71
IV TERAPY & Central Venous Catheters
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | erik-green |
| View: | 230 times |
| Download: | 7 times |
IV TERAPY &
Central Venous Catheters
INSERTION OF PERIPHERAL IV LINE
Aims
1. To gain peripheral venous access in order to:• administer fluids• administer blood products, medications and nutritional components2. To minimise the risk of complications when initiating IV therapy through:• judicious choice of equipment• careful choice of IV site• good insertion technique• aseptic preparation of infusions
Key points 1. Only nurses who have been certified as competent in the
insertion of IV cannula will perform this procedure. 2. Where the patient is less than 14 years of age, the IV
cannula will be inserted by a medical practitioner. The exception will be in the case of neonates where neonatal trained nurses may insert an IV cannula if directed by a medical officer
3. In the case of two unsuccessful attempts at insertion, the operator will seek the assistance of another experienced nurse for one additional attempt. After a total three unsuccessful attempts the assistance of a medical practitioner will be sought.
Known Complications of IV Therapy
PhlebitisContributing factors:
• Catheter material • Catheter size• Site of insertion • Skill of operator• Duration of cannula • Type of infusion• Dilution of solution • Host factors • Insertion in ED • Type of skin prep • Frequency of dressing change• Presence of infection
InfectionContributing factors:• Contaminated infusions• Inadequate skin preparation• Poor technique• Host factors
Extravasation
Contributing factors• Age• Site of cannula• Type of cannula• Duration of cannula• IV drug infusions
Selection of EquipmentCannula selection
1. Select cannula based on purpose and duration of use, and age of patient.2. Consider risk of infection and extravasation.3. Cannulae made from polyurethanes are associated with decreased risk of phlebitis.4. Steel needles have higher risk of extravasation and should be avoided where tissue necrosis is likely if extravasation occurs.

Skin prep
Antiseptic solution - 70% isopropyl alcohol, 0.5 - 1% Chlorhexidine.Use an aqueous based alternative if there is a known allergy to alcohol
