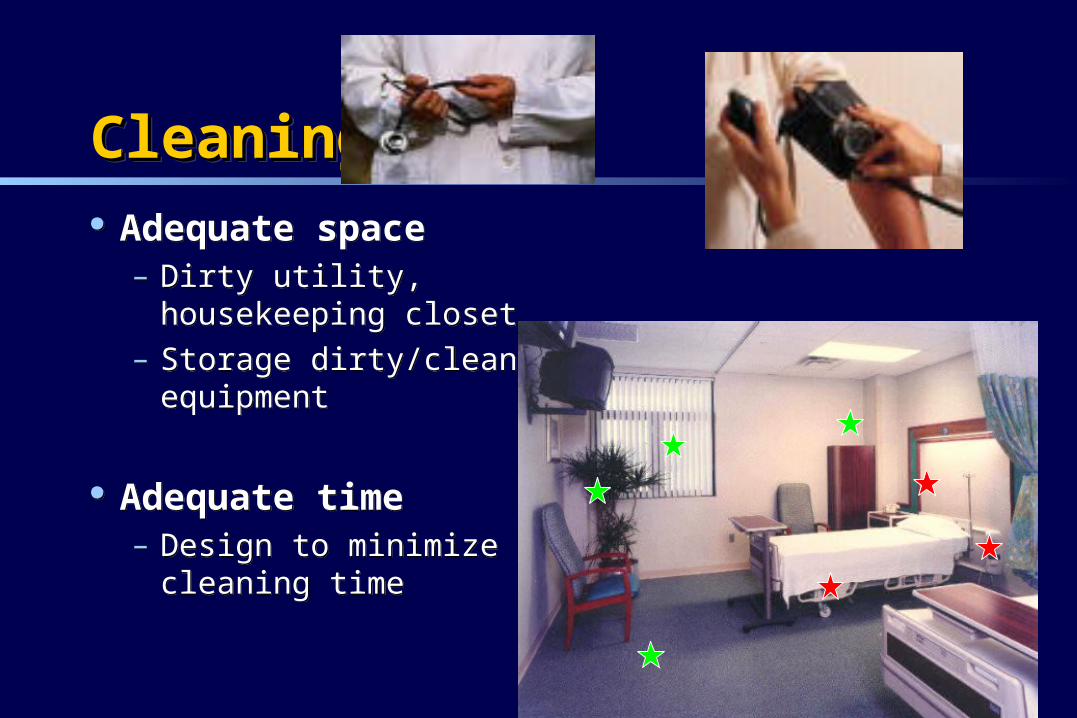
CleaningCleaningCleaningCleaning Adequate space
– Dirty utility, housekeeping closet
– Storage dirty/clean equipment
Adequate time– Design to minimize
cleaning time
Adequate space– Dirty utility,
housekeeping closet– Storage dirty/clean
equipment
Adequate time– Design to minimize
cleaning time
FundamentalsFundamentalsPrevention of transmissionPrevention of transmissionFundamentalsFundamentalsPrevention of transmissionPrevention of transmission
Hospital design Education Hand hygiene Routine practices and additional precautions
Hospital design Education Hand hygiene Routine practices and additional precautions
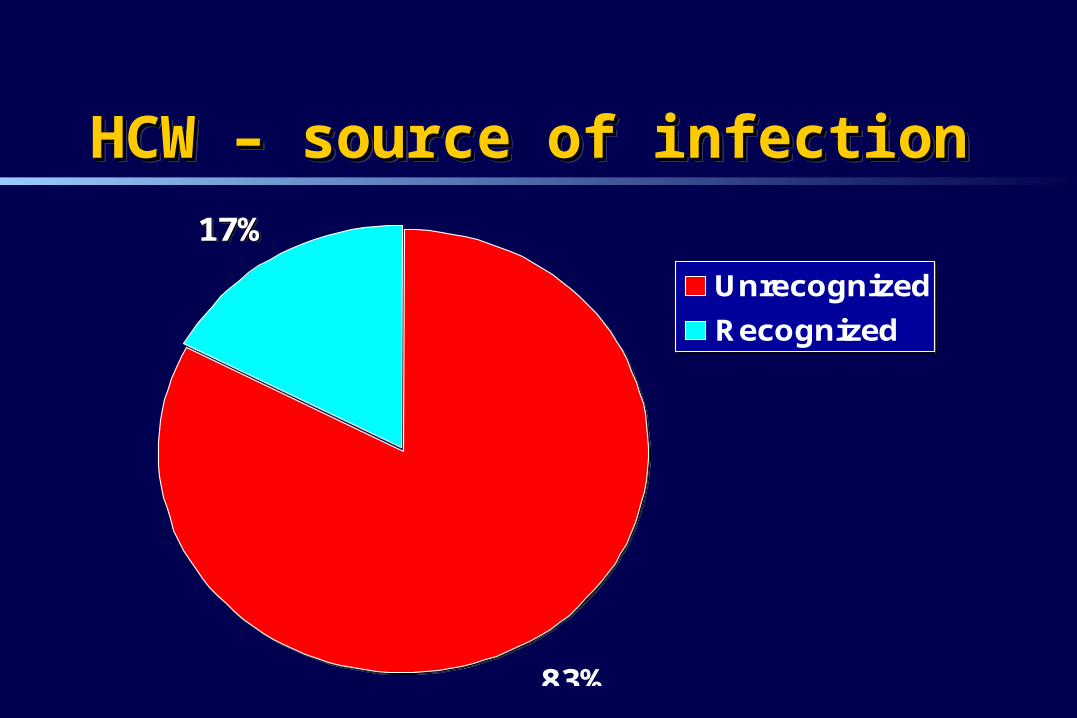
HCW – source of infectionHCW – source of infectionHCW – source of infectionHCW – source of infection17%
83%
Unrecognized
Recognized
17%
83%
Unrecognized
Recognized
Risk factors for TB in Canadian hospital Risk factors for TB in Canadian hospital laboratorieslaboratoriesRisk factors for TB in Canadian hospital Risk factors for TB in Canadian hospital laboratorieslaboratories
Menzies Am J Respir Crit Care Med 2002:67:599
Risk factor Odds ratio
Ratio of ventilation to that recommended (<0.5 compared to >=1)
1.3 (1.0-1.9)
Age of hospital wing (per 10 yrs) 1.5 (1.1-2.2)
% TB patients missed/delayed therapy
% TB patients admitted non-medical
% TB patients who died
2.0
2.0
2.5
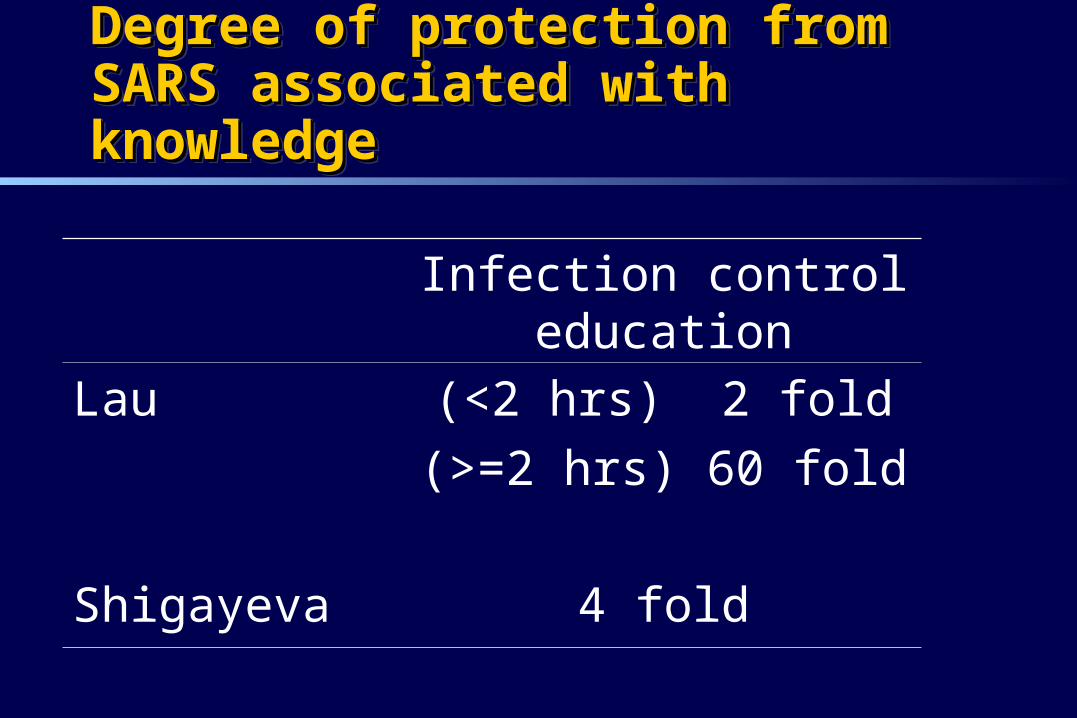
Degree of protection from SARS Degree of protection from SARS associated with knowledgeassociated with knowledgeDegree of protection from SARS Degree of protection from SARS associated with knowledgeassociated with knowledge
Infection control education
Lau (<2 hrs) 2 fold
(>=2 hrs) 60 fold
Shigayeva 4 fold
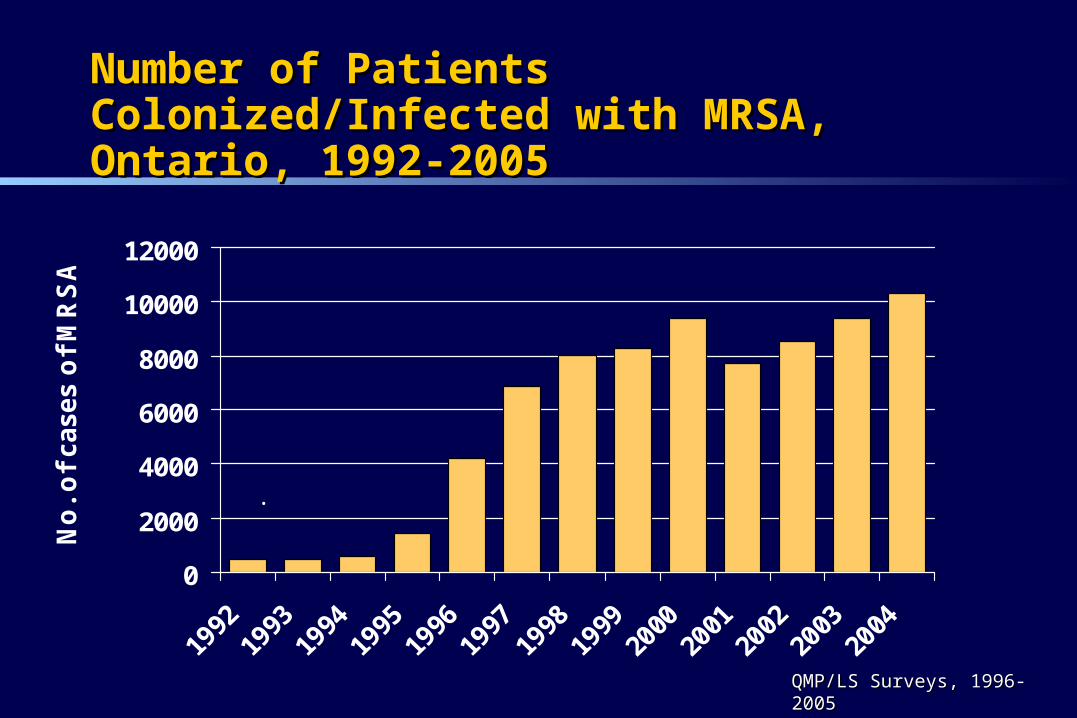
Number of Patients Colonized/Infected with MRSA, Number of Patients Colonized/Infected with MRSA, Ontario, 1992-2005Ontario, 1992-2005
0
2000
4000
6000
8000
10000
12000
No
. o
f cases o
f M
RS
A
.
