19
J Hornsby, B Carrick, DK Garg, TS Gill University Hospital of North Tees Colorectal NSSG Education & Audit Day 17/05/2013 Single-port Resection for Colorectal Cancer
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | aubrey-parker |
| View: | 213 times |
| Download: | 0 times |

J Hornsby, B Carrick, DK Garg, TS Gill
University Hospital of North Tees
Colorectal NSSG Education & Audit Day
17/05/2013
Single-port Resection for Colorectal Cancer

Evolution of Laparoscopic Surgery
1806 Bozzini’s “Lichtleiter“1
1901 1st laparoscopy1936 Lap. tubal ligation1985 Lap.Cholecystectomy2
2000s Laparoscopic colorectal surgery, Robotic surgery, Single port access, natural orifice transluminal endoscopic surgery
1Bush RB (1974). Urology 3(1): 119-123.2Reynolds W (2001): “The first laparoscopic cholecystectomy”. JSLS 5(1): 89-94.

Laparoscopic Colorectal Cancer Surgery
• Reduced blood loss• Less pain• Faster recovery• Shorter length of stay• Comparable morbidity &
mortality1
• Oncologically safe2
• Better cosmetic results• Gold standard
1Reza MM (2006): BJS 93(8): 921-928.2Jayne DG (2010): BJS 97(11): 1638-1645.
BJS 97(11) 211

SPA laparoscopic surgery
• Better cosmesis than conventional laparoscopy
• Technically challenging• Learning curve• Comparative outcomes
with conventional laparoscopic in audit of all colorectal cases1
1. Kanakala et al. Techniques in coloproctology. 2012

Single Port Laparoscopic Resections for Colon Cancer at North Tees
• Single port resections for colorectal cancer since November 2009
• Experience of > 100 benign cases
• Retrospective audit of all single port resections for colorectal cancer
• Data from notes, Theatreman, pathology system

Outcomes
• Patient profile• Operative time• Length of stay• Morbidity and
mortality• Dukes stage• Lymph node yield

Cases• DG 10 cases
• TG 21 cases
2009 2010 2011 2012 2013
R Hemicolectomy 0 1 5 7 3
L Hemicolectomy 0 0 3 1 2
Anterior resection 1 0 3 2 2

Age
• Mean 67.9
• Median 67
• Range 34 - 94
• BMI: Mean 24 (17.9-32.8), Median 24.8
• 4 patients had documented previous abdominal surgery
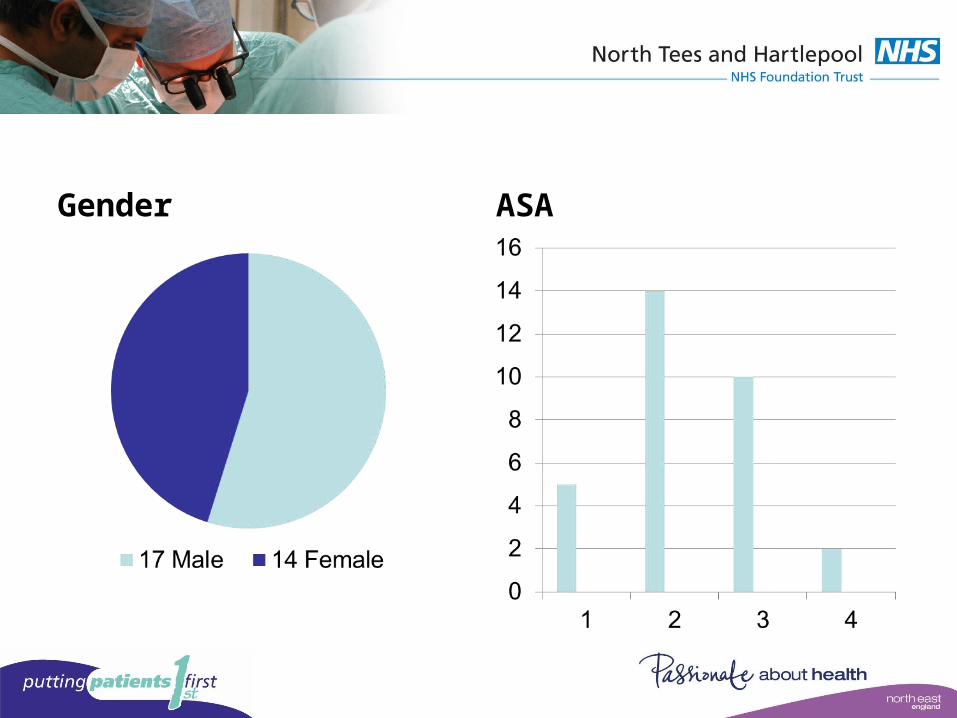
Gender ASA