Selection of Catheter Site
Choose a suitable vein. In adults, use long straight veins in an upper extremity away from the joints for catheter insertion - in preference to sites on the lower extremities. If possible avoidveins in the dominant hand and use distal veins first.Do not insert cannula on the side of mastectomy or AV shunts/Gortex. Transfer catheter inserted in a lower extremity site to an upper extremity site as soon as the latter is available.In paediatric patients, it is recommended that the cannula be inserted into the scalp, hand, or foot site in preference to a leg, arm, or ante cubital fossa site (Category II)
Reasons For Inserting Central Venous Catheters
Limited vascular access Administration of highly osmotic or caustic fluids
or medications Frequent administration of blood and blood
products Frequent blood sampling Measurement of CVP Hemodialysis
Type of CVC Inserted Depends On
Patient’s condition Anticipated length of therapy
Types Of Central Venous Catheters
Nontunneled central catheters Tunneled central catheters Peripherally inserted central catheters
(PICC) Implantable ports
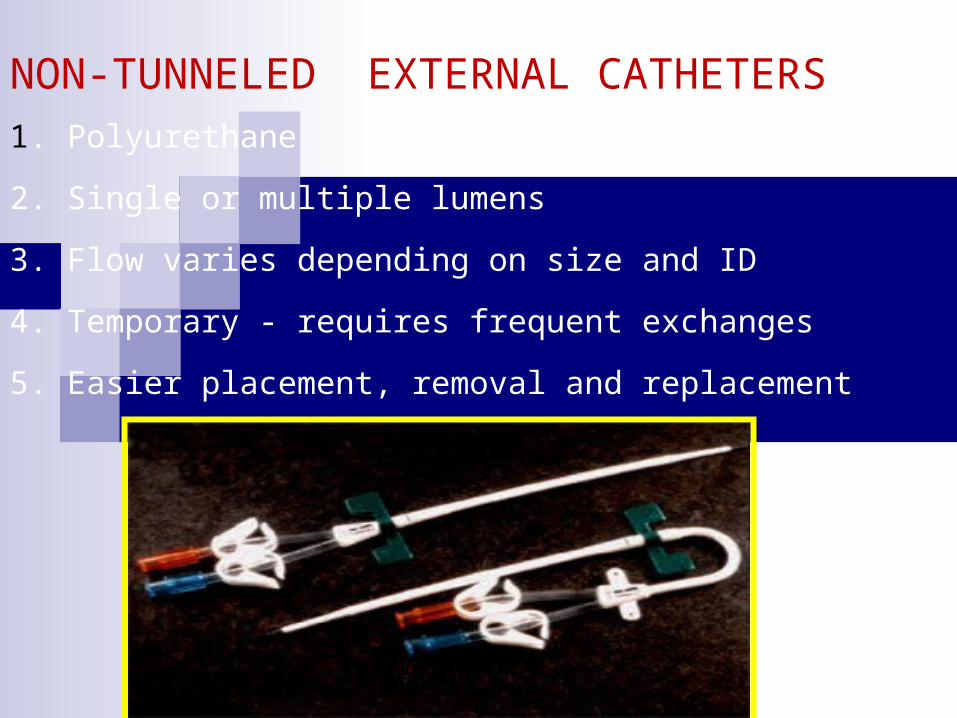
NON-TUNNELED EXTERNAL CATHETERS1. Polyurethane
2. Single or multiple lumens
3. Flow varies depending on size and ID
4. Temporary - requires frequent exchanges
5. Easier placement, removal and replacement
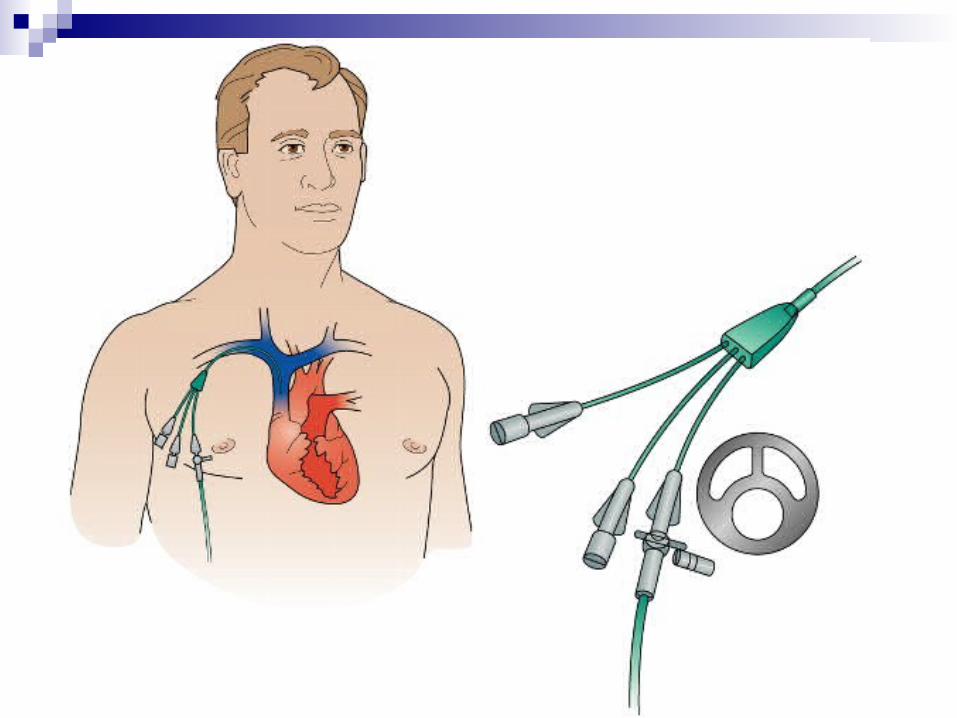
Nontunneled Central Venous Catheters
Used for short-term therapy Inserted percutaneously
Subclavian vein Internal jugular veinFemoral vein
Has from 1 to 4 lumens or ports Usually from 6 to 8 inches in length
Can be quickly inserted Not flexible and may break Dislodged more easily Has the highest infection rate Dressing changes required using aseptic
technique Unused ports must be routinely flushed with
heparin solution and clamped
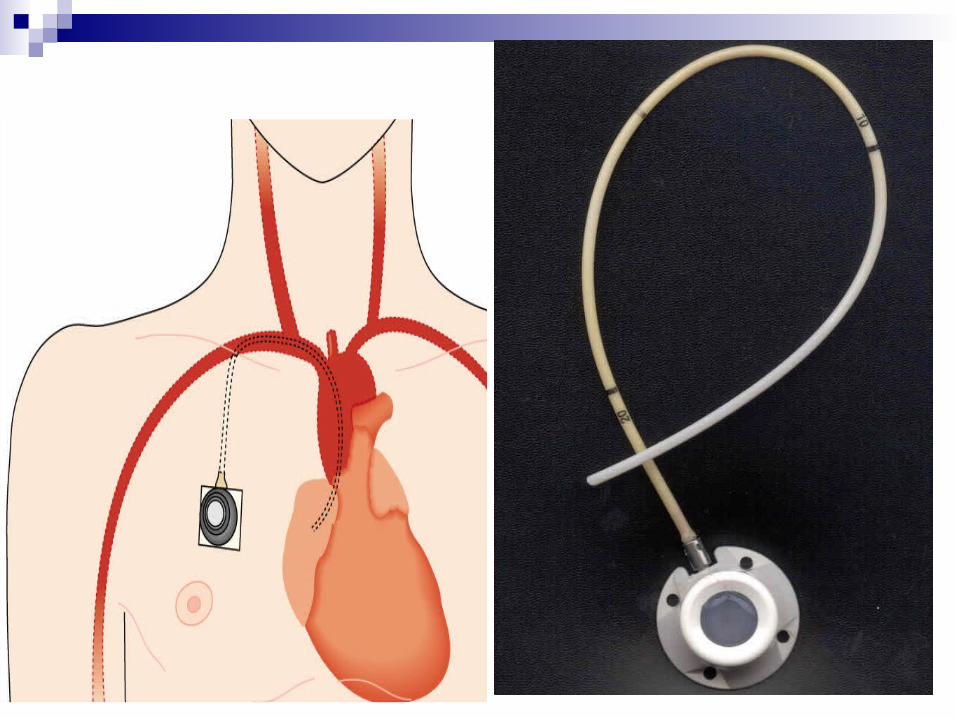
TUNNELED CATHETERS
1. Single or multiple lumens
2. Flow - variable
3. Long term
4. Easy access (no skin puncture)
5. Cuff - Dacron, vita
Tunneled catheter with cuffs
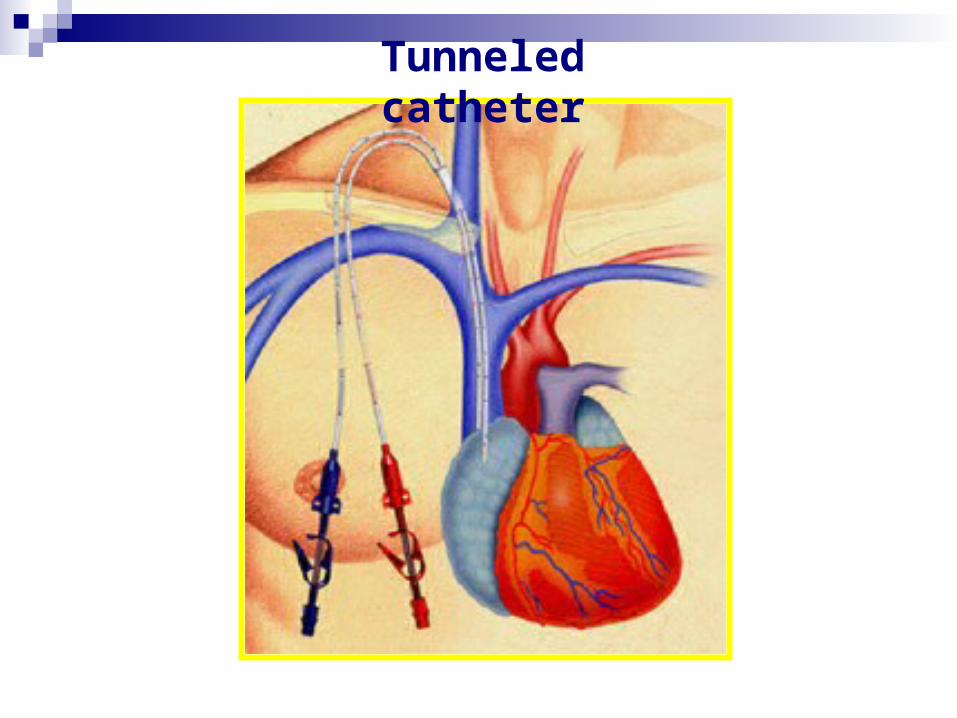
Tunneled catheter
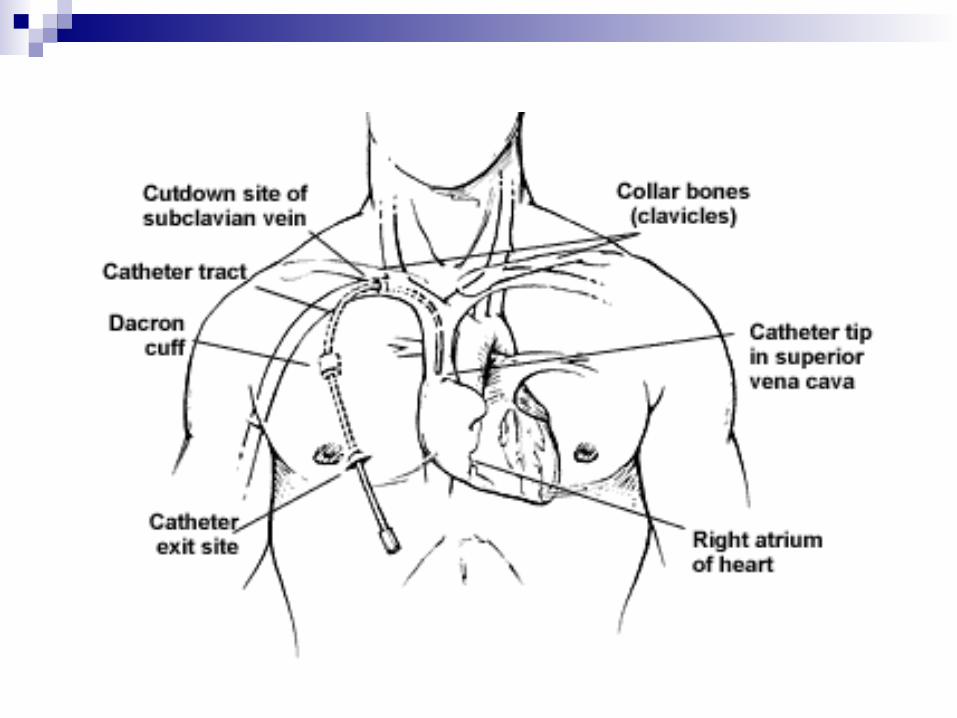
Tunneled Central Venous Catheters