QMP/LS Surveys, 1996-2005QMP/LS Surveys, 1996-2005
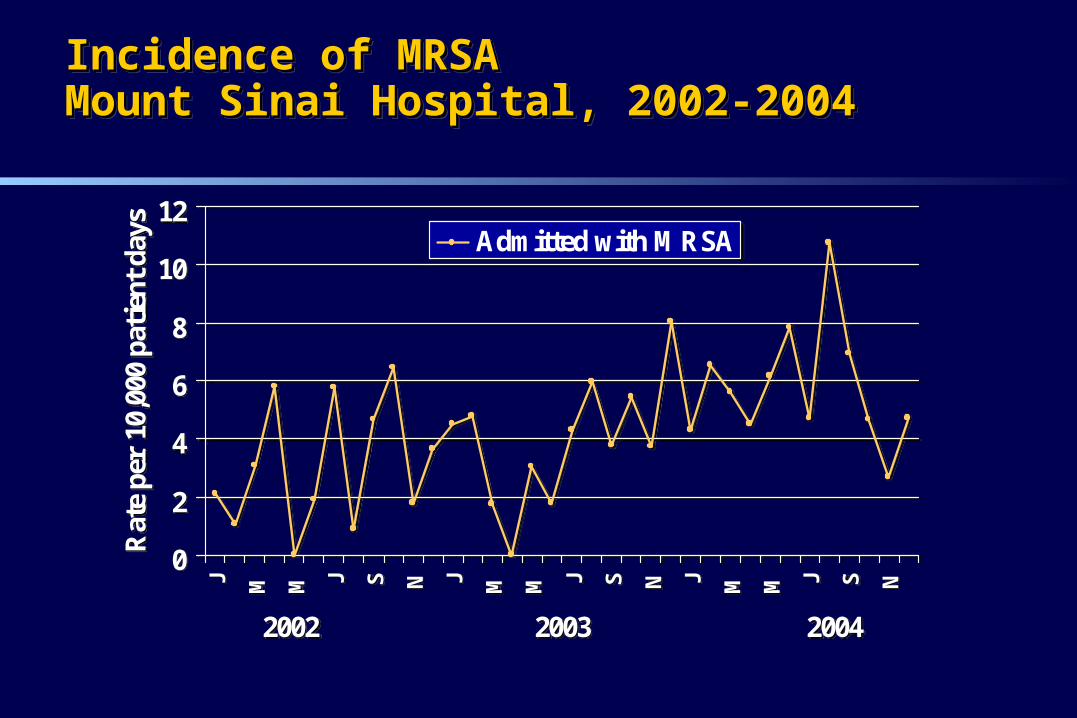
Incidence of MRSAIncidence of MRSAMount Sinai Hospital, 2002-2004Mount Sinai Hospital, 2002-2004Incidence of MRSAIncidence of MRSAMount Sinai Hospital, 2002-2004Mount Sinai Hospital, 2002-2004
0
2
4
6
8
10
12J M M J S N J M M J S N J M M J S N
2002 2003 2004
Rat
e pe
r 10
,000
pat
ient
day
s
Admitted with MRSA
0
2
4
6
8
10
12J M M J S N J M M J S N J M M J S N
2002 2003 2004
Rat
e pe
r 10
,000
pat
ient
day
s
Admitted with MRSA
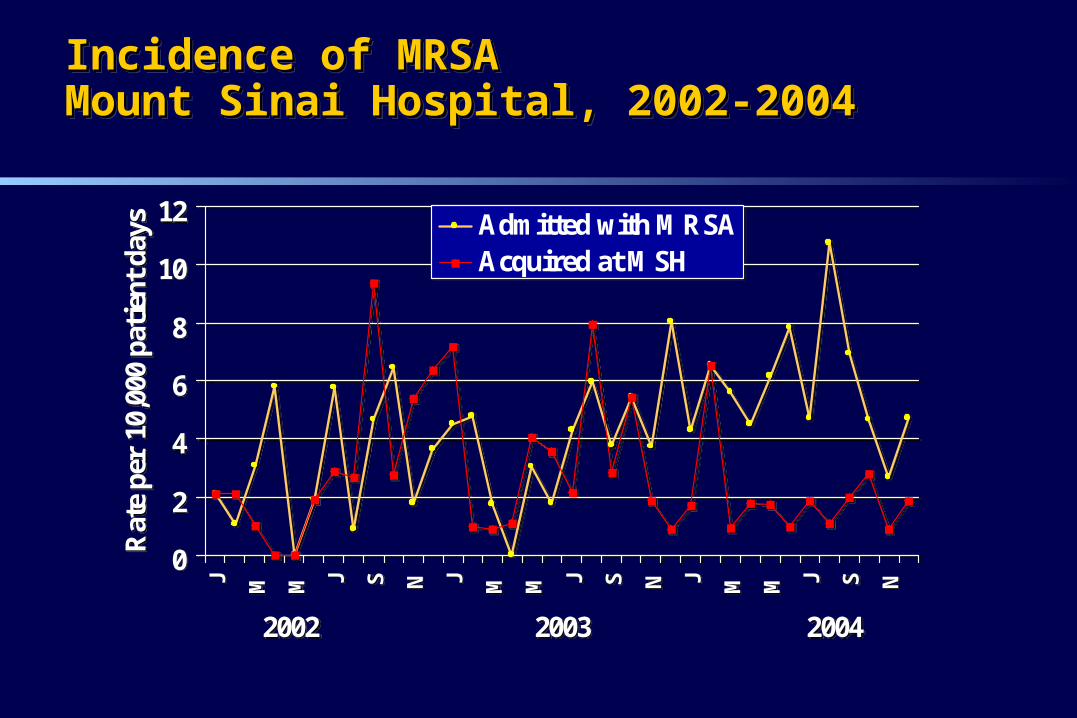
Incidence of MRSAIncidence of MRSAMount Sinai Hospital, 2002-2004Mount Sinai Hospital, 2002-2004Incidence of MRSAIncidence of MRSAMount Sinai Hospital, 2002-2004Mount Sinai Hospital, 2002-2004
0
2
4
6
8
10
12J M M J S N J M M J S N J M M J S N
2002 2003 2004
Rat
e pe
r 10
,000
pat
ient
day
s Admitted with MRSAAcquired at MSH
0
2
4
6
8
10
12J M M J S N J M M J S N J M M J S N
2002 2003 2004
Rat
e pe
r 10
,000
pat
ient
day
s Admitted with MRSAAcquired at MSH
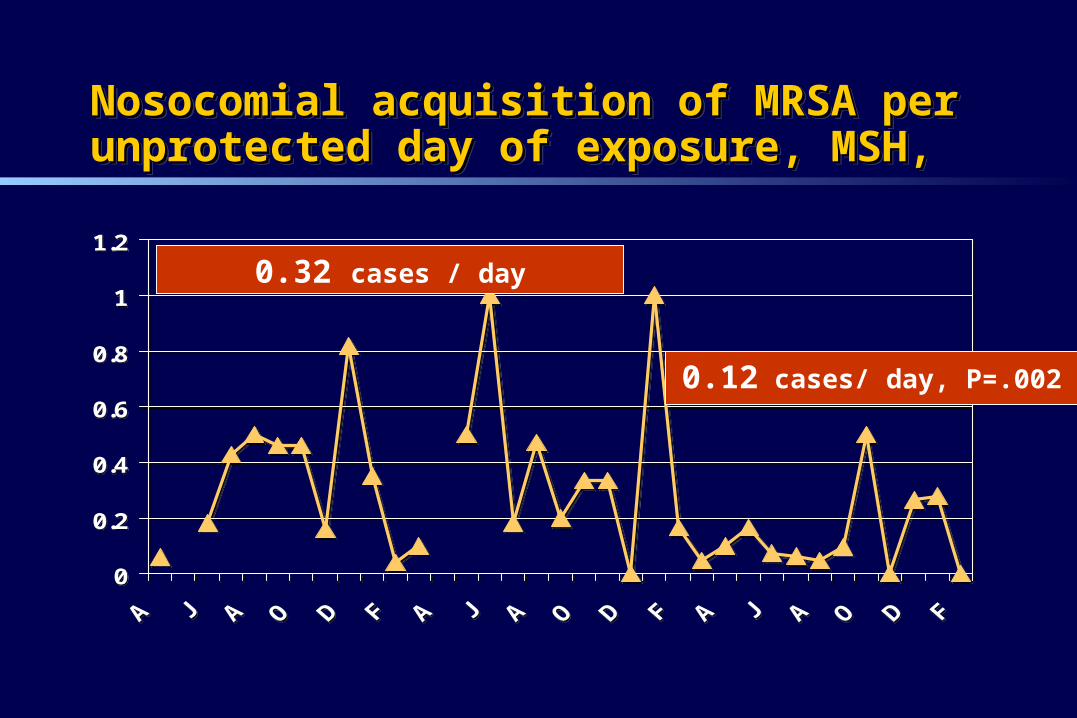
Nosocomial acquisition of MRSA per unprotected day Nosocomial acquisition of MRSA per unprotected day of exposure, MSH, of exposure, MSH, Nosocomial acquisition of MRSA per unprotected day Nosocomial acquisition of MRSA per unprotected day of exposure, MSH, of exposure, MSH,
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
0.32 cases / day
0.12 cases/ day, P=.002
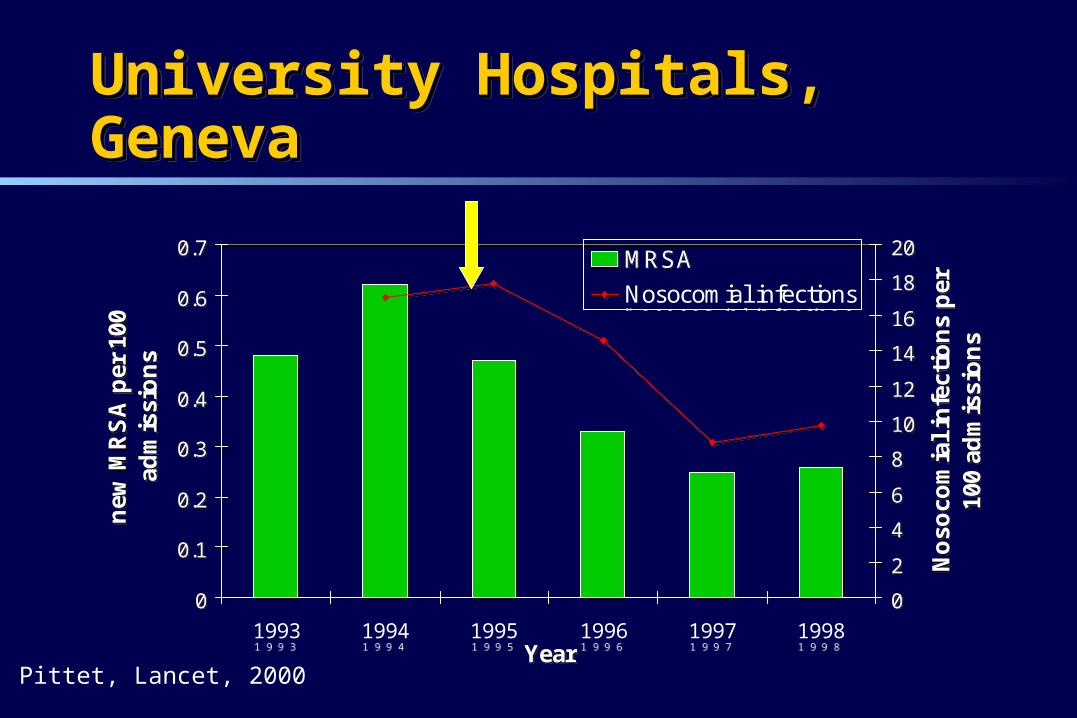
University Hospitals, GenevaUniversity Hospitals, GenevaUniversity Hospitals, GenevaUniversity Hospitals, Geneva
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
1993 1994 1995 1996 1997 1998Year
new
MR
SA
per
100
ad
mis
sio
ns
0
2
4
6
8
10
12
14
16
18
20
No
soco
mia
l in
fect
ion
s p
er
100
adm
issi
on
s
MRSA
Nosocomial infections
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
1993 1994 1995 1996 1997 1998Year
new
MR
SA
per
100
ad
mis
sio
ns
0
2
4
6
8
10
12
14
16
18
20
No
soco
mia
l in
fect
ion
s p
er
100
adm
issi
on
s
MRSA
Nosocomial infections
Pittet, Lancet, 2000
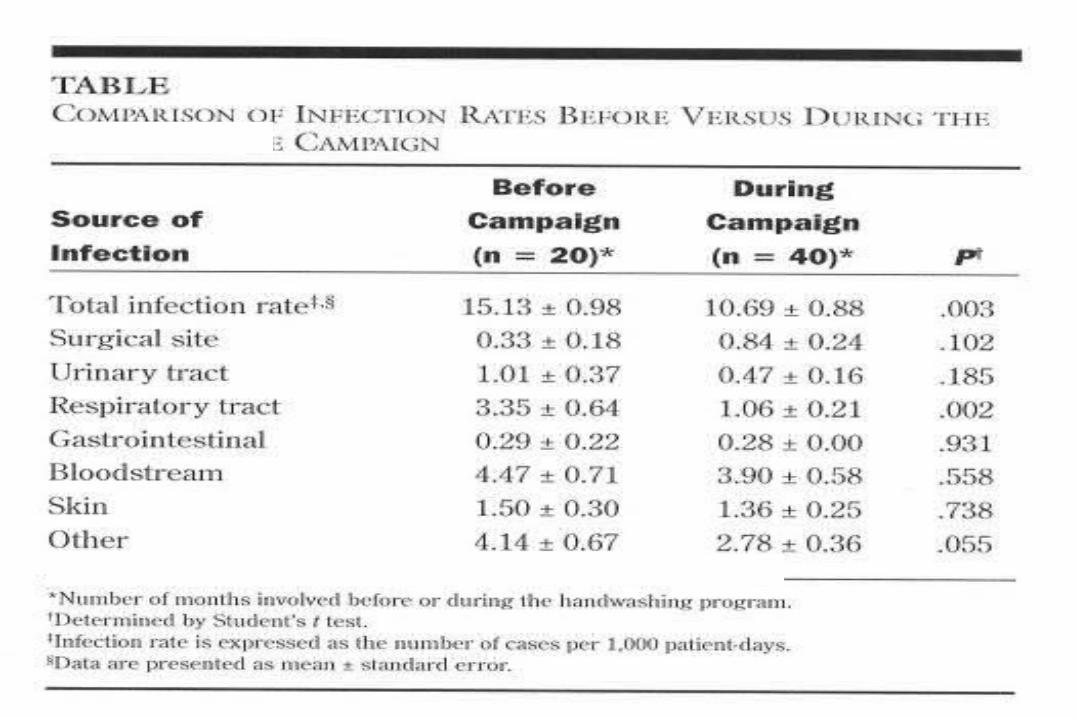
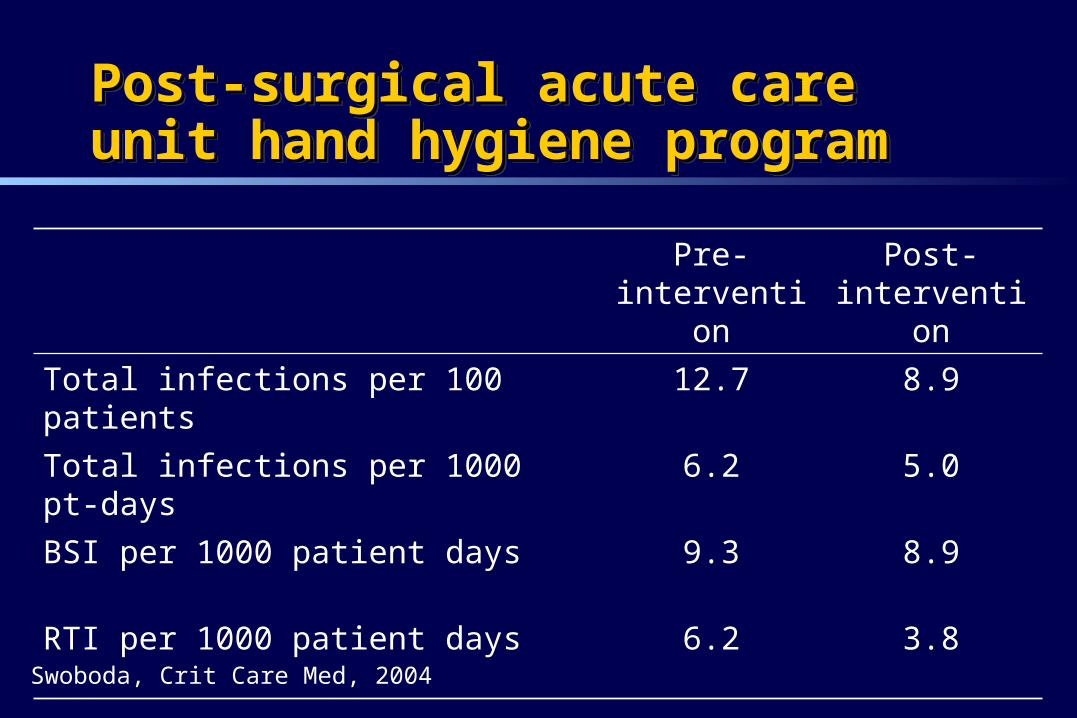
Post-surgical acute care unit hand hygiene Post-surgical acute care unit hand hygiene programprogramPost-surgical acute care unit hand hygiene Post-surgical acute care unit hand hygiene programprogram
Pre-intervention
Post-intervention
Total infections per 100 patients 12.7 8.9
Total infections per 1000 pt-days 6.2 5.0
BSI per 1000 patient days 9.3 8.9
