www.cfn-nce.ca Frailty Assessment of Older Canadians Using Emergency Services with Tablet Technology Jacques Lee, MD, MSc, FRCPC Sunnybrook Research Institute Webinar Series January 25, 2017
Transcript
www.cfn-nce.ca
Frailty Assessment of Older Canadians Using Emergency Services with Tablet Technology
Jacques Lee, MD, MSc, FRCPCSunnybrook Research Institute
Webinar SeriesJanuary 25, 2017
www.cfn-nce.ca
Reminder: Q-&-A session
• Follows Dr. Lee’s presentation
• Submit your Qs online during presentation
• We will answer as many Qs as time permits
2017-01-25
www.cfn-nce.ca
Reminder: Survey & Webinar
2017-01-25
• Survey will pop up on your screen after webinar • Feedback on how to improve webinar series
• Webinar slides & video available for viewing online within 1-2 days at:
• Wednesday, February 1, 2017 at 12 noon ETAntidepressant guidelines for long-term care residents with advanced frailty – results of CFN-funded Knowledge Synthesis Grant – Laurie Mallery, Constance LeBlanc and Michael Allen, Dalhousie University
• Wednesday, February 15, 2017 at 12 noon ETA scoping review of evidence for measuring frailty in pre-hospital and hospital settings – results of CFN-funded Implementation Grant – Olga Theou, Dalhousie University
• Wednesday, March 1, 2017 at 12 noon ETModeling changes in assessments to predict needs and guide care planning in home care – CFN-funded Knowledge Synthesis Grant – Debra Sheets and Stuart MacDonald, University of Victoria
• Emergency Services Staff Physician and Scientist at the Sunnybrook Research Institute in Toronto
• Director of Research for the Department of Emergency Services at the Sunnybrook Health Sciences Centre
• Assistant Professor, Clinician Scientist and former Director of Resident Scholarly Activities in the Department of Medicine at the University of Toronto
• Research focuses on improving the care of older adults who need emergency services
2017-01-25
Frailty Assessment of Older Canadians Using Emergency Services with Tablet Technology
Jacques Lee,MD, MSc, FRCPC
Frailty assessments of Older
Canadians Using Emergency
Services (FOCUS)
Canadian Frailty Network Webinar
Jacques S. Lee MD, MSc, FRCPC
Acknowledgements
• Canadian Frailty Network (CFN)
Implementation Grant 2015
• No conflicts to declare
Acknowledgments
My Qualifications?
• Knows how to read
• Knows where the library is
Acknowledgements Collaborators
• Dr. Mary Tierney, PhD
• Dr. Mark Chignell, PhD
• Tiffany Tong, PhD (Cand.)
• Dr. Judah Goldstein, PhD
• Dr. Ken Rockwood, MD PhD
• Dr. Marcel Emond, MD, PhD
• Dr. Marie-Josee Sirois
• Dr. David Ryan, PhD
• Mike Nolan, MA
Collaborators
• Dr. Alex Kiss, PhD
• Dr Gary Naglie, MD, MSc
National Coordinator
Joanna Yeung
Why?
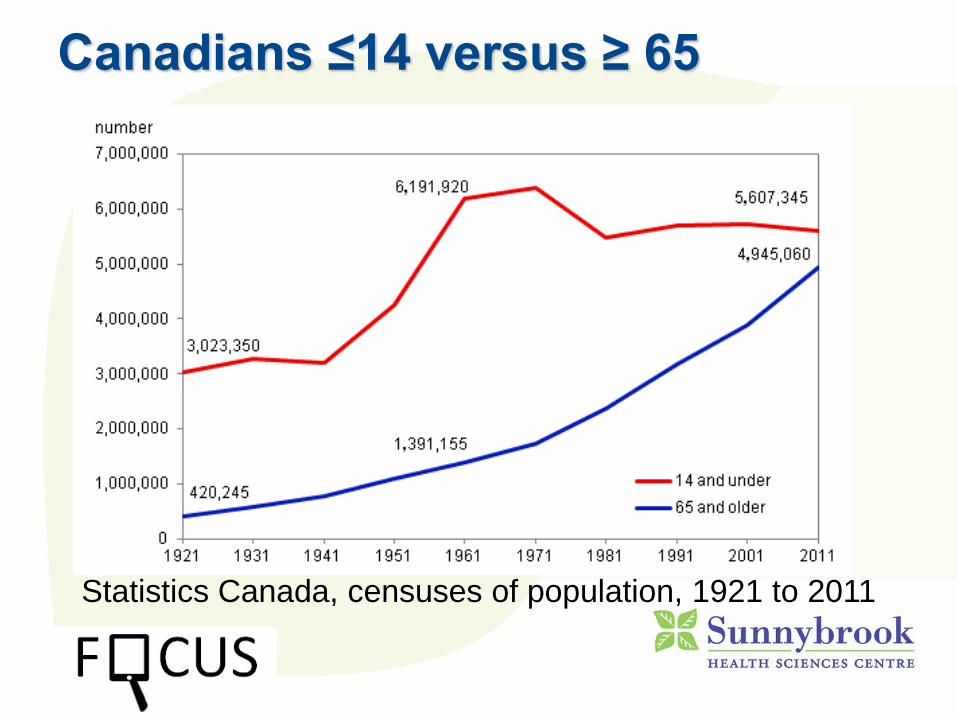
Canadians ≤14 versus ≥ 65
Statistics Canada, censuses of population, 1921 to 2011
Demographics
• For the first time in history as of July 2015,
The number of Canadians 65 and
older exceeds the number of
children 14 and younger 1
• The doubling of older people will happen
sooner in Canada than in any other G7
nation.
Are we ready for the Grey
Tsunami?
Our Ability to
provide care with
the CURRENT
overcrowding
raises grave
concerns for the
future…
Assessing Frailty in the ED
Sunnybrook ED - 60,000 visits / year
• 9 ED physicians and 30 nurses assess 160
- 226 patients per day
• 35 – 50 of those are aged 65 plus
• The vast majority are first time encounters
– no familiarity with patients history
• Rapid methods of assessing frailty are
needed for ED staff
Frailty in Older Canadians
• The majority of older Canadians, at any
age, are robust (56% of those ≥ 85)1
• But a significant minority suffer from frailty,
which makes them vulnerable to adverse
events 2-8 including
• Falls, Functional Decline, Infections
• DELIRIUM
Why is ED Delirium Important?
• Delirium is COMMON 9-15
- 10% in ED,
• Delirium is LETHAL16-17
- 1 year Mortality up to 35-40%
- INDEPENDENT RISK (AHR 2.1)
• Delirium is NOT ALWAYS REVERSIBLE
- Average 6-12 months to return to
baseline 18-19, Some never recover
• DELIRUM IS OFTEN UNRECOGNIZED
• Only recognized in 17% - 24% 20 -22
• 17% - 25 % of those with delirium discharged
home 20
• Mortality Risk 3 - 8.5 x higher if sent home with