Used for long term therapy Inserted surgically Small Dacron cuff sits in subcutaneous tunnel No dressing is required after cuff heals unless
the patient is immunocompromised Initially sutured but removed in 7 to 10 days External portion of the cath can be repaired
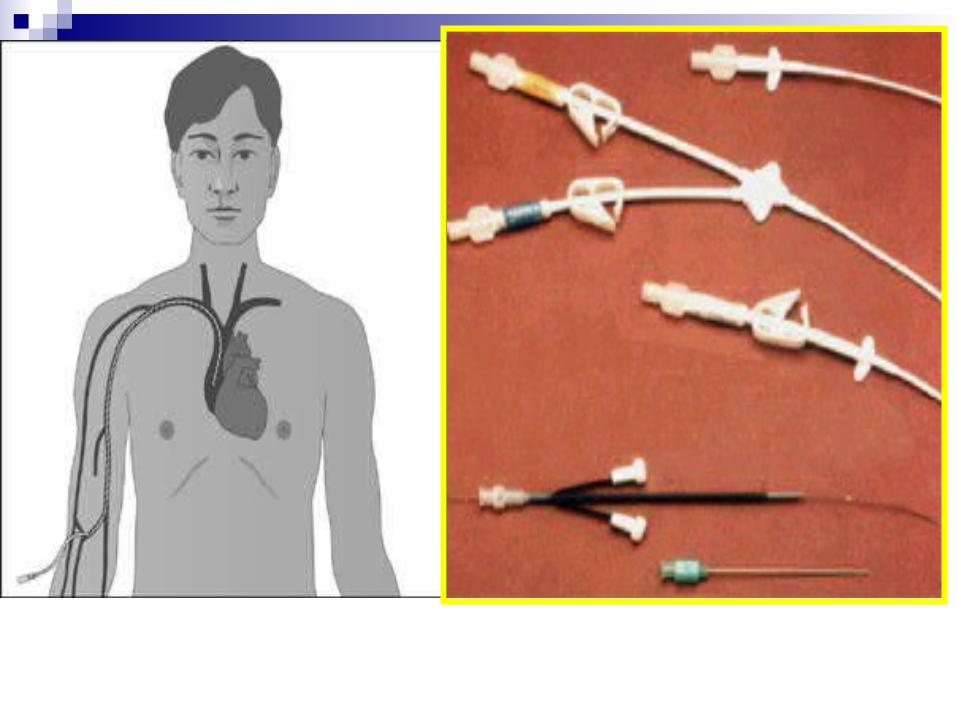
Peripherally Inserted Central Catheters (PICC)
Used for intermediate to long term therapy May be single or double lumen Inserted percutaneously
Basalic veinCephalic vein
Threaded into the superior vena cava May be inserted by specially trained RN
PICC LINES
1. Silastic or polyurethane
2. Single or double lumen
3. Low flow
4. Short - long term
5. Easy access
Infusing or drawing blood from smaller gauged PICC may be more difficult
Small gauged PICC infuse fluids slower and occlude faster
Measure and document external length of PICC with each dressing change
Dressing acts as a bacterial shield and helps anchor cath
Unused ports must be flushed with Heparin solution and clamped

SUBCUTANEOUS PORTS1. Single or double lumen
2. Flow - most commonly slow
3. Long term
4. Access requires needle puncture