RTI per 1000 patient days 6.2 3.8
Swoboda, Crit Care Med, 2004
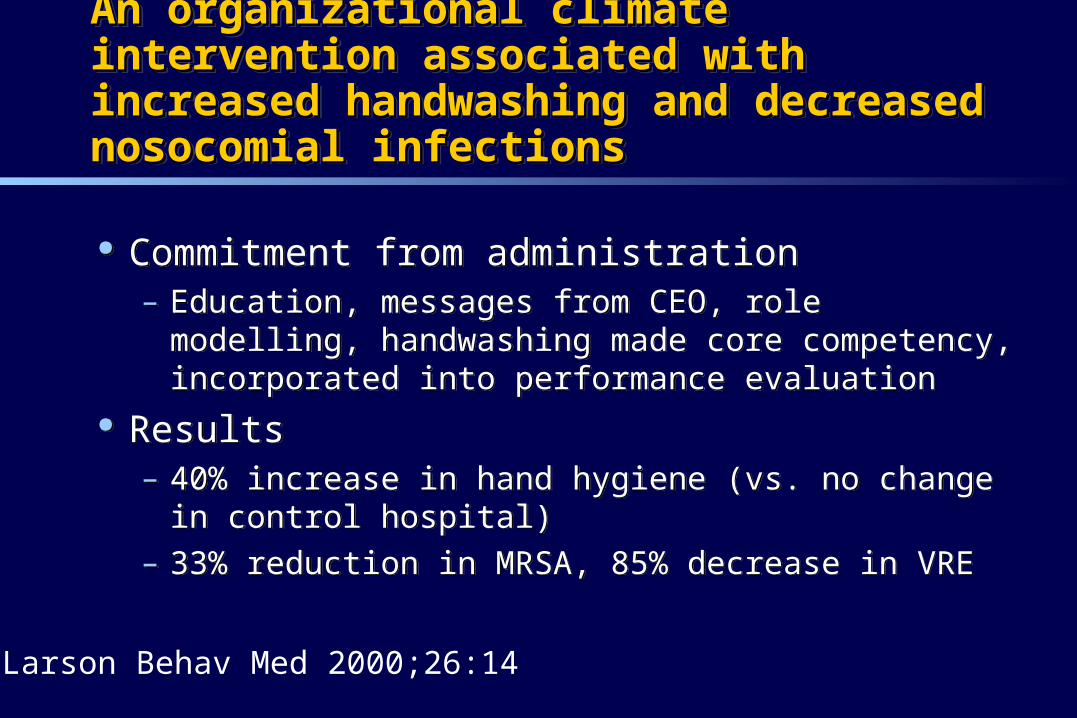
An organizational climate intervention associated An organizational climate intervention associated with increased handwashing and decreased with increased handwashing and decreased nosocomial infectionsnosocomial infections
An organizational climate intervention associated An organizational climate intervention associated with increased handwashing and decreased with increased handwashing and decreased nosocomial infectionsnosocomial infections
Commitment from administration– Education, messages from CEO, role modelling,
handwashing made core competency, incorporated into performance evaluation
Results– 40% increase in hand hygiene (vs. no change in control
hospital)– 33% reduction in MRSA, 85% decrease in VRE
Commitment from administration– Education, messages from CEO, role modelling,
handwashing made core competency, incorporated into performance evaluation
Results– 40% increase in hand hygiene (vs. no change in control
hospital)– 33% reduction in MRSA, 85% decrease in VRE
Larson Behav Med 2000;26:14
FundamentalsFundamentalsPrevention of transmissionPrevention of transmissionFundamentalsFundamentalsPrevention of transmissionPrevention of transmission
Hospital design Education Hand hygiene Routine practices and additional precautions
Hospital design Education Hand hygiene Routine practices and additional precautions
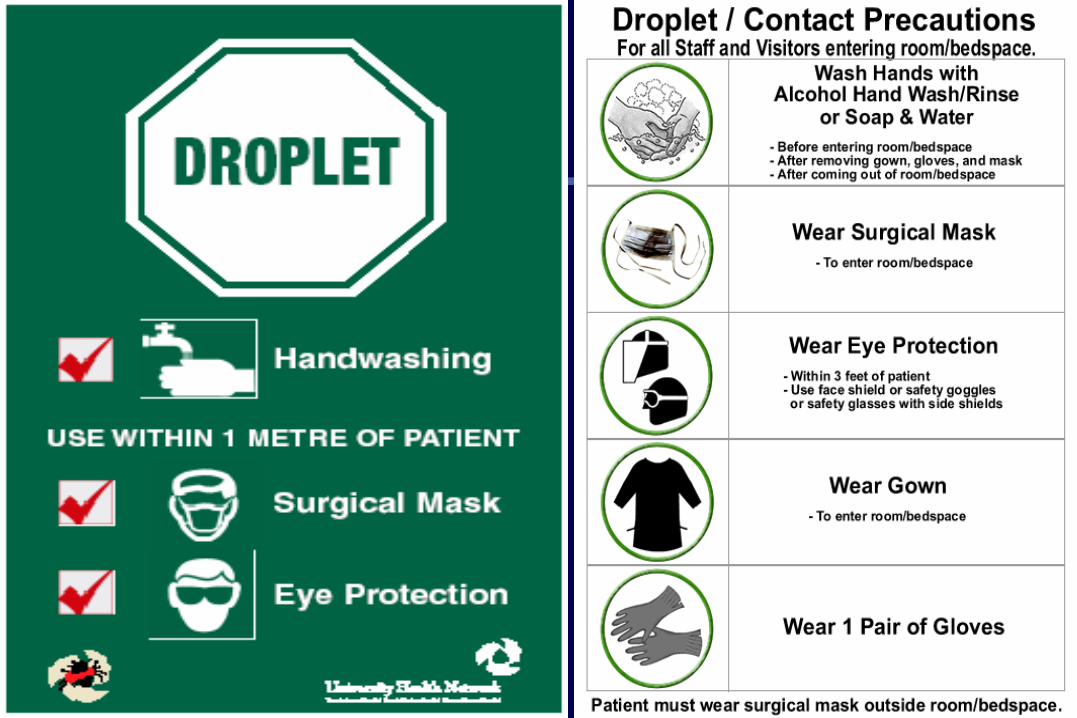
Routine practicesRoutine practices(US=Standard Precautions)(US=Standard Precautions)Routine practicesRoutine practices(US=Standard Precautions)(US=Standard Precautions)
Wear barriers to prevent:– Contact with blood/body fluids/non-intact skin– Exposure to droplets– (Gloves, eye protection, gowns)
Clean environmental surfaces/equipment
Wear barriers to prevent:– Contact with blood/body fluids/non-intact skin– Exposure to droplets– (Gloves, eye protection, gowns)
Clean environmental surfaces/equipment
When do you need additional precautions?When do you need additional precautions?When do you need additional precautions?When do you need additional precautions?
Diseases spread by the airborne route
Diseases spread by droplets
Diseases spread by contact with skin/the environment
Diseases spread by the airborne route
Diseases spread by droplets
Diseases spread by contact with skin/the environment
UNANSWERED QUESTION: IF HAND HYGIENE AND HOUSEKEEPING
ARE “ADEQUATE”, ARE ADDITIONALPRECAUTIONS NEEDED?