Operative time• Mean 140 mins (85-210)• R hemi 135 mins (85-
210)• L hemi/AR 156 mins
(104-170)

Length of Stay• Mean 5.8 days• Median 4• Range 3 – 25
Morbidity & Mortality
• No 30 day mortality, no leaks
• 2 (6.5%) wound infections
• 1 (3.2%) collection requiring US guided drainage
• 2 extended hospital stays
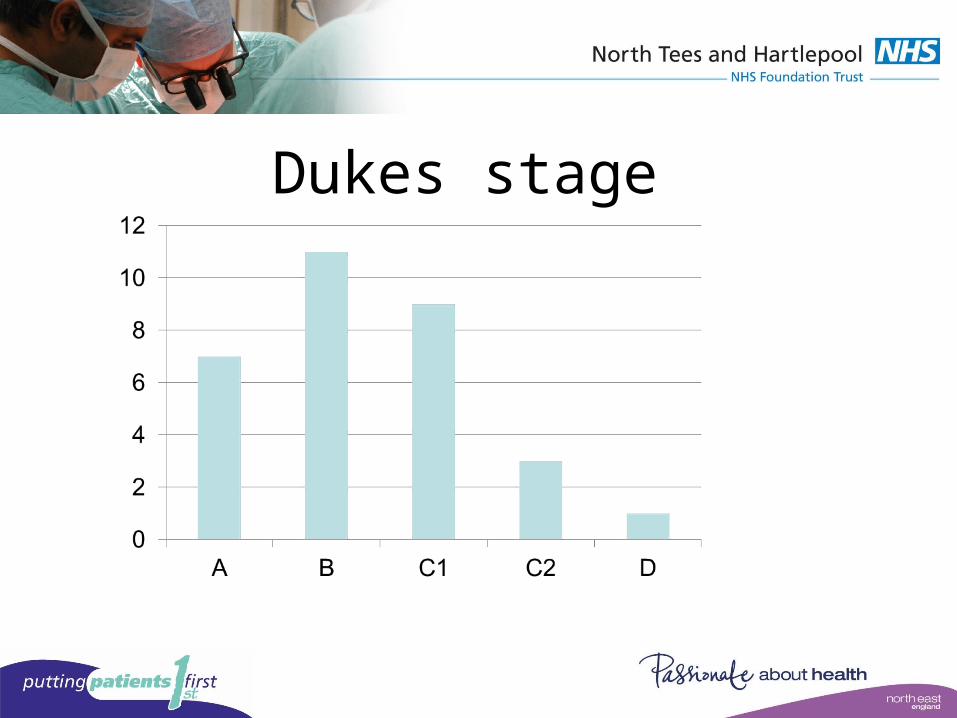
Dukes stage

Lymph node yield
• Mean 21.5, median 17, range 5-92
• 6 (19.4%) less than 12

Conclusion
• Initial results indicate that this technique appears to be safe without excessive operating times and recovery time
• Further audits required with longer follow up and comparison with conventional laparoscopic resections



Dukes Stage
B C1 C2 D
11 9 3 1

