5. Less maintenance
6. Activity is unlimited after site heals
7. Cosmetically more appealing
8. Concealed pocket retards infection (?)
SUBCUTANEOUS PORTS
Minimizes infection Huber needle must be used to access port Must always confirm needle placement before
med administration Transparent dressing covers Huber needle and
port Unused port is flushed every 28 days with
Heparin solution

SUBCLAVIAN VEIN COMPLICATIONS
STENOSIS THROMBOSI PINCH OFF
SYNDROME
Subclavian vein (SCV) access is prone to more complications than internal jugular vein (IJV)
ADVANTAGES OF THE RIGHT IJ
1. Larger
2. More superficial
3. Further from the lung
4. More direct route to the heart
5. Acute and chronic complications are reduced
CENTRAL VENOUS CATHETER PLACEMENT
1. Prep
2. Access
3. +/- Tunnel
4. Secure
Alcohol scrub to remove surface oils
Chlorhexidine scrub
Betadine prep (allow to dry)
Ioban dressing and drapes
Maximum Sterile Barrier - Surgical hats, gowns, masks & gloves
3 - 5 min. surgical scrub
Antibiotics (controversial) 30-60 min. prior
Cefazolin (Kefzol, Ancef) 1 gm IV or
Gentamycin 80 mg IV
PREP
General Nursing Care Of Patient With CVC
Always follow the institution’s policy and procedure
Before insertion, lines are initially flushed with saline
During percutaneous insertion of CVC in the subclavian or jugular, place patient in Trendlenberg or have him perform Valsalva maneuver
After insertion, an occlusive gauze or transparent dressing is applied
Blood is aspirated through all lumens to verify patency
Chest xray must be performed before use Each lumen of the cath is secured with a
Leur-lok cap or CLC 2000 device
Use only needless system to access ports Infusing devices are used for all infusions TPN is administered exclusively through a
dedicated line and port. Catheters must be clamped when
removing the cap and when not in use
Flushing of linesEach lumen is treated as a separate cath Injection caps are vigorously cleaned with
alcoholUse 10cc or larger syringe for administration
of meds or flush Turbulent flush technique is recommended
For med administration, use SAS methodIf port is not to be maintained with a
continuous infusion, end with Heparin flush solutionPeds 10kg> and adults – 100 units
Heparin/ml with preservativesNeonates and peds <10kg – 10 units
Heparin/ml without preservativesFor specific amounts see procedure
Clamp cath while infusing last ½ cc of flushIf CLC 2000 used, do not clamp cath until
syringe disconnected
Site assessment and determination of external cath length is performed and documented with each dressing change
Tubings are changed per protocol – 72hrs Caps and connections are changed per
protocol – 3-7 days
Dressing changes per protocolUse sterile techniqueChange when damp, soiled or loosenedChange every 7 days if transparentChange every other day if gauze is usedClean skin around insertion site with
alcohol in a circular motion. Also clean cath with alcohol
Use antmicrobial disk if indicatedForm a loop of the tubing or cath outside
the dressing and anchor securely with tapeLabel site with date, time and initialsDocument dressing change, condition of
site and length of external cath when appropriate
For drawing blood specimenDiscard initial sample of bloodCollect specimenFlush with 10cc salineFlush with Heparin solution if
indicated
Monitor for complicationsInfection
PhlebitisSepticemia or pyrogenic reaction
Air embolismThrombosis/occlusionExtravasationDamaged cath
COMPLICATIONS
1. Acute Procedural
2. Sub-acute Infection
3. Chronic
Infection
Catheter fragmentation
Non-function
COMPLICATIONS:ACUTE1. Spasm 4. Pneumothorax
2. Access failure 5. Malposition
3. Arterial puncture 6. Air embolus
AIR EMBOLUS: SYMPTOMS
1. Respiratory distress
2. Increased heart rate
3. pulse
5. Cyanosis
4. Poore in the level of consciousness
AIR EMBOLUS: TREATMENT
1. Left lateral decubitus (Durant’s) Position
2 100% O2
3. Vasopressin if necessary
4. Chest compression
5. Aspiration through catheter +/-
Mortality decreases from 90% 30%
with conventional treatment
COMPLICATIONS:CHRONIC
1. Infection
2. Catheter fragmentation
3. Non-function
Risk Factors
Four major risk factors are associated with increased catheter-related infection rates:Cutaneous colonization of the
insertion siteMoisture under the dressingProlonged catheter timeTechnique of care and placement of
the central line
Evidence-Based Strategies Selected to Reduce CLA-BSIs
1. Central line-associated bloodstream infections bundle
2. Hand hygiene
3. Maximal sterile barriers
4. Chlorhexidine for skin asepsis
5. Avoid femoral lines
6. Avoid/remove unnecessary lines
Hand Hygiene Cornerstone of any infection
prevention program Many studies have shown that
improvement in hand hygiene significantly decreases a variety of infectious complications
Insufficient or ineffective hand hygiene contributes significantly to a greater bacterial burden and subsequent spread of microorganisms within the environment
Hand Hygiene
Use of waterless alcohol-base hand rub Most effective and efficient
method for hand antisepsis against bacterial pathogens
When hands are visibly soiled, they should be washed with soap and water
Efficacy of Hand Hygiene Preparations in Killing Bacteria
Good Better Best
Plain Soap Antimicrobial soap
Alcohol-based handrub
Maximal Sterile Barriers
One study found a 6-fold higher rate of catheter-related septicemia when minimal sterile barriers (sterile gloves and small drape) were used instead of maximal sterile barriers
Raad II, Hohn H, Gilbreath J, et al. Prevention of central venous catheter-related infections by using maximal sterile barrier precautions during insertion. Infect Control Hosp Epidemiol. 1994;15:231–238.