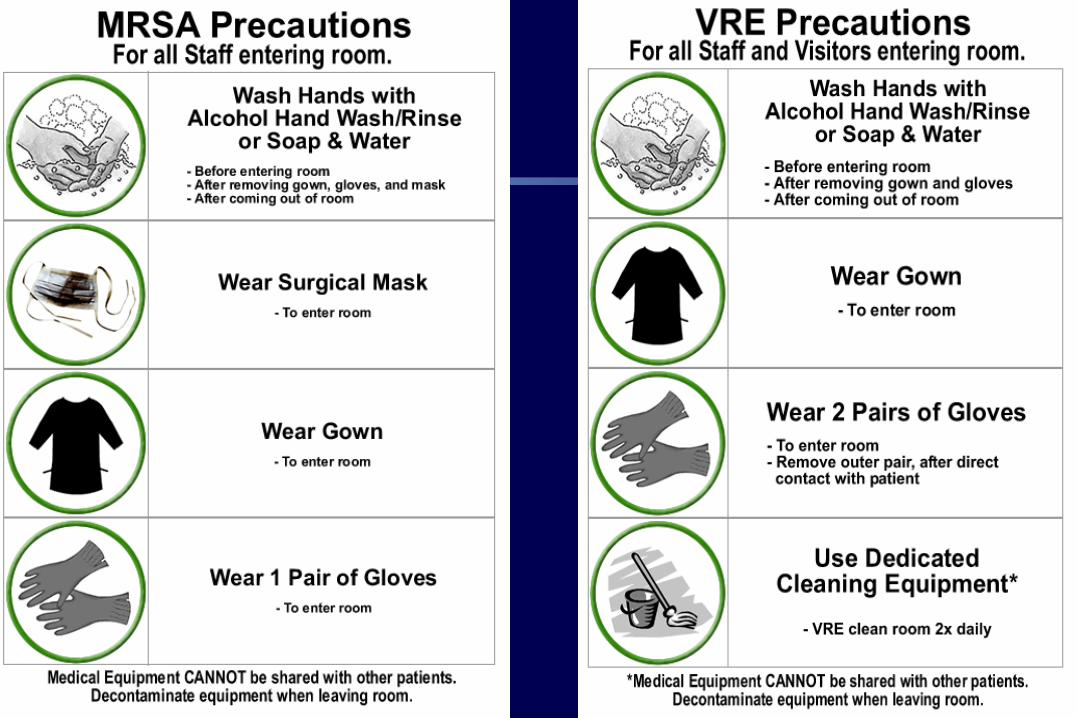
Additional precautionsAdditional precautionsAdditional precautionsAdditional precautions
MSH UHN
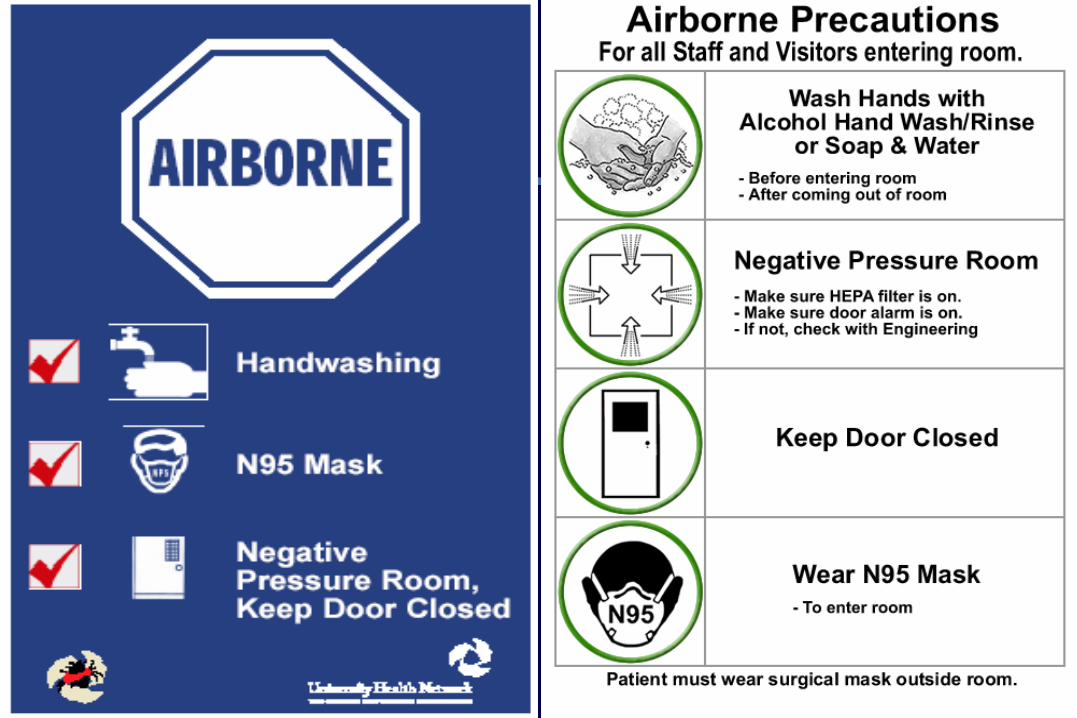
Airborne
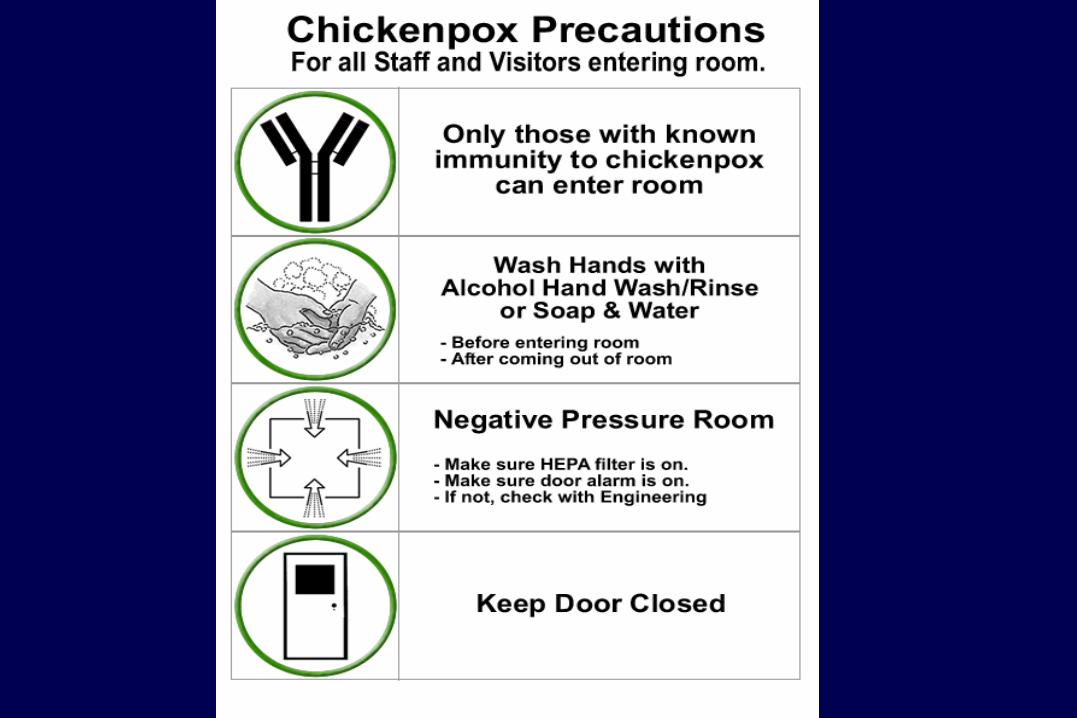
Chickenpox
Airborne
Droplet/contact Droplet
Contact
MRSA
VRE/C diff
Contact
Full (droplet/contact/Air)
Pulmonary tuberculosis (TB)• Varicella/Chicken Pox • Disseminated Shingles/Zoster• Measles
Pulmonary tuberculosis (TB)• Varicella/Chicken Pox • Disseminated Shingles/Zoster• Measles
Infections spread by the airborne routeInfections spread by the airborne routeInfections spread by the airborne routeInfections spread by the airborne route
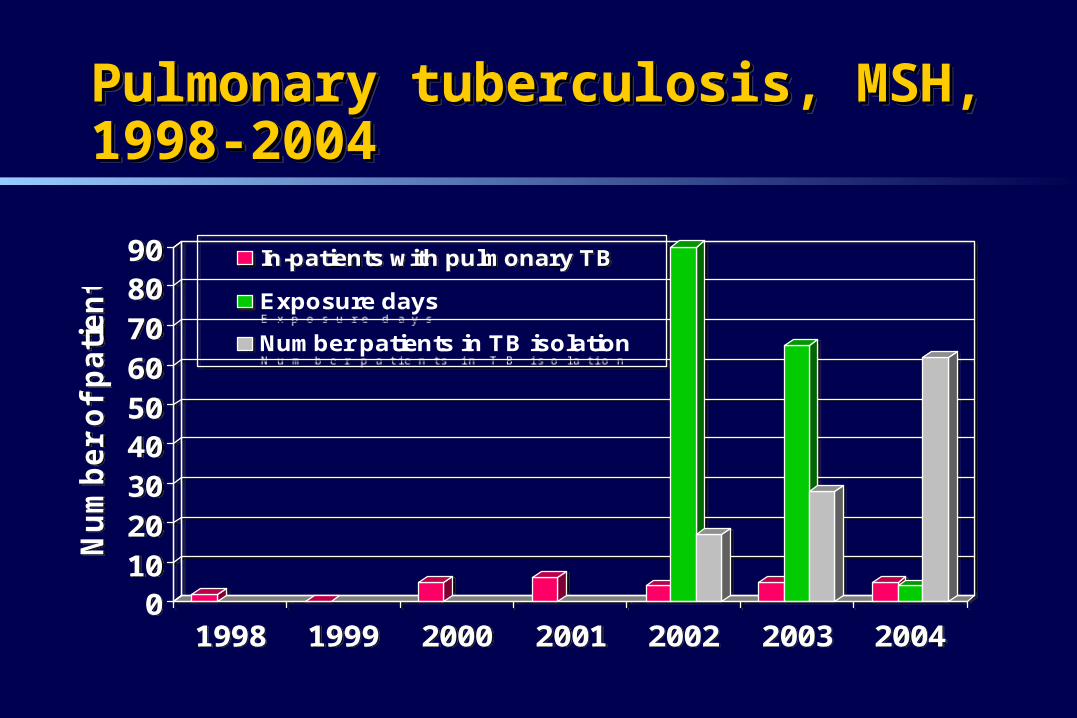
Pulmonary tuberculosis, MSH, 1998-2004Pulmonary tuberculosis, MSH, 1998-2004Pulmonary tuberculosis, MSH, 1998-2004Pulmonary tuberculosis, MSH, 1998-2004
0102030405060708090
Nu
mb
er
of
pa
tie
nts
1998 1999 2000 2001 2002 2003 2004
In-patients with pulmonary TB
Exposure days
Number patients in TB isolation
0102030405060708090
Nu
mb
er
of
pa
tie
nts
1998 1999 2000 2001 2002 2003 2004
In-patients with pulmonary TB
Exposure days
Number patients in TB isolation
Diseases spread by dropletsDiseases spread by dropletsDiseases spread by dropletsDiseases spread by droplets
Respiratory viruses Mycoplasma (primary atypical) pneumonia
N. meningitides Group A streptococci
Respiratory viruses Mycoplasma (primary atypical) pneumonia
N. meningitides Group A streptococci
Questions about droplet spreadQuestions about droplet spreadQuestions about droplet spreadQuestions about droplet spread
What is a droplet anyway?
What is contribution of droplet vs contact spread for these diseases?
How transmissible are they? How do patients acquire nosocomial respiratory viral diseases?
What is a droplet anyway?
What is contribution of droplet vs contact spread for these diseases?
How transmissible are they? How do patients acquire nosocomial respiratory viral diseases?
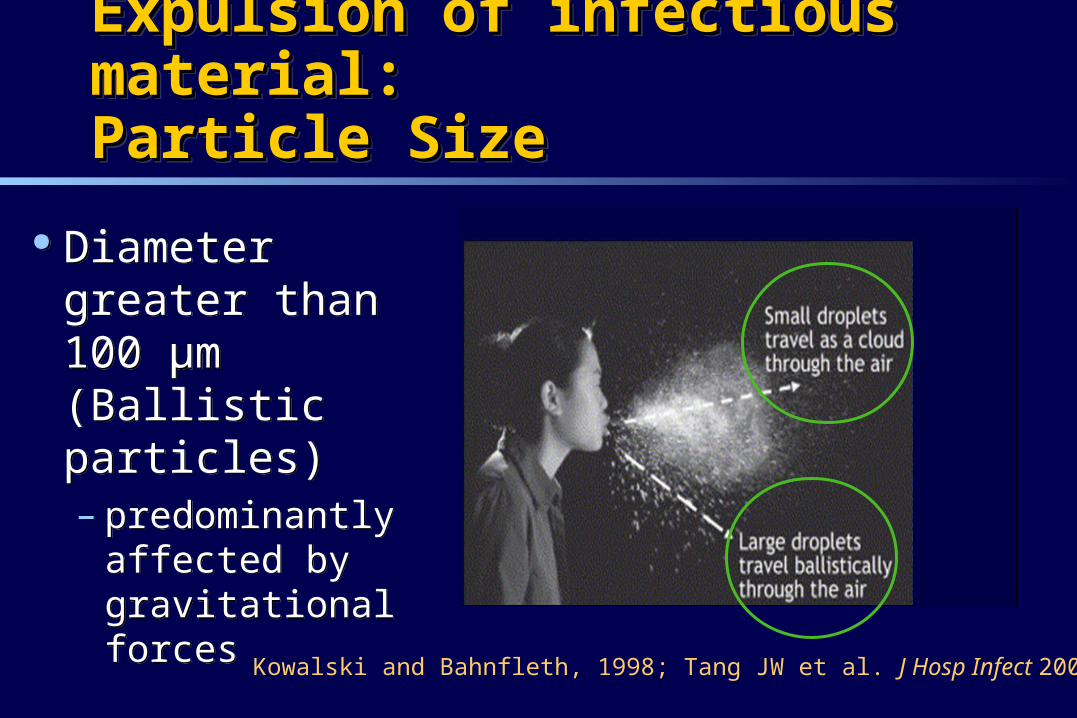
Expulsion of infectious material: Expulsion of infectious material: Particle SizeParticle SizeExpulsion of infectious material: Expulsion of infectious material: Particle SizeParticle Size
Diameter greater than 100 μm (Ballistic particles) – predominantly
affected by gravitational forces
Diameter greater than 100 μm (Ballistic particles) – predominantly
affected by gravitational forces
Kowalski and Bahnfleth, 1998; Tang JW et al. J Hosp Infect 2006
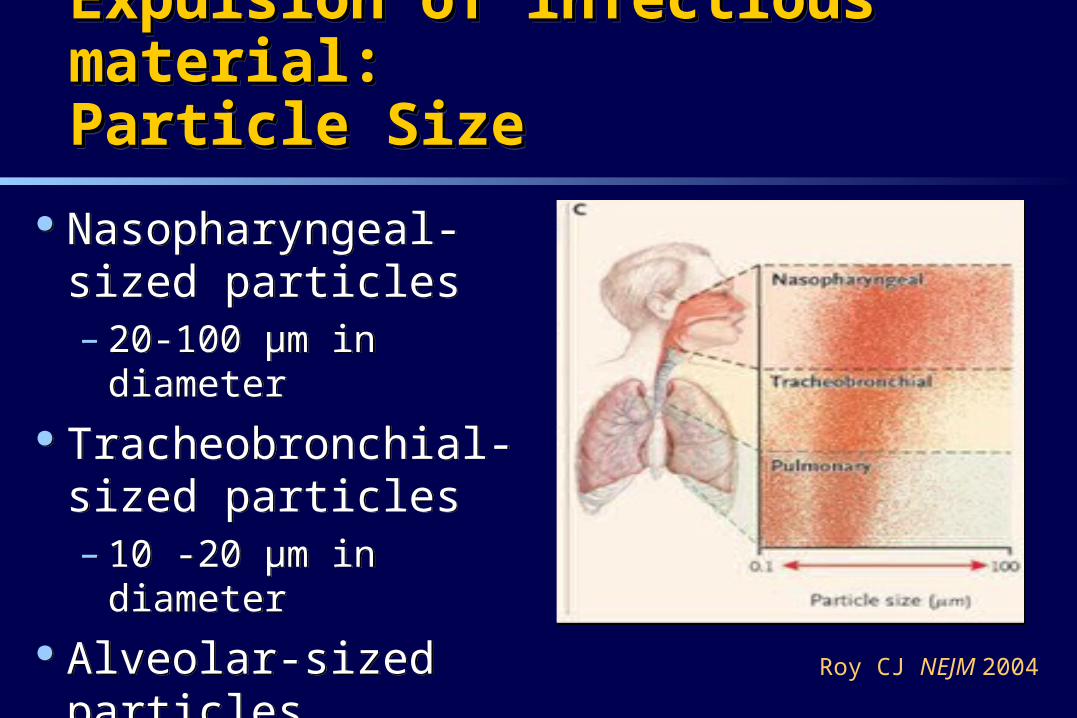
Nasopharyngeal-sized particles – 20-100 μm in diameter
Tracheobronchial-sized particles – 10 -20 μm in diameter
Alveolar-sized particles (pulmonary) – ≤10 μm in diameter
Nasopharyngeal-sized particles – 20-100 μm in diameter
Tracheobronchial-sized particles – 10 -20 μm in diameter
Alveolar-sized particles (pulmonary) – ≤10 μm in diameter Roy CJ NEJM 2004
Expulsion of infectious material: Expulsion of infectious material: Particle SizeParticle SizeExpulsion of infectious material: Expulsion of infectious material: Particle SizeParticle Size
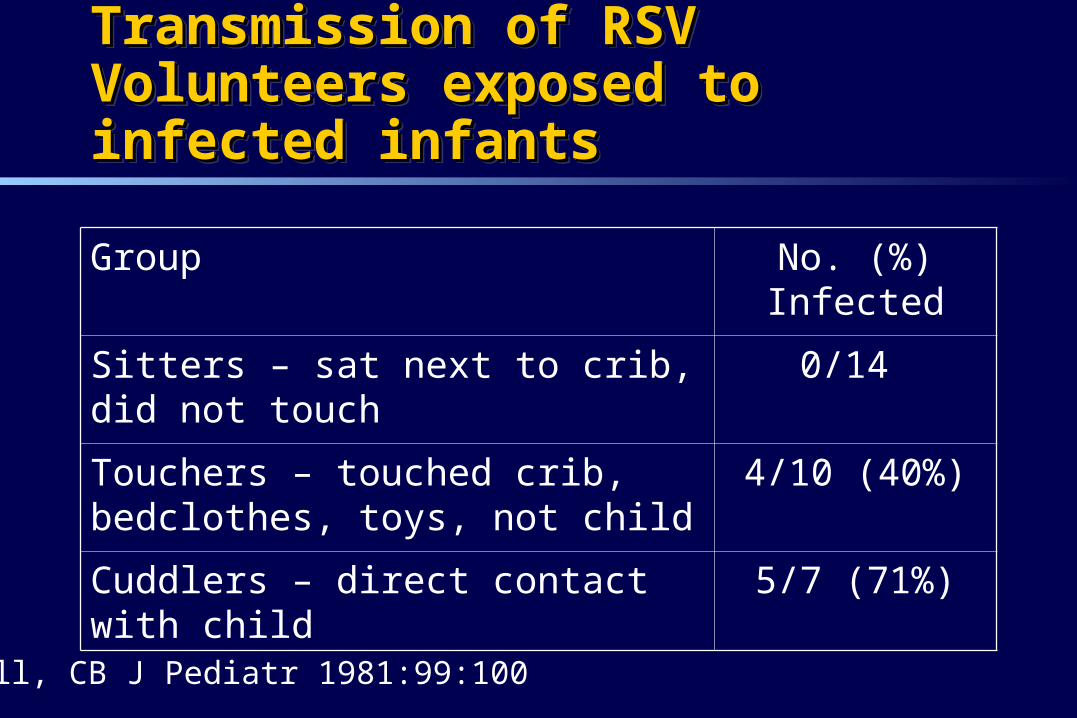
Transmission of RSVTransmission of RSVVolunteers exposed to infected infantsVolunteers exposed to infected infantsTransmission of RSVTransmission of RSVVolunteers exposed to infected infantsVolunteers exposed to infected infants
Group No. (%) Infected
Sitters – sat next to crib, did not touch
0/14
Touchers – touched crib, bedclothes, toys, not child
4/10 (40%)
Cuddlers – direct contact with child 5/7 (71%)
Hall, CB J Pediatr 1981:99:100
RSVRSVRSVRSV Hall et al. (1986)
– Goggles prevent transmission of RSV to staff
Leclair et al (1987)– Compliance with gown and gloves reduces
transmission of RSV in hospital
Hall et al. (1986)– Goggles prevent transmission of RSV to staff
Leclair et al (1987)– Compliance with gown and gloves reduces
transmission of RSV in hospital
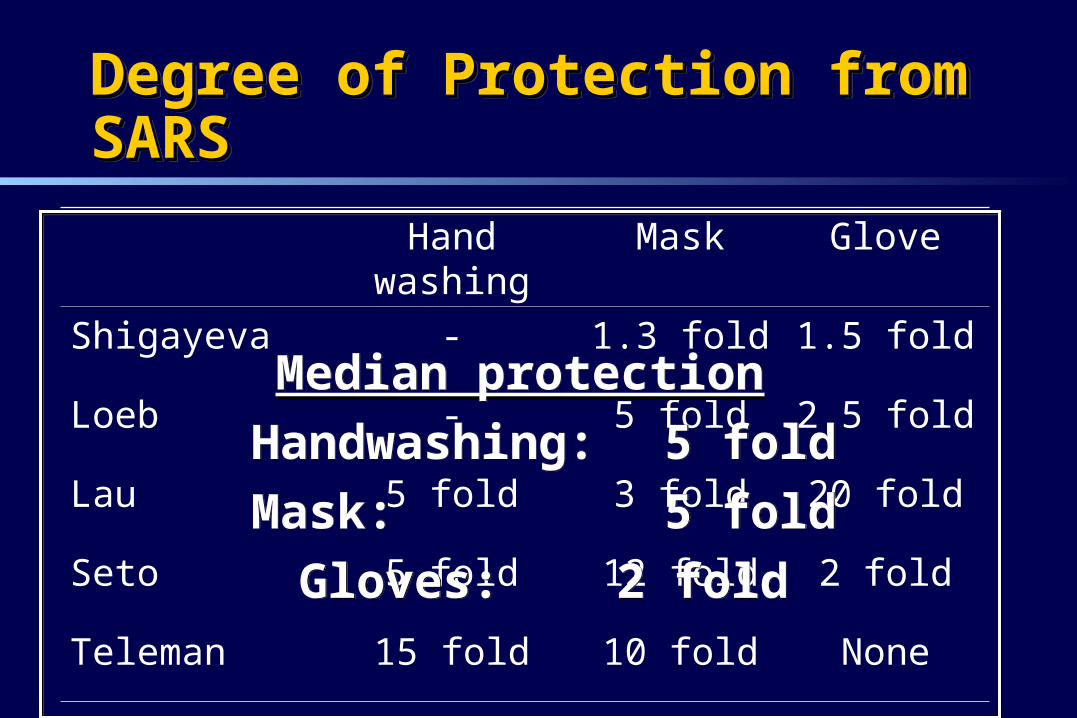
Degree of Protection from SARSDegree of Protection from SARSDegree of Protection from SARSDegree of Protection from SARS
Hand washing
Mask Glove
Shigayeva - 1.3 fold 1.5 fold
Loeb - 5 fold 2.5 fold
Lau 5 fold 3 fold 20 fold
Seto 5 fold 12 fold 2 fold
Teleman 15 fold 10 fold None
Median protection
Handwashing: 5 fold
Mask: 5 fold
Gloves: 2 fold
Median protection
Handwashing: 5 fold
Mask: 5 fold
Gloves: 2 fold
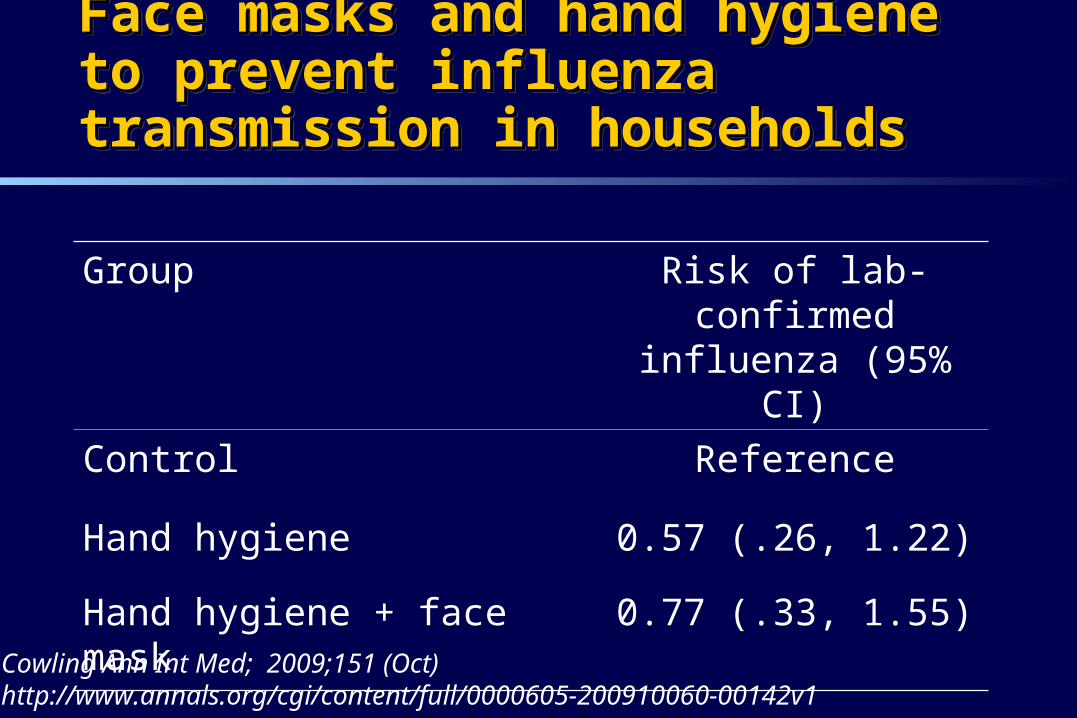