Chlorhexidine for Skin Asepsis
Studies have compared chlorhexidine gluconate (CHG) versus povidone iodine as a skin antiseptic for catheter insertion and routine insertion site care Recent meta-analysis, the use of CHG rather than
povidone iodine was found to reduce the risk of CLA-BSIs by approximately 50% in hospitalized patients who required short term catheterization
Chaiyakunapruk N, Veenstra, DL, Lipsky BA, Saint S. Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: a meta-analysis. Ann Intern Med. 2002;136:792–801.
Benefits of CHG
2% CHG in tincture of isopropyl alcohol has rapid bactericidal activity and is effective within 30 seconds after application versus 2-minute period for povidone iodine
CHG provides persistent bactericidal activity on the skin and maintains its activity in the presence of other organic material
Minimal systemic absorption
Site Selection: Avoid Femoral Lines
Insertion of CVCs can lead to serious and sometimes life-threatening complications, whether of mechanical, infectious, or thrombotic origin
Higher rate of infectious complications in study comparing femoral lines versus subclavian lines 19.8% vs 4.5%
Avoid and Remove Unnecessary Lines Once placed, there should be periodic, if
not daily assessment, of its continued need, with emphasis on prompt removal
Empowerment of Nursing
One of the most important steps in preventing CLA-BSIs is to empower the nursing staff to stop the central line insertion procedure if the guidelines were not followed
TYPES OF INFECTION
EXIT SITE, TUNNEL/POCKET or CATHETER
1. Cutaneous - pain, erythema, swelling, +/- exudate
2. Bacteremia - fever, leukocytosis and positive blood cultures
3. Septic thrombophlebitis - bacteremia, thrombosis and purulent discharge
INFECTION CAUSATIVE ORGANISMS
Staph epidermidis 25-50%
Staph aureus 25%
Candida 5-10%
INFECTION
1. Septic thrombophlebitis - remove catheter
2. Cutaneous - local treatment3. Bacteremia -
1. IV antibiotics 48 -72 hoursif improved - keep catheterif no change, worse or recursremove catheter or2. Exchange catheter over wire, 85% cure with treatment
Continue to treat infection for 10 - 14 days
If ineffective - try locking with thrombolytics between antibiotic doses and administer antibiotics through catheters
INFECTION
Discharge Teaching For The Patient With A CVC
Proper handwashing and principles of sterile technique
Dressing change procedure and frequency Flushing and cap change procedure and
frequency Observation of cath and insertion site
When to call the physicianTemp of 100.5F or greaterChills, dyspnea, dizzinessPain, redness, swelling, or drainage at
siteUnresolved resistance, pain or fluid
leaking while flushingHole or tear in cathExcessive bleeding at siteChange in length of external cathSwelling in neck, face, chest, or arm
General safety measuresNo sharp objects near cath Clamp cath when not in useNo pulling or tension on the cathDiscard syringes and needles in sharps
containerActivity limitationsUse a stress loop
Home health referral
Discontinuing A CVC Follow the institution’s policy and procedure For percutaneous internal jugular or subclavian
insertion sites, place patient in trendlenburg position and have him perform the Valsalva maneuver
Remove cath and apply pressure with an occlusive dressing over a petroleum gauze
Check cath to ensure tip is intact Document how patient tolerated procedure,
placement of dressing and cath tip intact