Face masks and hand hygiene to prevent Face masks and hand hygiene to prevent influenza transmission in householdsinfluenza transmission in householdsFace masks and hand hygiene to prevent Face masks and hand hygiene to prevent influenza transmission in householdsinfluenza transmission in households
Group Risk of lab-confirmed influenza (95% CI)
Control Reference
Hand hygiene 0.57 (.26, 1.22)
Hand hygiene + face mask 0.77 (.33, 1.55)
Cowling Ann Int Med; 2009;151 (Oct)http://www.annals.org/cgi/content/full/0000605-200910060-00142v1
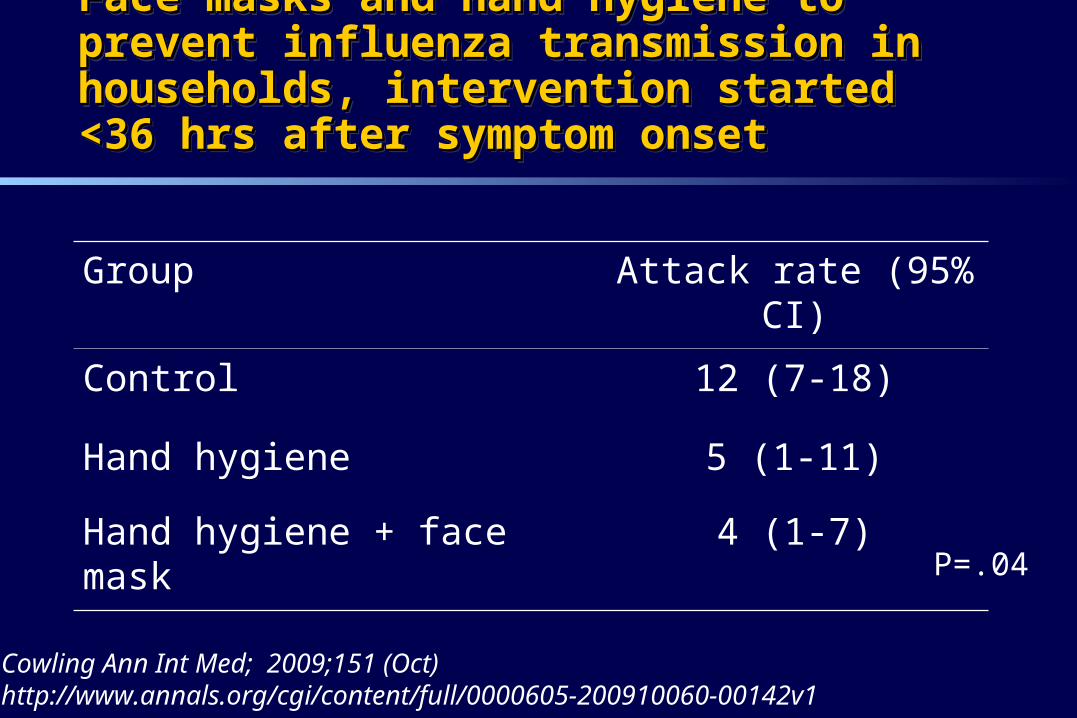
Face masks and hand hygiene to prevent influenza Face masks and hand hygiene to prevent influenza transmission in households, intervention started <36 transmission in households, intervention started <36 hrs after symptom onsethrs after symptom onset
Face masks and hand hygiene to prevent influenza Face masks and hand hygiene to prevent influenza transmission in households, intervention started <36 transmission in households, intervention started <36 hrs after symptom onsethrs after symptom onset
Group Attack rate (95% CI)
Control 12 (7-18)
Hand hygiene 5 (1-11)
Hand hygiene + face mask 4 (1-7)
Cowling Ann Int Med; 2009;151 (Oct)http://www.annals.org/cgi/content/full/0000605-200910060-00142v1
P=.04
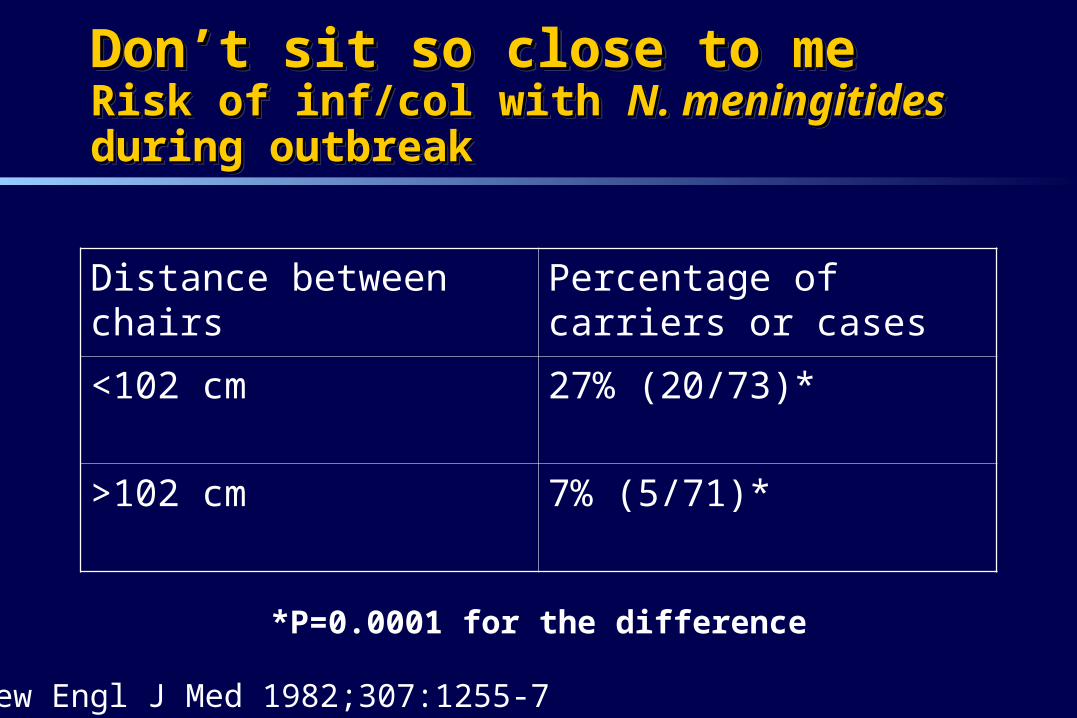
Don’t sit so close to meDon’t sit so close to meRisk of inf/col with Risk of inf/col with N. meningitidesN. meningitides during outbreak during outbreakDon’t sit so close to meDon’t sit so close to meRisk of inf/col with Risk of inf/col with N. meningitidesN. meningitides during outbreak during outbreak
Distance between chairs Percentage of carriers or cases
<102 cm 27% (20/73)*
>102 cm 7% (5/71)*
*P=0.0001 for the difference
New Engl J Med 1982;307:1255-7
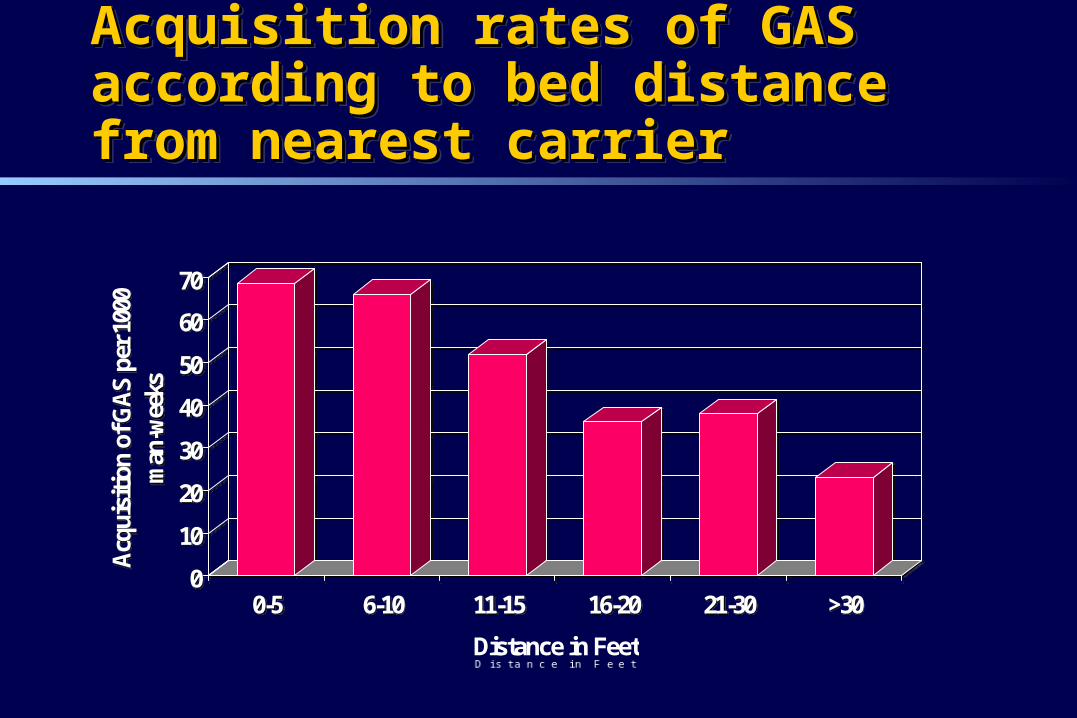
Acquisition rates of GAS according to bed Acquisition rates of GAS according to bed distance from nearest carrierdistance from nearest carrierAcquisition rates of GAS according to bed Acquisition rates of GAS according to bed distance from nearest carrierdistance from nearest carrier
0
10
20
30
40
50
60
70
Acq
uisi
tion
of G
AS
per 1
000
man
-wee
ks
0-5 6-10 11-15 16-20 21-30 >30
Distance in Feet
0
10
20
30
40
50
60
70
Acq
uisi
tion
of G
AS
per 1
000
man
-wee
ks
0-5 6-10 11-15 16-20 21-30 >30
Distance in Feet
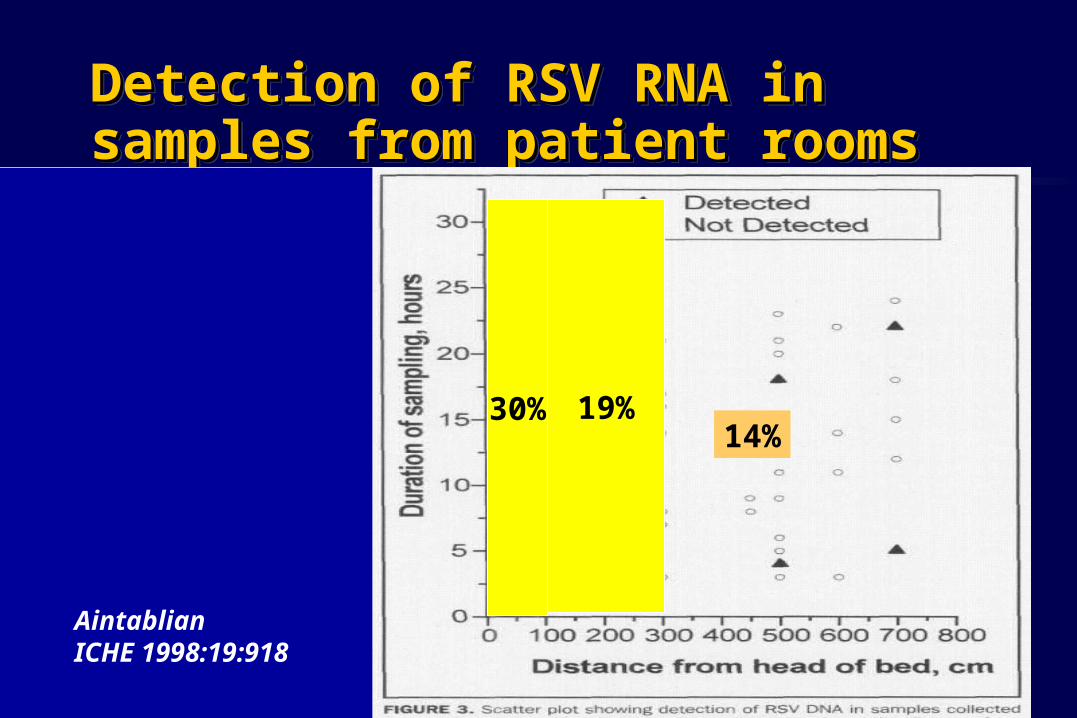
Detection of RSV RNA in samples from Detection of RSV RNA in samples from patient roomspatient roomsDetection of RSV RNA in samples from Detection of RSV RNA in samples from patient roomspatient rooms
AintablianICHE 1998:19:918
30% 19%14%
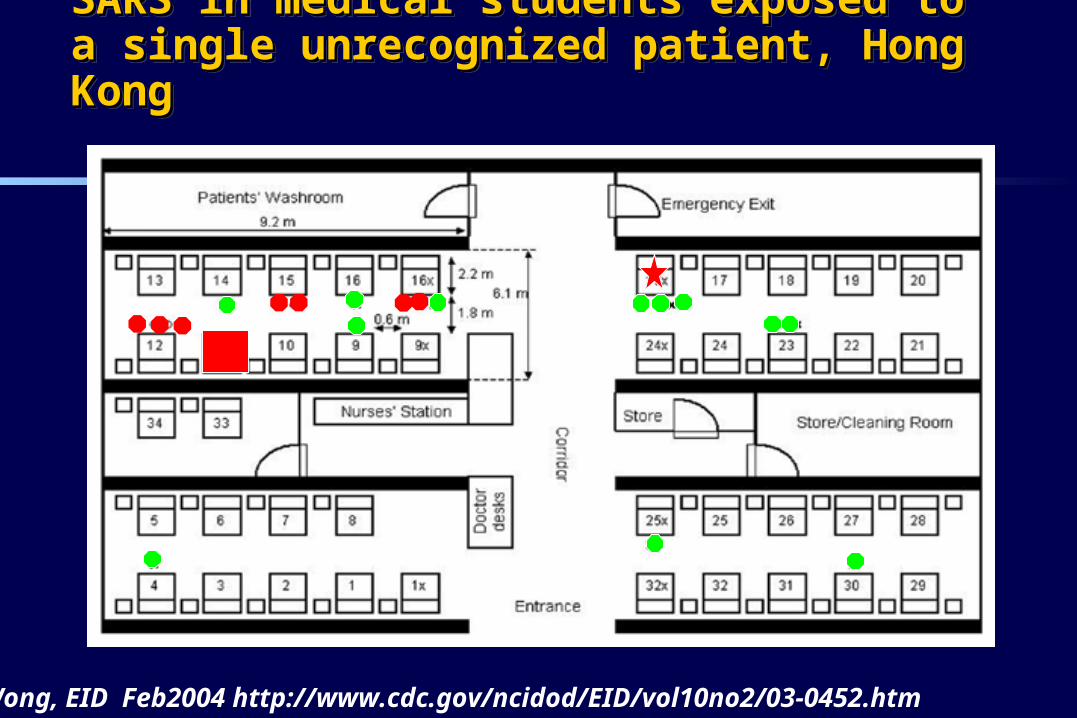
SARS in medical students exposed to a single SARS in medical students exposed to a single unrecognized patient, Hong Kongunrecognized patient, Hong KongSARS in medical students exposed to a single SARS in medical students exposed to a single unrecognized patient, Hong Kongunrecognized patient, Hong Kong
Wong, EID Feb2004 http://www.cdc.gov/ncidod/EID/vol10no2/03-0452.htm
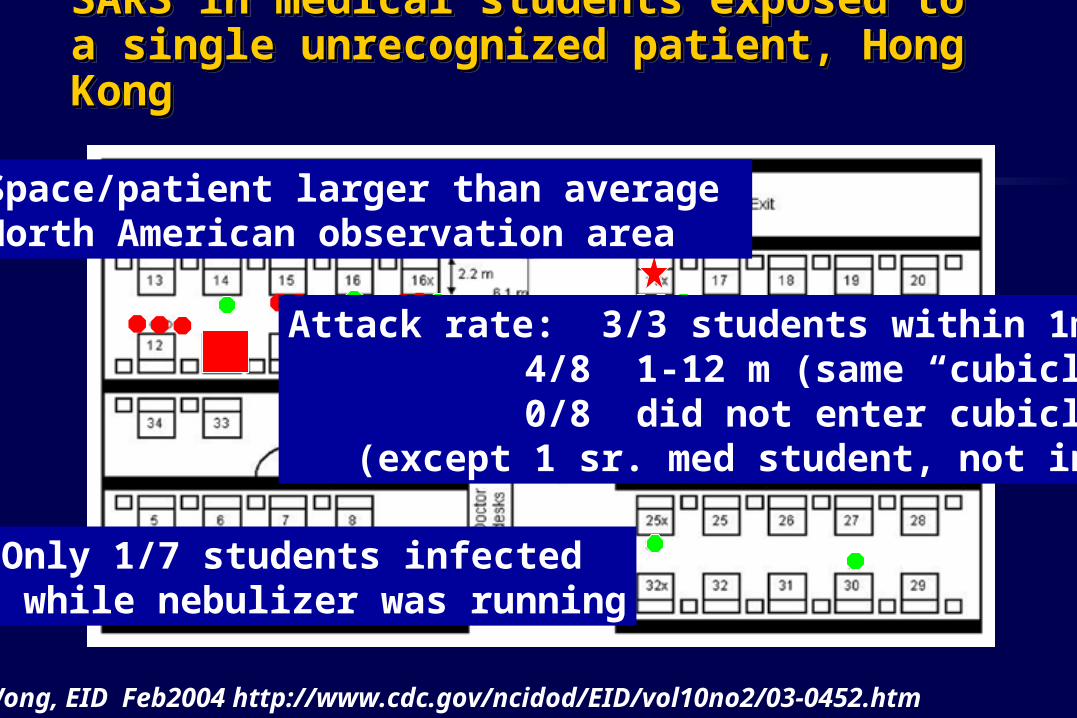
SARS in medical students exposed to a single SARS in medical students exposed to a single unrecognized patient, Hong Kongunrecognized patient, Hong KongSARS in medical students exposed to a single SARS in medical students exposed to a single unrecognized patient, Hong Kongunrecognized patient, Hong Kong
Wong, EID Feb2004 http://www.cdc.gov/ncidod/EID/vol10no2/03-0452.htm
Space/patient larger than average North American observation area
Only 1/7 students infected while nebulizer was running
Attack rate: 3/3 students within 1m 4/8 1-12 m (same “cubicle”) 0/8 did not enter cubicle
(except 1 sr. med student, not in cubicle)
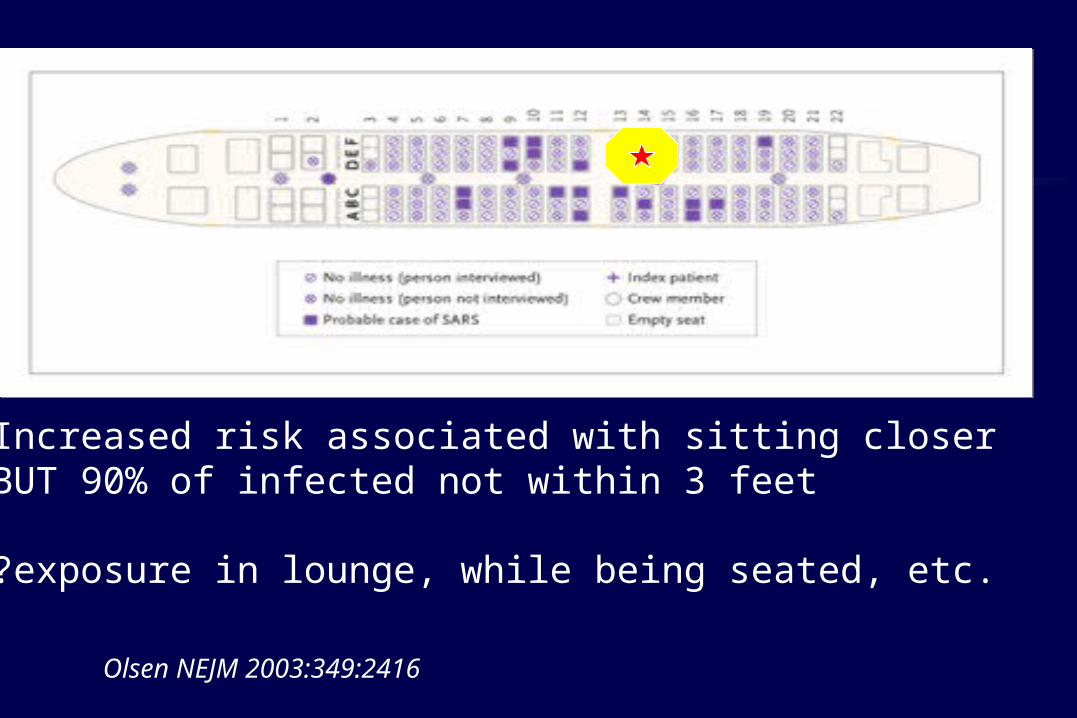
Increased risk associated with sitting closerBUT 90% of infected not within 3 feet
?exposure in lounge, while being seated, etc.
Olsen NEJM 2003:349:2416
Questions about droplet spreadQuestions about droplet spreadQuestions about droplet spreadQuestions about droplet spread
What is contribution of droplet vs contact spread for these diseases?
What is a droplet anyway?
How transmissible are they? How do patients acquire nosocomial respiratory viral diseases?
What is contribution of droplet vs contact spread for these diseases?
What is a droplet anyway?
How transmissible are they? How do patients acquire nosocomial respiratory viral diseases?
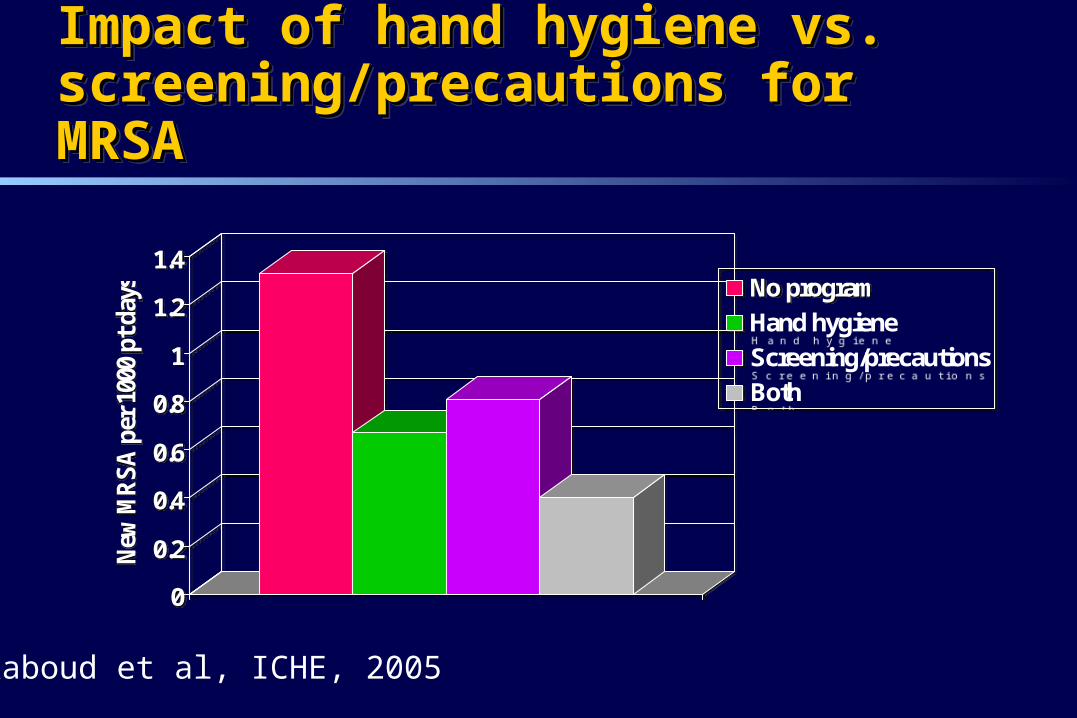
Impact of hand hygiene vs. Impact of hand hygiene vs. screening/precautions for MRSAscreening/precautions for MRSAImpact of hand hygiene vs. Impact of hand hygiene vs. screening/precautions for MRSAscreening/precautions for MRSA
0
0.2
0.4
0.6
0.8
1
1.2
1.4
New
MR
SA
per
100
0 pt
day
s No programHand hygieneScreening/precautionsBoth
0
0.2
0.4
0.6
0.8
1
1.2
1.4
New
MR
SA
per
100
0 pt
day
s No programHand hygieneScreening/precautionsBoth
Raboud et al, ICHE, 2005
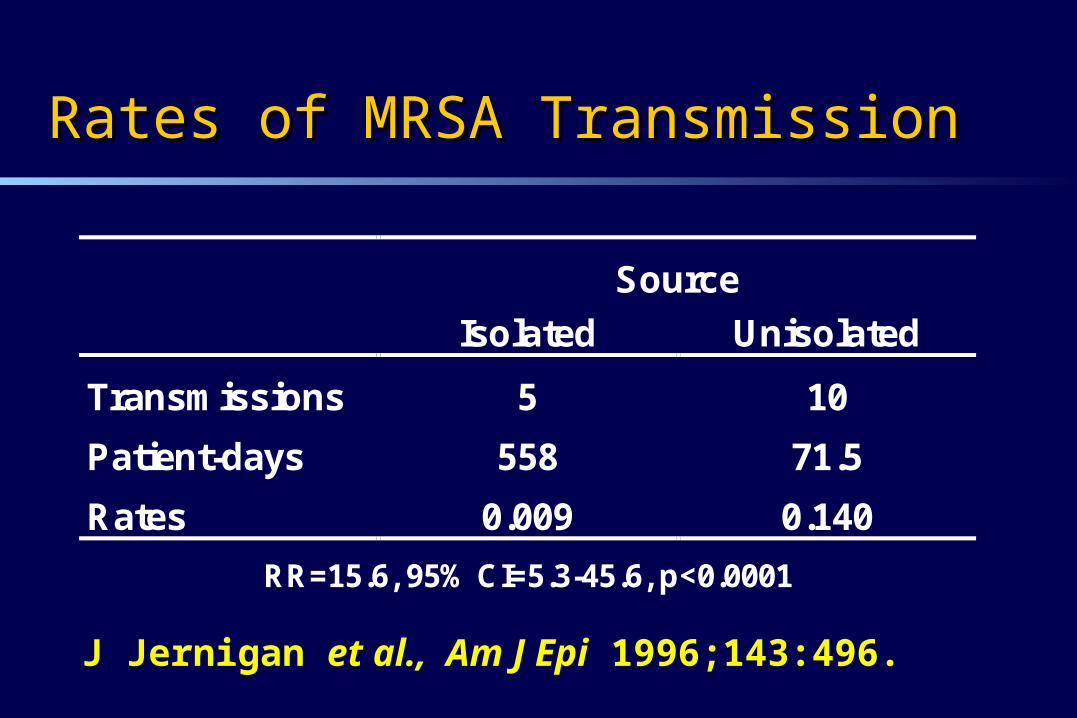
Rates of MRSA TransmissionRates of MRSA Transmission
Source
Isolated Unisolated
Transmissions 5 10
Patient-days 558 71.5
Rates 0.009 0.140
RR=15.6, 95% CI=5.3-45.6, p<0.0001
J Jernigan et al., Am J Epi 1996;143:496.
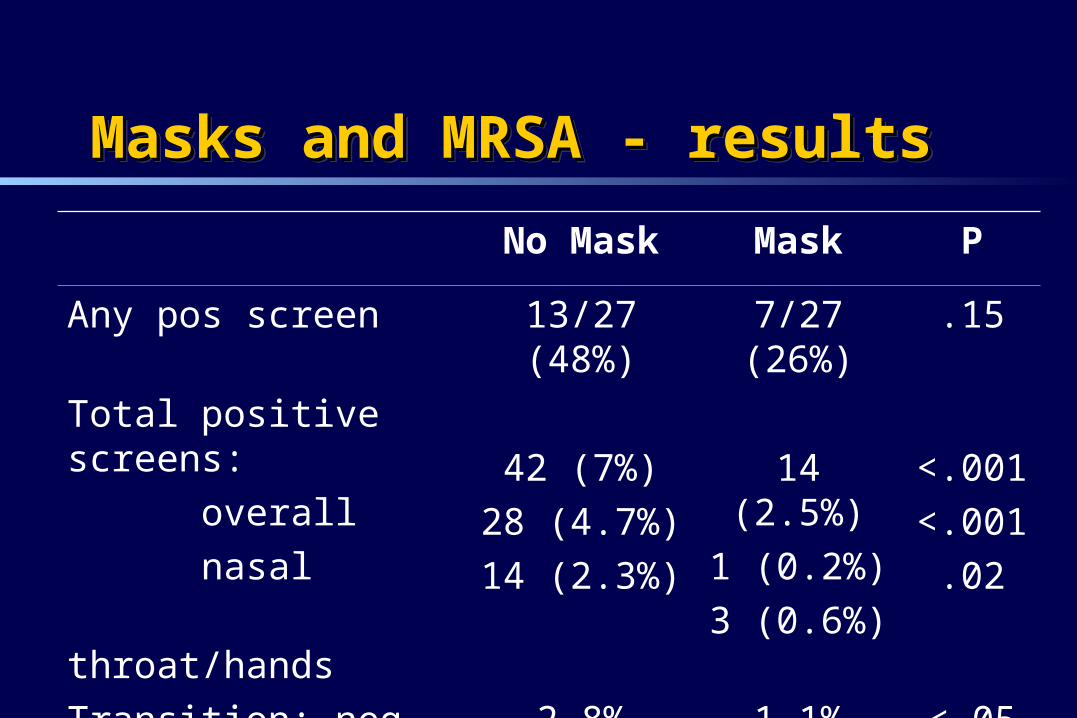
Masks and MRSA - resultsMasks and MRSA - resultsMasks and MRSA - resultsMasks and MRSA - results
No Mask Mask P
Any pos screen 13/27 (48%) 7/27 (26%) .15
Total positive screens:
overall
nasal
throat/hands
42 (7%)
28 (4.7%)
14 (2.3%)
14 (2.5%)
1 (0.2%)
3 (0.6%)
<.001
<.001
.02
Transition: neg-pos 2.8% 1.1% <.05
Green K et al, ICAAC 2002 (Abtr K661).
Ostrowsky BE et al, NEJM 2001;344:1427-1433.
Salmenlinna S et al, Euro JCM & ID 2000;19:101-107.
Esveld MI et al, Ned Tijdschr Geneeskd 1999;143:205-8.
Armstrong-Evans M et al, ICHE 1999;20:312-317.
Jochimsen E et al, ICHE 1999;20:106-109.
Verhoef J et al. Eur J Clin Micro Infect Dis 1999;18:461-466.
Kotilainen P et al. Emerg Infect Dis. 2003;9:169-75.
Silverblatt FJ et al, J Am Geriatr Soc 2000;48:1211-1215.
Studies Reporting Control of MRSA & VRE in Nonacademic Settings Using Active
Surveillance Cultures & Contact Precautions
Studies Showing Cost Benefit of ASC & CP forControlling MRSA & VRE
Jernigan JA et al, ICHE 1995;16:686.
Papia G et al, ICHE 1999;20:473-477.
Chaix et al, JAMA 1999;282:1745.
Montecalvo MA et al, ICHE 2001;22:437-42.
Bronstein M et al, SHEA 2002 (Abst 47, pg 51).
Karchmer TB et al, J Hosp Infect 2002;51:126.
Muto CA et al, ICHE 2002;23:429-435.
Calfee DP et al, ICHE 2002;23:407-410.
Lucet J et al, Arch Int Med 2003;163:181-88.
Evidence for environmental transmissionEvidence for environmental transmissionEvidence for environmental transmissionEvidence for environmental transmission
Organism can be isolated from the environment Organism can be cultured from gloves/hands that
have touched the environment Organism can be transferred from gloves/hands to a
clean site (patient or environment Exposure to contamination is associated with
acquisition of colonization/infection Reduction in contamination is associated with
reduced acquisition of colonization/infection
Organism can be isolated from the environment Organism can be cultured from gloves/hands that
have touched the environment Organism can be transferred from gloves/hands to a
clean site (patient or environment Exposure to contamination is associated with
acquisition of colonization/infection Reduction in contamination is associated with
reduced acquisition of colonization/infection
Evidence for environmental transmissionEvidence for environmental transmissionEvidence for environmental transmissionEvidence for environmental transmission GAS - ?implicated in 2/61 reported outbreaks
– bidet, plastic sheet RSV - Hall et al. transmission to volunteers MRSA
– before/after study of intervention: increase cleaning with focus on shared equipment/ dust removal (J Hosp Infect. 2001;49:109)
– Increased risk of MRSA acquisition by patients being admitted to room previously occupied by MRSA patient (3.9% vs. 2.9%, P=.04) (Huang AIM 2006;166:1945)
VRE – unpublished outbreak data C. difficile - evidence from outbreaks of “room” effect
GAS - ?implicated in 2/61 reported outbreaks– bidet, plastic sheet
RSV - Hall et al. transmission to volunteers MRSA
– before/after study of intervention: increase cleaning with focus on shared equipment/ dust removal (J Hosp Infect. 2001;49:109)
– Increased risk of MRSA acquisition by patients being admitted to room previously occupied by MRSA patient (3.9% vs. 2.9%, P=.04) (Huang AIM 2006;166:1945)
VRE – unpublished outbreak data C. difficile - evidence from outbreaks of “room” effect
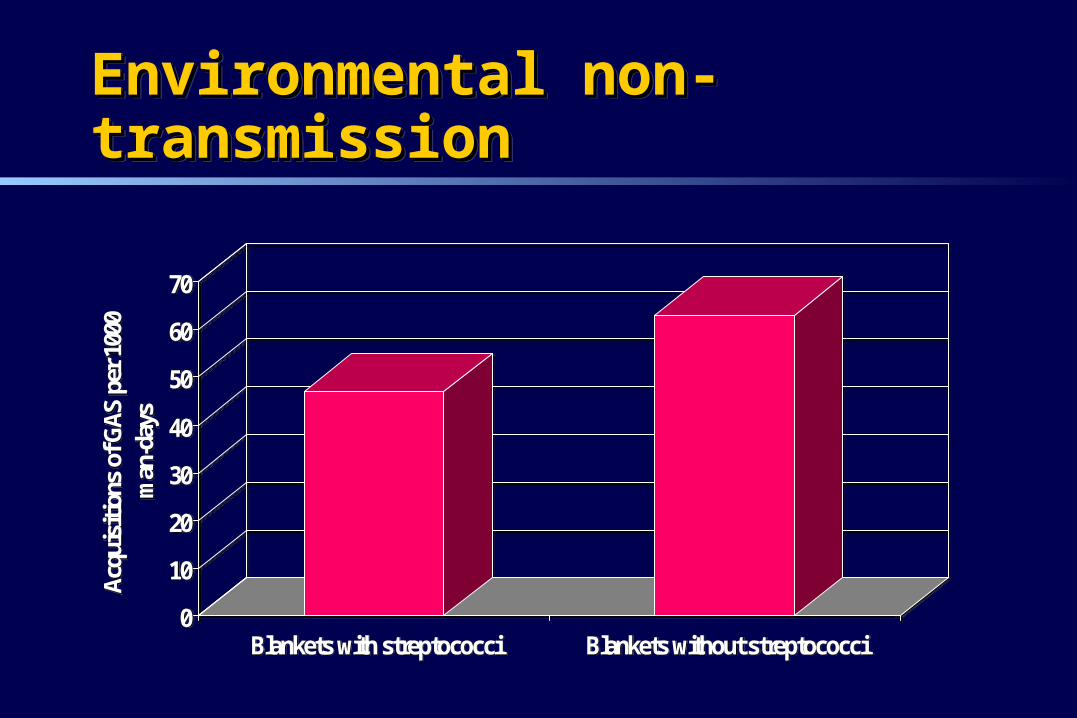
Environmental non-transmissionEnvironmental non-transmissionEnvironmental non-transmissionEnvironmental non-transmission
0
10
20
30
40
50
60
70
Acqu
isiti
ons
of G
AS p
er 1
000
man
-day
s
Blankets with streptococci Blankets without streptococci0
10
20
30
40
50
60
70
Acqu
isiti
ons
of G
AS p
er 1
000
man
-day
s
Blankets with streptococci Blankets without streptococci
GuidelinesGuidelinesGuidelinesGuidelines
Canadian infection control guidelines– http://www.phac-aspc.gc.ca/dpg_e.html#infection
US HICPAC guidelines– http://www.cdc.gov/ncidod/hip/Guide/guide.htm
AIA design guidelines http://www.aia.org/publications/guidelinesabout.asp
Canadian infection control guidelines– http://www.phac-aspc.gc.ca/dpg_e.html#infection
US HICPAC guidelines– http://www.cdc.gov/ncidod/hip/Guide/guide.htm
AIA design guidelines http://www.aia.org/publications/guidelinesabout.asp